
Abstract
Self-poisoning is one of the commonest reasons for an adolescent to present to an emergency department although the epidemiology of the behaviour is difficult to determine. Moreover, the directe treatment costs are high, the phenomena of repeat presentations are common, the long-term risk for suicide is increased and proven interventions to reduce the repetition of this behaviour are lacking. In the UK the Oxford Monitoring System for Attempted Suicide has been used to report on the period 1985–1995 [1]. A substantial increase occurred in the rate of adolescent (< 20 years) deliberate self-harm (DSH), 28.1% overall (27.7% in males, 28.3% in females) and in repetition of DSH for both sexes. The financial cost per individual presentation with selfpoisoning or attempted suicide is difficult to assess. However, the direct costs have been variously reported as UK Pounds 425 [2] and Swedish Krona 62 000 [3]. Repetition may also reflect ongoing morbidity worthy of psychiatric treatment. In addition, recurrent self-harm has been identified as a risk factor for subsequent completed suicide [4–6]; hence the identification of a highrisk group may also provide an opportunity to decrease the risk of early death in this population. Repetition of self-poisoning may be modifiable if suitable risk factors can be identified.
The literature about repetition of DSH is difficult to interpret [7]. Most of the studies that report risk factors or correlates for repetition have focused on the identification of individual subjects who have been or will become ‘repeaters’. Conversely, most of the intervention studies aimed at ‘repetition’ have attempted to reduce rates of repetition rather than prevent individuals from becoming ‘repeaters’ [8]. There are a small number of studies which have attempted to identify risk factors for adolescent subjects who repeat self-poisoning. These studies have used different methodologies and different subject groups; defined by terms like DSH (mostly self-poisoning), attempted suicide, or parasuicide, differing definitions of repetition, different study variables and different methods of analysis. Although most used clinical groups identified by presentation, admission or treatment in a general hospital [1, 9–12], some used community samples [13]. It is difficult to compare results from these studies.
In an early study from Helsinki, [6] 406 consecutive suicide attempts by 364 subjects (15–19 years) over a 10-year period were assessed by psychiatric interview using a preformatted research form to record variables. Repetition was defined by history of suicide attempt prior to the index hospital treated episode. Univariate correlates of repetition were: unemployment, homelessness, problems of family integration, previous psychiatric hospital treatment, current psychiatric outpatient care, lower levels of adaptive function, excessive alcohol use, abuse of medicinal drugs, abuse of illegal drugs and criminal acts. Presence of psychosis did not correlate with repetition. A comparison of 43 first time hospital treated suicide attempts with 38 hospital treated attempters with a past history of attempts, reported multiple attempters as having less school success, poorer school attendance, more serious suicide intent, more hostility and dysphoria and a greater number of (lifetime) stressful life events [9].
From Oxford, a recent, detailed study used standardized measures of psychological variables in relation to repetition of DSH by individuals, reported on 45 subjects (13–18 years) [10], where repetition was defined by an episode of DSH preceding hospital treatment or occurring in the 12 months following the index episode. Univariate correlates of repetition (at the index admission) were; higher scores for depression, hopelessness and trait anger; lower scores for selfesteem, self-rated problem solving and effectiveness of problem solving. However, when controlled for level of depression these differences disappeared. Assessment and management of depression was recommended as the most important consideration for reducing adolescent DSH.
In Sydney, a three year retrospective case record study of 112 adolescents (13–20 years) of attempted suicide defined by recording of ICD-9 codes E950.0 to E959.9 was reported [11]. Repetition was defined from the medical record to be any other occasion of hospital admission for the same ICD-9 codes. A multiple logistic regression analysis was done for 99 subjects with any repetition within 12 months of the index episode used as the response variable. The significant adjusted odds ratios and (CI 95%) were: chronic medical condition 3.29 (1.11–9.78), nonaffective psychosis 3.81 (1.05–13.89), alcohol abuse 3.56 (1.02 12.42) and drug abuse 4.22 (1.29–13.84). Sexual abuse 3.03 (0.95–9.71) was only significant at the p = 0.06 level, but was regarded as worthy of further consideration by the authors.
In a US community study, using a discriminant function analysis to distinguish repeaters from single suicide attempters, a four factor solution was found for the repeaters: less physically attractive, greater functional impairment due to medical illness, hypomanic personality style and loss of a parent before age 12 years [13].
For our study, in a population-based clinical sample (hospital treated) of all categories of poisoning, we attempted to identify correlates of repetition episodes (event rates) rather than for individual repeaters (subject rates). This was done with the intention of identifying factors that could be used for later intervention studies aimed at reducing repetition rates, direct treatment costs and hopefully morbidity. However, we chose to include subject-based variables for the study variables, which might be more generalizable to other clinical settings, rather than ‘system’ variables which we thought would be more likely to vary substantially in other areas which do not have our long standing system of multidisciplinary service delivery [14]. We also decided to include all types of poisoning; deliberate, recreational and accidental. This was done for several reasons. For hospital-based treatment this is the population generating the total direct costs incurred, true accidental poisoning in adolescents is very rare and ‘recreational’ poisonings presenting for hospital treatment may sometimes be misclassified ‘deliberate’ types but nonetheless have a similar increased rate of subsequent premature death and suicide as for ‘deliberate’ types [15].
Aim
This study aimed to determine the correlates of representation (event rates) following an index episode of hospital treatment for self-poisoning in an unselected group of adolescents presenting for treatment to a regional poisoning service.
Method
Subjects
The Hunter Area Toxicology Service (HATS) is a regional referral service for all cases of poisoning for an adolescent and adult population of around 500 000 people. A search was performed on the Hunter Area Toxicology Service (HATS) database, described in more detail elsewhere [16], for all index presentations during the study period with an episode of self-poisoning by adolescents aged between 10 and 19 years from January 1991 until December 1995. Subjects were included whose poisoning episode was classified as deliberate, recreational or accidental. The outcome of interest was re-presentation to HATS with each subsequent episode of self-poisoning of any type during the study period, determined by further search of the HATS database.
Independent variables and rating procedures
The study factors were used from the index admission:
The categorization of employment status was made by the admitting clerical staff at presentation.
These emergency department assessments were not made according to any diagnostic system or formal criteria. In a study of 740 adolescents (13–19 years) with self-poisoning, the medical officer's rating of current substance abuse was compared with the gold standard of DSM-IV criteria as rated by clinical psychiatric assessment and found to have a sensitivity of 91% and a specificity of 60% [17]. It is likely that this rating of ‘substance abuse’ reflects a pattern of drug and/or alcohol use which includes any use, misuse, abuse and dependence, thought to be clinically relevant by the medical officer. As such, ‘any substance abuse’ is likely to include a greater number of subjects than that defined by the psychiatric assessment and DSM-IV Substance Related Disorder category.
The clinical data were recorded on a preformatted toxicology admission data collection form reported elsewhere [18].
Analyses
Time-event analysis was used due to the widely differing follow up-times between subjects. The advantage of this method being that exposure variables can be adjusted for the follow-up time. We calculated unadjusted rate ratios per person-year exposure to each of the study factors using Stata® [19, 20]. Each of these rate ratios were also adjusted for potential confounding effects, such as gender, age, unemployment, psychiatric diagnosis or ‘substance abuse’, as appropriate, using a Mantel-Haenzel method [19]. For the analysis of the psychiatric diagnostic variables, those patients who did not have a psychiatric assessment were excluded from the analysis. Comorbidity of psychiatric disorder was not considered as a confounding variable because the individual diagnostic categories were the factors of interest in the study. In addition, a failure curve with 95% confidence bands was constructed for the first representation.
The HATS database and its collection procedures has been reviewed by the Hunter Area Research and Ethics Committee.
Results
There were 450 patients who presented on a total of 551 occasions. There were 372 ‘index’ admissions classified as deliberate self-poisoning (DSP), 67 as recreational and 11 as accidental. Three hundred and ninety-four individuals presented on one occasion, 34 on two, 12 on three, 5 on four, 2 on six and 1 each on five, seven and nine occasions which represents a patient-based rate for repetition of 12.4% over the 5 years of the study. Figure 1 is a failure curve of representation following an index admission with self-poisoning. The failure curve represents the probability, and the 95% CIs for that probability, of representing within a defined time-period. For example, the probability of re-presenting within one year was 0.09 (0.07–0.12) and within 5 years was 0.16 (0.12–0.21). The median and modal age at initial presentation was 17 years. Sixty-eight (15%) subjects were aged 10–14 at initial presentation and 382 (85%) subjects were aged 15–19. Three hundred and nine (69%) subjects were female and 141 (31%) were male. Details of employment were obtained from 445 subjects. One hundred and fifty-three patients were unemployed at the time of initial presentation. Of the remainder 210 were students, 57 full-time employees, six were part-time employees, 15 pensioners and four were categorized as ‘other’.
Failure curve, with 95% confidence bands, for the first re-presentation after the index admission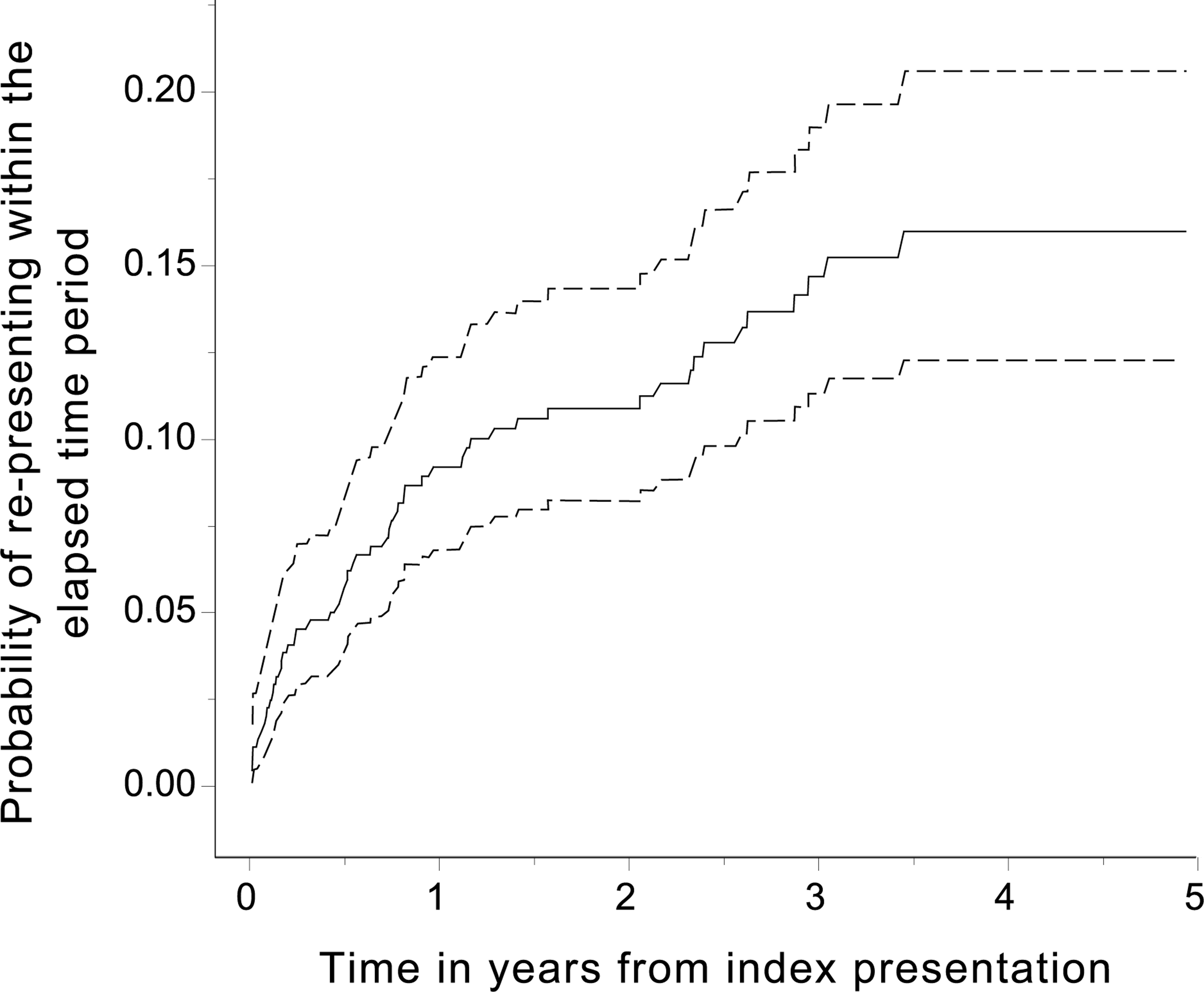
Three hundred and sixty-five (81%) subjects underwent psychiatric assessment during their index presentation and the number of subjects with diagnoses in each diagnostic group is summarized in Table 1. Some subjects had diagnoses in multiple diagnostic groups. One hundred and sixty-seven (37%) subjects were rated by the emergency department medical officer as having any current or past (ever) alcohol or substance abuse (including nicotine). These results are summarized in Table 2.
Risk of re-presentation episodes by demographics and psychiatric diagnosis
The unadjusted and adjusted rate ratios for factors contributing to representation rates are summarized in Tables 1 and 2. The significant variables on univariate analysis were: unemployment, schizophrenia and other psychotic disorders, personality disorder, ‘any substance abuse (ever)’, ‘benzodiazepine abuse’, ‘alcohol abuse’ and ‘intravenous substance abuse’. The significant variables on multivariate analysis were: schizophrenia and other psychotic disorders, personality disorder, ‘any substance abuse (ever)’, ‘alcohol abuse’ and ‘benzodiazepine abuse’. ‘Intravenous substance abuse’ and unemployment were no longer significant.
Risk of re-presentation episodes for medical officer rating of ‘substance abuse’ (ever) n = 450
Discussion
The analysis of re-presentation following an initial event of self-poisoning in adolescence poses problems given the tendency for some patients to represent on multiple occasions. An approach taken in previous studies has been to use the first re-presentation as the outcome measure, thereby identifying the individual's risk for re-presentation following any given admission. The approach we have taken in the present study is to perform a statistical analysis of multiple events over time thereby examining the contribution of each putative risk factor to the overall frequency of re-presentations. This, we believe, gives a better measure of the impact of a risk factor upon the need to allocate resources, aimed at reducing the rates of repetition, rather than an approach aimed at identifying individuals who will subsequently repeat. Most interventions have been aimed at reducing the frequency of repetition and we would suggest that interventions could be best informed by identifying risk factors for both event-based and patientbased repetition.
In our catchment area the recurrence risk (patientbased) for DSP patients (all ages) within one year is around 13% [21]. The finding that 12.4% of adolescents (patient-based rate) will re-present with self-poisoning during the 5 years of the study is consistent with previous reports in the literature. In one study, 9.5% repeated within a mean follow-up period of 2.8 years [22], and in a second study 14% were referred to hospital for further self-poisoning or self-injury within the following year [23]. Consistent with the present study, repetition of self-poisoning occurs most frequently in the first few months after an initial admission [22]. This is also similar to the findings in adult populations where a review paper reported a median time to repetition of deliberate self-harm was 72 days [24]. Early repetition has also been reported for community samples for ‘attempted suicide’ [13] although this is not necessarily for hospital treatment.
In the present study, the risk factors having the strongest association with episodes of recurrent self poisoning were ‘any substance abuse (ever)’, ‘alcohol abuse’, ‘benzodiazepine abuse’, schizophrenia and other psychotic disorders (DSM-IV) and personality disorder (DSM-IV). Comparison with the literature is difficult. The finding of an association between benzodiazepine abuse and repetition of self-poisoning is new and may reflect a phenomenon that is localized to the Newcastle region or to adolescents. Our results are most similar to another Australian study, which found chronic medical illness, nonaffective psychosis, alcohol abuse and drug abuse to be risk factors for identifying repeaters [11]. The present study did not consider medical illness as a study variable.
There are very few interventions that have been demonstrated in randomized controlled trials to be effective in reducing the repetition of DSP/DSH. For psychological interventions, only Dialectical Behaviour Therapy (for chronically parasuicidal adult females meeting criteria for Borderline Personality Disorder) [25] and a brief Interpersonal Therapy intervention for hospital DSH patients [26] have been reported as effective. Both of these relied on self-report measures of repeat parasuicide or DSH, and most episodes of repetition did not involve re-presentation to hospital. In a very small series of patients with personality disturbance, it was found that depot flupenthixol [8] was beneficial in reducing repetition. A further study using a RCT design but a post-hoc analysis suggested a reduction in repetition following treatment with paroxetine [27]. Intervention strategies may have to rely on targeting community groups, clinical groups (DSP/DSH) or high-risk subgroups within these clinical groups for whom modifiable risk factors can be identified and ‘treated’. The identification of high-risk groups for repetition might enable targeting of such interventions especially when insufficient resources exist for provision of these treatments to all self-poisoning patients.
Although interventions to reduce repetition of DSP have been largely unsuccessful in adult groups and largely untested in adolescent samples there are some possible interventions that might be reasonable to try. In a recent review of interventions aimed at adolescents, it was concluded that there are effective indicated, selective and universal interventions for important risk factors for depression and suicidal behaviour [28]. That is to say that the interventions have been shown to be effective in reducing the risk factors themselves rather than the outcome of completed suicide. Of these effective interventions aimed at risk factors, interventions for substance abuse and alcohol abuse were noted. Unfortunately, these interventions are rarely implemented, even in indicated populations.
The limitations of the present study are in the ability to generalize the results to a broader population, the use of hospital presentations alone and that the results should not be interpreted in the context of an individual's risk. The literature on repetition of adolescent self-poisoning has focused on the individual's risk for being classified as a ‘repeater’. The use of hospital presentation for case identification (and outcome) means that the results should be interpreted in terms of the impact of the risk factors upon health service, particularly hospital service, utilization. The present study aimed to determine those factors contributing to the rates of repetition rather than an individual's risk for repetition and therefore should be thought of as population characteristics rather than identifying an individual. Nonetheless, interventions aimed at individuals with these characteristics could be used in attempts to reduce subsequent episodes of repetition.
Conclusions
Efforts to prevent recurrence of self-poisoning episodes should be directed towards nonaffective psychoses, personality disorders and substance (particularly alcohol and benzodiazepine) abuse. This would require psychiatric assessment of all adolescents who present with self-poisoning in order to identify diagnostic defined at risk groups. This requirement is largely consistent with the current recommendations by the Australasian College of Emergency Medicine and the Royal Australian and New Zealand College of Psychiatrists [29]. Moreover, a rating by the medical officer in a emergency department as to whether a patient has ever had any substance, particularly alcohol or benzodiazepine, abuse would be possible in all but the most poorly resourced hospitals and may be a useful initial screening device.
Further elucidation of the factors contributing to representation episodes of self-poisoning may require better hospital surveillance systems, standardized assessment instruments, inclusion of social and functional as well as diagnostic measures, consistent definitions of subject groups and repetition, as well as studies from different geographical locations.