
Abstract
Keywords
Although it is widely accepted that a variety of genetic, temperamental and childhood experiences contribute to the development of personality dysfunction, there has been remarkably little effort to examine across more than one personality disorder the relative contributions of such temperamental and childhood risk factors. For instance, there is reasonable evidence that individual factors such as maternal and parental neglect [1, 2], childhood emotional, physical and sexual abuse [3–5], temperament [6–8] and childhood and/or adolescent axis I psychopathology [9–12] are all contributors to adult personality disorder. However, studies which examine all of these variables simultaneously in a group of patients are notably lacking.
The most valid approach to the diagnosis and classification of personality disorders remains contentious, but DSM-IV lists 10 specific personality disorders, which are grouped into three clusters (termed A, B and C). There are many difficulties with this approach to classification, not the least being that many patients who meet criteria for one personality disorder also meet criteria for other personality disorders. When clinicians or researchers use structured interviews, such as the Personality Disorder Examination (PDE) or the Structured Clinical Interview for DSM – axis two (SCID-II), about 30–60% of patients meet criteria for one or more personality disorders, but without structured interviews clinicians make personality disorder diagnoses on considerably fewer patients [13]. Clinically, borderline personality disorder is perceived as the most problematic, and one of the more common, while avoidant personality disorder is usually the most common. Epidemiologically and forensically, antisocial personality disorder has been the most studied. In the Australian National Survey of Mental Health and Wellbeing, obsessive compulsive (anankastic) personality disorder was the most common [14], but the authors reveal there were major limitations on how personality disorders were diagnosed in this community study.
One relatively new approach to the assessment of personality, which bridges genetics, psychobiology and traditional clinical diagnoses is the Psychobiological Model of Temperament and Character developed by Cloninger [15]. Temperament refers to automatic emotional responses to experience that are moderately heritable and stable throughout life, while character refers to self-concepts and individual differences in goals and values which influence choice, intention and meaning [16]. In this model there are four dimensions of temperament: novelty-seeking which reflects the propensity for approach and exploration; harm avoidance which reflects the propensity to withdraw and worry; reward dependence which reflects the propensity for attachment and dependence; while persistence reflects the propensity for diligence and perseverance. While lack of character development, most notably low self-directedness is a feature of all individuals with personality disorders [6, 17–19], temperament influences which specific personality disorder an individual may have [8, 20]. Thus patients with cluster C (anxious) personality disorders have high harm avoidance, patients with cluster B (impulsive) personality disorders have high novelty-seeking, while patients with cluster A (eccentric or odd) personality disorders have low reward dependence. Furthermore, within clusters combinations of temperament influence which specific personality disorder an individual has. In cluster C, avoidant personality disorder is only associated with high harm avoidance, while dependent is associated with high harm avoidance and high reward dependence, and obsessive compulsive is associated with high harm avoidance and high persistence. In cluster B, histrionic is associated with high novelty-seeking and high reward dependence, antisocial is associated with high novelty seeking, low harm avoidance and low reward dependence, while borderline is associated with the combination of high harm avoidance and high novelty-seeking.
We have utilized data collected from a cohort of depressed patients participating in a long-term treatment trial examining predictors of outcome [21, 22] and examine the relative contributions of: (i) temperament; (ii) childhood environmental factors such as parental neglect and abuse experiences; and (iii) childhood and adolescent axis I psychopathology, to the development of the two most common personality disorders: avoidant and borderline. Avoidant personality disorder not only tends to be the most common personality disorder in clinical samples of depressed patients [23, 24], but also represents cluster C personality disorders. By contrast, borderline personality disorder is one of the cluster B personality disorders, and is often seen as the most severe and/or most clinically problematic personality disorder.
Method
Patients
The depressed outpatients in this study were recruited for a 5 year prospective outcome study, with initial randomization to fluoxetine or nortriptyline as the first antidepressant drug. More details on the clinical characteristics, social functioning and response to treatment of these patients are presented in other papers [21, 22, 25, 26]. In brief, patients needed to be suffering from a current major depressive episode as a principal diagnosis, and be suitable and willing to receive treatment with antidepressant medication. Psychiatric exclusion criteria were minimized [27], but included severe alcohol and/or drug dependence as a principal diagnosis, schizophrenia, a history of mania (but not hypomania) and severe antisocial personality disorder which would make compliance with the research protocol problematic. However, during the study no patient interviewed by a clinician was actually excluded from the study because of severe alcohol and/or drug dependence, or due to severe antisocial personality disorder. Patients were also excluded if they had a current major medical illness. After giving written informed consent, patients reported for a detailed clinical and neurobiological evaluation prior to treatment. This study was approved by the Canterbury Ethics Committee.
Assessment of personality disorders
At the baseline clinical assessment, patients completed a series of self-report questionnaires which included the Structured Clinical Interview for DSM-III-R – personality questionnaire (SCID-PQ) [28]. Over the following weeks, and after the initiation of antidepressants, the treating psychiatrist completed the Structured Clinical Interview for DSM-III-R – Axis Two (SCID-II) [28], utilizing the results from the SCID-PQ as an initial screen for personality disorder criteria. A sample of the SCID-II interviews were subjected to interrater reliability checks. This involved the videotaping of the psychiatrists’ SCID-II interview; the video was then rated by a second psychiatrist. A third psychiatrist in a separate interview independently assessed the patient with a SCID-II interview. The interrater reliability for all three assessments was satisfactory, and the kappa for presence/absence of any personality disorder between the treating psychiatrist and the third psychiatrist who conducted an independent interview was 0.70.
Assessment of risk factors for personality disorders
(i) Parental neglect was assessed by using the care scale of the Parental Bonding Instrument [29]. For this paper the maternal and paternal care scales were combined and the scores collapsed to create quartiles from no neglect (i.e. high care) to severe neglect (i.e. low care).
(ii) Childhood abuse was assessed by independent interview conducted by a research nurse (RMA) who systematically asked all patients about a variety of experiences including childhood abuse. This involved questioning on psychological/emotional abuse, physical abuse and sexual abuse. Details of sexual abuse included separate questioning about non-contact and contact abuse, and sexual abuse involving sexual intercourse. Each form of abuse was rated as absent, mild or severe, and the varying forms of abuse were combined to create a single abuse score ranging from zero (no abuse) to three (severe childhood abuse).
(iii) Temperament was assessed by patient self-report using Cloninger's Temperament and Character Inventory (TCI) [30]. In this study the four temperament measures (harm avoidance, novelty seeking, persistence and reward dependence) were collapsed into quartiles for purposes of analysis. We did not consider that the character measures represented risk factors for personality dysfunction, but should be considered correlates of personality dysfunction [6, 31].
(iv) Childhood and adolescent psychopathology was collected by the treating psychiatrist when completing the Structured Clinical Interview for DSM-III-R (SCID) [32] and the SCID-II for conduct disorder. Based upon the SCID interview, we considered childhood and adolescent psychopathology as disorders having an onset prior to the age of 18 years. We thus extracted the data on age of onset of any anxiety disorder (panic disorder, agoraphobia without panic, social phobia, specific phobia or obsessive compulsive disorder), age of onset of first hypomanic episode, age of onset of alcohol or drug dependence and age of first major depressive episode. In the case of anxiety disorders or substance dependence we utilized the youngest age of onset of any disorder.
Statistical approach and methods
All data from the study was entered into the relational database PARADOX, and transferred to SYSTAT for statistical analysis. The primary outcome variables were the categorical diagnoses of avoidant personality disorder and borderline personality disorder. Risk factors were collapsed into two, three or four ordinal categories; and the principal approach used was logistic regression. Initially, each potential risk factor was examined in a univariate manner against the two personality disorder outcomes. After completing the univariate analyses all significant risk factors were entered into a multivariate analysis. Non-significant risk factors were deleted one by one to obtain a final multivariate model.
The decision to collapse risk factors into two, three or four ordinal categories (e.g. quartiles for continuous measures) and to utilize personality disorders as categorical outcomes was based upon making results easily interpretable by clinicians. However, comparable analyses have been run using risk factors (e.g. temperament dimensions) and outcome variables (i.e. personality disorder symptoms) as continuous measures. Regardless of categories or dimensions, both as risk factors or outcomes, the results are similar.
Results
Prevalence of personality disorders
In this study we recruited 195 depressed patients. Axis II diagnostic interviews were not completed on 12 patients, and a further three patients did not complete all their questionnaires such as the TCI. This study is therefore based on 180 patients for whom we had complete axis II interview data and risk factor data. Of these 180 patients, 46% (n = 82) met criteria for one or more personality disorders; 14% (n = 26) met criteria for two; and 12% (n = 22) met criteria for three or more personality disorders. The most common personality disorders were avoidant (24%, n = 43) and borderline (17%, n = 30) followed by paranoid (15%), obsessive compulsive (9%) and histrionic (5%). Of the 43 patients with avoidant personality disorder, eight also met criteria for borderline personality disorder.
Demographic risk factors
From Table 1 it can be seen that gender was not a risk factor for either avoidant or borderline personality disorder. However, increasing age was significantly associated with a lower risk of borderline, but not avoidant personality disorder.
The relationship between demographic and childhood environmental factors and the probability (%) of avoidant and borderline personality disorders
Childhood environmental risk factors
Table 1 shows that with increasing parental neglect (i.e. lower care scores on the PBI), that the probability of both avoidant and borderline personality disorder diagnoses increase. Table 1 also shows that with increasing levels of childhood abuse the probability of both personality disorders increases. As neglect and abuse may occur together we created a third variable, abuse and/or neglect which was the worst rating on either of the two separate scales. Again, increasing levels of abuse and/or neglect were significantly associated with increasing rates of both personality disorders. Thus, in the case of borderline personality disorder the rate of this diagnosis went from 0% in those who had experienced neither abuse nor neglect to 28% in those who were rated as having experienced severe abuse and/or neglect. It is of note that the combined abuse and/or neglect variable was a stronger predictor of borderline personality disorder than either variable separately; but for avoidant personality disorder the combined abuse and/or neglect variable added little to the neglect variable alone. As abuse added little to the neglect variable alone, we have used the simplest model (i.e. neglect) in further analyses.
Temperamental risk factors
From Table 2 it can be seen that the probability of an avoidant personality disorder increases markedly from 3% to 47% with increasing harm avoidance.
The relationships between temperament and the probability (%) of avoidant and borderline personality disorders
Existing data from Cloninger's Psychobiological Model of Personality finds that the temperamental risk pattern for borderline personality disorder is a combination of high novelty-seeking with high harm avoidance [17, 30]. This combination reflects an approach – avoidance (novelty-seeking – harm avoidance) conflict which may be the temperamental substrate of affectivity instability. We thus created a further temperamental variable (named borderline temperament) by multiplying novelty-seeking with harm avoidance, and dividing the resulting score into quartiles. This novelty-seeking by harm avoidance variable (borderline temperament) was related to borderline personality disorder (OR = 1.57; 95% CI 1.10, 2.24; p = 0.013) with the rate of borderline personality disorder increasing from 6%, through 18 −19%, to 25% by quartile.
Childhood and adolescent psychopathology risk factors
Table 3 shows the relationships between childhood and adolescent psychopathology and risk of avoidant and borderline personality disorders. From this table it can be seen that early onset of the first major depressive episode increased the risk of both personality disorders. Early onset anxiety disorders markedly increased the risk for avoidant, but not borderline, personality disorder. Number of childhood conduct symptoms increases the risk of both personality disorders, but is especially marked in the case of borderline personality disorder. Early onset alcohol and/or drug dependence markedly increased the rate of borderline, but not avoidant, personality disorder; as does early onset hypomanic episodes.
The relationships between childhood and adolescent psychopathology and the probability (%) of avoidant and borderline personality disorders
Multivariate prediction of avoidant personality disorder
In a multivariate logistic regression, three variables made significant independent contributions to predicting the presence of an avoidant personality disorder. These three variables were: harm avoidance (adjusted OR = 2.81; 95% CI 1.75, 4.51: p < 0.0.002); an early onset anxiety disorder (adjusted OR = 1.90; 95% CI 1.24, 2.93; p = 0.003); and parental neglect (adjusted OR = 1.68; 95% CI 1.15, 2.46; p = 0.007).
We also utilized avoidant personality disorder symptoms as a dimensional outcome variable and the same three risk factors (harm avoidance, early onset anxiety disorder and parental neglect) were retained with multiple linear regression. Together these three variables explained over 35% of the variance in avoidant personality disorder symptomatology.
Multivariate prediction of borderline personality disorder
In a multivariate logistic regression, four variables made significant independent contributions to predicting the presence of a borderline personality disorder. These were: childhood abuse and/or neglect (adjusted OR = 2.21; 95% CI 1.24, 3.94; p = 0.007); age of first depressive episode (adjusted OR = 2.03; 95% CI 1.20, 3.43; p = 0.008); conduct disorder symptoms (adjusted OR = 1.82; 95% CI 1.07, 3.10; p = 0.027); and early onset alcohol or drug dependence (adjusted OR = 2.57; 95% CI 1.00, 6.59; p = 0.050). Neither borderline temperament (novelty-seeking x harm avoidance) nor adolescent hypomania made significant independent contributions. However, borderline temperament was associated with adolescent hypomania, with childhood conduct disorder symptoms, with adolescent alcohol or drug dependence and with early age of first depressive episode. Given the associations between these variables we re-ran the multivariate logistic regression but excluded childhood and adolescent psychopathology; in this situation both abuse and/or neglect (adjusted OR = 2.50; 95% CI 1.48, 4.21; p = 0.001) and borderline temperament (i.e. high noveltyseeking x harm avoidance temperament) (adjusted OR = 1.62; 95% CI 1.12, 2.35; p = 0.011) made significant contributions to the presence of a borderline personality disorder.
In multiple linear regression, using number of borderline personality disorder symptoms as a dimensional outcome, essentially similar findings emerged. Thus, the combination of neglect and/or abuse, conduct disorder symptoms, early age of first depressive episode and adolescent onset alcohol or drug dependence explained about 30% of the variance in borderline symptomatology. The combination of abuse and/or neglect, borderline temperament, and early age of first depressive episode explained about 25% of the variance.
Another presentation of these results is shown in Figs 1, 2. Figure 1 shows that in those without abuse and/or neglect (none, mild) and without borderline temperament (low novelty seeking x harm avoidance) that no patients met criteria for borderline personality disorder. In those with one but not both risk factors, 8 −9% had borderline personality disorder; while in those with abuse and/or neglect (moderate or high) and with borderline temperament (high novelty-seeking x harm avoidance) 31% met criteria for borderline personality disorder.
The combined impact of childhood abuse and/or neglect with borderline temperament (i.e. high novelty-seeking x harm avoidance) on the probability of developing borderline personality disorder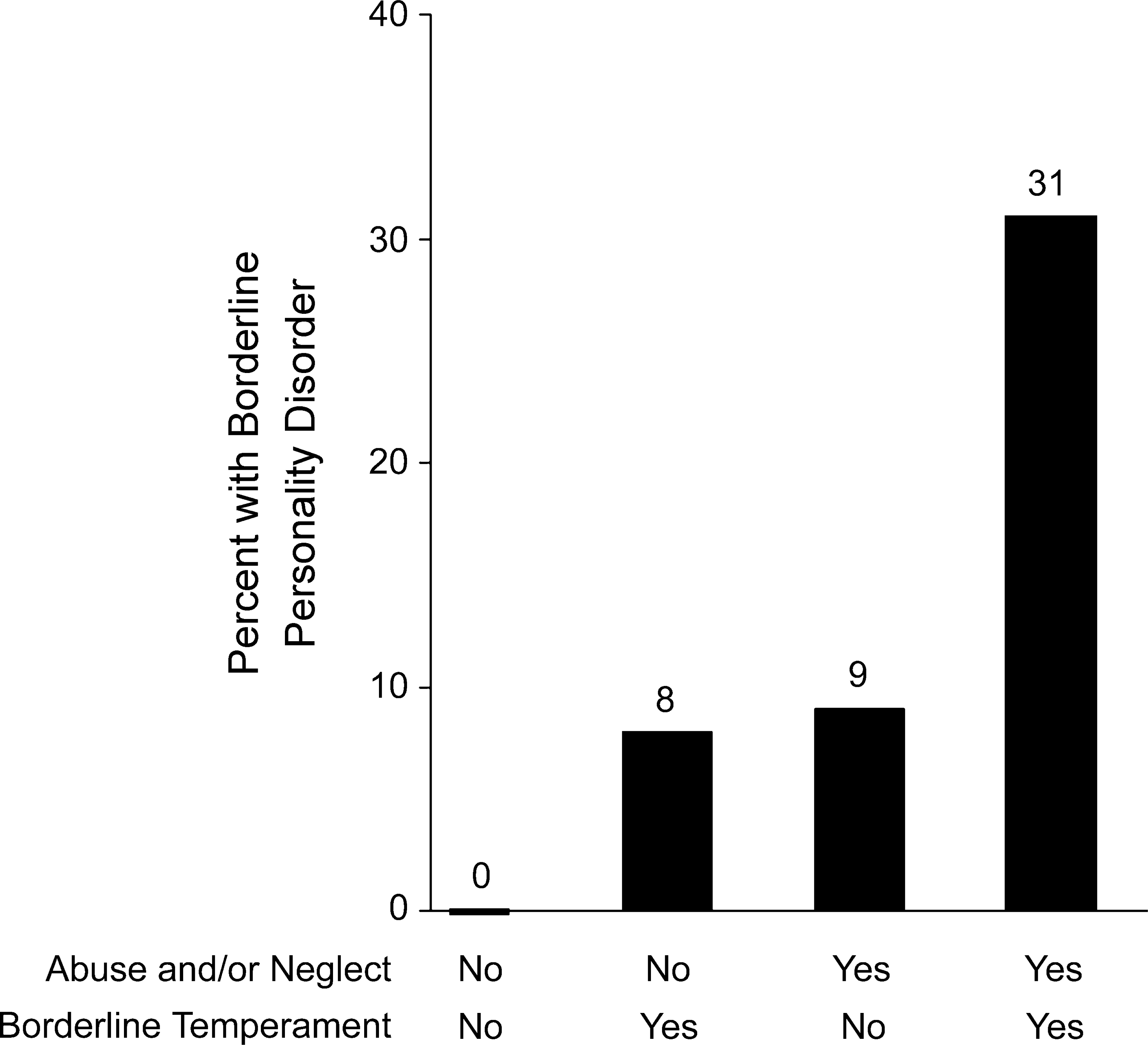
Figure 2 shows the additional impact of childhood or adolescent psychopathology on the probability of a borderline personality disorder in those who had experienced childhood abuse and/or neglect and who had borderline temperament (i.e. high novelty-seeking x harm avoidance).
The additional impact of childhood or adolescent psychopathology in those with abuse and/or neglect and borderline temperament on the prevalence of borderline personality disorder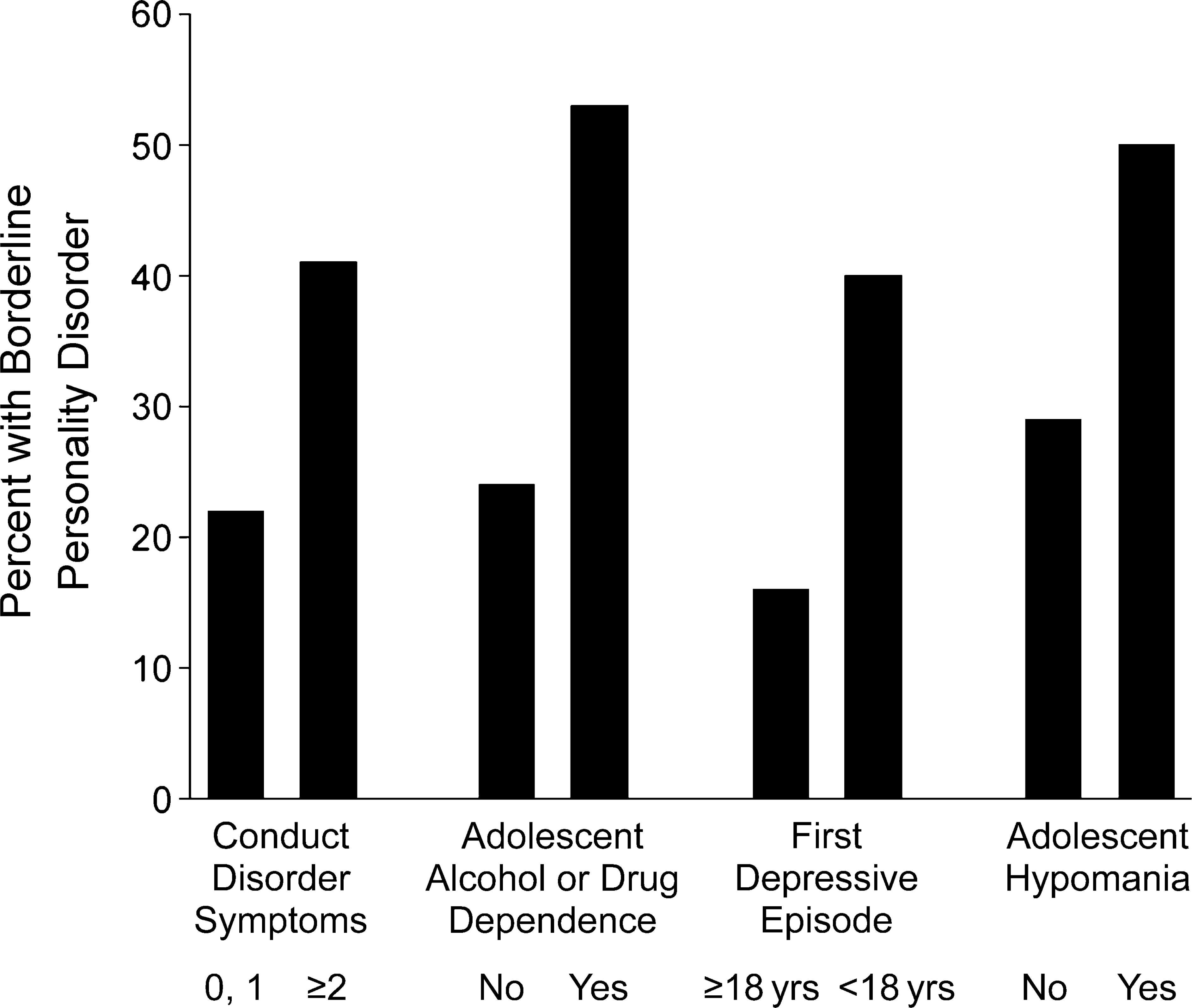
Comorbid avoidant and borderline personality disorder
As eight patients met criteria for both avoidant and borderline personality disorder, we examined this subset of patients as a separate specific group, although they had been included in both sets of analyses. In general, this comorbid group tended to be more extreme on general risk factors (e.g. parental neglect) and to show both sets of specific risk factors (e.g. high harm avoidance and histories of hypomania).
Discussion
Avoidant personality disorder
The major risk factor for avoidant personality disorder in this study is the temperament trait of harm avoidance. Harm avoidance in personality models such as Eysenck's is introverted neuroticism [16, 33]. Thus, introverted neurotic or shy anxious personality traits appear to be the largest risk factor, although this is compounded if a patient also develops a childhood or adolescent anxiety disorder. Perhaps it is not surprising that childhood or adolescent anxiety disorders are additional risk factors, as the most common childhood anxiety disorder in this sample was social phobia; and the comorbidity of social phobia with avoidant personality disorder is well described. It is also of interest that there are shared genetic factors between personality traits such as neuroticism and anxiety and depressive disorders [34–37]. The third identified risk factor was parental neglect.
Borderline personality disorder
Currently, some clinicians believe that childhood abuse is the cause of borderline personality disorder; but the data here show that while it is an important risk factor, it is neither necessary nor sufficient. Thus 8% of patients who reported no abuse developed borderline personality disorder, and 67% of patients with severe abuse did not develop borderline personality disorder. Combining childhood abuse with parental neglect was a more powerful risk factor than abuse alone. Linehan similarly believes that abuse is neither necessary nor sufficient for the development of borderline personality disorder. Linehan uses the term ‘invalidating’ environment as a more general description of childhood environmental variables which interactively contributes to the development of borderline personality disorder [38], while we have used a narrower terminology of abuse and/or neglect.
Furthermore, there is a fundamentally important interaction between abuse and/or neglect and either temperament or childhood and adolescent psychopathology. If in the first instance we limit discussion to the interaction of abuse and/or neglect with borderline temperament (high novelty-seeking x harm avoidance) then 0% of depressed patients with neither risk factor develop borderline PD while 8 −9% develop this personality disorder with one risk factor, but 31% develop borderline personality disorder with both risk factors. This ‘gene – environment’ interaction is remarkably reminiscent of the adoption studies of another cluster B personality disorder, antisocial personality disorder [39].
The temperamental substrate of borderline personality disorder involves moderate or greater levels of both novelty-seeking (tendency to approach) and of harm avoidance (tendency to withdraw). Thus, clinicians may underestimate the importance of temperament, as their borderline personality disorder patients may not present as extreme on either measure, just moderately high on both.
To decrease the probability of individuals with a borderline temperament developing borderline personality disorder, parents and caregivers need to understand this temperamentally driven approach – avoidance conflict. It is necessary for caregivers to accept the emotional extremes of euphoria and anger, and the relationship extremes of love and hate, if developing children and adolescents are to accept and learn about their own temperamentally driven conflicts.
In a community sample, Cloninger and colleagues have clearly shown that a borderline temperament with high novelty-seeking and harm avoidance is associated with considerably greater risk of impaired character development, as reflected by low scores on the character measures of self-directedness and cooperativeness [16].
It is not surprising that there were also associations between borderline temperament and conduct disorder symptoms, adolescent alcohol and drug dependence, adolescent depression and hypomania. However, this means that many individuals with borderline potential may be seeing child and adolescent mental health professionals. Theoretically this provides opportunities to intervene in the developmental pathways towards borderline personality disorder.
The links between childhood and adolescent depressive disorders and adult borderline personality disorder are being increasingly recognized [11, 40], as are the links between adolescent substance dependence and borderline personality disorder. The links between childhood and adolescent bipolar spectrum disorders and borderline personality disorder are also being increasingly recognized [41, 42].
Limitations
All studies have their limitations, and in this study they can be conceptualized as: (i) the reliability and validity of the outcome measures (avoidant and borderline personality disorders); (ii) the reliability and validity of the risk factors; and (iii) the fact that this was a clinical sample and not a random community sample.
Ideally, a study such as this should be repeated as a longitudinal prospective community study, but such studies are rare, expensive and time-consuming, and their generalisability to clinical practice is often limited. Furthermore, the concept of personality disorders has largely arisen out of clinical practice, because clinicians had to deal with the reality of managing challenging patients. The relative contributions of risk factors to avoidant and borderline personality disorder may be different in a community sample or in a sample of psychiatric outpatients or inpatients with other axis I disorders. However, major depression is the most common disorder in outpatient practice, and we anticipate that the findings reported here are applicable across many clinical settings.
It is often suggested that it is difficult to make axis II diagnoses when patients are depressed. While there is little doubt that mood state affects self-rating of personality, there is also reasonable evidence that clinician interviews using semistructured diagnostic interviews appear to remove a large part of the mood effects [43]. Indeed, when conducting SCID-II interviews it is often necessary to repeatedly remind patients that you are enquiring about how they usually are, not how they are at present. The alternative, of only assessing personality disorders after the depressive disorder has been treated, is fraught with more problems than assessing patients when depressed. Given that only about a half of depressed patients respond to a first antidepressant, do you assess personality after one, two or three or more antidepressant trials? Delaying making the diagnosis ensures that those with treatment-resistant mood disorders will disproportionately also receive a personality disorder diagnosis, and that the incorrect prophecy of a personality disorder diagnosis being associated with poor outcome will be fulfilled [44].
As the diagnosis of any personality disorder is not absolutely reliable, this limits the extent to which risk factors can completely predict the outcome variable. Indeed, with a kappa of 0.7 for a personality disorder diagnosis, then the upper limit on the percent variance that risk factors can explain is about 50% (0.7 2 _ 100). To thus explain 25–35% of variance suggests that the major risk factors have been identified in these models. This is even more so when we consider that the risk factors themselves have been treated as simple two, three or four point categorical variables. Whether the DSM-IV approach to separating axis I and axis II disorders is optimal, and whether DSM has the appropriate criteria for valid avoidant and borderline personality disorder diagnoses are broader issues and cannot be addressed in this paper. However, we do not support endless committees slightly altering diagnostic criteria. Until such time as we have more valid and widely accepted views on the interplay of axis I and axis II and how best to assess both, we consider it desirable to utilize existing criteria and guidelines, but to retain a healthy scepticism as to their ultimate validity.
A final limitation is that the risk factors for personality disorders were assessed concurrently with the personality disorder diagnosis. However, clinicians are always going to face this dilemma as they develop an aetiological formulation for the patients they see. There is reasonable evidence that the self-report parental care scale is valid and stable even when patients are depressed [45]. Interviews (done independently of clinicians making the axis II diagnoses) of childhood abuse appear valid, although a single interview may underestimate the extent of past abuse. Finally, temperament measures are reasonably stable over time, and while harm avoidance (like neuroticism) does vary with mood, all patients were depressed when they completed the initial temperament measures [16]. It is of note though that the temperament self-report by patients with borderline personality may be less reliable than those of others, as judged against other significant reports on temperament or self-report 6 months later (unpublished. data). However, our evidence suggests that borderline personality disorder patients under-report their novelty-seeking scores when depressed. Thus, if there were any impact on our results, it would be to make novelty-seeking (and also noveltyseeking x harm avoidance) a greater risk factor than estimated in this paper.
Conclusions
We have shown that temperament, childhood environment and childhood and adolescent psychopathology all make significant contributions to the development of avoidant and borderline personality disorder in depressed outpatients. For avoidant personality disorder the key risk variables appear to be a shy anxious temperament (high harm avoidance), childhood anxiety disorders and deficient parental care. For borderline personality disorder there are more complicated interactions of childhood abuse and neglect, borderline temperament (high novelty seeking and high harm avoidance), with childhood and adolescent psychopathology including conduct disorder, alcohol and drug dependence, hypomania and depression.
Footnotes
Acknowledgements
This research was funded by the Health Research Council of New Zealand. We thank all clinicians and patients involved, and especially Isobel Stevens and Robyn Abbott for their contributions.