
Abstract
Dissociation has been defined as a failure to integrate information and experiences in the normal way and it manifests as experiences of amnesia, depersonalization, derealization, and absorption [1]. There is strong evidence of a relationship between dissociation and childhood maltreatment [2], where dissociation is considered to serve as a defense mechanism against intolerable, trauma-associated memories and feelings. Dissociation is a key feature in certain diagnostic groups, such as dissociative disorders [3], [4], post-traumatic stress disorder [5], and personality disorders [6]. Associations between high levels of dissociation and eating disorders [7], [8], substance abuse [9–11], and anxiety and mood disorders [11], [12] have also been demonstrated. Apart from the psychological components of dissociation, the importance of somatoform dissociative symptoms has been established [12], [13], and it has also been associated with childhood adverse experiences [14]. Somatoform dissociation denotes phenomena that are manifestations of a lack of integration of somatoform experiences, reactions and functions [13]. Although dissociation has been widely studied, there is still controversy over the classification [13], [15], [16] and epidemiology of dissociative disorders [17], and the aetiology of dissociative phenomenon [11].
Several recent studies have suggested that dissociative features and alexithymia may be related. Alexithymia, characterized by constriction in experiencing emotions and difficulties in communicating feelings [18], also appears to be correlated with trauma [19]. Some studies have found a relationship between dissociation and alexithymia [20–23], but it has been argued that a depressed mood accounts for the group differences between the Toronto Alexithymia Scale (TAS) and Dissociative Experiences Scale (DES) scores [24]. Alexithymic features have also been strongly related to depressive symptoms [25].
Both dissociation and alexithymia have been independently associated with self-mutilative behaviour [26]. A strong relationship between dissociation, suicide attempts and self-mutilation was found in a large nonclinical sample [27], and studies with small clinical patient groups have suggested a direct link between dissociation and suicidal behaviour [6], [28], [29]. However, it is probable that earlier studies with small clinical or student groups have presented selection bias. The relationships between dissociation, depression, alexithymia, and suicidality have not yet been studied in a general population.
The development of reliable and valid dissociation scales, such as the Dissociative Experiences Scale (DES) and the Dissociation Questionnaire (DIS-Q) [3], [4], [30], [31], has made it possible to carry out studies on population samples. Earlier studies [31–33] have shown that dissociative experiences are quite common, and their prevalence has ranged from 1.0% to 12.8%, depending on the scale used or on the cutoff point selected to indicate a high level of dissociation. Recent studies [10], [17] have questioned the highest estimates of the prevalence of dissociative disorders in the general population. Instead of considering dissociation as a continuum from normal to pathological, a typological model has been developed [4], [17], [34]. A subscale derived from the DES, the Dissociative Experiences Scale-Taxon (DES-T), was developed to better distinguish between pathological dissociation, such as amnesia and depersonalization, and nonpathological dissociation, such as absorption. The prevalence of pathological dissociation (DES-T ≥ 20) has been found to be 3.3% [17] and 4.4% [10] in two North American population samples. Pathological dissociation assessed with the DES-T has been associated with male gender, ethnicity (African-American), and alcohol abuse [10]. However, a European study with a large selected sample found no differences between men and women in the total (DES) or pathological dissociation (DES-T) scores [35].
The purpose of our study was to assess the prevalence of pathological dissociation by DES-T in a general population, and to identify factors associated with it. We also studied the relationship between pathological dissociation, depression, alexithymia, and suicidality in a general population sample.
Subjects and methods
Subjects
The study was conducted in the district of Kuopio, which is located in the central-eastern part of Finland. Our population sample included 3004 subjects aged 25–64 years randomly selected from the National Population Register. Study questionnaires were mailed for the first time in April 1998, and again to the non-respondents in May 1998. A total of 2050 questionnaires were returned, giving a response rate of 68.2%. Due to incomplete data, 49 subjects were excluded from the analysis. The final sample (n = 2001) included 885 (44.2%) men and 1116 (55.8%) women. More men (n = 572, 39.3%) than women (n = 382, 25.5%) were non-responders (p < 0.001). The non-responding men were younger than the responding men (42.1 years vs. 44.8 years, p < 0.001), but no respective difference in age was found among women.
Methods
Dissociation
Dissociative symptoms were evaluated with the Finnish version of the Dissociative Experiences Scale (DES). The scale is a 28-item, selfreport instrument for the measurement of dissociative experiences; it has been found to have a test-retest reliability of 0.84 and to be highly reliable, internally consistent, and temporally stable [30]. Cronbach's alpha was 0.93 in our study. The scale takes approximately 10 minutes to complete and yields item, subscale, and total scores, which all range from 0 to 100. The individual's total score is the mean of the 28 items, and higher scores indicate greater levels of dissociation. The scale has been used earlier in population samples [32], [33], and has been shown to discriminate significantly between patients with dissociative disorders, other disorders and normal control subjects when a cutoff score of 30 is used [3], [4].
The DES has been divided in three factors or subscales [3], all measuring different aspects of dissociative experiences. The absorption and imaginative involvement factor (DES-ABS) has mostly been considered to reflect the non-pathological aspects of dissociation. The amnestic (DES-AMN) and depersonalization-derealization (DES-DD) factors have consisted more of questions measuring pathological dissociation.
A Dissociative Experiences Scale-Taxon (DES-T) with eight items from the DES has been developed to more clearly distinguish the pathological component of dissociation [17], [34]. This scale measures identity alteration, depersonalization, derealization, discontinuation of awareness, dissociative amnesia, and auditory hallucinations. According to previous research, a cutoff score of 20 in DES-T has been suggested to be optimal to discriminate subjects with dissociative disorders [8], [17]. A cutoff point of 20 on the DES-T in a general population sample has been shown to correctly identify 100% of taxon members and 97% of non-taxon members [17]. Therefore, we selected this cutoff point to divide our sample in high dissociators (DEST ≥ 20) and low dissociators (DES-T < 20). The other 20 items form the non-pathological component of the DES (DES-NP) [36].
Alexithymia
The prevalence of alexithymia was screened using the Finnish version [37] of the 20-item Toronto Alexithymia Scale (TAS-20) [38]. The total scores of the TAS-20 were categorized according to the recommendations of Taylor and coworkers [39]; thus a score ≥ 61 indicated alexithymia, and ≤ 51 no alexithymia. Subjects with a TAS-20 score between 51 and 61 were categorized as intermediate. In multivariate analysis the intermediate group was combined with the nonalexithymic group.
Depression
The level of depression was assessed using the 21-item Beck Depression Inventory (BDI) [40]. In bivariate analysis the scores were divided into four groups: 0–9 (normal mood); 10–18 (mild depression); 19–29 (moderate depression); and 30–63 (severe depression). The three groups with scores ranging from 10 to 63, indicating subjective symptoms of depression, were combined in multiple logistic regression analysis.
Suicidality
One of the BDI items (number nine) screens the severity of suicidal tendencies [41]. The responses ‘I have definite plans to commit suicide’, ‘I would kill myself if I had a chance’ and ‘I feel I would be better off dead’ indicate the presence of suicidal ideation, and subjects choosing those options were considered suicidal. The response ‘I have no thoughts of harming myself’ indicates the absence of suicidal ideation (non-suicidal).
Sociodemography
The subjects were questioned about their sociodemographic background (sex, age, marital status, and place of residence). In addition, a single question was asked to assess each of the following factors: years of education (≥ 9 years = high vs. < 9 years = low); subjective working ability (good vs reduced or unable to work = reduced); financial situation (good or fairly good = good vs. fairly poor or poor = poor); alcohol consumption (2–3 times/week or more = frequently vs. once a week or less = seldom); current smoking (yes vs. no).
Statistical analysis
Pearson's bivariate correlation analysis was used to measure the association between the selected items of the DES and between DES and DES-T scores. Relationships between the continuous variables were assessed with the Mann–Whitney U-test or by analysis of variance (ANOVA) when appropriate. Pearson's chi-squared test with continuity (Yates') correction was used to analyse the associations between pathological dissociation and class variables. Multiple logistic regression analysis was performed with four different models to study the independent associations of possible risk factors with pathological dissociation. Data processing was carried out with the SPSS 11.0 statistical software program. All tests were two-tailed.
Results
Scores of 20 or higher in the DES-T were recorded from 68 (3.4%) subjects, of whom 32 (3.6%) were men and 36 (3.2%) were women. The correlation between DES and DES-T scores was 0.89 (p < 0.001).
The mean total DES score for the entire sample was 8.0 (SD 8.1) (Table 1). The mean total DES score was lower in men than women (7.8 vs. 8.2, z = −2.1, p = 0.034), and it declined slightly but not significantly with age. The mean score of DES-AMN increased with age, and the mean score of DES-ABS declined significantly with age. When assessing men and women separately there was only one statistically significant trend with age in the mean scores of all variables: the mean score of DES-ABS declined with age in women. The mean score of DES-AMN (z = −2.3, p = 0.021) was higher in men compared with women, and the mean scores of DES-ABS (z = −2.3, p = 0.020) and DES-NP (z = −2.1, p = 0.037) were higher in women than men.
Means (SD) of the DES, the amnestic subscale (DES-AMN), the absorption and imaginative involvement subscale (DES-ABS), the depersonalization-derealization subscale (DES-DD), the pathological taxon (DES-T), and the non-pathological part (DES-NP) according to gender and age
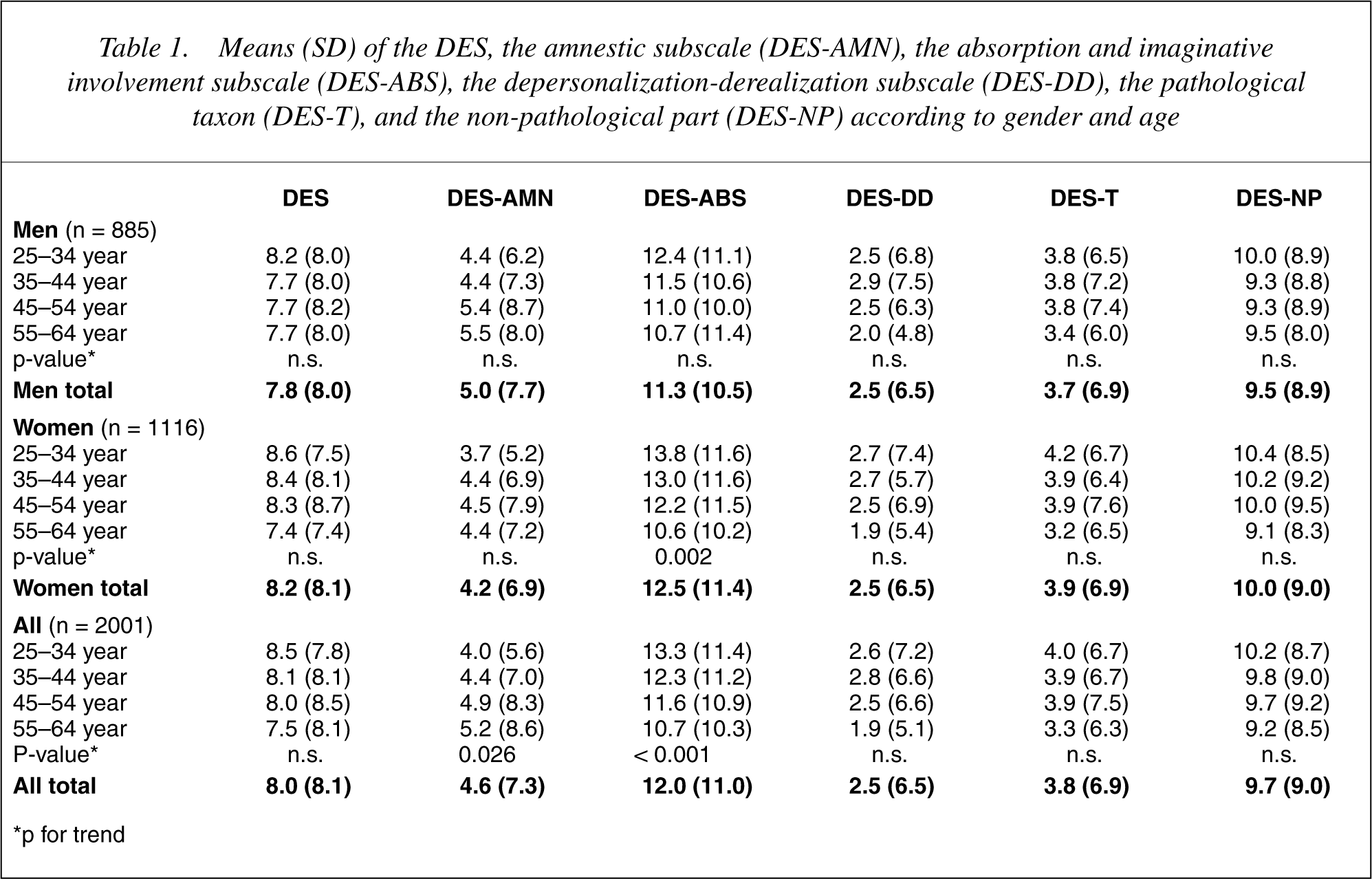
∗p for trend
The prevalence of high dissociators (DES-T ≥ 20) according to sociodemographic and psychiatric variables is presented in Table 2. Depressive symptoms, alexithymia, and suicidality had a strong association with pathological dissociation. Single, divorced or widowed male subjects were quite often high dissociators. A poor financial situation was associated with pathological dissociation, but it was statistically significant only in men. In subjects with a reduced working ability the prevalence of high dissociators was higher than in those with a good working ability in both genders. Frequent alcohol consumption was associated with pathological dissociation in women and current smoking in men. The place of residence and education had no association with pathological dissociation (data not shown).
Prevalence (%) of high dissociators (DES-T≥20) according to gender, background and clinical variables
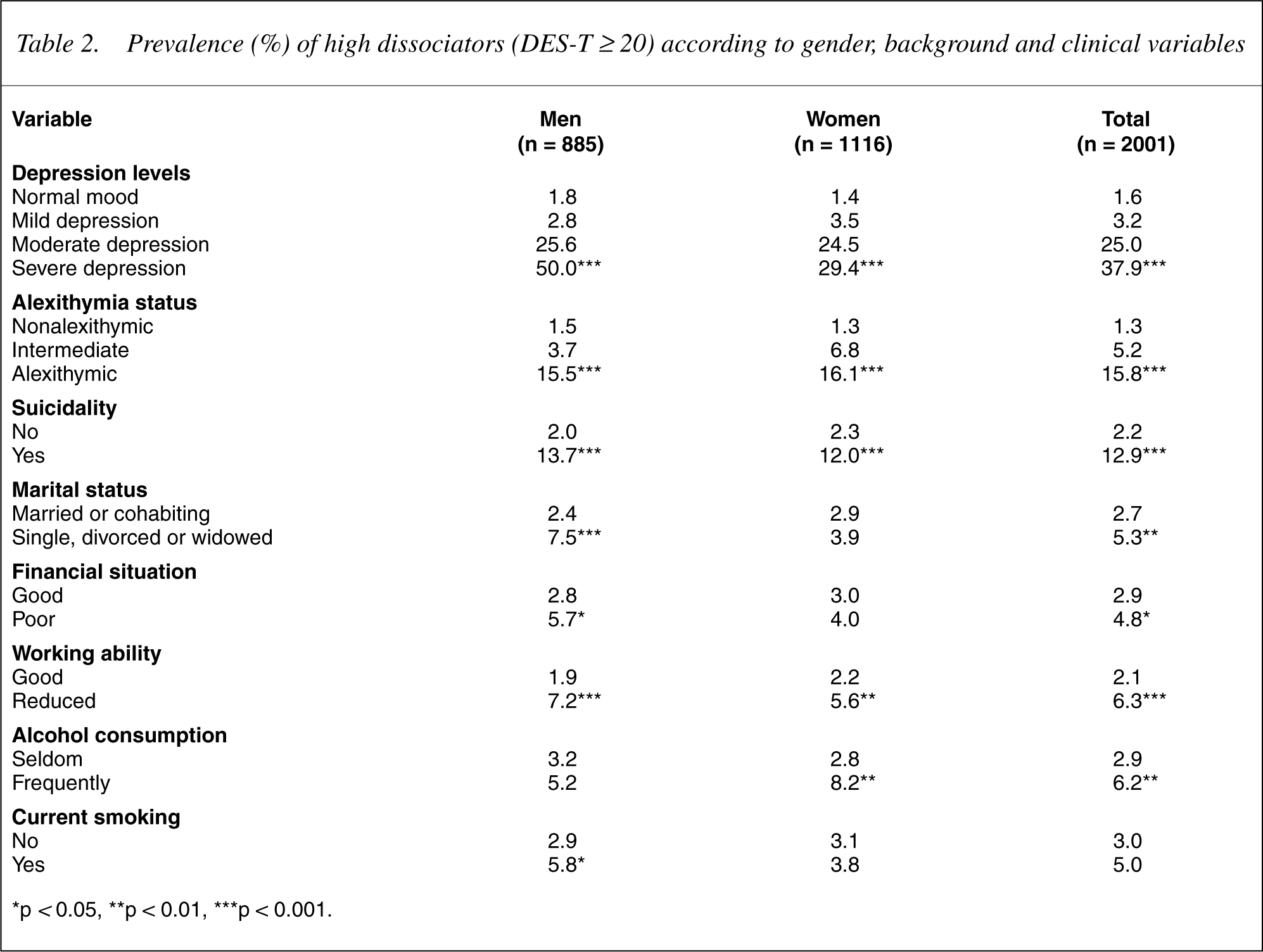
∗p <0.05, ∗∗p < 0.01, ∗∗∗p < 0.001.
Table 3 presents the results of the multiple logistic regression analysis performed on four models, each including one psychiatric symptom variable and the sociodemographic variables, and one model in which all three psychiatric symptom variables were included. In Model 1, pathological dissociation was significantly associated with depression. Subjects with depression had a nearly nine-fold greater risk of pathological dissociation compared with subjects with a normal mood. In Model 2, the likelihood of pathological dissociation was more than seven-fold greater in alexithymic subjects compared with subjects without alexithymia. In Model 3, the odds of pathological dissociation were over four-fold greater among suicidal subjects compared with non-suicidal subjects. In Model 4, all three psychiatric symptom variables were included in the same multiple logistic regression model to assess significant independent relationships with pathological dissociation. The odds ratios of pathological dissociation remained statistically significant in depressive (AOR 3.85 95% CI = 1.90), alexithymic (AOR 4.01 95% CI = 2.49), and suicidal (AOR 2.19 95% CI = 1.13), subjects. Frequent alcohol consumption had a significant association with pathological dissociation in all models.
Multiple logistic regression models of factors associated with pathological dissociation (DES-T ≥20)
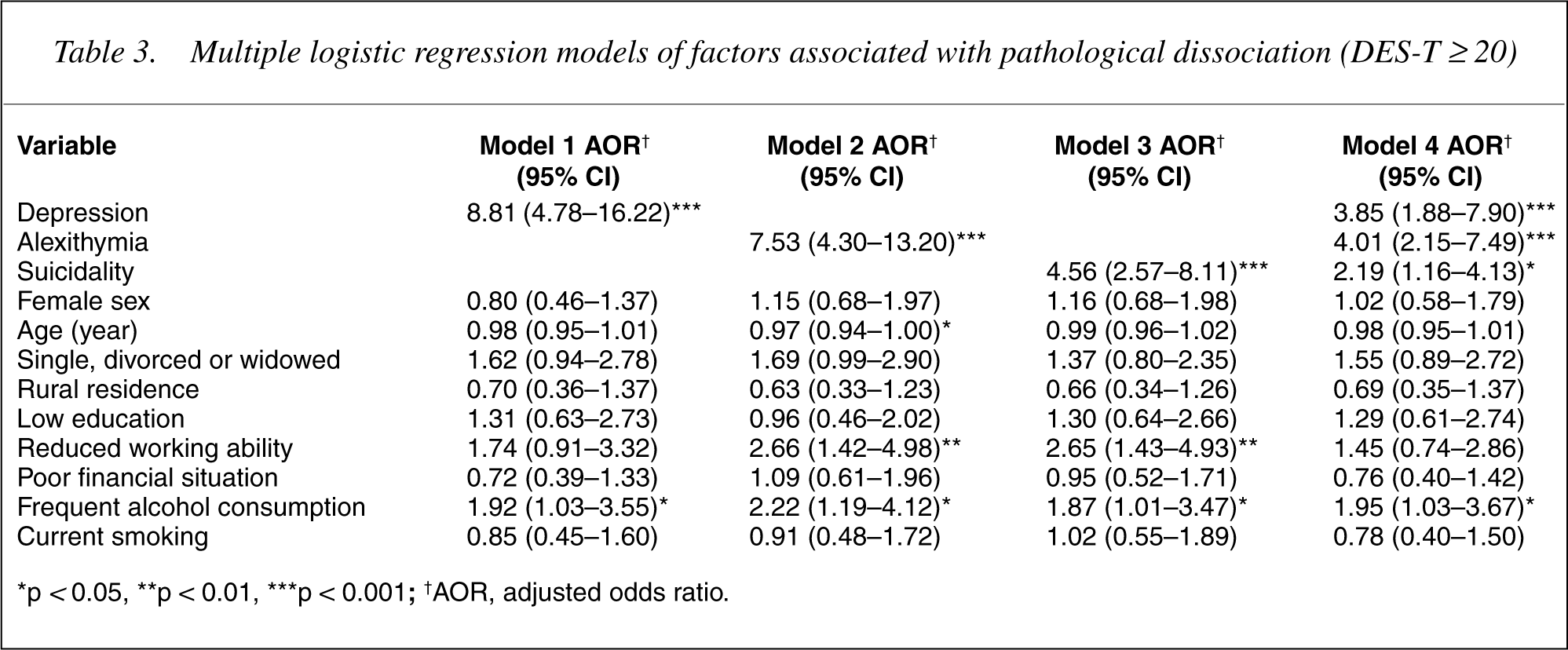
∗p <0.05, ∗∗p < 0.01, ∗∗∗p < 0.001; †AOR, adjusted odds ratio.
Discussion
Pathological dissociation was strongly associated with depression, alexithymia, and suicidality in our general population sample. There is evidence from earlier studies of the complex associations between dissociation, somatization and affect dysregulation in the adaptation to trauma [42]. Because trauma variables were not included, our study could not determine aetiology, but clearly demonstrated the comorbidity of pathological dissociation.
Recently, contradictory views concerning the associations between alexithymia and dissociation have been reported in different clinical [21], [24] and non-clinical [20], [22], [23] samples, but to our knowledge no results have been published on general populations. In one study with patients and non-clinical subjects [21], TAS total scores were significantly higher in a pathological dissociation group compared with participants without pathological dissociation. In our study, alexithymia had a statistically significant association with pathological dissociation even after adjusting for depression in logistic regression analysis.
Although the nature of the link between dissociation and alexithymia is not yet known, it has been suggested in earlier studies that the link could be the ability to cope with stressful events [20], [21], [23]. There is strong evidence [2], [11], [42], [43] that traumatic events contribute to the formation of dissociative experiences, as dissociation separates overwhelming mental events from consciousness. Alexithymia may also be viewed as a defense against such affects. In this context, alexithymia is termed secondary alexithymia to differentiate the construct from primary alexithymia, which has been assumed to be genetic or biological in origin [44]. However, it is not possible to determine the relationship between alexithymia and pathological dissociation further due to the cross-sectional design of our study.
A clear association between dissociation and mood disorders has been found in one study at the population level [11]. A recent study with depersonalization disorder cases found considerable comorbidity between depersonalization disorder and depression [16]. Furthermore, in a study with chronic pelvic pain patients, dissociative disorders were best predicted by self-reported anxiety and depression, and the DES [12]. We found a strong relationship between pathological dissociation and current depressive mood, and the prevalence of high dissociators increased linearly with increasing BDI scores, supporting the earlier findings that dissociative pathology is linked with substantial comorbidity [11], [12], [16]. The DES has been conceptualized a trait measure [3], and DES-T distinguishes subjects with chronic pathological dissociative states that can be permanent without treatment [34]. Therefore, it is more probable that a tendency for chronic dissociation increases a person's risk for developing future depressive symptoms rather than that current depression temporarily increases the subject's dissociative symptoms.
Dissociation has been associated with self-mutilation or self-harming behaviour in a number of heterogenous patient studies [6], [26], [28], [29], and these have suggested a direct link between dissociation and self-mutilation even after adjusting for other coexisting variables such as depression. In a large sample of high-school students, dissociation associated with suicide attempts and selfmutilation [27]. Suicidality is closely associated with affective disorders, but in our study it proved to be independently associated with pathological dissociation after adjusting for several important covariates. It is important to note that we have now also found the relationship to be significant in the general population.
Frequent alcohol consumption also had a significant association with pathological dissociation in our sample. In two earlier community studies, high dissociation [11] or pathological dissociation [10] has been associated with a substance use disorder. In a small sample of women with eating disorders, alcohol abuse was clearly linked to DES-taxon scores [8]. In Finland it is common to consume large amounts of alcohol at one time, and subjects using alcohol frequently also very probably have high levels of consumption. A limitation is that we did not ask about the volume of alcohol consumed. In addition, frequent alcohol consumption was more common among men than women in our study, but the bivariate association between pathological dissociation and frequent alcohol consumption was significant in women and the total sample. This association between pathological dissociation and frequent alcohol use might represent an attempt at self-medication to relieve the distress associated with the symptoms of dissociation.
There have been no published studies on the prevalence of pathological dissociation (DES-T) in European population samples, but total dissociation (DES) scores have tended to be lower in Europe compared with North America [15]. According to our results, the prevalence of pathological dissociation in Finland was at the same level as in previous North American population studies [10], [17]. While the total DES score was higher in women than men in our study, gender did not affect the DES-T scores. In addition, there were no statistically significant associations between age and the DES or DES-T scores. These results differ from a previous community study, where men had higher scores in DES-T compared with women, and the scores declined with age [10]. The age range in our study did not include subjects from 18–25 years of age, and this might influence the detected prevalence and associations with age, as younger subjects have scored significantly higher in the DES [10], [33]. In addition, the differences between Europe and North America are possibly due to cultural factors. Young men were the least likely to respond to our questionnaire, and this might also influence the results for the prevalence of dissociation and the DES and DES-T scores.
Our results with the DES subscales were similar to a recent study with a large, selected German sample [35]: men scored higher in the amnesia subscale compared with women, and there was no gender difference in the DES-T scores. The gender difference in the amnesia subscale was also found in a Dutch population sample [31]. As dissociative amnesia represents a diagnostic criterion for post-traumatic stress disorder (PTSD), it may be that men and women react differently to traumatizing events, and there may be gender differences in the storage, consolidation and retrieval of traumatic memories [35]. The total DES score, the scores for the absorption and imaginative involvement factor, and the nonpathological part of the DES were higher in women than men in our study. Our results suggest that the pathological aspects of dissociative experiences are equally common in both genders, but the non-pathological dissociative symptoms are more prevalent among women.
Our study was cross-sectional and had some limitations. Although it revealed strong associations between several psychiatric variables, the causal relationships could not be determined. The assessment of suicidality and alcohol consumption was performed with only one question instead of a validated scale, and the results should therefore be considered with caution. In addition, the self-administered questionnaire may cause difficulties in understanding and completing the Dissociative Experiences Scale.
Our sample size was by far the largest to date as a population sample, and the response rate was satisfactory compared with previous studies [10], [33]. We consider our results to give a reliable estimate of the prevalence of pathological dissociation in a Finnish population, which appeared to be almost identical to the Canadian sample [17].
Conclusions
Statistically significant associations were found between pathological dissociation, current depressive mood, alexithymia and suicidality in the general population. All population studies of dissociation and its associates have been carried out in cross-sectional study designs. Prospective studies are needed to provide further insight and a deeper understanding of the aetiology of dissociation.