
Abstract
Objective:
Prior and repeated self-harm hospitalisations are common risk factors for suicide. However, few studies have accounted for pre-existing comorbidities and prior hospital use when quantifying the burden of self-harm. The aim is to quantify hospitalisation in the 12 months preceding and re-hospitalisation and mortality risk in the 12 months post a self-harm hospitalisation.
Method:
A population-based matched cohort using linked hospital and mortality data for individuals ⩾18 years from four Australian jurisdictions. A non-injured comparison cohort was matched on age, gender and residential postcode. Twelve-month pre- and post-index self-harm hospitalisations and mortality were examined.
Results:
The 11,597 individuals who were hospitalised following self-harm in 2009 experienced 21% higher health service use in the 12 months pre and post the index admission and a higher mortality rate (2.9% vs 0.3%) than their matched counterparts. There were 133 (39.0%) deaths within 2 weeks of hospital discharge and 342 deaths within 12 months of the index hospitalisation in the self-harm cohort. Adjusted rate ratios for hospital readmission were highest for females (2.86; 95% confidence interval: [2.33, 2.52]) and individuals aged 55–64 years (3.96; 95% confidence interval: [2.79, 5.64]).
Conclusion:
Improved quantification of the burden of self-harm-related hospital use can inform resource allocation for intervention and after-care services for individuals at risk of repeated self-harm. Better assessment of at-risk self-harm behaviour, appropriate referrals and improved post-discharge care, focusing on care continuity, are needed.
Introduction
Self-harm has been an increasing cause of hospitalisation and mortality in high-income countries over the past decade (Haagsma et al., 2016). More than 800,000 individuals die due to suicide each year worldwide (World Health Organization, 2017). In Australia, there were 2282 suicides in 2010–2011 and an estimated 27,000 hospitalisations following self-harm annually (Harrison and Henley, 2014). For each completed suicide, there can be up to an estimated 10–40 suicide attempts (Haukka et al., 2008; Tidemalm et al., 2008). Evidence suggests that between 12% and 33% of self-harm attempts are repeated at 1 year after an initial occurrence (Gilbody et al., 1997; Hassanyeh et al., 1989; Lilley et al., 2008) and that prior self-harm is a common risk factor for suicide (Bickley et al., 2013; Haukka et al., 2008; Perry et al., 2012; Singhal et al., 2014), with up to one-quarter of suicides preceded by a prior self-harm event (Owens et al., 2002).
Examining repeated self-harm episodes can assist in clarifying patterns of self-harm behaviour over time, in identifying opportunities for intervention and post-discharge after care, including continuity of care, and in quantifying the burden of self-harm on the health care system (Bickley et al., 2013; Owens et al., 2002; Perry et al., 2012). A limited number of studies have taken into account the influence of pre-existing comorbid conditions and previous hospital use when attempting to quantify the burden of self-harm hospitalisations (Singhal et al., 2014). In the main, efforts to examine the burden and determine the risk of re-hospitalisation and mortality after a self-harm hospitalisation have largely involved small case–control studies involving a few hospitals (Bickley et al., 2013; Hunt et al., 2009; Zahl and Hawton, 2004) or hospital-based comparison cohorts (Singhal et al., 2014). No prior population-based studies of repeat health service use post a self-harm hospitalisation have included a comparison cohort drawn from the general population and neither have previous studies examined hospital use in the 12 months prior to the index self-harm hospitalisation. This study aims to quantify hospitalisation in the 12 months preceding and re-hospitalisation and mortality risk in the 12 months post a self-harm hospital admission using a population-based matched cohort design.
Materials and methods
Study design
The study design was a population-based matched cohort study of individuals aged ⩾18 years using probabilistically linked emergency department (ED), hospitalisation and mortality records from four Australian states during 1 January 2008 to 31 December 2010. Ethical approval was obtained from Human Research Ethics Committees associated with each health department. The study method has been described elsewhere (Mitchell et al., 2016) and is summarised here.
Data sources
Hospitalisation records included all inpatient admissions from all public and private hospitals in New South Wales and Queensland and from public hospitals in South Australia and Tasmania. The hospitalisation record contains information on patient demographics, diagnoses, external cause(s), procedures and type of hospitalisation. Diagnoses and external cause codes were classified using the International Classification of Diseases, 10th Revision, Australian Modification (ICD-10-AM) (National Centre for Classification in Health, 2006). ED presentations were only available for public hospitals. Mortality data were obtained from each jurisdiction’s Registry of Births, Deaths and Marriages.
Self-harm index hospitalisation and non-injured comparison cohorts
The first self-harm hospitalisation (i.e. the index hospitalisation) was identified using a principal diagnosis of injury (ICD-10-AM: S00-T75 or T79) and an external cause of self-harm (ICD-10-AM: X60-X84) in 2009. Self-harm was defined as ‘purposely self-inflicted poisoning or injury suicide (attempted)’ (National Centre for Classification in Health, 2006). A non-injured comparison cohort was randomly selected using each jurisdiction’s electoral roll for individuals who were not hospitalised with an injury in 2009. As it is compulsory to vote in Australia, most individuals aged ⩾18 years should be registered on an electoral roll. The non-injured cohort were matched 1:1 on age, gender and postcode of residence at the date of the index self-harm admission of their matched counterpart. All ED presentations, hospital admissions and mortality records for the self-harm and non-injured cohorts were obtained for the period 1 January 2008 to 31 December 2010.
Comorbidity identification
The Charlson Comorbidity Index (Quan et al., 2011) was used to identify comorbidities from hospital diagnosis classifications using a 12-month look-back period from the admission date of the index self-harm admission for both the self-harm and the matched non-injured cohort. Comorbidities were categorised as none, mild-moderate (1–2) and severe (⩾3). Mental health conditions (ICD-10-AM: F20-F50), alcohol misuse and dependence (ICD-10-AM: F10, Y90, Y91, Z50.2, Z71.4, Z72.1) and drug-related dependence (ICD-10-AM: F11-F16, F19, Z50.3, Z71.5, Z72.2), all factors associated with self-harm risk (Skegg, 2005), were also identified using diagnosis classifications.
Urban and rural identification
The Australian Statistical Geographical Standard Remoteness Area (Australian Bureau of Statistics, 2011) was used to identify rural and urban residents. Remoteness is derived based on distance to service centres, and the five remoteness categories were collapsed into urban (i.e. major cities) and rural (i.e. inner regional, outer regional, remote and very remote).
Pre-existing health service use, readmission and mortality
Hospitalisations 12 months preceding and 12 months post the index self-harm hospital admission were identified for both the self-harm cases and their non-injured counterparts. Prior and subsequent hospitalisations for self-harm (ICD-10-AM: X60-X84), unintentional poisoning (ICD-10-AM: X40-X59), undetermined intent injuries (ICD-10-AM: Y10-Y34) and mental and behaviour disorders (ICD-10-AM: F00-F99) and injuries (ICD-10-AM: S00-T98) were identified using external cause codes and principal diagnoses, respectively. The total hospital length of stay (LOS) in the 12 months preceding and subsequent to the index self-harm admission was calculated for both the self-harm and matched non-injured cohort. Hospital readmission was defined as readmission within 12 months of the index injury hospital discharge for any cause. Twelve-month mortality was calculated from the admission date of the index self-harm admission for both the self-harm cohort and their matched counterpart. All individuals were followed either to death or to the end date of the study timeframe (up to 365 days following the index self-harm admission). Cause of mortality was identified using the underlying cause and up to 20 antecedent cause-of-death fields. Self-harm deaths were considered to be any deaths categorised as self-harm (ICD-10: X60-X84), unintentional poisoning (ICD-10: X40-X59) or undetermined intent injuries (ICD-10: Y10-Y34) in order to avoid underestimating mortality due to self-harm (Zahl and Hawton, 2004).
Person-time at risk
Where an individual died within 12 months of the index self-harm hospitalisation, survival time post the index hospitalisation was calculated by subtracting the date of the index hospital admission from the date of death for those who self-harmed and their matched counterpart. Person-time at risk was calculated each month for 12 months post the date of the index hospitalisation for both the self-harm and non-injured comparison cohort (excluding deaths). Mortality per 1000 patient-years was also calculated.
Data management and analysis
All analyses were performed using SAS version 9.4 (SAS Institute, 2014). All hospital episodes of care related to one hospital admission were linked to form a single period of care. Descriptive statistics were conducted, and chi-square tests of independence compared the characteristics of individuals hospitalised following self-harm with the comparison cohort.
Negative binomial regression was used to quantify associations between self-harm and counts of hospital admissions 12 months post the index hospitalisation using rate ratios and 95% confidence intervals (95% CIs). Variables included in the final model were age group, sex, urban status, number of Charlson comorbidities (i.e. 0, 1–2 or ⩾3), alcohol use and dependence (Y/N), mental health conditions (Y/N), drug-related dependence (Y/N) and log of pre-injury cumulative hospital LOS, with person-time included as an offset. Matching variables were included in the model to control for any possible confounding from matching variables (Pearce, 2016). The attributable risk percent (AR%) was calculated by subtracting 1 from the adjusted rate ratio (ARR), divided by the ARR, multiplied by 100 (Woodward, 2005). Rates of hospitalisations were calculated by month, accounting for person-time at risk, in the 12 months before and after the date of the index hospitalisation for both the self-harm and non-injured cohorts.
Results
Cohort characteristics
There were 11,597 individuals who were hospitalised in 2009 following self-harm, with a mean age of 38.6 years (standard deviation [SD] = 14.9). Females accounted for 57.6% of those hospitalised following self-harm, with 68.2% of individuals aged between 18 and 44 years. Sixty-six percent of those who self-harmed resided in an urban setting. The majority of self-harm injuries involved self-poisoning (83.3%), and the self-harm cohort had a mean hospital LOS of 5.7 days (SD = 15.9). The self-harm cohort had a higher proportion of Charlson comorbidities, mental health diagnoses, alcohol misuse and drug-related dependence than their matched counterparts (Table 1). Of the individuals who were hospitalised following self-harm, 3262 (28.1%) had a diagnosis of anxiety-related disorders, 2669 (23.0%) depression, 703 (6.1%) schizophrenia, 597 (5.2%) bipolar disorder and 364 (3.1%) neurological disorders.
Demographic characteristics of self-harm hospitalisations of individuals aged 18+ years and matched non-injured comparison cohort in 2009, linked hospitalisation data in Australia.
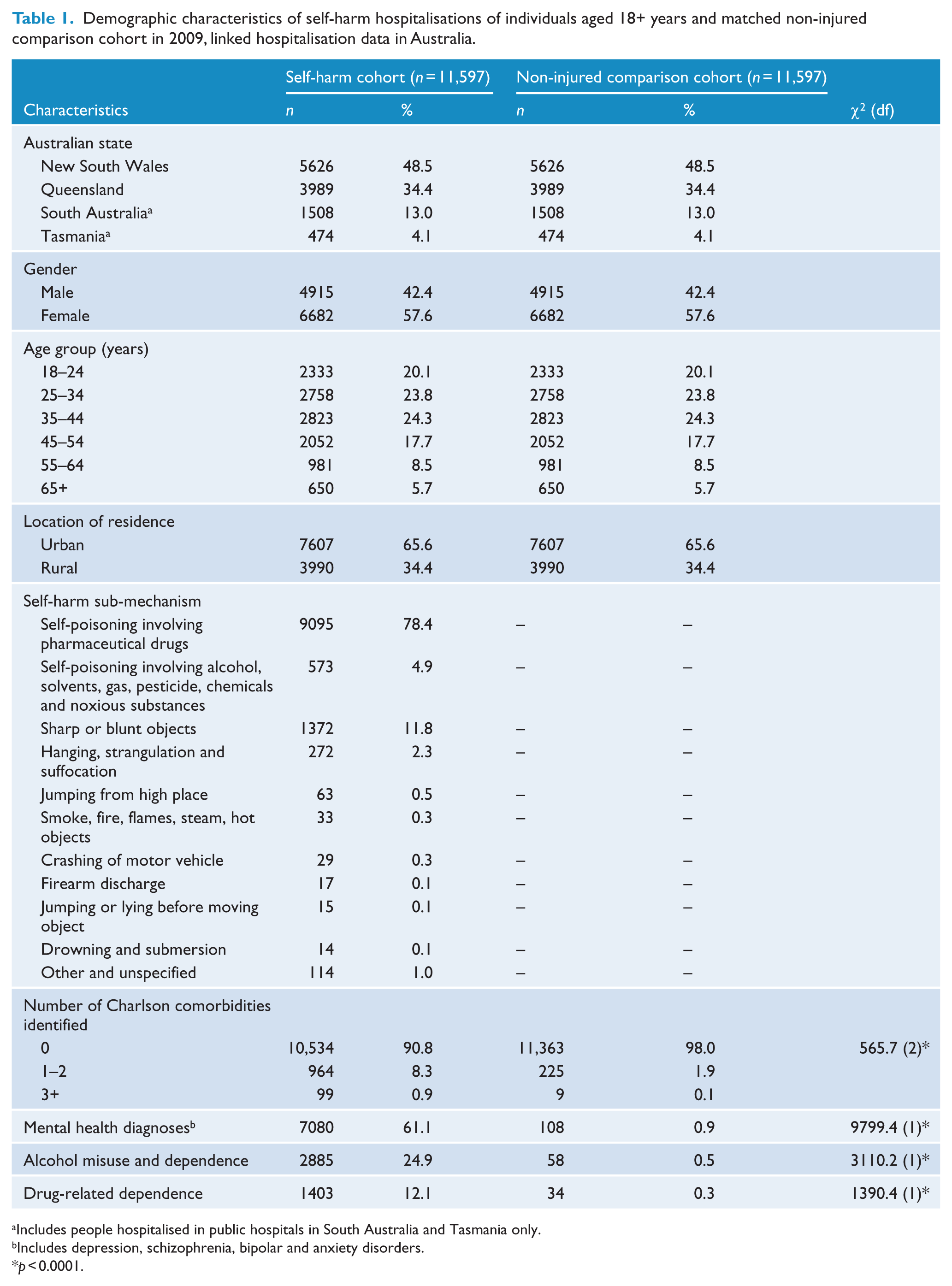
Includes people hospitalised in public hospitals in South Australia and Tasmania only.
Includes depression, schizophrenia, bipolar and anxiety disorders.
p < 0.0001.
Health service use 12 months pre and post the index admission
The self-harm cohort experienced a higher proportion of health service use in the 12 months pre (20.5% vs 10.1%) and post (21.2% vs 10.6%) the index admission and a higher mortality rate (2.9% vs 0.3%) than their matched counterparts (Table 2). For the individuals in the self-harm cohort who had a hospital admission preceding the index hospitalisation, 2042 (38.9%) and 815 (15.5%) of the principal diagnoses of the hospital admission immediately preceding the index admission were for mental and behavioural disorders and injuries, respectively. Sixty-two percent of external cause codes of the hospital admission immediately preceding the index admission were for self-harm (52.3%), unintentional poisoning (4.9%) or the intent was undetermined (5.2%). Of the individuals in the self-harm cohort with multiple hospital admissions prior to the index admission, 1109 prior admissions had an external cause of self-harm, 213 of unintentional poisoning and 171 were classified as undetermined intent.
ED and hospital admission characteristics and 12-month mortality of self-harm hospitalisations of individuals aged 18+ years and matched non-injured comparison cohort 12 months pre and post the index self-harm hospitalisation, linked ED presentation, hospitalisation and mortality data in Australia.
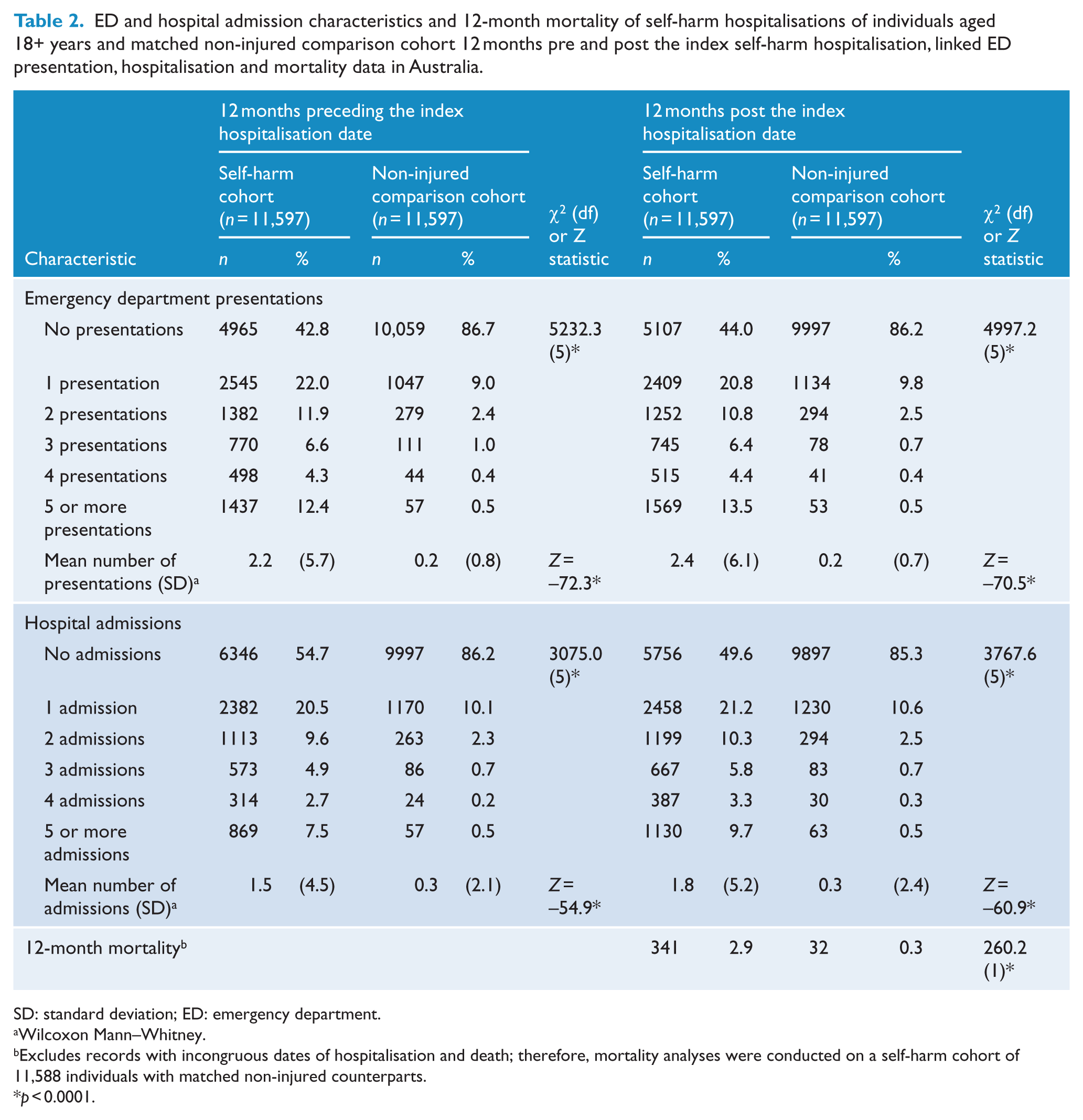
SD: standard deviation; ED: emergency department.
Wilcoxon Mann–Whitney.
Excludes records with incongruous dates of hospitalisation and death; therefore, mortality analyses were conducted on a self-harm cohort of 11,588 individuals with matched non-injured counterparts.
p < 0.0001.
For the individuals in the self-harm cohort who had a hospital admission post the index hospitalisation, 2311 (39.6%) and 1607 (27.6%) of the principal diagnoses of the first hospital admission immediately post the index admission were for mental and behavioural disorders and injuries, respectively. Sixty-eight percent of external cause codes of the hospital admission immediately post the index admission were for self-harm, unintentional poisoning or the intent was undetermined (i.e. 60.0%, 4.2% and 4.1%, respectively). Of the individuals in the self-harm cohort with multiple admissions post the self-harm index admission, 1995 of these admissions had an external cause of self-harm, 301 of unintentional poisoning and 228 were classified as undetermined intent. The hospital admission rates per 100 person-months 12 months pre and post the index hospitalisation were highest for the self-harm cohort, particularly in the first 24 months following the index admission (Figure 1).
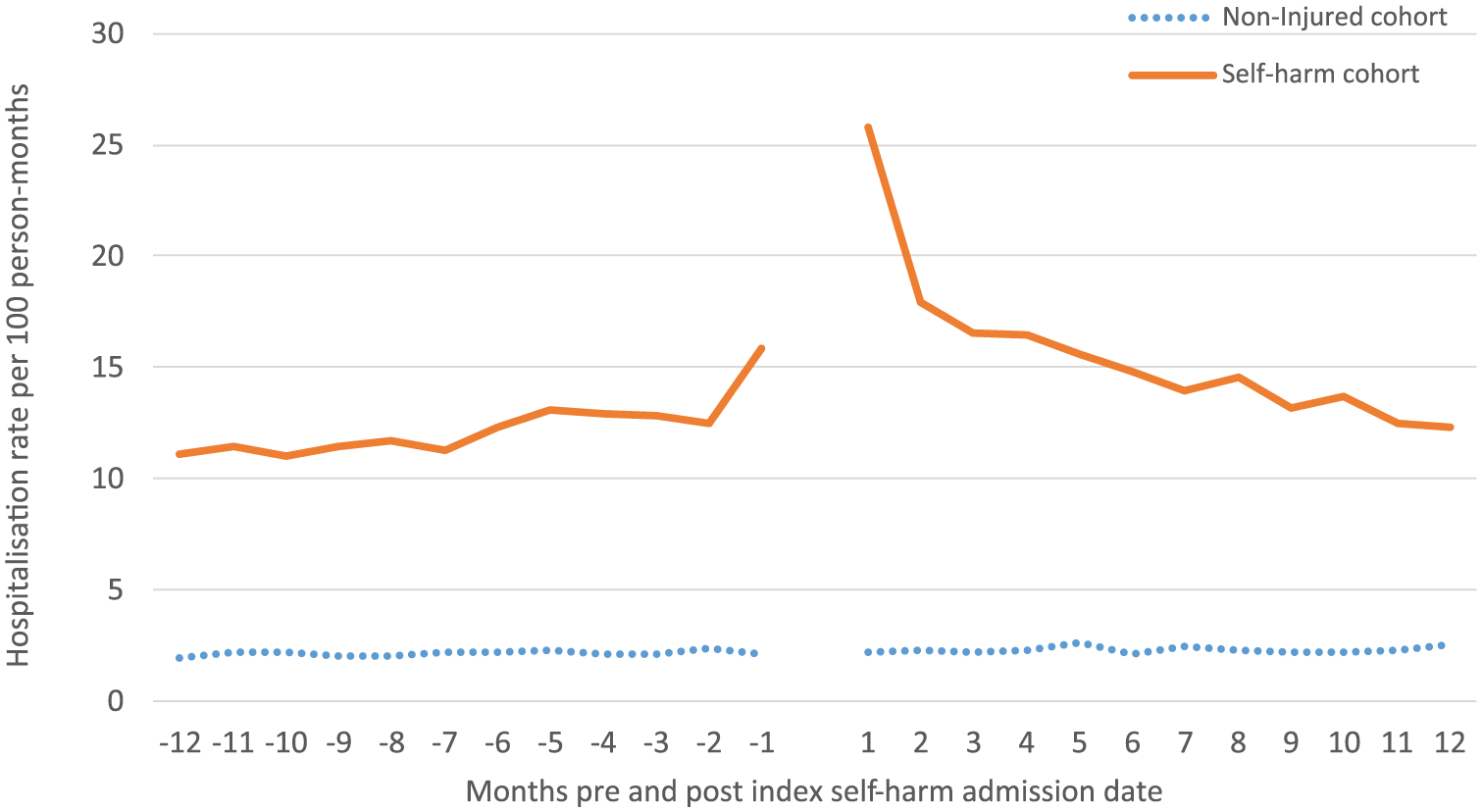
Hospitalisation rates per 100 person-months 12 months pre and post the index self-harm hospital admission by month for injured and non-injured comparison group, linked hospitalisation and mortality data in Australia.
Hospital readmission rate ratios 12 months post the index admission
The number of days spent in hospital subsequent to the index hospitalisation was highest for females and individuals aged 25–34 years. The ARRs for hospital readmission were highest for females (ARR: 2.86; 95% CI: [2.33, 3.52]) and individuals aged 55–64 years (ARR: 3.96; 95% CI: [2.79, 5.64]) and lowest for individuals aged 35–44 years (ARR: 2.26; 95% CI: [1.53, 3.34]). The proportion of attributable hospital readmissions in the 12 months post the index admission ranged from 56% to 75% by age group (Table 3).
Cumulative days spent in hospital and rate ratios of hospital admissions for individuals aged 18+ years and matched non-injured comparison cohort within 12 months post the index self-harm hospitalisation, linked hospitalisation and mortality data in Australia.
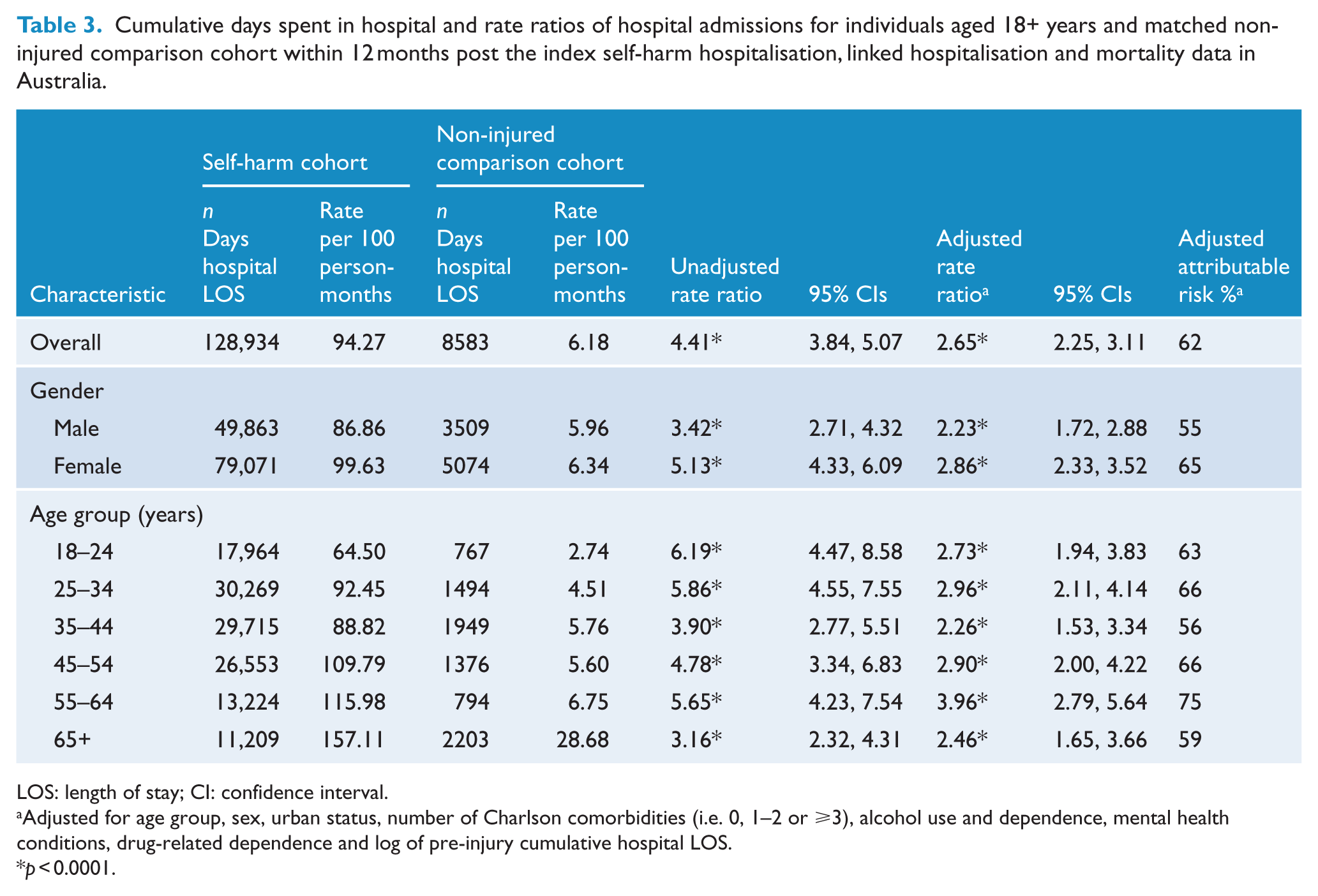
LOS: length of stay; CI: confidence interval.
Adjusted for age group, sex, urban status, number of Charlson comorbidities (i.e. 0, 1–2 or ⩾3), alcohol use and dependence, mental health conditions, drug-related dependence and log of pre-injury cumulative hospital LOS.
p < 0.0001.
Mortality 12-months post the index admission
Mortality in the 12 months post the index hospitalisation was higher for the self-harm compared to the non-injured cohort, particularly in the first month following the index admission (Figure 2). There were 373 deaths in the 12 months post the index hospitalisation: 341 in the self-harm cohort and 32 in the comparison cohort. Of the deaths in the self-harm cohort, 70.4% had self-harm, unintentional poisoning or an undetermined intent cause of death recorded (i.e. 46.0%, 14.1% and 10.3%, respectively). There were 133 (39.0%) deaths in the self-harm cohort within 2 weeks of hospital discharge. Of these, 89 were specified as due to self-harm (71.9%), unintentional poisoning (19.1%) or of an undetermined intent (9.0%). Mortality per 1000 patient-years for the self-harm cohort was 32.02 and for the non-injured cohort was 2.94.
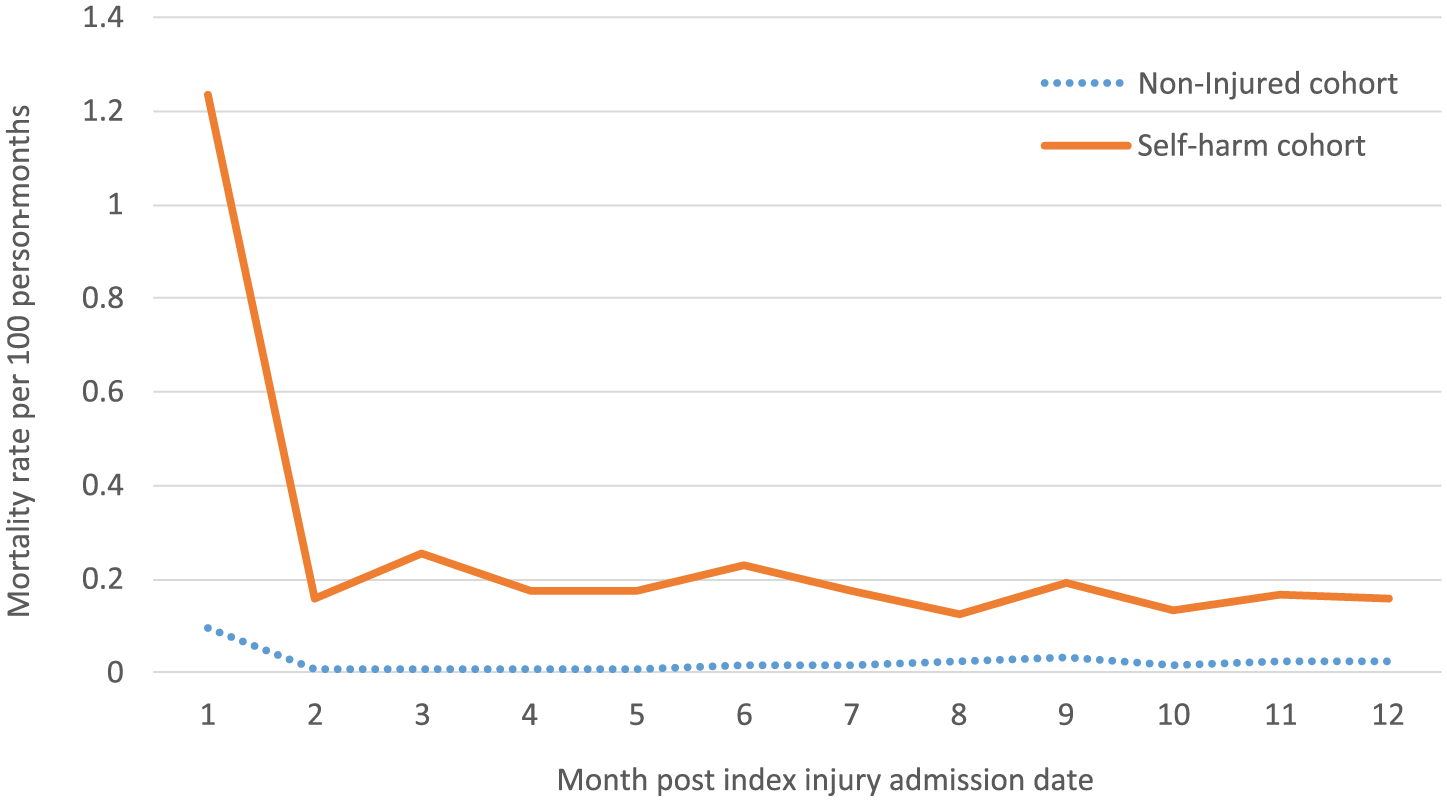
Mortality rates per 100 person-months 12 months pre and post the index self-harm hospital admission by month for injured and non-injured comparison group, linked hospitalisation and mortality data in Australia.
Discussion
This study quantified hospital admissions in the 12 months preceding and re-hospitalisation and mortality risk in the 12 months after a self-harm hospitalisation using a population-based matched cohort from the general population and after adjusting for pre-existing comorbidities. This study identified that the self-harm cohort had a higher rate of hospital admissions pre and post the index hospitalisation and that they had worse survival at 12 months after their index admission than their matched counterparts. The self-harm cohort had more than double the rate of hospital readmissions in the 12 months post the index hospitalisation compared to their matched comparisons, even after adjusting for the number of comorbidities, mental health conditions, alcohol misuse and dependence, and drug-related dependence. The adjusted attributable risk identified that between 55% and 75% of the post-index hospitalisations were likely to be related to the index admission after taking into account comorbid health conditions, with the attributable risk proportion fluctuating with age.
Hospitalisations pre- and post-index self-harm admission
Twenty-one percent of the self-harm cohort had a hospital admission in the 12 months preceding and 21% of the self-harm cohort had a hospital admission in the 12 months after the index hospitalisation. Of these, at least 52.3% and 60.0% of these pre- and post-index admissions, respectively, were for self-harm, with just less than 10% of each of these admissions recorded as unintentional poisoning or undetermined intent. Previous research has identified around 22% of ED re-presentations (Perry et al., 2012), and 16% of hospital readmissions (Owens et al., 2002) were for repeat self-harm events. However, a limitation of prior research has been that it largely only considered readmission to the same hospital (Owens et al., 2002), so it may have underestimated hospital readmissions.
Mortality risk
The self-harm cohort had higher mortality, particularly within the first month post the index admission, with over one-third of deaths in the self-harm cohort occurring in the first 2 weeks after discharge and with two-thirds of these deaths recorded as self-harm, unintentional poisoning or of undetermined intent. Likewise, studies of mortality risk among psychiatric patients have identified a high self-harm risk in the first few weeks post-discharge (Bickley et al., 2013; Goldacre et al., 1993), suggesting that discharge was likely to have been premature despite apparent recovery (Bickley et al., 2013).
Determination of intent
The determination of intent is not always straightforward for either hospital or mortality records. To avoid underestimating mortality due to self-harm, deaths due to self-harm, unintentional poisoning and deaths of undetermined intent for the self-harm cohort were reported together in this study as has been conducted previously (Zahl and Hawton, 2004). In the same vein, hospital readmissions following the index admission, classified as self-harm, unintentional poisoning or of undetermined intent, were also reported for the self-harm cohort. A prior study of poisoning-related mortality has suggested creating a category of ‘death from drug self-intoxication’ (DDSI) to try to establish better enumeration of all poisoning deaths, regardless of intent (Rockett et al., 2010). It may be that reporting hospitalisation relating to self-harm, unintentional poisoning and undetermined intent would result in better determination of likely self-harm-related hospitalisations, after a prior self-harm hospitalisation.
Strengths and limitation of using data linkage
This research used probabilistic data linkage to link ED presentation and mortality data to hospitalisation records. Records were linked based on identifying variables (such as name, address, date of birth, date of hospital admission/separation). Probabilistic linkage involves using probability weights to identify the strength of whether or not records are a true match. Records with probabilities within certain thresholds are considered to be a match and records outside the threshold are not considered to be a match. Problems can arise in trying to identify true matches when individuals have the same combination of identifying variables, such as the same name and date of hospital admission, or where one or more of the data variables that are being used to identify matches are missing. One of the strengths of probabilistic data linkage is that the probability weights can be modified, which adds flexibility in the matching process. However, as matching occurs based on probability weights, it has the potential to increase errors in identifying true matches (Clarke, 2004). Within this study, probabilities that were outside the matching threshold were clerically reviewed to determine whether they should be considered to be true matching records or not.
In Australia, hospitalisation data are based on episodes of care, with each hospital visit usually involving multiple episodes of care as an individual moves between phases of care within a hospital (eg. a patient moving from intensive care to a ward and then to rehabilitation would result in three episodes of care) or is transferred between hospitals. Data linkage allows all health records related to one individual to be flagged by giving each individual a unique study identifier. In this study, the unique identifier along with other information, such as admission and separation dates/times and mode of separation, from the hospital records was used to ‘link’ all the episodes of care related to one self-harm hospitalisation and to also identify subsequent and antecedent hospitalisations either related to self-harm or other causes. Using data linkage in this study has enabled the examination of the trajectory of health care use related to self-harm attempts for the population of four states in Australia.
Limitations
There were several limitations associated with this study. It is possible that self-harm is under-enumerated as some people may not indicate that they intended self-harm or may be unable to confirm their intent due to ambiguity of their motive or the nature of their injury (Tovell et al., 2012). This study only considered health service use in terms of hospital use, and it is possible that individuals may have also used other medical services, such as general practitioners. No private hospitalisation information was able to be obtained from two Australian states. However, 81% of hospitalisations that are injury-related occur at public hospitals in Australia (Australian Institute of Health and Welfare, 2015). It is possible that equity of access to health services may have played a role in whether an individual was admitted to hospital (Cryer and Langley, 2006), and this would have had an impact on both case and comparison cohort selection.
It is possible that there are people missing from the electoral roll, especially young people and older people who may be incapacitated (Mitchell et al., 2014), and this may have restricted the people able to be selected for the comparison cohort. The number of comorbidities identified is likely to be under-enumerated, as only health conditions that are relevant to the current hospital episode of care are reported in each hospital record. However, by using a 1-year look-back period, better estimates of the prevalence of comorbidities are likely to have been obtained (Preen et al., 2006). Data validity was not assessed, and it is possible there may be some misclassification in hospital or mortality records.
Clinical implications
Better quantification of the burden of self-harm-related hospital use can assist to inform resource allocation for intervention and after-care services for individuals at risk of repeated self-harm. Likewise, better enumeration of likely self-harm hospital readmissions is needed and could be conducted by reporting readmissions related to self-harm, unintentional poisoning and undetermined intent for individuals who have previously had a self-harm hospital admission. With at least 21% of the self-harm cohort having at least one hospital readmission following a prior self-harm hospitalisation and one-third of deaths in this cohort in first 2 weeks post-discharge, it is suggestive of the need for better assessment of at-risk self-harm behaviour, appropriate referrals and improved follow-up and post-discharge care (Bickley et al., 2013; Perry et al., 2012), with a focus on care continuity. The evidence for effective post-discharge interventions to prevent and/or reduce repeat hospital admission for self-harm is not clear-cut (Hetrick et al., 2016). Brief contact interventions, such as letters, postcards and telephone calls, show promise but are not likely to be as effective for individuals with long-term psychiatric problems (Milner et al., 2015). Individually targeted psychological or psychosocial interventions involving cognitive behavioural therapy or psychodynamic interpersonal therapy have been advocated (Carter et al., 2016; Hetrick et al., 2016).
Footnotes
Acknowledgements
The authors wish to thank the New South Wales (NSW) Ministry of Health, the Queensland Department of Health, the South Australian Department of Health and Ageing and the Tasmanian Department of Health and Human Services for providing access to their emergency department presentation and hospital admission data collections; the NSW, Queensland, South Australian and Tasmanian Registries of Births, Deaths and Marriages for providing access to mortality data; and the NSW, Queensland, South Australian and Tasmanian electoral commissions for providing access to their electoral rolls. The authors would also like to thank the Centre for Health Record Linkage (CHeReL), the Statistical Services Branch of the Queensland Department of Health, SA-NT DataLink, the Tasmanian Data Linkage Unit and the Centre for Data Linkage for conducting the record linkage.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The research was supported by the Population Health Research Network with funding from the Australian Government National Collaborative Research Infrastructure Strategy and the Western Australian Minister for Science and Innovation. C.M.C. was supported by a Public Health Fellowship (ID 428254) from the National Health and Medical Research Council (NHMRC) Australia.