
Abstract
Suicidal ideation is a necessary but not sufficient precursor for attempted suicide and suicide. While suicide, and to a lesser extent attempted suicide, is generally accepted to be associated with psychiatric illness, particularly depression [1,2], as well as with external psychosocial and traumatic events, the importance of suicidal ideation is sometimes minimised when considering whether or not it may be an indicator of psychiatric illness. Although an association between suicidal ideation and such illness has been demonstrated, usually this has been in clinical samples. Indeed, to the best of our knowledge the risk attributable to psychiatric illness and the psychosocial and traumatic events for suicidal ideation has not yet been examined in a general population sample.
This lack of examination is an important issue for public health, because the risk factors for suicide lack specificity and are notoriously unreliable in the prediction of individual suicide [3,4]. It may be more beneficial to utilise risk factors for suicide or suicidal ideation within population-based approaches, rather than to attempt to predict individual suicide risk. Therefore, every effort should be made to clarify those factors which may contribute to suicidal ideation in the general population in order that informed decisions can be made about public health intervention programs.
The present study was part of a broader examination of the mental health status of a random and representative sample of the South Australian population [5]. It involved the administration of two measures of general mental health, one of which can be used to assess suicidal ideation. In addition, demographic data and information about traumatic events were collated. This allowed the calculation of relative and attributable risk of suicidal ideation for a range of variables.
Method
Data for this study were collected using a computer-assisted telephone interviewing (CATI) system. It is known that 97% of households in South Australia have a telephone connection [6]. Households in South Australia were selected at random from the electronic White Pages. A letter introducing the health survey was sent to the household of each selected telephone number, with the information that the survey would be conducted by telephone within the next 8 weeks. Within each household an adult (18+ years) was selected at random on the basis of the last person to have had a birthday. Up to five call backs were made to interview the selected respondents and no replacements were made for those who were unobtainable. Interviews were conducted in English, Italian, Greek and Vietnamese.
The CATI interview allows immediate entry of data from the questionnnaire screen to the computer database. There were nine interviewers, and 5% of their subjects were selected at random for validation by a supervisor. All interviewers adhered to quality control requirements after rigorous training. The CATI also has a range of checks on each response and automatically rotates response categories in order to minimise bias.
Data were weighted by age, sex, geographic region and on the probability of selection in the household, to provide estimates for the South Australian population. The population profile for weighting was obtained from the Australian Bureau of Statistics 1995 Estimated Resident Population [7].
Instruments
The measures of mental health were the 28-item general health questionnaire (GHQ) [8] and the quality-of-life instrument, the 12-item short-form health survey (SF-12) [9,10], which comprises a subset of questions of the SF-36. The GHQ-28 and the SF-36 have been validated for Australian populations [11–13]. The SF-12 has a mental component summary cut-off score delineating ‘clinical depression’ [10,14]. None of the SF-12 items refer to suicidal ideation.
There was no specific emphasis on enquiry about suicidal ideation in the survey, and it was assessed on the basis of responses to four questions contained in the 28-item GHQ, as described previously [15,16]. These questions were: ‘Have you recently felt that life is not worth living?’; ‘Have you recently found yourself wishing you were dead and away from it all?’; ‘Have you recently had thoughts of the possibility that you might do away with yourself?’; and ‘Have you recently found the idea of taking your own life kept coming into your mind?’.
The binary method of scoring the GHQ was utilised, with the negative responses ‘not at all’ and ‘no more than usual’; and ‘definitely not’ and ‘I don't think so' given a score of 0, and the positive responses of ‘rather more than usual’ and ‘much more than usual’ or ‘has crossed my mind’ and ‘definitely has’ were given a score of 1. A positive response to any of the four questions was considered indicative of suicidal ideation.
Social and demographic data included gender, age, level of income, work status, use of alcohol and smoking status. Recorded psychosocial events that had occurred in the last 12 months included unplanned loss of a job; a new job; family or domestic violence; the death of someone close; discrimination by others; moving home; home being robbed or burgled; relationship breakdown; and serious injury or illness.
Information about specific traumatic events that had occurred throughout the individual's life included the experience of direct combat in war; being in a life-threatening accident; being involved in a fire, flood or other natural disaster; witnessing somebody being badly injured or killed; being raped; being sexually molested; being seriously physically attacked or assaulted; being threatened with a weapon, held captive or kidnapped; and being tortured or the victim of terrorists.
Data analyses
The association between suicidal ideation and factors such as the presence of clinical depression as delineated by the SF-12 and other specific psychosocial stressors was estimated by calculating the relative risk that an individual factor would contribute to suicidal ideation relative to a baseline or control condition [17,18].
While the relative risk of suicidal ideation is of interest, of more specific value is the population-attributable risk [19], which has also been referred to as the population-attributable risk per cent [20], the attributable fraction [21] and the aetiologic fraction [22]. The underlying assumptions for the validity of the statistic are that there is a causal relation between the risk factor and disease; that those previously exposed would have the unexposed risk of the disease if the risk factor was eliminated; and that the risk factors are independent of each other. The population-attributable risk provides a measure of the proportion of a disease which can be associated with exposure to a risk factor or the proportion of that disease which would be eliminated in the exposed risk factor group if the incidence of the disease was reduced to the unexposed risk factor level [23,24]. Population-attributable risk is usually expressed as a percentage and, in comparison with the relative risk or odds ratio, it takes into account the total population who were exposed to the risk factor. Although it appears paradoxical, the summation of the percentages is usually appreciably more than 100% because risk factors are not mutually exclusive.
The formula used to calculate the population-attributable risk is:
where RR is the relative risk of acquiring the disease and P(E/D) is the probability (exposure/disease) or the proportion of those exposed to that risk factor who develop the disease [19,25].
Univariate analyses, using Cox regression methods [26], was used to assess the relationship of demographic and health indicator variables to suicidal ideation. Variables that were significant at the 0.25 univariate level were entered into multivariate Cox regression analyses to examine which variables best jointly predicted suicidal ideation [27]. Nonsignificant variables [p > 0.05] were subsequently omitted in the modelling process until a satisfactory model was obtained.
Principal component analysis was used to test for multi-colinearity. Significant variables at the univariate stage were entered into a factor analysis to determine the eigenvalues. Multi-colinearity was deemed to be not present if the largest eigenvalue divided by the lowest eigenvalue did not exceed the value of 20 [28]. Tests for confounders and likely interaction combinations were assessed on the final mutivariate model.
Univariate and multivariate data analyses were performed using SPSS Version 8.0 (SPSS Inc., Chicago, IL, USA) and STATA 5.0 (STATA, College Station, TX, USA), respectively.
Results
The initial eligible sample consisted of 3384 subjects, and 2501 participated in the survey, representing a 74% response rate. There were 395 (11.7%) refusals; 356 (10.5%) could not be contacted after five attempts; 53 (1.6%) were unable to speak English, Italian, Greek or Vietnamese; 64 (1.9%) were incapacitated and unable to be interviewed; and 12 (0.4%) terminated the interview before the completion of data gathering.
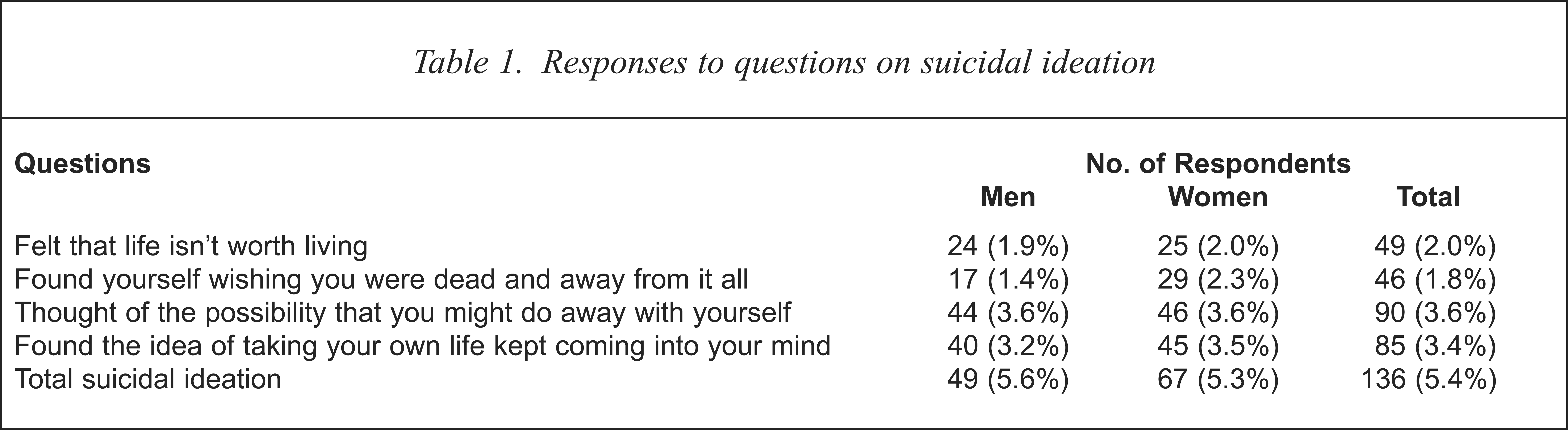
The responses to the individual questions related to suicidal ideation are presented in Table 1. Overall 5.4% (95% CI: 4.6–6.2%) of subjects (5.6% of men and 5.3% of women) scored at least one response indicative of suicidal ideation.
Responses to questions on suicidal ideation
The univariate associations between demographic, psychosocial and health risk indicators and suicidal ideation are presented in Table 2. There were a number of significant associations among these. Unemployment and having an income of less than $A40 000 per year; using alcohol at a level considered to be high risk; having SF-12 delineated clinical depression; having experienced a psychosocial event in the last 12 months; and being exposed to one or more traumatic events were significantly associated with suicidal ideation. Being between 35 and 54 years of age approached statistical significance.
Univariate associations between suicidal ideation and demographic, psychosocial and health risk indicators
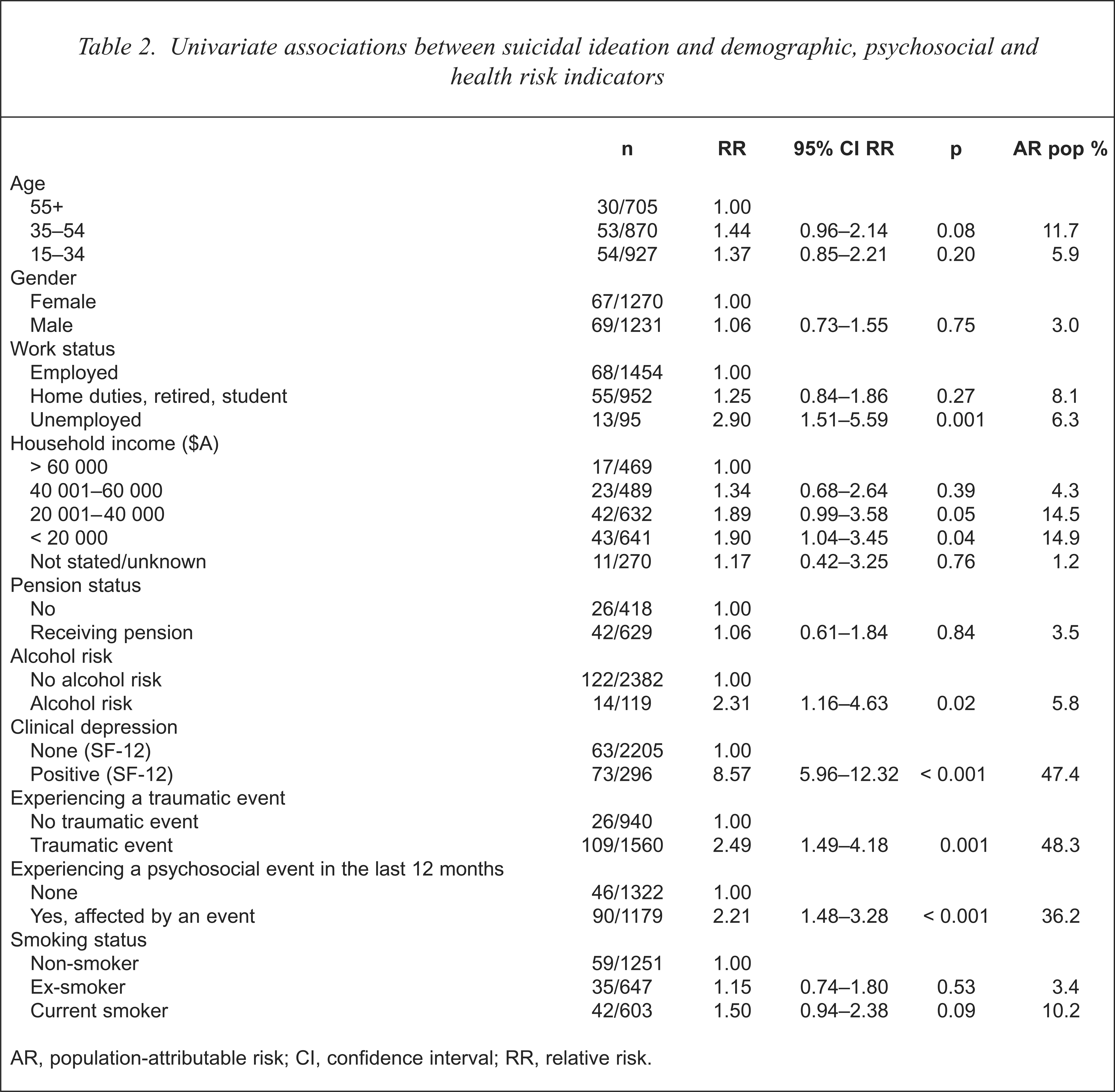
AR, population-attributable risk; CI, confidence interval; RR, relative risk.
The univariate associations between individual psychosocial events and suicidal ideation are presented in Table 3. Most attained statistical significance, including unplanned loss of a job; family or domestic violence; death of somebody close; discrimination; moving house; being robbed or burgled; having a marriage/relationship breakdown; and sustaining a serious illness or injury.
Univariate associations between suicidal ideation and specific psychosocial events
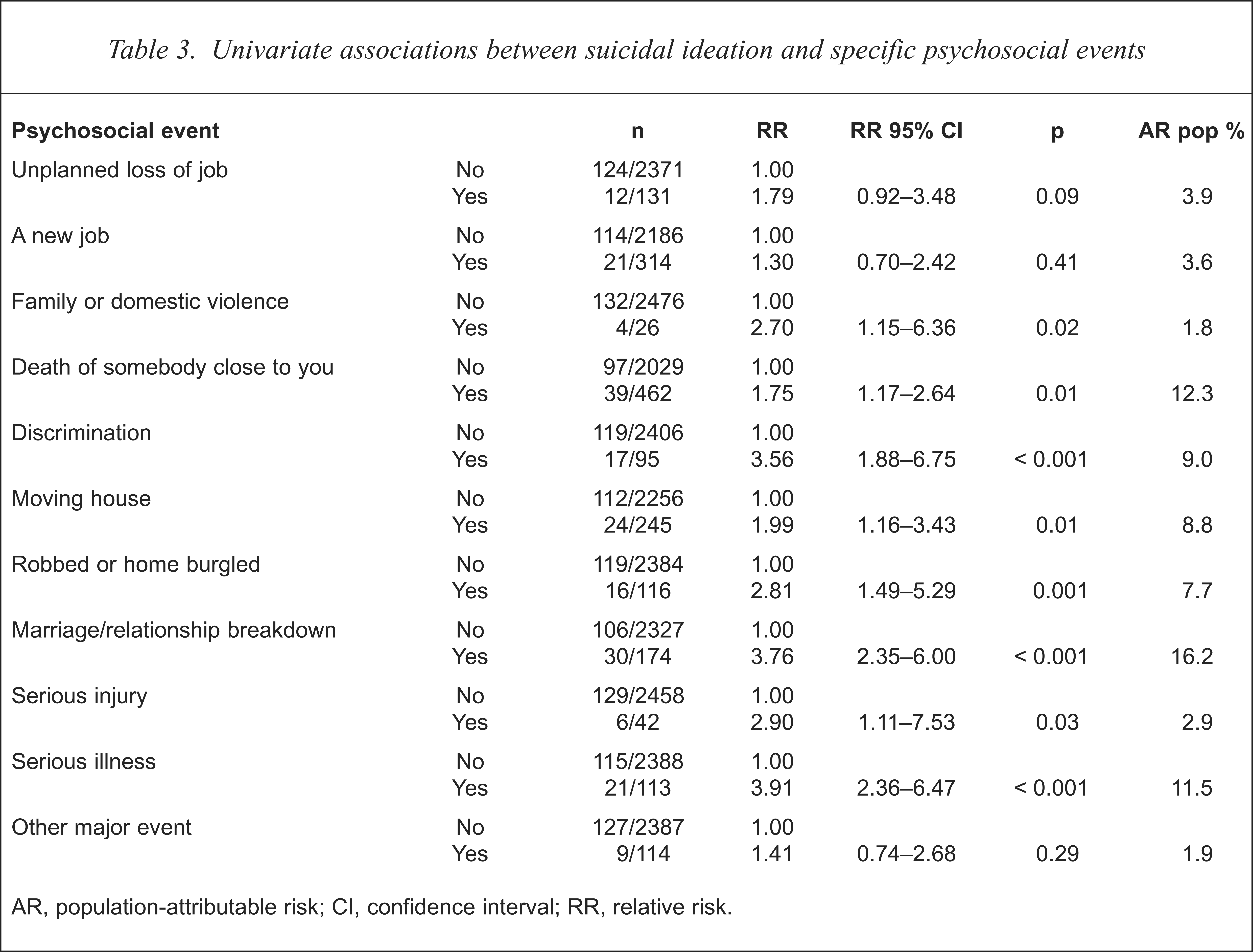
AR, population-attributable risk; CI, confidence interval; RR, relative risk.
The univariate associations between individual traumatic events and suicidal ideation are presented in Table 4. Apart from having direct combat experience and being involved in a fire, flood or other natural disaster, each of the other traumatic events attained statistical significance, including involvement in a life-threatening accident; witnessing somebody being badly injured or killed; being raped or sexually molested; being seriously physically attacked or assaulted; being threatened with a weapon, held captive or kidnapped; or being tortured or the victim of terrorists.
Univariate associations between suicidal ideation and specific traumatic events
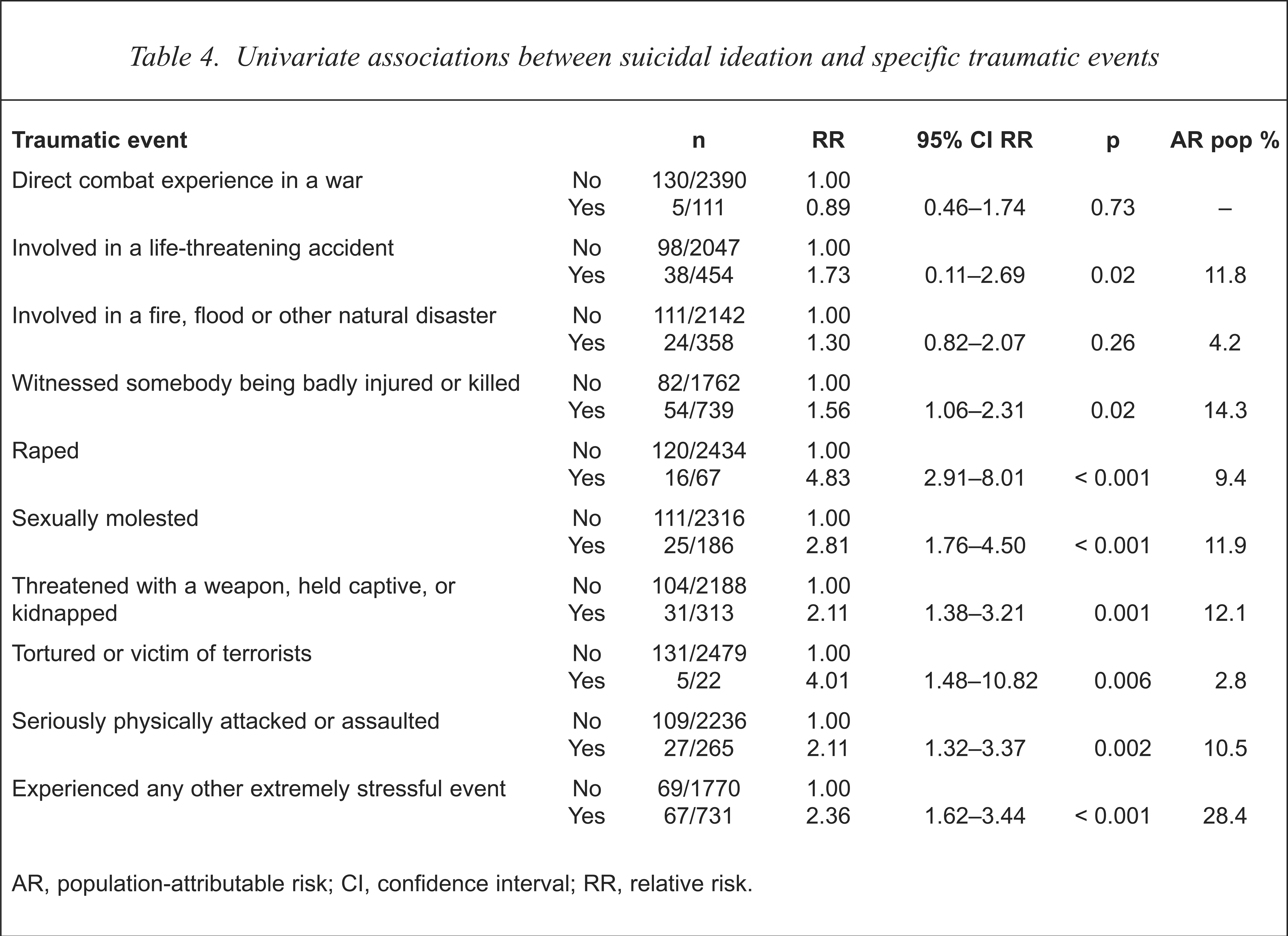
AR, population-attributable risk; CI, confidence interval; RR, relative risk.
The multivariate associations between variables of interest and the extent to which they contribute to suicidal ideation are presented in Table 5. To optimise power in the multivariate analyses the psychosocial and traumatic events variables were collapsed and recoded according to whether or not there had been exposure to one or more psychosocial or traumatic events. No interactions or confounders were detected.
Multivariate association between suicidal ideation and variables of interest
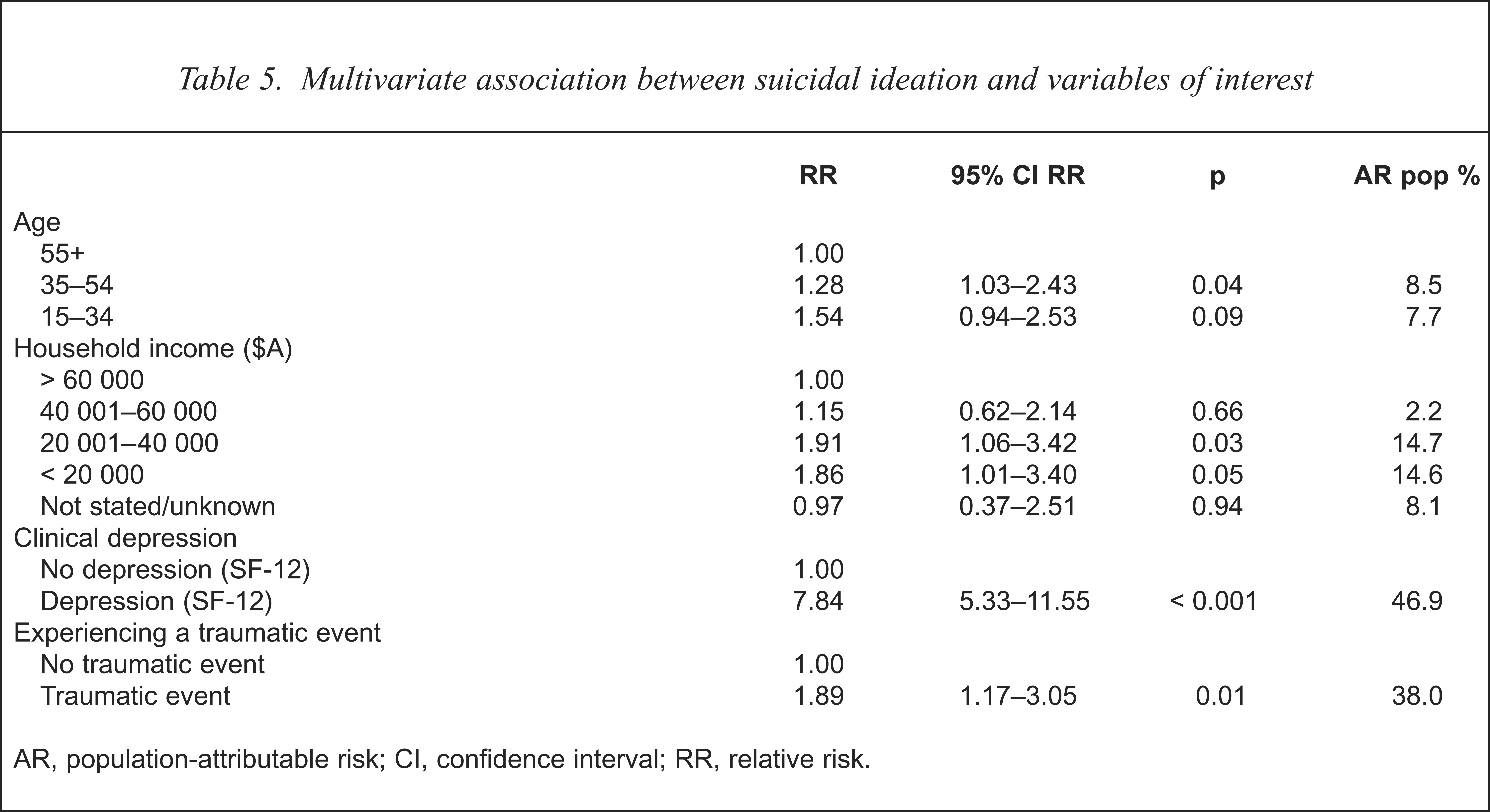
AR, population-attributable risk; CI, confidence interval; RR, relative risk.
The attributable risk analyses showed that 46.9% of suicidal ideation in a random community sample was attributed to SF-12 delineated clinical depression (p < 0.001); 38.0% to experiencing a combination of traumatic events (p < 0.01); 14.7% and 14.6% to having an income in the range $A 20 001 to $A 40 000 and less than $A 20 000 respectively (p < 0.05); and 8.5% to being in the 35–54 years of age group (p < 0.05). The risk attributable to the youngest age group (15–34) approached significance.
The risk attributable to having had exposure to one or more specific psychosocial events did not attain statistical significance in the multivariate analysis, with the relative risk falling to 1.45 compared to 2.21 for the univariate analysis (see Table 2).
Discussion
This study reports the first analysis of population-attributable risk of suicidal ideation in a random and representative population survey. The results demonstrate the importance both of clinical depression and of significant traumatic events in association with suicidal ideation, with multivariate analyses delineating 46.9% population-attributable risk to clinical depression and 38.0% to the experiencing of one or more traumatic events.
Together, these variables represent an important target for the reduction of suicidal ideation, if appropriate and effective interventions can be developed.
The significance of individual psychosocial and traumatic events could not be subjected to multivariate analyses because of the small number of people in the community experiencing suicidal ideation and a specific traumatic event. However, the univariate analyses indicated the importance of several recent psychosocial events, with marriage or relationship breakdown, death of someone close and serious illness having 16.2%, 12.3% and 11.5% population-attributable risk, respectively. Similarly, for specific lifetime traumatic events, there was a 14.3%, 11.9% and 9.4% population-attributable risk, respectively, for witnessing somebody being badly injured or killed, being sexually molested, or being raped. These findings in relation to the traumatic events are not unexpected and are consistent with the increased relative risk for suicidal behaviour of those with post-traumatic stress disorders reported in a subset of the Epidemiological Catchment Area (ECA) study [29].
Clearly, specific psychosocial and traumatic events are of importance to each individual. However, when multivariate analyses were undertaken, which allow for the joint effects of different variables, even the summation of all the psychosocial events no longer remained statistically significantly associated with suicidal ideation, whereas the summation of traumatic events did. This was the case even though the psychosocial events had occurred in the last 12 months whereas the traumatic events occurred at any time in the individual's life. Nevertheless, the population–attributable risk for the summation of traumatic events fell from 48.3% for the univariate analysis to 38.0% for the multivariate analysis, appreciably less than the 46.9% for clinical depression, which remained virtually unchanged from the 47.4% for univariate analysis. This suggests that although it is important to the individual to prevent or minimise the impact of specific psychosocial and traumatic events, for public health, a focus on the prevention, detection and treatment of clinical depression may have a more productive influence on suicidal ideation, and as a result reduce suicide and attempted suicide.
To some these results may be unexpected, as suicidal ideation is sometimes considered to be a readily understandable reaction to stressors or an existential questioning of the meaning of life. However, these findings, in a random community sample of 2501 subjects, emphasise the importance of clinical depression as the most significant single contributing factor to suicidal ideation. Indeed, the findings are consistent with the Swedish clinical work of Skoog et al. [30] who, in a study focusing on elderly people, noted that it was ‘commonly believed that the feeling that life is not worth living or the wish to die is normal in old people’, but found that such feelings were ‘most often associated with a mental disorder’, usually depression.
The use of population-attributable risk analyses appears to have been overlooked in studies on suicidal behaviour until very recently [2,31,32]. In a case–control study of serious suicide attempts, Beautrais et al. [2] reported varying degrees of population-attributable risk for serious suicide attempts depending on age and sex, with men under 30 years and women over 30 years having population-attributable risks indicating that elimination of mood disorders would reduce serious suicide attempts by up to 64% and 80%, respectively.
Beautrais [32] has also recently re-analysed published data from a series of other studies of suicide by Shaffer et al. [33] and Gould et al. [34,35] and also by Brent et al. [36–40], where odds ratios were reported and sufficient information about confounding variables was provided to allow the population-attributable risk to be calculated. Beautrais found that ‘mood (affective) disorders’, which for purposes of comparison are synonymous with the delineation of ‘clinical depression’ in the present study, had population-attributable risk for suicide of 45.7% in the studies of Shaffer et al. [33] and Gould et al. [34,35] and it was 36.8% in the Brent et al. studies [36–40].
It is striking that these figures, although for those who have made suicide attempts and those who have died by suicide, are of the same order as the present study, in which 46.9% of suicidal ideation was associated with clinical depression. Such results counter the popular view that suicide attempts and suicidal ideation occur in ‘normal’ people confronted with life stressors, and highlight the fact that clinical depression per se has to be considered seriously in its own right or in association with other events.
It is pertinent to reflect that in the context of attempted suicide, Beautrais [31] stated that ‘attempts to de-stigmatise suicide by suggesting that everyone is equally vulnerable to suicide when under stress misrepresents the important role of mental disorders in suicidal behaviours’, with the result that potentially treatable illnesses such as depression would not be detected. We submit that the same applies to suicidal ideation. Indeed, just as Shaffer et al. [41] noted that suicidal behaviour would be less imitated if it was depicted as ‘a deviant act by someone with mental illness’, our results suggest that it would be less likely that the importance of suicidal ideation would be minimised if the attributable risk of clinical depression to suicidal ideation was better understood.
There are potential limitations to the interpretation of these data. Data gathering by telephone interview could be criticised, but its validity has been demonstrated with face-to-face interviews [6,13]. In addition, there was a good response rate of 74%, with 11.7% refusals and a number of others precluded for reasons such as the inability to speak one of the four languages used in the survey. The use of the SF-12 to delineate clinical depression could also be queried, as it is not as well recognised as more established instruments. However, it has been validated in previous studies [9,10] and it has the advantage of brevity.
It is of note that the delineation of suicidal ideation in 5.4% of subjects in this study is lower than in some other reports [42,43]. However, we have no reason to doubt that a positive response to any of the four questions related to suicidal ideation in the GHQ would provide a valid indication of the presence of suicidal ideation. Furthermore, each of the questions appears to have face validity, and the questions are similar to those in other instruments that have been used. It is also reassuring that the results are consistent with previous studies that have examined suicidal ideation in representative community populations [44,45], rather than in specific opportunistic groups, such as high school or college students [43], which are generally unrepresentative of the population.
Limitations in the use of the population-attributable risk statistic should also be acknowledged [46,47]. The attributable risk calculated for depression does not take account of the existence of co-morbid psychiatric conditions such as posttraumatic stress disorder, which could be mediating factors for the significant population-attributable risk of traumatic events to suicidal ideation. This further emphasises the need to determine the presence of psychiatric illness when assessing those with suicidal ideation.
Within these constraints we consider the present results from a random and representative non-clinical population to be of importance. They re-affirm the significant contribution of specific traumatic events and also indicate, unequivocally, the magnitude of the contribution of clinical depression to suicidal ideation, with the population-attributable risk of depression indicating that elimination of mood disorders would reduce suicidal ideation by up to 46.9%. From the public health point of view it has been stated that ‘attributable risks guide policy makers when it is time to take action’ [46]. The focus of that action now appears to be more clearly defined.