
Abstract
Background:
The Australian Institute of Health and Welfare has reported an increased rate of hospital-treated intentional self-harm in young females (2000–2012) in Australia. These reported increases arise from institutional data that are acknowledged to underestimate the true rate, although the degree of underestimation is not known.
Objective:
To consider whether the reported increase in young females’ hospital-treated intentional self-harm is real or artefactual and specify the degree of institutional underestimation.
Methods:
Averages for age- and gender-standardised event rates for hospital-treated intentional self-harm (national: Australian Institute of Health and Welfare; state: New South Wales Ministry of Health) were compared with sentinel hospital event rates for intentional self-poisoning (Hunter Area Toxicology Service, Calvary Mater Newcastle) in young people (15–24 years) for the period 2000–2012. A time series analysis of the event rates for the sentinel hospital was conducted.
Results:
The sentinel hospital event rates for young females of 444 per 100,000 were higher than the state (378 per 100,000) and national (331 per 100,000) rates. There was little difference in young male event rates – sentinel unit: 166; state: 166 and national: 153 per 100,000. The sentinel hospital rates showed no change over time for either gender.
Conclusion:
There was no indication from the sentinel unit data of any increase in rates of intentional self-poisoning for young females. The sentinel and state rates were higher than the national rates, demonstrating the possible magnitude of underestimation of the national data. The reported increases in national rates of hospital-treated self-harm among young females might be due to artefactual factors, such as changes in clinical practice (greater proportion admitted), improved administrative coding of suicidal behaviours or possibly increased hospital presentations of community self-injury cases, but not intentional self-poisoning. A national system of sentinel units is needed for the accurate and timely monitoring of all hospital-treated self-harm.
Introduction
Hospital-treated self-harm is common (Nock et al., 2008), costly (Sinclair et al., 2006) and associated with subsequent repetition, suicide and all-cause mortality (Carroll et al., 2014; Reith et al., 2004). A recent systematic review reported that the most common form of self-harm is intentional self-poisoning (median 90%), followed by self-cutting (10.5%) and other methods, such as hanging, jumping and burning (6.2%; Carroll et al., 2014), known as self-injury. While only a minority of self-harm comes to clinical attention, hospital-treated self-harm officially accounts for over 26,000 admissions and approximately 89,000 bed days in Australian hospitals each year (Tovell et al., 2012). In Australia, the age group of 15–24 years has the highest reported hospitalised self-harm event rate: 345 and 143 per 100,000 for females and males, respectively (RANZCP, 2016).
However, our institutional record systems for monitoring this important public health issue have acknowledged deficiencies (McKenzie et al., 2006). Institutional reports of intentional self-harm draw data from hospital record systems where events (but not individuals) are identified through extraction of data for episodes of care (admissions) with relevant self-harm diagnostic codes (specifically, ICD-10-AM: X60–X84). This means that the reliability of the reported rates is dependent on two main factors: the clinical decision regarding whether treatment can be provided entirely within the Emergency Department (ED) or whether hospital admission is required, and the non-clinical accuracy of the coding by administrative staff (Harrison and Henley, 2014; McKenzie et al., 2009). While the magnitude of this underestimate has not been quantified in Australian datasets, a recent Norwegian study reported that only 49% of deliberate self-harm admissions were adequately coded (Mellesdal et al., 2014).
There are regional alternatives to these institutional data sources with more accurate and timely data about hospital-treated self-harm available from ‘sentinel’ hospitals. Sentinel hospitals have known catchment populations and routine clinical and administrative data capture processes and regularly report on all cases (admitted and non-admitted) presenting for treatment. Sentinel units for hospital-treated self-harm exist in the United Kingdom (Oxford, Leeds, Manchester; Hawton et al., 2007), Australia (Newcastle; Hiles et al., 2015) and New Zealand (Christchurch; Beautrais, 1994), and they provide a useful comparison point for institutional data. For example, institutional data from Australia reported age-standardised hospital-treated self-harm event rates for 2010–2011 as 148 per 100,000 for females and 87 per 100,000 for males (all ages; Pointer, 2013), while the sentinel unit in Newcastle (NSW) reported age-standardised event rates restricted to intentional self-poisoning (not self-cutting or other self-injury methods) of 220 per 100,000 for females and 113 per 100,000 for males (Hiles et al., 2015) highlighting the substantial underestimation of self-harm events in official institutional datasets.
Over the past decade, reports from the AIHW have highlighted an increase in national rates of overall hospital separations for intentional self-harm from 105 per 100,000 in 1999 to 117 per 100,000 in 2010–2011 (AIHW, 2008a, 2008b; Pointer, 2013), representing a statistically significant rise of 0.5% per year (AIHW, 2013, 2018). The rate increase has been consistently identified by AIHW as being due to a rate increase specific to young females (<24 years), while rates for other age and gender groups have remained relatively stable over time (AIHW, 2008a, 2008b; Harrison and Henley, 2014; Pointer, 2013). The reported increase has been uncritically accepted as a real increase in self-harm behaviour and widely repeated in the general community and suicide prevention media (e.g. ABC, 2013, 2016; Suicide Prevention Australia [SPA], 2016). However, it remains unclear as to whether any reported changes are due to real changes in rates or a consequence of artefactual factors or a combination.
Recently, there have also been reported increases in ED presentations (not restricted to admissions) of young people for treatment of suicidal behaviours in different states in Australia. For New South Wales (NSW; 2010–2014), the combined number of presentations for suicidal ideation, self-harm or intentional self-poisoning showed the greatest increase for the 10- to 19-year-old age group (mean annual increase of 27% per year; Perera et al., 2018). In Victoria (2008–2015), self-harm presentations to the ED reportedly increased by 53% (Hiscock et al., 2018). An accompanying editorial indicated some of the limitations of administrative data sets, including the possibility of inaccurate coding practices and acknowledged that there had been no increase in mental disorder prevalence in young people since 1998 from community estimates, while concluding that the reported increases were likely to be due to a failure of available alternative community services for young people with mental health problems (Sawyer and Patton, 2018).
The aims of this study were, for the period 2000 to 2012, as follows:
(a) Compare the hospital-treated self-harm event rates reported by the AIHW (national) and NSW Ministry of Health (MoH; state) with the hospital-treated intentional self-poisoning event rates at the Newcastle sentinel hospital;
(b) Estimate the extent of underestimation in official institutional records by calculating a best estimate rate for hospital-treated self-harm for young females and young males;
(c) Evaluate changes in hospital-treated event rates for intentional self-poisoning over time in the Newcastle sentinel hospital.
The answers to these research questions will help identify the degree of underestimation in official data sources and provide a basis to consider whether the reported increased event rates are real or artefactual.
Method
Data sources
The AIHW publish official, publicly available reports on hospitalised self-harm, collating data across public and private hospitals within Australia. They report incidence and event rates of intentional self-harm as drawn from hospital records for admission for any injury case where the first reported that external cause is intentional self-harm (as indicated by a diagnosis code of X60–X84). Data specific to NSW and Hunter New England Local Health District are available in the public domain through the NSW MoH. Data specific to the sentinel unit were extracted from the locally held data with ethics approval from the Hunter New England Human Research Ethics Committee.
Setting
Australia has a total population of 23 million (19.5 million adults) with the majority living on the eastern seaboard. NSW is the most populous state in Australia with approximately 7 million residents, including over 5 million living in the capital, Sydney. The state comprises 15 health districts including Hunter New England Local Health District. This health district spans 25 local government areas across the Hunter, New England and Lower Mid North Coast regions and has 38 hospitals providing care for up to 1 million people. Newcastle is the largest city within the Hunter New England region and hosts most of the tertiary health services and teaching hospitals.
The regional Hunter Area Toxicology Service (HATS) is based at the Calvary Mater Newcastle hospital. It has provided hospital-based treatment for poisoning patients, including intentional self-poisoning patients, since 1987. HATS services a primary referral area with an urban–suburban population of 400,000 and is a tertiary referral centre for an additional rural population of around 250,000. All poisoning presentations to EDs are admitted (or notified) to HATS under the clinical care of the attending clinical toxicologist and medical and psychiatric staff use a preformatted clinical record sheet to prospectively collect toxicological, clinical and psychiatric information on all patients (Buckley et al., 1999). Data are routinely entered into a database separate to the hospital’s main medical record system by staff blind to study hypotheses. The service does not comprehensively cover childhood (<14 years) poisonings.
Data extraction
National population rates for hospital separations for intentional self-harm were drawn from AIHW reports (Berry and Harrison, 2006, 2007; Bradley and Harrison, 2008; Helps et al., 2002; Kreisfield et al., 2012; Kreisfeld and Harrison, 2010; McKenna and Harrison, 2012; Norton et al., 2012; Tovell et al. 2012). State (NSW) and the Hunter New England Local Health District rates were drawn from the data available in the public domain from the NSW MoH (www.healthstats.nsw.gov.au; accessed 17 November 2016). These rates are age and gender standardised.
For the sentinel hospital, data were extracted for HATS admissions that occurred between 1 July 2000 and 30 June 2012. Data were restricted to presentations for intentional self-poisoning for people residing within the postcodes of the primary referral area (local government areas of Newcastle, Lake Macquarie and Port Stephens). Poisonings classified as recreational/chronic misuse, accidental, iatrogenic or occupational were excluded from the study data. A total of 2075 admissions were recorded for 1359 individuals aged 15–24 years for the study period. Event rates were calculated from these data for the 15- to 24-year age group and by gender (male, female). They were age and gender standardised using population data for the local government areas within the sentinel hospital’s referral catchment area.
Data analysis
To account for non-reported annual data in the AIHW records, rates were averaged across 2-year periods and charted using the TREND function in Microsoft Excel 2010. A standardised rate ratio was calculated for the 15- to 24-year age group by gender, using the rates for each of the national and state datasets compared to the sentinel hospital (HATS). Graphical comparisons were presented for the sentinel unit (HATS) versus the local health district (HNELHD: MoH), state (NSW: MoH) and national (AIHW) data. We report the HATS sentinel unit intentional self-poisoning rates and the local health district self-harm rates as the best estimates per 100,000 per year for young males and young females.
Trends in monthly frequency of hospital-treated intentional self-poisoning events (for 144 months, covering the period of July 2000 to June 2012) for the HATS primary referral area (all ages and 15–24 years and 15–29 years) were analysed with a series of autoregressive integrated moving average (ARIMA) interrupted time series regression models, stratified by gender. Time series regression models were specified to account for autocorrelation (in this instance, likely seasonal effects), random variation and trend (or ‘drift’) that are inherent in time series data (SAS Institute, 2012). ‘Period’ was specified in time series regression models to estimate the linear trend over the study period. Statistical analyses of the linear trend shown in Table 2 were completed using PROC ARIMA in SAS 9.4.
Results
Hospital-treated self-harm comparison of age event rates
The national age-standardised self-harm event rate for young females was 332 per 100,000, while the state rate was 378 per 100,000. Both of these were much lower than the sentinel hospital rate of 444 per 100,000, which was for intentional self-poisoning events only. The annual age-standardised rates for young males were more similar with 153, 166 and 166 per 100,000 at the national, state and sentinel hospital, respectively (Table 1). For young females, the standardised rate ratio for the sentinel unit compared to the national and state data was 1.34 (95% confidence interval [CI] = [1.12, 1.61]) and 1.17 (95% CI = [0.97, 1.41]), and for young males it was 1.09 (95% CI = [0.82, 1.46]) and 0.99 (95% CI = [0.74, 1.33]), respectively.
Average annual event rates (and standard deviations) per 100,000 of hospital-treated intentional self-harm by gender between 2000 and 2012.
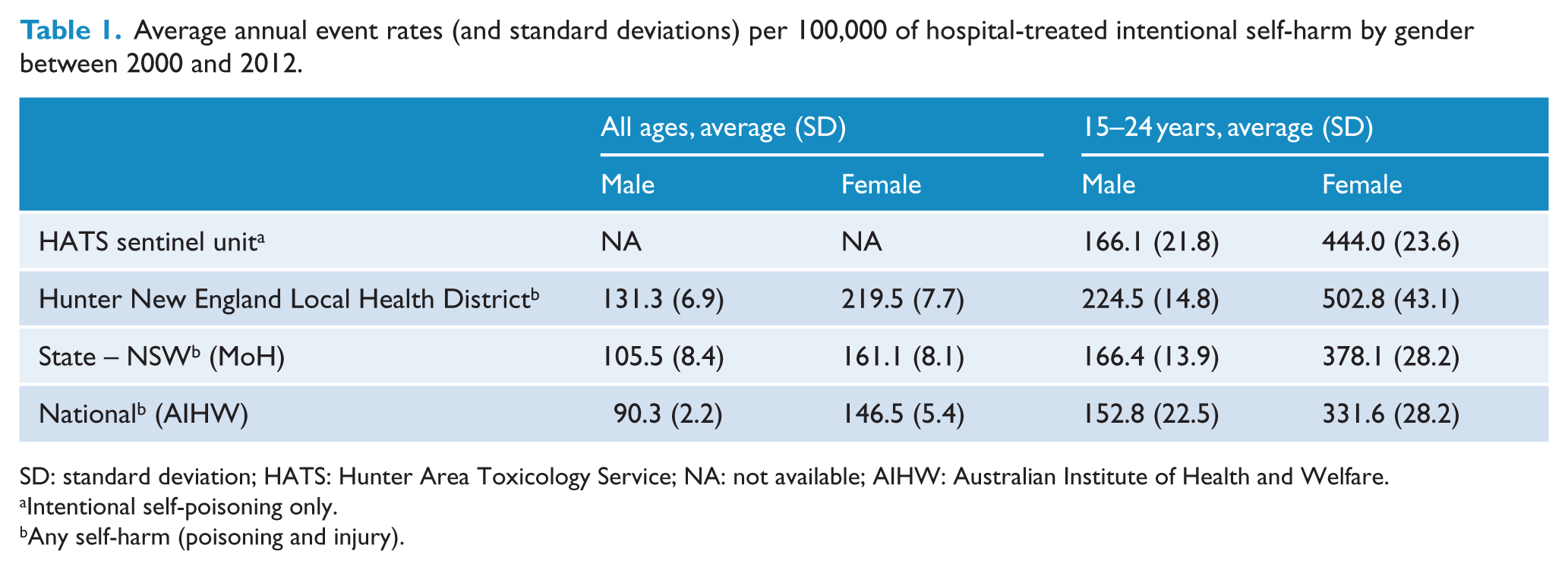
SD: standard deviation; HATS: Hunter Area Toxicology Service; NA: not available; AIHW: Australian Institute of Health and Welfare.
Intentional self-poisoning only.
Any self-harm (poisoning and injury).
Best estimates of event rates
The Hunter New England Local Health District event rates (which included the data for the sentinel unit and other hospitals) were higher than the sentinel hospital’s rates for young females and males, with the local health district event rates reflecting the inclusion of both intentional self-poisoning and self-injury events in the overall self-harm rate. This gives a best estimate for self-harm for the Hunter New England Local Health District of 225 for young males and 503 for young females per 100,000 per year (see Table 1 and Figure 1).
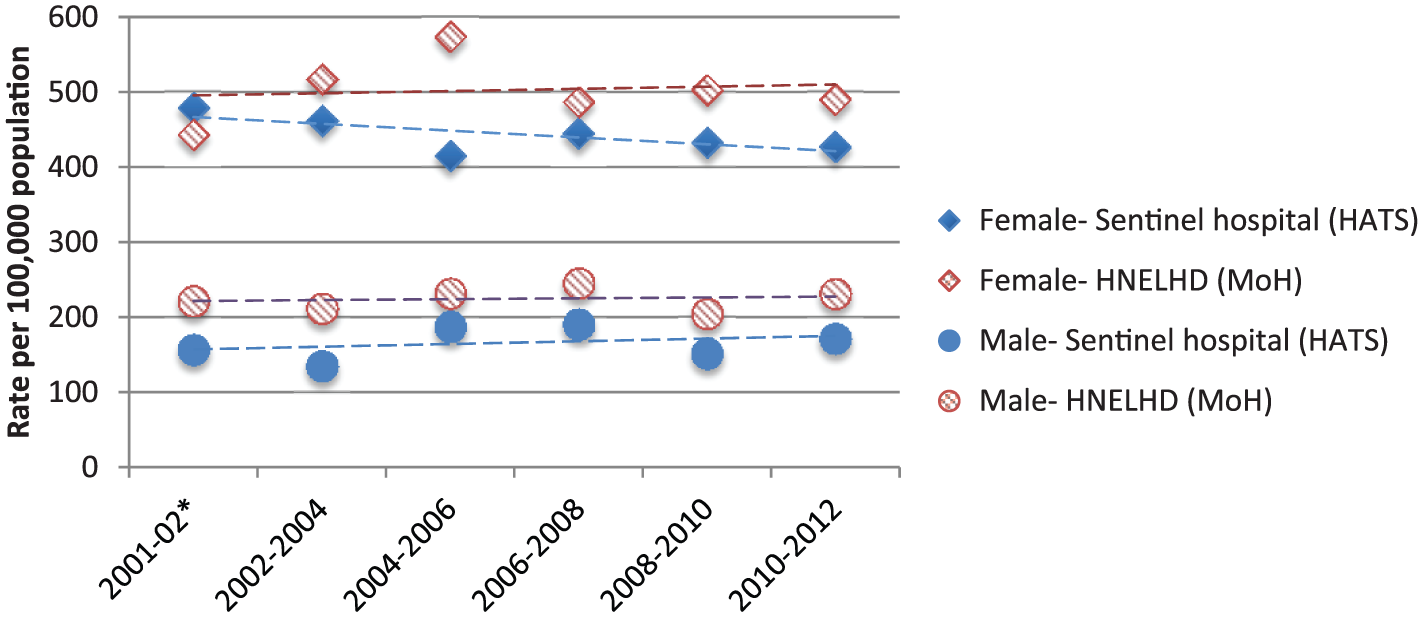
Rates for hospital-treated events by gender for the 15- to 24-year age group for sentinel hospital (intentional self-poisoning) and Hunter New England Local Health District (self-harm).
Using the best median estimate of 90% of hospital-treated self-harm being intentional self-poisoning (Carroll et al., 2014), this would approximate to, for young males, 203 separations for intentional self-poisoning and 22 separations for self-injury and, for young females, 453 separations for intentional self-poisoning and 50 separations for self-harm per 100,000 each year. It should be acknowledged that the median estimates used for these calculations are not mutually exclusive, since some self-harm events might include, for example, both intentional self-poisoning and self-injury or self-cutting and other forms of self-injury.
We can also use Australian data to further contextualise these estimated proportions of intentional self-poisoning and self-injury. Recent Australian estimates for separations (admitted patients only) reported that the proportion presenting with intentional self-poisoning (excluding gaseous poisoning) was 81% for 2010–2011 (Harrison and Henley, 2014; Pointer, 2013), 82% for 2012–2013 (Pointer, 2015) and 81% for 2014–2015 (Pointer, 2018). These Australian institutional data have the usual limitations; separations are for admitted patients and exclude cases treated entirely within the ED, gaseous poisonings are excluded (usually carbon monoxide from vehicular exhaust an additional 1.2%) and cases using both intentional self-poisoning and self-harm are not accounted for since these reports use only the first ICD code recorded. It is well recognised that a sizable proportion of injury with a sharp object (mostly superficial cutting) is accompanied by self-poisoning in hospital-treated cases (Hawton et al., 2004) and that methods change over time with repeat attempts, especially cutting changing to poisoning (Owens et al., 2015). Once these limitations are acknowledged, it seems that for Australian populations the proportion with intentional self-poisoning is very close to the international pooled median estimates of 90% (Carroll et al., 2014).
Changes over time
At the sentinel hospital, there was no statistically significant change over time in the event rate of hospital-treated intentional self-poisoning from 2000 to 2012. Specifically, there was no evidence of an increase or a decrease in secular trends over the study period, for males or females aged 15–24 years or 15–29 years (see Figure 2 and Table 2).
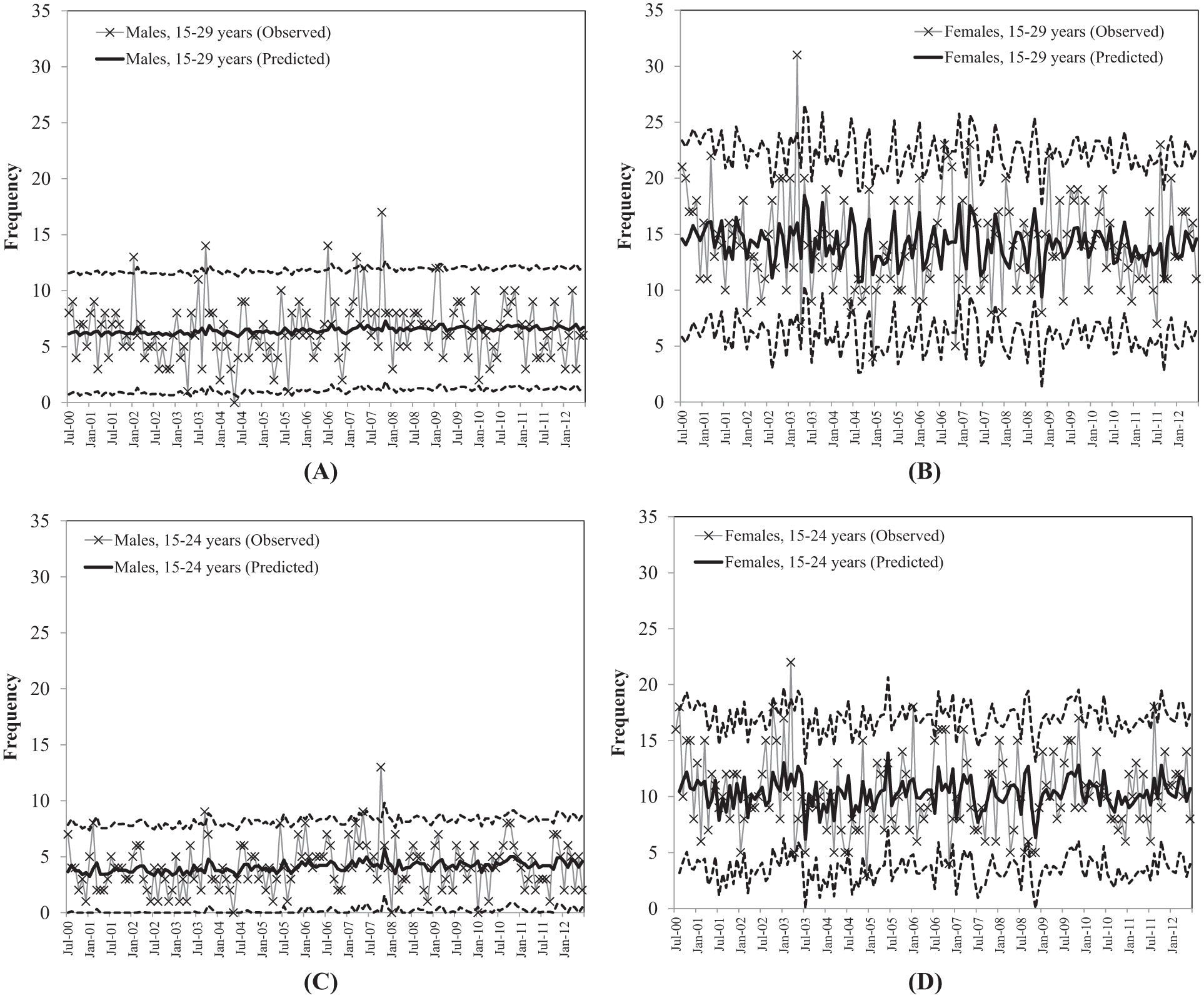
Trends in monthly frequency of intentional self-poisoning for HATS sentinel unit (July 2000–June 2012; observed counts and predicted counts from ARIMA models presented): (A) males, (B) females, (C) males, 15–24 years, and (D) females, 15–24 years.
Linear trend in monthly frequency of intentional self-poisoning for HATS sentinel unit (July 2000–June 2012).
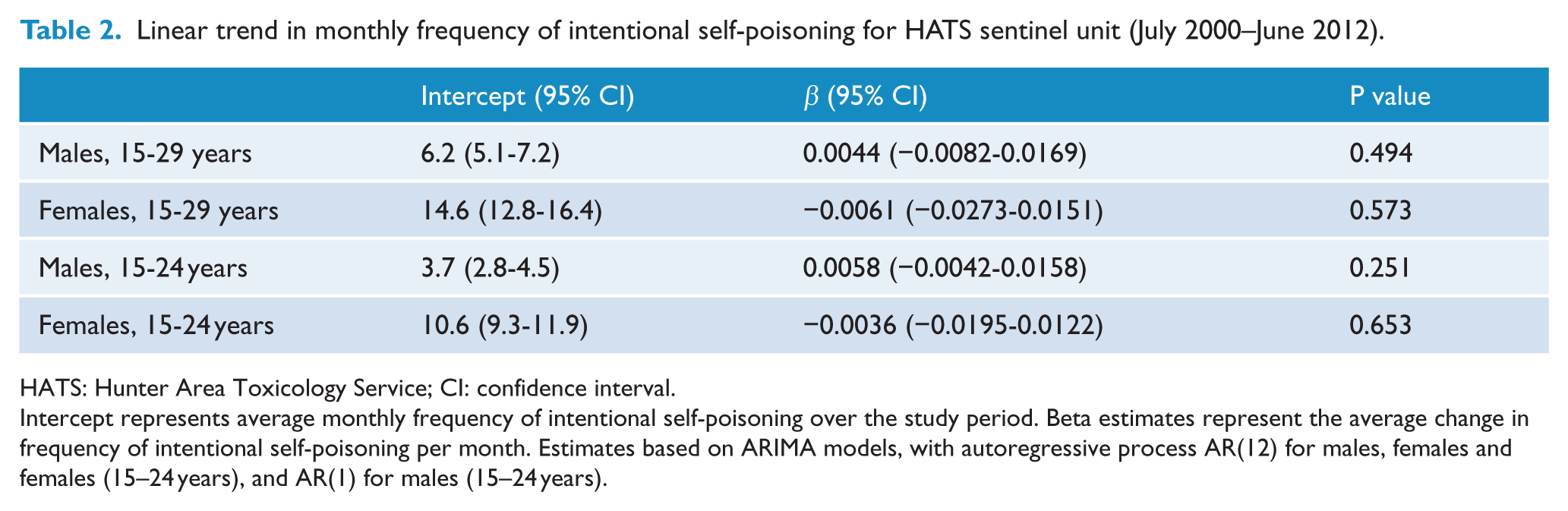
HATS: Hunter Area Toxicology Service; CI: confidence interval.
Intercept represents average monthly frequency of intentional self-poisoning over the study period. Beta estimates represent the average change in frequency of intentional self-poisoning per month. Estimates based on ARIMA models, with autoregressive process AR(12) for males, females and females (15–24 years), and AR(1) for males (15–24 years).
The state and sentinel hospital event rates for young females showed a generally consistent difference in the rates, with lower values for the state rates probably representing the underestimation of institutional data at the state level (Figure 3). In contrast to the sentinel hospital rates, the national dataset showed an apparent increase in self-harm rates for young females over time; however, even the highest 2-year event rate for self-harm was below the intentional self-poisoning event rate at the sentinel hospital for the same 2-year period (2010–2012; see Figure 4).
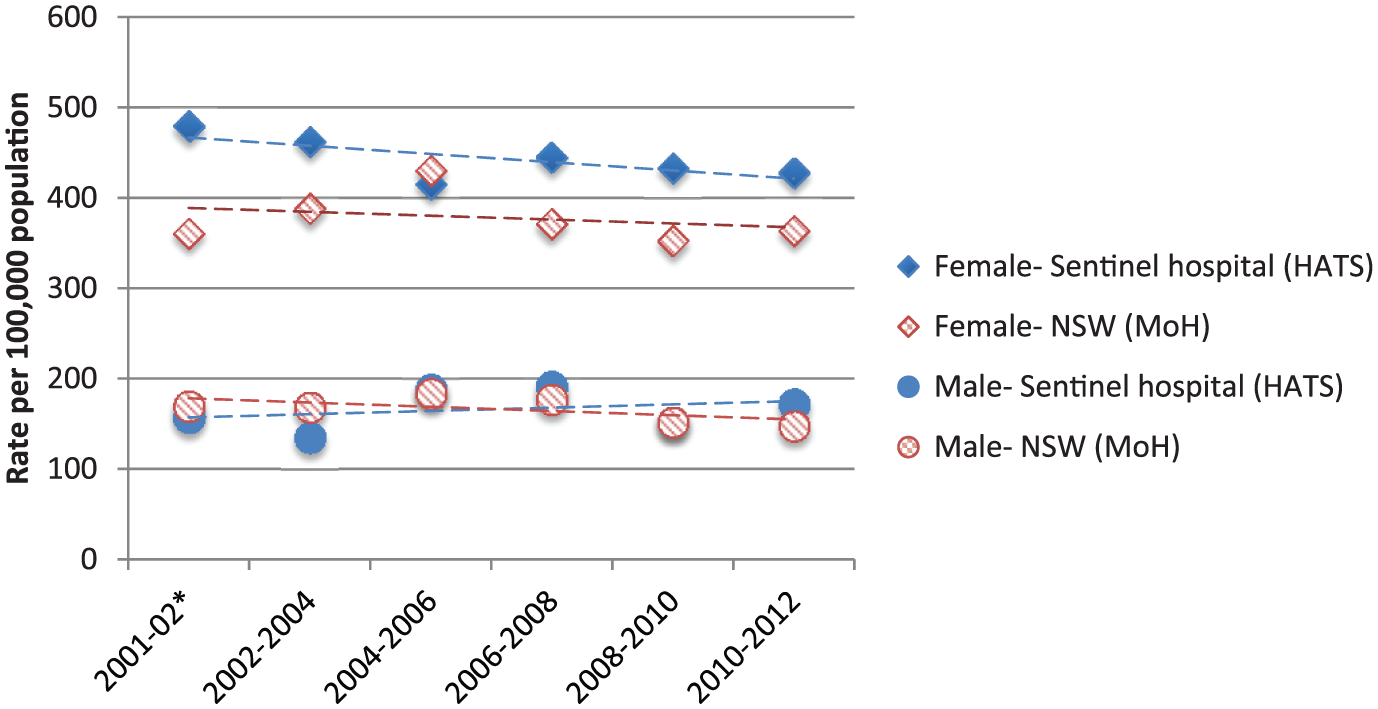
Rates for hospital-treated events by gender for the 15- to 24-year age group for sentinel hospital (intentional self-poisoning) and New South Wales (self-harm).
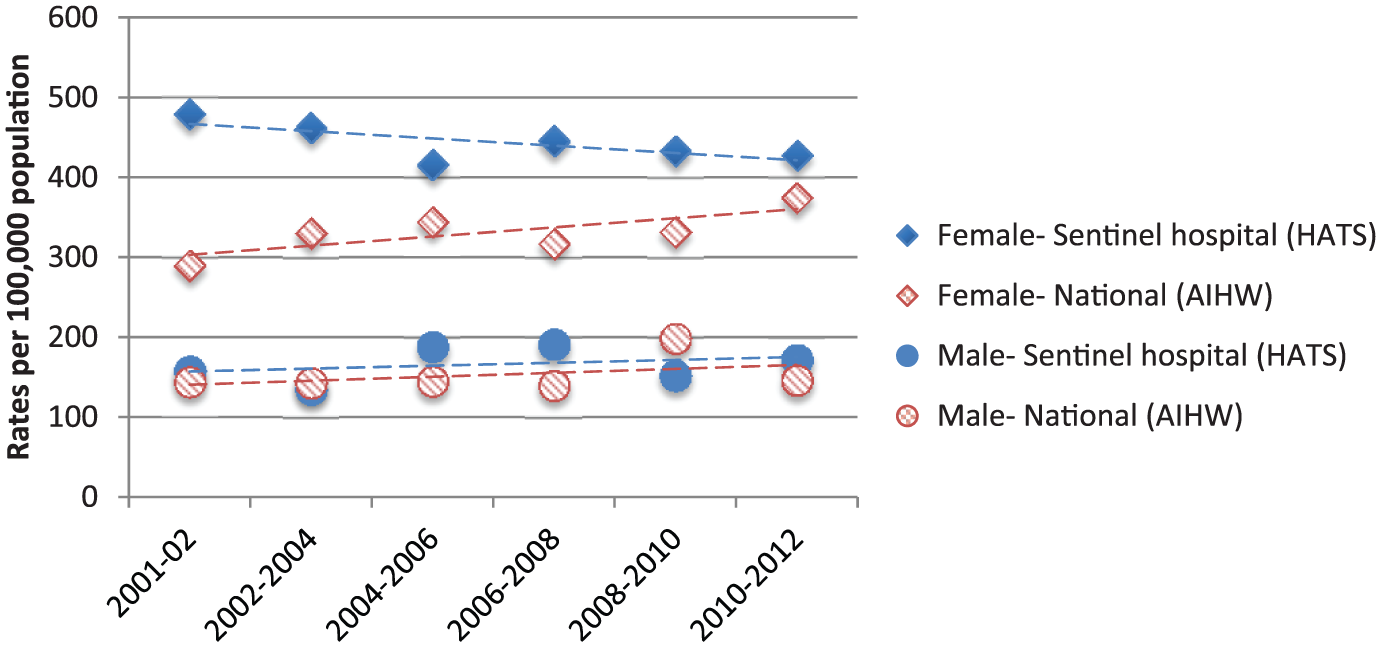
Rates for hospital-treated events by gender for the 15- to 24-year age group for sentinel hospital (intentional self-poisoning) and national data (self-harm).
Discussion
Main findings
While, as expected, females were found to have much higher event rates of hospital-treated self-harm than males across all data sources, the reported increase in the national event rate for hospital-treated self-harm for young females was not apparent within the sentinel hospital, the local health district or the NSW state data. Furthermore, event rates for females in the 15- to 24-year age group were consistently and substantially higher in the sentinel hospital (and the local health district) than the national and state rates. These findings have a number of implications.
First, these data provide a foundation from which a best estimate for the actual rate of hospital-presenting self-harm rates can be made. The sentinel hospital event rates are limited to intentional self-poisoning but reflect data for all presentations for which there was a consistent admission and coding policy within a known catchment area throughout the time period of interest. The local health district rates provided by the MoH are somewhat higher than the sentinel unit rates because the sentinel data comprise the major intentional self-poisoning component of the local health district data, whereas the local health district rates also include non-poisoning self-harm (i.e. self-injury) admission event rates and cover a broader geographical catchment area. Thus, while the local health district rates will still be underestimated, the magnitude will be much less than for other institutional data.
Arguably, the Hunter New England local health district rates may not be representative of the national rates and perhaps this health district has real rates of much greater magnitude than nationally. It was not the aim of this paper to evaluate the impact of variations in catchment area population characteristics on rates of hospital-treated self-harm and therefore HATS rates cannot be directly extrapolated to other populations in NSW or Australia. However, the reported rates were generally age and gender standardised, which account for variations in the underlying age and gender structure of the populations. Generally, we would expect some variation by metropolitan, regional and small hospital centres and by population characteristics like socio-economic level. However, we would suggest that the considerable disparity between sentinel and national rates might well be a consequence of artefactual error (reflecting lower admission rates which do not account for presentations treated entirely within the ED and/or less accurate coding of admissions across hospitals nationally), the implication being that the reported increases could be easily accounted for by small changes in admission rates by clinicians or improved coding of suicidal behaviour by administration staff during the study period.
The reported increases in ED presentations (event rates) are more difficult to compare directly because of the different time periods, age groups and definitions used and the combination of male and female data. For NSW (10–19 years), it was reported that for 2012 the rates for self-harm were 150 per 100,000 and those for intentional self-poisoning were 65 per 100,000 (estimated from published figures), which were substantially below the rates (for 15–24 years) in the Hunter New England local health district and the sentinel hospital. This also suggests a major underestimate in the ED presentation data and reported increases in rates could be accounted for by improved coding alone.
It is also important to note that neither the local health district nor state data showed any specific increases in rates of young females’ self-harm during the study period. The increase identified in the national data would have to have been a consequence of increases in rates within other states and territories and of a magnitude that they would impact the national rates despite the stability of the rates in the most populous state in Australia. Taken together, these findings suggest that hospital-presenting intentional self-poisoning rates, at least within NSW, are stable, with other factors accounting for the apparent increases in the national data.
Second, the stability of rates over time for the sentinel hospital highlights the possibility that any rate changes identified at the national level may also be due to increased presentations of non-poisoning self-harm, such as cutting, burning, scratching or other forms of self-injury. The AIHW have begun to explore this as a possibility and in their most recent report noted that the recent increase in rates of self-harm for females appeared to be due to an increase in presentations for self-harm as a result of contact with a sharp object; however, they did not explore this with regard to age group (Harrison and Henley, 2014). A recent similar investigation of increasing hospital admissions for suicidal behaviour (including admissions for intentional self-harm and suicidal ideation) in the Northern Territory showed that there had been a specific and substantial increase in hospitalisation for self-harm for Indigenous people and that cutting was the method that had shown the greatest average percentage increase over time, with intentional self-poisoning showing little change in rate of presentation (Leckning et al., 2016). However, it is unclear whether these changes were due to real changes in numbers of presentations to hospital or changes in admission procedures or improvements in coding accuracy. It should be recognised that community self-harm is more common than hospital-treated self-harm and that self-injury is the more common type in community populations (RANZCP, 2015). A small percentage change in patient behaviour, that is, increased presentation for hospital treatment by community self-injury populations, could account for an increase in self-injury presentations at the ED. In the United Kingdom, where sentinel monitoring is reported in key geographical areas (Oxford, Manchester, Derby), there has been a confirmed increase in self-harm noted since 2007 (Geulayov et al., 2016).
Third, this study has highlighted the role that local data can play in understanding outcomes identified in aggregated data and emphasises the need for quality, accessible, timely information. When comparing rates, it is clear that there is wide variation. Nationally, rates for hospital-treated self-harm vary by state from 97 per 100,000 to 151 per 100,000 (AIHW, 2012), as well as varying within states, between primary health network regions and within regions, with increasing remoteness being associated with increasing rates (AIHW, 2016; Harrison and Henley, 2014; Pointer, 2015). Being able to unpack and understand the factors that underpin local rates is essential to being able to plan for and put in place systems and services that will be able to address a community’s needs. This can only be done if data monitoring systems accurately capture presentation data. The establishment of improved surveillance, monitoring and information systems that collect regional data on intentional self-harm is recommended in the Royal Australian and New Zealand College of Psychiatrists’ recent clinical practice guideline for the management of deliberate self-harm (RANZCP, 2015) and this study highlights the ongoing need for a sentinel monitoring system.
Furthermore, the stability of the rates reported at the sentinel hospital, local health district and state level in this study is consistent with the conclusions drawn from systematic reviews on the prevalence of self-harm, which have identified that rates of self-harm have been relatively stable and disparity or changes in rates over time appear more likely due to methodological factors (such as how self-harm is measured) rather than changes in actual prevalence (Muehlenkamp et al., 2012; Swannell et al., 2014). This also highlights the need for monitoring systems that are accurate and timely. A system of sentinel units from carefully selected regions across the country could be combined to provide estimates at the national level that would complement the current institutional national data.
Policy and practice implications
These findings have important policy and practice implications. They highlight the role that sentinel units can play in providing comparison points for aggregated data. In addition to the capacity to provide reliable, accurate, timely and regionally relevant data monitoring, sentinel unit surveillance provides a much stronger foundation from which self-harm risk factors can be understood, clinical management patterns explored and effectiveness of interventions tested, because they can track individuals over time and collect additional demographic and clinical information relevant to the episode of care provided. As the AIHW have started to do, the findings flag the need to identify the degree to which any increases are due to rises in presentations of other types of self-harm, particularly cutting. If cutting (or another self-injury method) accounted for the apparent increases in rates in young females, it would be opportune to specifically consider and identify how hospitals can best manage these presentations and the nature of the most effective type of aftercare. Finally, the findings are a reminder to our own local health services as to the importance of considering what can be done to reduce the rate of intentional self-poisoning among young females (as the rate remains substantially higher than males) and of the need to continue to look for possible ways to enhance current services and systems supports.
Limitations
This study would have been strengthened through access to the national and state-level raw data or to more segmented versions of the aggregated data. Furthermore, the study relied on data from a sentinel unit for intentional self-poisoning (rather than self-harm more generally) and used data available in the public domain as comparators. These factors meant that analyses were limited to the degree to which the data were comparable and the sorts of conclusions that could be drawn specifically about intentional self-poisoning or self-injury or more generically self-harm. Having additional local comparison points with known referral populations and management strategies would have further strengthened the conclusions of this study.
Conclusion
The findings from this study suggest that it is unlikely that reported increases in rates of self-harm among young females are due to increases in rates of intentional self-poisoning among this age and gender group. It will be important to further investigate the degree to which increases are due to changes in non-poisoning self-harm presentations, that is, self-injury, or to changes in hospital clinical management or administrative coding of self-harm. This study highlights the importance of establishing a system of sentinel units for monitoring and comparison purposes and ensuring that health service planning and policy development is based on best estimates of the true rates.
Footnotes
Acknowledgements
We thank Prof. Nicholas Buckley for his comments on an earlier version of this manuscript.
Declaration of Conflicting Interests
Professors GL Carter and I Whyte have management and clinical responsibilities for patients seen through the Hunter Area Toxicology Service. Carter was Chair of the Royal Australian and New Zealand College of Psychiatry Clinical Practice Guidelines for Deliberate Self-Harm. The opinions expressed do not represent the opinions of the Calvary Mater Newcastle hospital or the Royal Australian and New Zealand College of Psychiatry.
Funding
K. McGill’s position was funded by the Burdekin Suicide Prevention Programme and administered by Hunter New England Mental Health Services.