
Abstract
Deliberate self-harm (DSH) is one of the top five causes of acute medical admissions to hospital for both men and women in the UK [1]. The most common subgroup of DSH, deliberate self-poisoning (DSP), has been estimated to account for up to 5% of all general hospital admissions in Australia [2]. The risk for death by suicide after presentation with DSH or attempted suicide has been reported as up to 300 times that of the general population [3–10]. The rate of suicide after DSH lies somewhere between 0.5% and 2% after 1 year and above 5% after 9 years [11]. A recent review of DSH studies reported that the suicide rate is highest in the first months after an episode of DSH but that risk for eventual suicide remains elevated in longer-term follow-up studies [1]. Moreover, DSH populations have also been reported to have increased mortality by causes other than suicide: all-cause death, death by disease or natural causes, uncertain or undetermined causes, accident and homicide [3],[5–7],[12–14].
Risk factors have been identified for early death following presentation with DSH. They include: male gender; older age; psychiatric illness (particularly schizophrenia, depression, bipolar disorder and substance related disorders); medical illness; and substance abuse [5], [6], [8], [15]. Specifically following self-poisoning, identified additional risk factors for completed suicide include: more than one previous suicide attempt; age; living alone; migrant status; and being widowed or separated [3], [16]. Men and women have different rates and time-trends of suicide and tend to use different methods, hence they perhaps should be treated as distinct groups [17].
Suicide prevention strategies rely in part on identification of high-risk clinical groups or individual risk factors for completed suicide, in order to target interventions. Our aims in the present study were to determine the risk factors for subsequent suicide, premature death and allcause death after an index presentation for deliberate or recreational self-poisoning.
Method
A prospective longitudinal cohort design was used. Follow-up was for the duration of the study, a maximum of 10 years. Subjects were identified from a clinical database maintained by the Hunter Area Toxicology Service (HATS), described in more detail elsewhere [18]. All admissions with deliberate or recreational self-poisoning from 1 January 1991 to 31 December, 2000 were selected and the first episode in the period was used as the index episode for all analyses. Transgender were excluded, as were patients who died prior to being discharged from hospital during their index admission.
Data linkage was performed with the National Death Index (NDI) of the Australian Institute of Health and Welfare (AIHW) for the survival analyses. The NDI contains mortality data provided from death certificates from the registrars of births, deaths and marriages in all Australian states and territories. Cause of death was recorded from the death certificate according to ICD-9 or ICD-10 [19]. The data from the NDI and the HATS database were matched by first name, last name, date of birth, maiden name and sex, using a probabilistic method. The NDI matching process has a reported sensitivity of 88.8% and specificity of 98.2% [20]. The data-linkage was performed for deaths occurring on or before 31 December, 2000.
The independent variables were:
Type of poisoning: deliberate or recreational, classified by emergency department staff and reviewed by HATS staff at a weekly review meeting;
Demographics: age, gender by patient self report;
Emergency department ratings by resident medical staff: history of lifetime and current substance dependence and/or abuse and previous ‘suicide attempt’ (from patient self-report and hospital records).
Psychiatric diagnoses: major DSM-IV categories (from initial DSM-III-R and DSM-IV data) [21]. Diagnoses were assigned by psychiatric staff after direct clinical assessment of the patient and these diagnoses were reviewed at a subsequent weekly meeting. Individual disorders were mapped to DSM-IV major diagnostic categories for analyses and reporting. Those cases not seen by the psychiatry service were excluded from the multivariate analysis as ‘missing data’. Absence of psychiatric assessment was examined as an independent variable.
Discharge destination: home, self-discharge, absconding, voluntary public psychiatric hospital, involuntary public psychiatric hospital, private psychiatric hospital, nursing home and other.
Three outcome (dependent) variables were determined:
suicide (defined by the authors from death certificate data);
premature death (suicide death plus accidental death, homicide and death from substance-related causes);
all-cause death (premature death plus death by natural causes). Cox proportional hazards modelling was used for both univariate and multivariate statistical tests using Stata® [22], [23]. Life-table and log-rank analyses were also performed. All independent variables were initially tested using univariate analysis and those variables significant at the p < 0.05 level were included in the multivariate analyses. The multivariate testing employed a backward stepwise technique. Results from the multivariate analysis were expressed as adjusted hazard ratios with 95% confidence intervals. Two variables identified by the literature review as strongly associated with subsequent suicide (substance dependence and/or abuse and ‘previous suicide attempt’), were included in the initial multivariate analysis for the suicide and premature death models. For suicide death, separate multivariate analyses were performed for men and women using the same strategy as above.
Age-standardized suicide and mortality rates and their respective 95% CIs for the cohort were calculated using data supplied by the AIHW, using Stata®. This data comprised death and suicide data for the time period 1991–2000 inclusive, and their corresponding population data.
The Hunter Area Research Ethics Committee and the AIHW ethics committee approved the research protocol.
Results
A total of 4121 eligible patients were identified in the database as of 31 December, 2000. For 16 of the putative matches, the death date had occurred before the discharge date and these patients were also excluded from the analysis, as these cases most likely represented mismatched data. This left 4105 patients in the cohort, of whom 228 (5.6%) subsequently died (all causes) during the period of follow-up (Table 1). One hundred and twenty-two patients (3.0%) died a premature death and 58 patients (1.4%) died from suicide. The failure curves for allcause death, premature death and suicide (Fig. 1) indicate that after 10 years of follow-up approximately 2% of patients committed suicide, approximately 5% died a premature death and approximately 11% died from all causes. Formal psychiatric assessment was performed on 3489 (85%) of the patients, 3347 (91%) of the deliberate self-poisonings and 142 (33%) of the recreational self-poisonings.
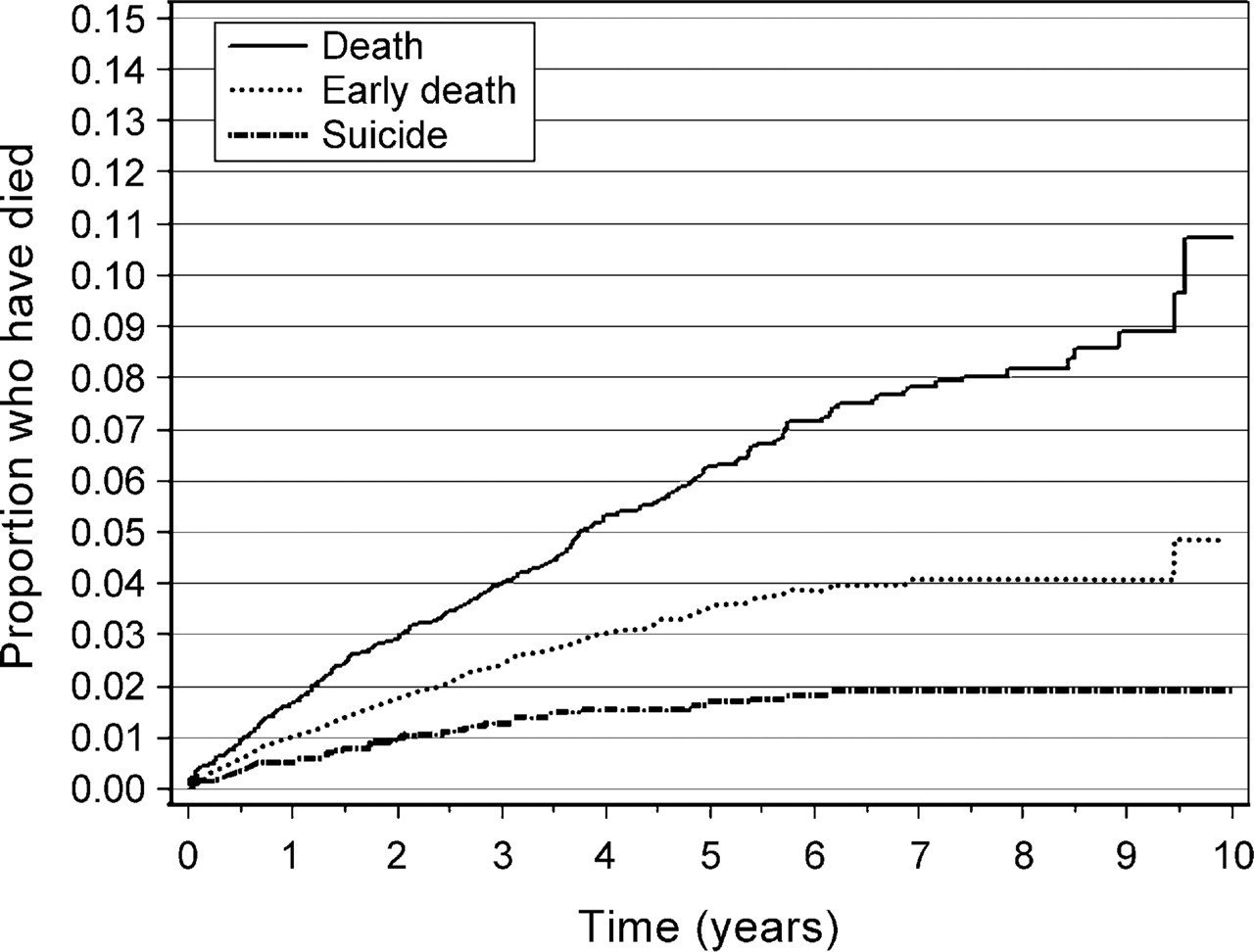
Failure curves for all-cause death, premature death and suicide.
Cause of death classifications by gender
Univariate risk factors and protective factors
The risk factors for death, early death and suicide are displayed in Table 2. Male gender, discharge to involuntary psychiatric hospital admission and absconding were risk factors for all three outcomes. Increasing age was a risk factor for suicide and all-cause death. ‘Disorders arising in infancy, childhood and adolescence’ and ‘schizophrenia and other psychoses’ were risk factors for both suicide and premature death. Recreational poisoning and substance misuse were risk factors only for premature death. Other conditions that may be a focus of clinical attention and discharge to home were associated with reduced risk for all three death outcomes.
Univariate risk factors, at index presentation, for all-cause death, premature death and suicide, hazard ratio (95% CI)
Post hoc analyses
Of 24 patients who absconded, four died, one from opioid dependency, two suicided by hanging and one suicided by jumping from a height. All these deaths occurred between one and two years after discharge. None of the nine patients discharged to gaol subsequently died, the deaths in the ‘other’ discharge destination occurring in those who were homeless or discharged to hostel accommodation. Of the six patients with ‘disorders arising in infancy childhood and adolescence’ who died, three had conduct disorder, two had a developmental disorder and one had attention deficit hyperactivity disorder. Of 18 additional patients who presented with accidental poisoning, four died, three by suicide. For accidental poisoning, the hazard ratio for suicide, compared with the study population, was 9.29 (95% CI = 2.93–29.42).
Multivariate analysis
Suicide
The significant risk factors in the final model were: ‘disorders arising in infancy childhood and adolescence’, 5.28 (95% CI = 2.04–13.65); male gender, 4.25 (95% CI = 2.21–8.14); discharge to involuntary psychiatric hospital admission, 3.20 (95% CI = 1.78–5.76); and increasing age, 1.02 (95% CI = 1.01–1.04). The significant protective factor was: ‘other conditions that may be a focus of clinical attention’, 0.19 (95% CI = 0.06–0.62).
For men the risk factors in the final model were: ‘disorders arising in infancy childhood and adolescence’, 5.35 (95% CI = 1.83–15.65); discharge to involuntary psychiatric hospital admission, 2.92 (95% CI = 1.50–5.70); and increasing age, 1.02 (95% CI = 1.00–1.04). The significant protective factor was: ‘other conditions that may be a focus of clinical attention’, 0.18 (95% CI = 0.04–0.73). For women the risk factors in the final model were: previous suicide attempts, 6.60 (95% CI = 1.43–30.37); discharge to involuntary psychiatric hospital admission, 3.88 (95% CI = 1.16–13.02); and increasing age, 1.03 (95% CI = 1.00–1.07).
Premature death
The risk factors in the final model were: other discharge destination, 4.88 (95% CI = 1.53–15.53); male gender, 3.54 (95% CI = 2.26–5.54); ‘disorders arising in infancy childhood and adolescence’, 2.24 (95% CI = 1.00–5.14); and discharge to involuntary psychiatric hospital admission, 1.77 (95% CI = 1.08–2.90). The significant protective factor was: ‘other conditions that may be a focus of clinical attention’, 0.20 (95% CI = 0.09–0.46).
All cause death
The risk factors in the final model were: male gender, 4.20 (95% CI = 2.18–8.06) and discharge to involuntary psychiatric hospital admission, 1.89 (95% CI = 0.89–4.01). The significant protective factors were: ‘other conditions that may be a focus of clinical attention’, 0.21 (95% CI = 0.07–0.68) and discharge home, 0.51 (95% CI = 0.25–1.05).
Suicide rates and standardized mortality ratios
The standardized all-cause mortality ratio was: for men, 6.42 (95% CI = 5.44–7.57); for women, 4.39 (95% CI = 3.56–5.41); and combined, 5.21 (95% CI = 4.58–5.93). The standardized suicide mortality ratio was: for men, 20.55 (95% CI = 15.24–27.73); for women, 22.95 (95% CI = 13.82–38.11); and combined, 19.42 (95% CI = 15.0–25.12).
Discussion
The advantage of the methodology of the present study is the ability to determine death and cause of death from an entire country for a cohort of patients originating in one geographical region. Patients who present with selfharm may be difficult to follow up over such a long period of time, hence the use of data-linkage between databases has enabled this longitudinal study to be carried out over a 10-year period. The main disadvantage is that some of the patients who died may have been missed by the matching process [20] but this may also happen with any study that utilizes death registries, and cohort studies in turn are often unable to track a significant proportion of patients. The use of death certificate data may also tend to underestimate the proportion of deaths that were suicide but this was partially overcome by analyzing early deaths in addition to suicides.
Although the literature is difficult to interpret, the suicide rates in the present study (projected as 2% over 10 years) are lower than those reported previously following self-harm [3–9],[24]. From previous reports, the median suicide rate after self-harm at 1 year is 1%, 3% for 1–5 years, 3% for 5–10 years and 7% for >10 years [1], [11]. The suicide rate in the first year after self-harm, has been reported as being 100-fold higher than the general population [1]. The HATS SMR for suicide was 19.42. The lower suicide rate in the present study may be due to the interventions used in the Hunter region, which include intensive psychiatric assessment and availability of follow-up [25]. This is supported by similar long-term suicide rates from a centre with a similar interest in patients with self-harm [26]. Alternatively the differences may be due to social, cultural or demographic differences between the present study and previous studies. A study performed in Denmark in patients who had presented with self-poisoning found a higher suicide rate and a ratio of male: female suicide closer to unity, than in the present study [3], but the background suicide rate for that population was also higher.
The HATS all-cause death rate of 5.5% for a mean follow-up period of 5 years was less than the reported rate in medically serious suicide attempters in New Zealand (8.9%) followed up for a 5-year period [24]. However, the HATS SMR for all cause death was 5.21, very similar to the nearly five times greater rate of observed to expected all-cause death in the New Zealand subjects.
‘Disorders arising in infancy childhood and adolescence’ has not previously been reported as a risk factor for suicide in this patient group. However, there is support from the literature for male gender, discharge to involuntary psychiatric hospital admission and increasing age as risk factors. Imprisonment has previously been described as a protective factor in men [9]. Factors that were not studied that have been implicated by previous studies include: migrant status [16]; planning of suicide attempt [8]; suicidal intent [4], [5]; and chronic somatic disease [27]. Other conditions that may be a focus of clinical attention were protective for all three outcomes even after controlling for confounders, including psychiatric comorbidity, in the models. This suggests that after psychiatric assessment, those subjects with uncomplicated ‘other conditions’ can be safely discharged from hospital with very low risk of death.
Neither drug and alcohol misuse (resident rating) nor substance related disorder (psychiatric diagnosis) was associated with any death outcome in the present study. Substance abuse has previously been found to be unrelated to the risk of subsequent suicide in patients who present with self-poisoning [3], although, drug abuse was a risk factor for all cause death, natural causes, accidents and uncertain cause of death. There have been reports of an association between narcotic abuse and subsequent suicide in Australian patients who have presented with self-harm [8], [28].
Risk factors for men and women are different [8]. Prior self-harm was a risk factor in women and the diagnosis of disorders in childhood was a significant risk factor in men. The first presentation at hospital for men may be important to detect and treat psychiatric disorders as a suicide prevention intervention. More ‘violent’ or ‘lethal’ methods of suicide, such as gunshot and hanging, are more common in men. In our study there were no deaths from gunshot, which is remarkable in a highrisk suicide group, suggesting that in a DSP population there is less likelihood to switch to more ‘violent’ methods than in other suicide populations.
Several findings support psychiatric assessment for all deliberate self-poisoning patients. Absconding from care was a major risk factor for subsequent suicide. Many cases of absconding patients did not have a psychiatric assessment and would have been excluded from the multivariate analyses. Absconding has been a risk factor for suicide by psychiatric inpatients [29], [30]. Psychiatric assessment has been associated with a twofold reduction in repetition of DSH in the UK [31], but we are not aware of studies showing absconding patients at increased risk of death in self-poisoning subjects. Absconding was a rare event in our study, probably because the HATS service uses techniques to reduce this. Subsequent suicide of these patients occurred 1–2 years after presentation. This indicates that these factors identify a person at risk of suicide for some time after presentation and represent a patient characteristic.
Implications for service delivery are that interventions aimed at suicide prevention may need to be structured differently by gender and age. Psychiatric assessment should be performed on all patients presenting with selfpoisoning in keeping with guidelines that this be done for all hospital-treated DSH cases [32]. Effective service provision in the general hospital also needs to be provided to reduce the number of patients absconding without psychiatric assessment.