
Abstract
Introduction
There is robust evidence that suicide risk is significantly greater in populations with schizophrenia than in the general population (Harris and Barraclough, 1997; Inskip et al., 1998). It is estimated that 10% of patients with schizophrenia will suicide (Harris and Barraclough, 1997; Siris, 2001), with risk of suicide completion 40 times higher than in the general population (De Hert and Peuskens, 2000). Australian data support this pattern (Access Economics, 2002). Many factors have been suggested as risk factors for suicide, most of which are shared between the general population and populations with schizophrenia (Hawton et al., 2005), although some suicide risk factors are schizophrenia-specific (Siris, 2001).
Broadly, suicide risk factors in schizophrenia segregate into four categories: (i) socio-demographic factors such as male gender, being divorced, or being unemployed; (ii) personal, social and family history factors such as living alone and recent loss events; (iii) characteristics of schizophrenia such as command hallucinations and agitation; and (iv) comorbid disorders and behavioural factors such as previous suicide attempts, depression, alcohol abuse/dependence, and drug abuse/dependence (Hawton et al., 2005). Other factors, such as marriage, are generally reported as protective against suicide (Kposowa, 2000; Luoma and Pearson, 2002).
Drug use disorders have been widely implicated in suicide (Hawton et al., 2005). However, studies examining the relationship between alcohol and suicide have reported mixed results; alcohol has been proposed as a major risk factor for suicide in the general population (Allebeck et al., 1987; Rossow, 2005), but has not been consistently reported as a risk factor for suicide in schizophrenia (Allebeck et al., 1987; Hawton et al., 2005).
Most studies examining alcohol and suicidal behaviour report data on completed suicides, although studies examining the relative risk of attempted suicide in those with alcohol use disorders have been undertaken (Bolton and Robinson, 2010; Borges et al., 2000; Fergusson et al., 2000; Nock et al., 2009). In the general population, evidence for an association between substance use, suicide attempts and suicide completion shows mixed results. While multiple studies have reported that suicide attempters with general drug use disorders are more likely to subsequently complete suicide, other studies report that suicide attempters with alcohol use disorders are less likely to subsequently complete suicide (for details see Rossow, 2005). Furthermore, a robust, stronger association between alcohol abuse and attempted suicide has been reported than between alcohol abuse and completed suicide (Rossow et al., 1999).
The literature specifically examining potential association of alcohol and drug use disorders with suicide attempts in schizophrenia is sparse and reports mixed results. A recent Turkish study (n = 300) reported a higher rate of alcohol abuse/dependence in suicide attempters than non-attempters with schizophrenia, and higher rates of lifetime major depressive episodes (Uzun et al., 2009). Previous studies examining schizophrenia/schizoaffective disorder have variously reported: a weak relationship between alcohol use disorders and suicide attempts, with depression explaining a far greater proportion of variance in suicide attempts than alcohol (Bartels et al., 1992); no difference in substance abuse rates between those with suicide attempts and those with no attempts (Gupta et al., 1998; Harkavy-Friedman et al., 1999); and increased suicidal ideation in current substance misusers compared to past and non-substance misusers, with no differences in depression (Kamali et al., 2000).
Given the complexity and lack of consensus regarding the associations between substance misuse variables and suicide attempts in schizophrenia, this question warrants further investigation. The genetics research group at the Queensland Centre for Mental Health Research (QCMHR) recruited Australian individuals (n = 821) with schizophrenia and related disorders for genetic analyses. We studied the demographic and clinical characteristics of this sample, specifically examining associations between substance misuse variables and suicide attempts.
Materials and methods
Sample recruitment
The sample was recruited during two related collaborative US/Australian studies examining genes and schizophrenia, collectively termed the Molecular Genetics of Schizophrenia study. The first study examined affected sibling pairs for a linkage analysis (for details see Suarez et al., 2006), including families with a proband with schizophrenia, plus one or more siblings with schizophrenia or schizoaffective disorder, and their parents if available. The second study examined unrelated individuals (singletons) with schizophrenia or schizoaffective disorder for a genome-wide association study (for details see Shi et al., 2009). Eligible families and individuals were recruited from a range of sources, including local treatment facilities, physician referrals, community organisations, supported accommodation facilities and advertisements. For the purposes of this study, only the Australian participants were included. Most participants were recruited in South East Queensland (78%), although participants were also recruited from Melbourne (11%), Adelaide (6%), Sydney and surrounds (4%), Tasmania (< 1%) and North Queensland (< 1%). The total sample comprised 821 affected individuals, 654 of whom were unrelated singletons and 167 of whom were first-degree related individuals contained within 79 independent families.
All participants gave written informed consent and consented to an interview, a blood sample for DNA, and review of their psychiatric records. Local Institutional Review Board approval was obtained for both studies.
Inclusion/exclusion criteria
We included all probands and their first-degree relatives who had a Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) (APA, 1994) diagnosis of schizophrenia or schizoaffective disorder. To standardise schizoaffective diagnoses, we operationalised the mood syndrome duration criterion at ≥ 30% of total illness duration, consistent with other major genetic studies (for details see Suarez et al., 2006).
Exclusion criteria for individuals were: (i) inability to give informed consent to all aspects of the study; (ii) psychosis judged to be secondary to substance use or a known neurological disorder such as epilepsy; (iii) severe intellectual disability (any impairment that precluded informed consent, and any individual with an IQ assessed below 55 according to formal testing/medical record evidence); and (iv) aged under 18 years.
Clinical ascertainment
The following routine sources of information were obtained
Diagnostic Interview for Genetic Studies (DIGS)
Trained clinicians (psychiatrists, psychologists, clinically trained scientists, social workers) used the semi-structured DIGS (Nurnberger et al., 1994) to obtain information relevant to the diagnosis of psychotic, mood and substance-use disorders in accordance with DSM-IV criteria (APA, 1994), the comorbidity of these disorders, proband medical history, and ratings of the positive and negative symptoms of schizophrenia.
Family Interview for Genetic Studies (FIGS)
A family informant (when possible) or the proband was interviewed about the family psychiatric history using the FIGS (Gershon et al., 1988; Maxwell, 1992). The DIGS and FIGS were developed by the National Institute for Mental Health in the USA specifically for use in genetic studies (Calkins et al., 2007), and have been used regularly in major international schizophrenia studies (Calkins et al., 2007; Shi et al., 2009; Suarez et al., 2006).
Medical records assessment
All available medical records were retrieved for each participant and then assessed by trained clinicians.
Narrative summary
A trained clinician, usually the interviewer who conducted the DIGS, prepared a case summary based on all information obtained from the DIGS, FIGS and medical records assessment.
Best Estimate Final Diagnosis (BEFD)
DIGS interview, interviewer narrative, available medical records and FIGS reports formed the basis for diagnostic review. Diagnoses were assigned using the BEFD procedure (Leckman et al., 1982), with two experienced psychiatrists independently reviewing all available information and formulating diagnoses, then conferring to assign a consensus diagnosis. Outstanding questions were resolved through discussion and sometimes involved collection of further clinical information. BEFDs were made not only for schizophrenia and related disorders, but also for substance abuse/dependence disorders. The BEFD method is widely used in schizophrenia studies (Calkins et al., 2007; Shi et al., 2009; Suarez et al., 2006).
Diagnostic inter-rater reliability
Inter-rater reliability was assessed within the Australian/American sample (for details see Suarez et al., 2006). Briefly, 68 cases had BEFD generated by multiple sites, and Cohen’s kappas (Cohen, 1960) were 0.88 for schizophrenia and 0.89 for schizoaffective disorder, with no notable variation reported across sites.
Statistical analysis
Outcome and explanatory variables
Two dichotomous outcome variables were specified: (i) ‘Any suicide attempt’, comparing individuals reporting a previous suicide attempt (n = 315) with those who did not (n = 497); and (ii) ‘Multiple suicide attempts’, comparing individuals who reported two or more previous suicide attempts (n = 180) with those reporting none (n = 497).
Explanatory variables included lifetime substance use disorders and a range of potential confounders of the proposed association between substance use disorders and suicidality. Substance use was defined as three binary variables specifying the presence/absence of DSM-IV diagnoses of lifetime alcohol use, cannabis use and other illicit drug use disorders, respectively. An additional polysubstance use variable was also defined, and coded as nominal with five categories: 1, ‘no drug use disorder’; 2, ‘combined alcohol and cannabis use disorders’; 3, ‘combined alcohol and other illicit drug use disorders’; 4, ‘combined cannabis and other illicit drug use disorders’; and 5, ‘combined alcohol, cannabis and other illicit drug use disorders’. Parameter estimates for this variable were based on dummy variable coding, with the first category (1, ‘no drug use disorder’) specified as the reference. Additional explanatory variables were: age at psychosis onset (years); duration of untreated psychosis (years); illness duration (years); years of formal schooling; gender; previous psychiatric hospitalisation (yes/no); and marital status, current living arrangements and current employment status, each coded as a nominal variable with categories as shown in Table 1.
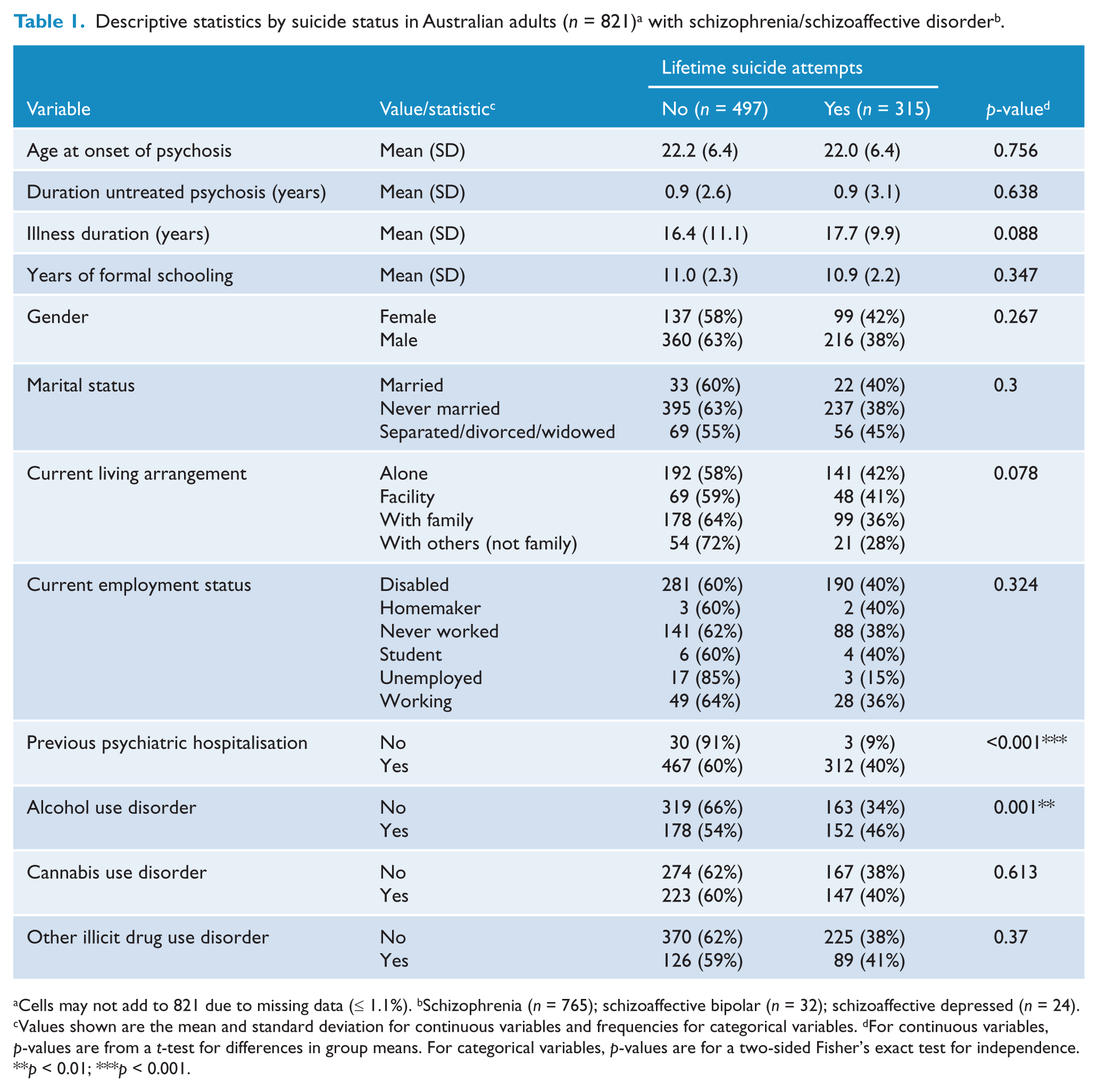
Cells may not add to 821 due to missing data (≤ 1.1%). bSchizophrenia (n = 765); schizoaffective bipolar (n = 32); schizoaffective depressed (n = 24). cValues shown are the mean and standard deviation for continuous variables and frequencies for categorical variables. dFor continuous variables, p-values are from a t-test for differences in group means. For categorical variables, p-values are for a two-sided Fisher’s exact test for independence.
p < 0.01; ***p < 0.001.
Descriptive statistics (means and standard deviations, or frequencies) were used to summarise the distribution of all explanatory variables; this was performed separately for participants with and without reported suicide attempts (see Table 1). For continuous explanatory variables, group means were statistically tested for equivalence using t-tests. For categorical variables, contingency table frequencies were compared using a Fisher’s exact test for independence (two-sided).
Multivariate logistic regression was then used to model the odds of one or more previous suicide attempts as a function of explanatory variables. Our sample included 79 nuclear family groups, individuals within which may be more similar with regard to suicide attempt risk than unrelated individuals owing to shared socioeconomic and environmental circumstances. Consequently, to ensure valid inference in the presence of clustered samples, we employed a generalised estimating equation (GEE) method. Specifically, we used the alternating logistic regression (ALR) implementation of GEE, which models within- cluster correlations using odds ratios, as appropriate for binary outcomes (Diggle et al., 1994). An exchangeable correlation structure was specified; that is, the association between any two relative pairs was assumed to be the same. Standard errors and confidence intervals were calculated using robust variance estimators. All analyses were performed using SAS v9.2 (SAS Institute Inc.).
Before building multivariate models, univariate analyses were conducted to explore the distribution and correct functional form of individual explanatory variables. Transformations were applied if fitted relationships were clearly nonlinear. Multivariate regression models were then built via step-wise backwards elimination. Initially, all potential predictors of suicide attempt risk (see Table 1) were placed in the model. At each iteration, the least significant predictor was removed and the model was refitted to check that remaining parameter estimates were not substantially altered. Step-wise variable deletion was repeated until all remaining variables made a significant partial contribution to predicting the odds of a lifetime suicide attempt at α = 0.1. The final multivariate model was subjected to typical diagnostic procedures to confirm goodness of fit and robustness to outliers or influential points.
Results
The present study was drawn from 821 individuals. We excluded up to nine individuals (1.1%) from analyses due to missing data. DIGS, FIGS and narrative summary data were available for over 90% of participants. Best-estimate final diagnoses were available for all participants. There were 580 males (71%) and 241 females included. Diagnoses included schizophrenia (n = 765, 93%), schizoaffective bipolar (n = 32, 4%), and schizoaffective depressed (n = 24, 3%).
Table 1 shows descriptive statistics for the sample with regard to a number of variables potentially associated with suicide risk, including substance use disorders. Results are stratified by the presence/absence of reported suicide attempts. The prevalence of suicide attempts in the sample was 315/812 = 38.8%. Individuals with and without suicide attempts did not differ with regard to most of the variables assessed, but differed significantly (with p< 0.05) in the frequency of previous psychiatric hospitalisation (suicide attempts were present in 40% of those with a previous hospitalisation and only 9% of those without) and alcohol use disorder (with suicide attempts recorded for 46% of affected individuals versus 34% of those unaffected).
Multivariate model results
In multivariate models, the association between suicide attempts and individual substance use disorders was examined separately for individuals with any recorded suicide attempt and those with multiple recorded suicide attempts, to identify whether predictors of multiple attempts differ in their nature or effect size. The fitted multivariate models for these two outcomes are referred to as Model 1 and Model 2, respectively.
Model 1 (see Table 2) showed that alcohol use disorders, female gender and number of psychiatric hospitalisations predicted risk of any suicide attempt at α = 0.1; however female gender merely showed a trend (p = 0.085), with only alcohol use disorder (p = 0.001) and number of psychiatric hospitalisations (p < 0.0001) reaching significance at the conventional level (α = 0.05). These two variables each demonstrated a strong positive association with risk of any suicide attempt after adjustment for other variables in the model. After adjusting for gender and number of psychiatric hospitalisations (#PH), a diagnosis of alcohol use disorder was associated with an odds ratio of 1.66 (95% CI, 1.23 to 2.24) for at least one suicide attempt, compared with individuals without an alcohol use disorder. The number of psychiatric hospitalisations was quartic root transformed, entering the model as (#PH)¼, due to a highly right-skewed distribution on the original scale (range 0–104, mode 3, median 5, mean 8). As a result of this transformation, the odds ratio associated with a one-unit increase in #PH depends upon the reference value of #PH. Back-transformed odds ratios and 95% CIs for this explanatory variable are shown for key reference values in Table 2. The model suggests that after adjusting for gender and alcohol use disorder, the greatest increase in suicide attempt risk is associated with one’s first psychiatric hospital admission, with an odds ratio of 3.36 (95% CI, 2.31 to 4.88) compared to never-hospitalised individuals. The increment in risk associated with subsequent hospitalisations diminishes steadily, with a negligible increase in risk associated with an increase from #PH = 103 to #PH = 104 (the highest value in our sample: OR = 1.009, 95% CI, 1.006 to 1.012).
Final multivariate regression model showing predictors of the presence/absence of any suicide attempt (Model 1) a .
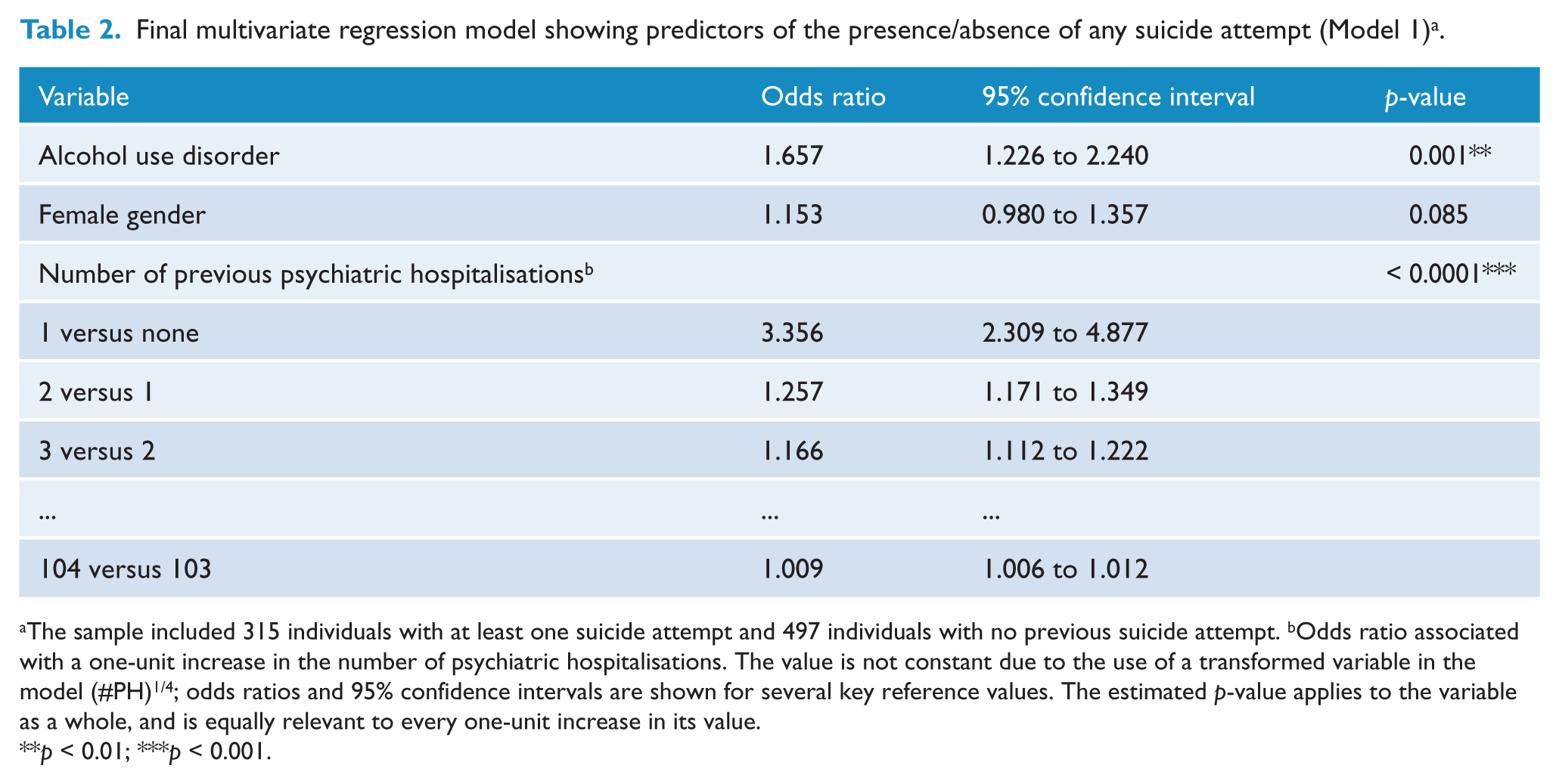
The sample included 315 individuals with at least one suicide attempt and 497 individuals with no previous suicide attempt. bOdds ratio associated with a one-unit increase in the number of psychiatric hospitalisations. The value is not constant due to the use of a transformed variable in the model (#PH)1/4; odds ratios and 95% confidence intervals are shown for several key reference values. The estimated p-value applies to the variable as a whole, and is equally relevant to every one-unit increase in its value.
p < 0.01; ***p < 0.001.
Exploratory analyses of Model 1 showed no evidence for an interaction between alcohol abuse/dependence and gender in mediating suicide attempt risk, or for an effect of cannabis abuse/dependence, other illicit drug abuse/dependence, or any two- or three-way interactions between substance use disorder variables (p-values > 0.1 for each of these variables when added into the model, both as main effects alone and in combination with interaction terms).
In Model 2 (see Table 3), the same three variables that were associated with risk of any suicide attempt in Model 1 were also associated with risk of multiple suicide attempts. Unique to Model 2, however, is that estimated effect sizes (odds ratios) were consistently higher and more significant for each explanatory variable. Alcohol use disorder was associated with an approximate doubling of the odds (OR = 2.12, 95% CI, 1.46 to 3.07) of multiple suicide attempts, after adjusting for gender and #PH. The effect of female gender was modest but now significant after adjusting for alcohol use and #PH (OR = 1.28, 95% CI, 1.05 to 1.56, p = 0.013), and one’s first psychiatric hospitalisation was associated with a more than quadrupled odds of multiple suicide attempts (OR = 4.60, 95% CI, 2.90 to 7.29, p < 0.0001), with estimated odds ratios diminishing with subsequent hospitalisations. Similar to Model 1, there was no indication for an effect of cannabis use disorder, other illicit drug use disorder, interactions between substance use disorder variables, or interactions between gender and substance use disorders upon risk of multiple suicide attempts.
Final multivariate regression model showing predictors of the presence/absence of multiple suicide attempts (Model 2) a .
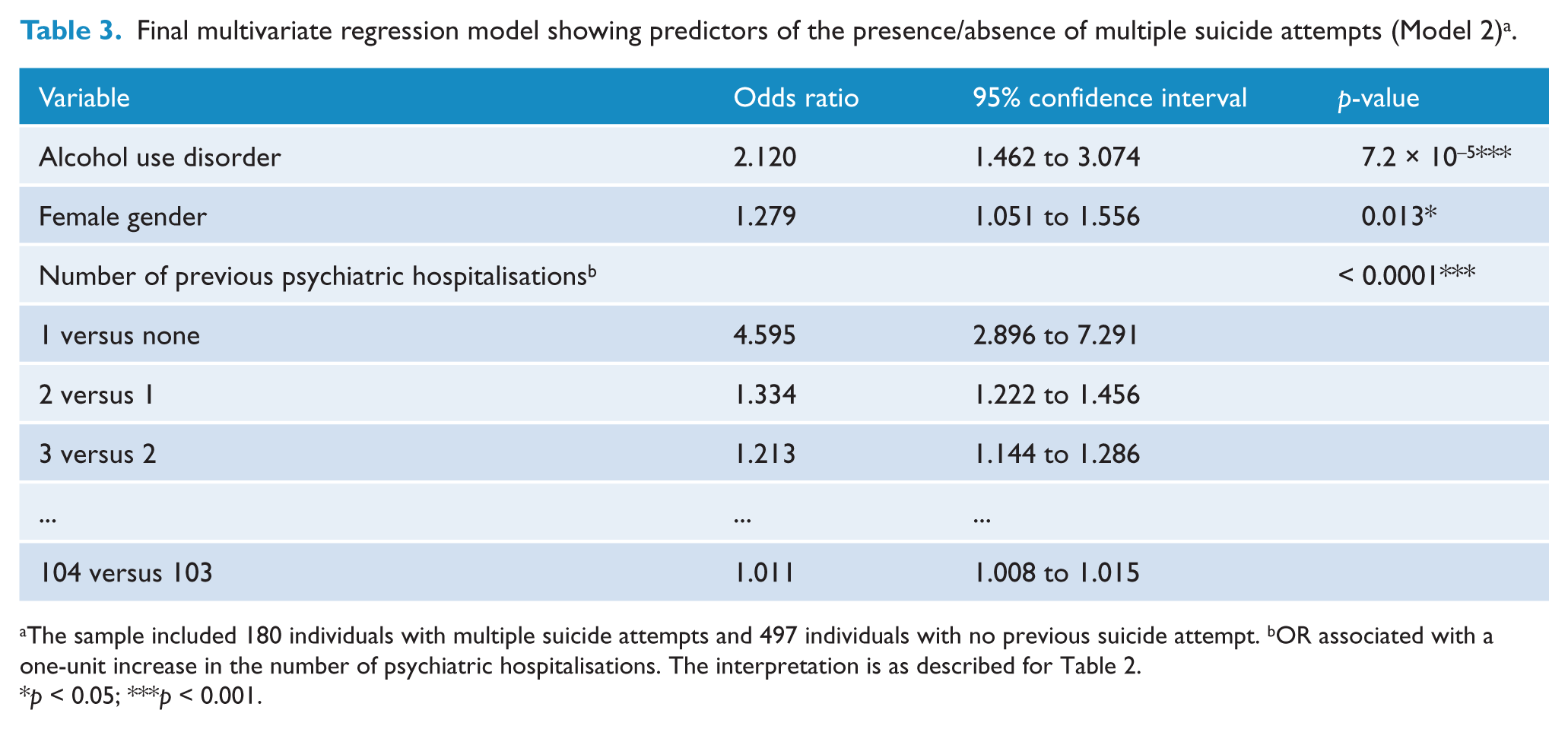
The sample included 180 individuals with multiple suicide attempts and 497 individuals with no previous suicide attempt. bOR associated with a one-unit increase in the number of psychiatric hospitalisations. The interpretation is as described for Table 2.
p < 0.05; ***p < 0.001.
Association between suicide attempts and polysubstance misuse, adjusting for demographic and clinical variables
After examining the association between suicide attempts and individual substance use disorders, an additional model was fitted to assess the suicide attempt risk associated with multiple substance use disorders. This model (Model 3) was analogous to Model 1 where the outcome was presence/absence of any suicide attempt, except that individuals only entered the model if they reported multiple substance use disorders. Individuals with no substance use disorders were included as the reference category.
Results for Model 3 are shown in Table 4. Only one variable, number of psychiatric hospitalisations, was associated with risk of any suicide attempt at the conventional significance level (α = 0.05), demonstrating similar effect size and significance as observed in Model 1. The polysubstance use explanatory variable was not associated with suicide attempt risk. A similar multivariate model could not be satisfactorily fitted to determine predictors of multiple suicide attempts due to insufficient sample sizes in a number of cells of the polysubstance use disorder × multiple suicide attempts contingency table.
Results of multivariate regression modelling of presence/absence of any suicide attempt including polysubstance abuse/dependence as a predictor (Model 3).
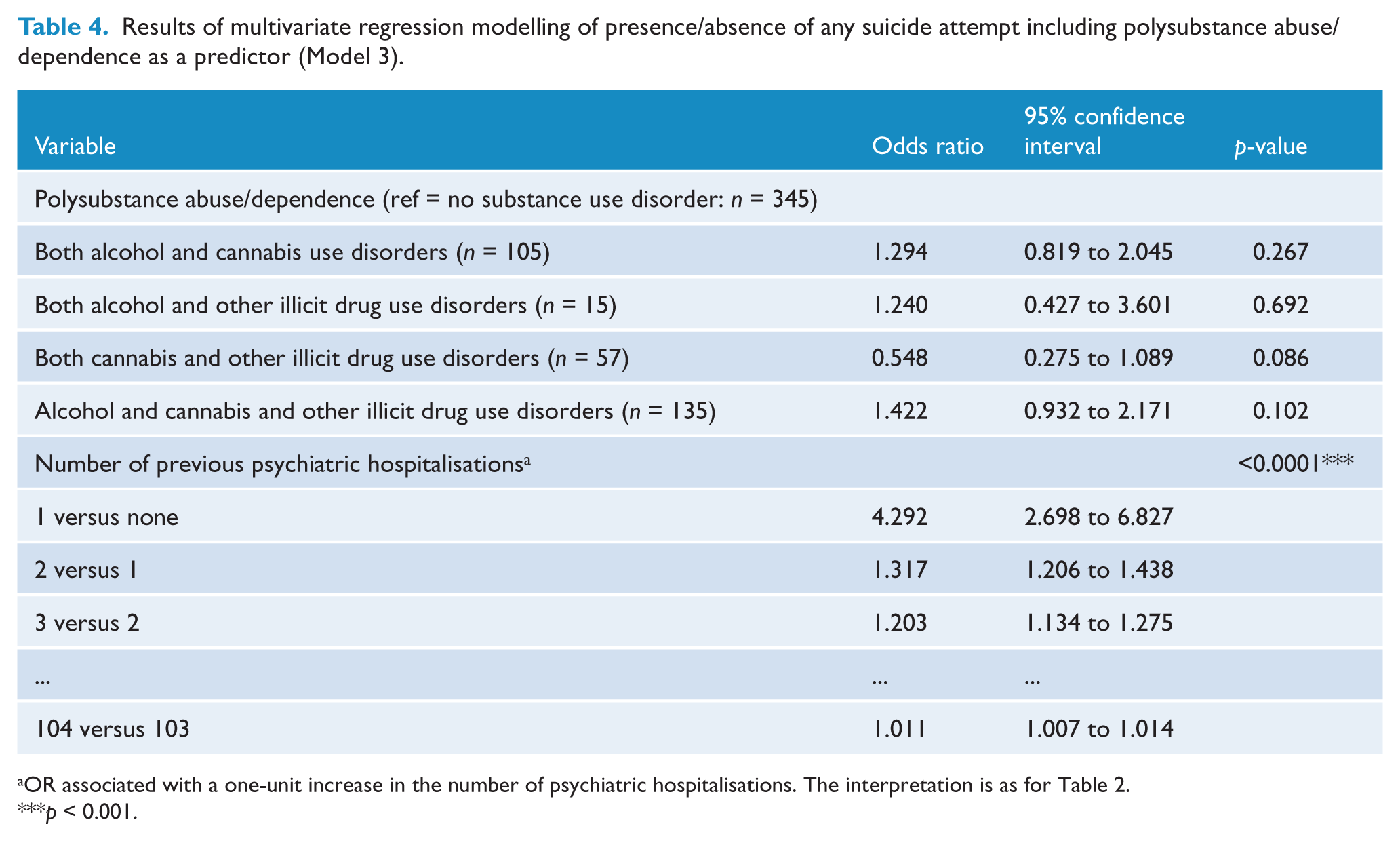
OR associated with a one-unit increase in the number of psychiatric hospitalisations. The interpretation is as for Table 2.
p < 0.001.
Discussion
This study clearly demonstrated a strong association between lifetime DSM-IV alcohol abuse/dependence and risk of lifetime suicide attempts in a large Australian schizophrenia sample. However, there was no evidence for association between cannabis use, other drug use or polysubstance use disorders with attempted suicide. A similar finding (alcohol abuse/dependence significantly associated with suicide attempts; no association of other drug abuse/dependence) was reported by Uzun et al. (2009) in Turkey. The authors noted these findings as counter-intuitive, and suggested that the low drug use rate in their cohort (4.3%) may have been a contributing factor. However, in our sample, alcohol and drug use disorder rates (alcohol 41%, cannabis 46%, other illicit drugs 27%) are significantly higher than those in the Uzun et al. (2009) study, and also higher than lifetime prevalence rates reported in Australia (any substance use disorder 24.7%) (Slade et al., 2009). We suggest, therefore, that other factors may explain these results beyond data anomalies.
Our detection of significant association between female gender and multiple suicide attempts may result from the complex, differential role of gender in suicide attempts and completions. A pattern of men completing suicide more frequently than women has been identified in individuals both with and without schizophrenia (De Hert et al., 2001; Hor and Taylor, 2010). In schizophrenia samples, women appear to have significantly more suicide attempts than men when samples of individuals who subsequently complete suicide (usually segregated into completers versus non-completers) are analysed (Allebeck et al., 1987; Karvonen et al., 2007); although the gender difference is absent when samples comprising living individuals (usually segregated into attempters versus non-attempters) are studied (Allebeck et al., 1987; Harkavy-Friedman et al., 1999; Uzun et al., 2009). This distinction may explain our modest gender effect (OR = 1.279, 95% CI, 1.051 to 1.556), given that our sample is cross- sectional. Gender was non-significant, consistent with the literature, when we segregated into attempters versus non-attempters (Model 1); whereas our multiple attempts versus no attempts distinction (Model 2) may be accessing a subsection of individuals who will subsequently complete suicide, a subsection where women have more suicide attempts. This makes intuitive sense, because a history of suicide attempts is a significant risk factor for subsequent completion (Hawton et al., 2005; Hor and Taylor, 2010).
The robust, significant association between psychiatric hospitalisations and suicide attempts in all models is probably due to a combination of two factors. First, because suicide attempts often lead to hospitalisation, it makes intuitive sense that individuals with more attempts would have more hospitalisations as a result. Second, variables relating to illness course or severity may be involved in risk of suicide attempts, with those with an illness course resulting in more psychiatric hospitalisations more likely to also have suicide attempts. We intend to test this hypothesis in future analyses.
Not surprisingly, alcohol abuse/dependence had a stronger effect when assessing the likelihood of multiple lifetime suicide attempts (Model 2) as opposed to any suicide attempt (Model 1). In the general population a link between alcohol abuse and increased occurrence of multiple suicide attempts has been observed (Rossow, 2005).
Our finding that drug use disorders and polysubstance use disorders were not significantly associated with suicide attempts in schizophrenia contrasts markedly with a French study that examined parasuicide in patients with psychosis (Verdoux et al., 1999). This study reported that polysubstance use was highly related to risk of suicide attempts. Furthermore, they identified illicit drug abuse as the robust indicator, whereas alcohol became non-significant when analysed alone.
Important differences between our study and the Verdoux et al. (1999) study may explain these differences. Notably, Verdoux et al. (1999) had a much smaller sample (n = 65), and their cohort comprised first admission cases including all psychoses. In contrast, our cohort was chronic in nature, and we included only individuals with schizophrenia/schizoaffective disorder, specifically excluding individuals with a primary diagnosis of substance-induced psychosis. A subset of patients in the Verdoux et al. (1999) study, for whom cannabis may be at least partially causal in their psychosis (which would logically increase the significance of relationships between cannabis and other variables) were excluded from our study.
Our study did not identify marital status, current employment status, or current living arrangements as significant predictors of suicide attempts in schizophrenia. Each of these has been previously implicated in suicide risk (Hawton et al., 2005). We suggest that our study design may be implicated in this lack of identified association: marital status, employment status and living arrangements variables were all current ratings at the time of assessment, whereas our suicide attempts variable was assessed as a lifetime rating. The temporal relationships between these variables may be important in their relationships.
Strengths of our study included clinical diagnosis using the BEFD method, which is the gold standard given the currently available methods of classifying schizophrenia. Furthermore, there were minimal missing data in the sample, and the sample size (n > 800) was large, providing good power to robustly identify statistical associations.
Methodological limitations
First, the samples were collected for specific genetic studies; thus this was not a representative schizophrenia sample. More precisely, it contained sib-pairs as well as unrelated individuals recruited opportunistically. A high rate of recruitment from hostels, for example, may result in over-representation of drug abuse/dependence, although increased drug abuse in boarding house accommodation was not identified in a study of substance abuse and schizophrenia in Australia (Fowler et al., 1998).
Second, these findings can only inform us about suicide attempts, and cannot be generalised to all suicidal behaviour, as our sample consisted entirely of living individuals, and there have been identified differences in the characteristics of those who attempt suicide and those who complete suicide (DeJong et al., 2010). This probably explains our different finding to the Hawton et al. (2005) systematic review of schizophrenia and completed suicide. Despite this, the characteristics of suicide attempters are an important field for investigation in their own right, even though direct comparison with suicide completion cannot be made.
Third, generalisability is further limited because we conducted a cross-sectional study, and both the suicide variables and substance use disorder variables were assessed as lifetime ratings. Therefore temporal relationships could not be explored, and there is no opportunity to follow up our cohort.
Finally, we did not include mood and symptom variables in our analyses. There appears little consensus regarding the influence of depression in suicide attempts for people with schizophrenia. In future analyses, we plan to include symptom, mood and illness course variables to examine their relationship with substance use and suicidality in schizophrenia.
Conclusions
Our finding that alcohol use disorders but not cannabis or other illicit drug use disorders are related to suicide attempts in a large, well-ascertained Australian schizophrenia sample is robust and worthy of further investigation. It replicates the finding of a recent Turkish study (Uzun et al., 2009), meaning that this counter-intuitive association has now been reported in populations with both low and high rates of substance use disorders. Further investigation of the role of mood and illness symptoms is warranted. Our finding may be clinically useful, suggesting that alcohol may be a risk factor for suicide attempts in schizophrenia, independent of comorbid substance abuse/dependence.
Footnotes
Acknowledgements
We thank all participants and their families. We thank Dr Elizabeth Holliday for providing statistical expertise in preparing the manuscript. We also acknowledge the contributions of Deborah Nertney, Professor John McGrath, the MGS Australian recruitment team, and the MGS Consortium.
Funding
This work was funded by: the United States National Institute of Mental Health (grant number RO1 MH59588) and Queensland Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.