
Abstract
Under the heading of eating disorders, DSM-IV specifies three diagnoses: anorexia nervosa (AN), bulimia nervosa (BN) and eating disorders not otherwise specified (EDNOS) of which binge eating disorder (BED) is one of them. AN's typical characteristics include refusing to maintain a minimal body weight, serious fear of gaining weight, important problems with thinking about their body type and size, and, in female patients, the presence of amenorrhoea after the menarche. Patients with BN have the strong perception that they cannot control their eating or overeating during binge episodes. BN is characterized by repeated episodes of binge eating followed by inappropriate compensatory behaviours such as self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise. In DSM-IV BED there are binge eating episodes but not compensatory behaviours [1].
For many years AN has been known as one of these disorders but an answer is still being sought for whether or not BN is a newly emerged disorder or if not an old disorder defined in a new way or its reflection or a different manifestation of AN.
In adolescence and young adulthood the incidence of AN among women is 0.5–1% and the incidence of BN is 1–3% in Western countries [1]. In a university in the eastern US it was reported that in a study of 1965 students the incidence of BN among girls was 1.3% and among boys was 0.1% according to DSM-III or DSM-IV criteria [2]. In another study with Texas University students 1.3% of girls and 0.2% of boys were found to have BN [3]. In a study to determine the frequency of AN in five different groups of young people in three different countries, the frequency of AN seen among young girls living in Munich was 1.1%, in one region of Greece the frequency among girls was 0.41% and in another region 0.35%. In the same study there was no AN found among Greek boys and girls or Turkish boys [4].
In research conducted in Western societies, the lower self-esteem [5–7], child abuse [8–11] and poor family functioning [12–14] have been identified as risk factors for EDs. But it is not clear that these are also risk factors for EDs in non-Western societies.
There are important cultural and social factors in the aetiology of EDs. It is known that these disorders are characteristic of Western societies and rarely seen in other societies [15, 16]. In Western societies it is observed that sociocultural pressures, the value placed on physical appearance in women's sexual role, the presentation of extremely thin women as the ideal body image and the emphasis on the importance of a woman's physical appearance for social success are risk factors for the development of EDs [17]. These values are not different from Western societies for women in urban areas of Turkey and these are also increasing among women in rural areas through TV and mass media.
The diagnosis of AN is easy after the first stage because the physical changes in AN is clear. However, in BN the patient may have a normal weight or may be overweight, and contrary to AN it is difficult to recognize and diagnose. In addition, the percentage of the cases of BN that admit for treatment is very low. This situation, also the case for BED, which is more prevalent among obese people than the general population, increases the importance of epidemiological studies [18].
Although there are a large number of studies in Western societies on the characteristics and frequencies of EDs, there are very few studies in developing societies or emigrants to the west and in the rural areas of these societies. This situation makes it hard to understand the cultural aspect of EDs and to compare the societies with each other.
The purpose of this study was to determine the frequency of EDs among university students in a rural area (Sivas City) of Turkey, and to compare the groups based on the sociodemographic data, history of child abuse and neglect, family functions and self-esteem with a healthy control group regarding EDs, and also to compare the results based on the results of studies done both in the west and in our country.
Method
Research population and sampling
The subjects for the research were selected from students enrolled in university programs on the Cumhuriyet University campus. The Cumhuriyet University Student Services Director selected students according to faculty, university program and class. Medical students in the 5th and 6th year and students in the county professional university programs were not included in the study. In our study the target was to achieve 10% of the total number of students. When the students were identified and placed into sample groups, the plan was to reach the 1st, 2nd, 3rd and 4th year classes of every program to represent every university program and every class. The sample included 10% of the total of students from all of the classes. The total number of students on the Cumhuriyet University campus was 11 275. Of these students 4125 were female and 7151 were male. Of this total number of students, 691 students who were in the county professional schools and 289 students in the 5th and 6th years of medical school were not included in the study. Our study population was made up of 11 275 students. Our goal was to reach 1127 students.
Permission for the study was obtained in writing from the office of the rector of Cumhuriyet University. Simple random sampling method was used to obtain a sample representative of the university population of 1003 students who were informed about the study. Twenty-three students (2.29%) declined to accept to participate in the study.
Data collection tools
Sociodemographic Information Form: A sociodemographic questionnaire was developed for this study that assessed: name, age, sex, economic situation, height (metres), weight (kg), body mass index (BMI) obtained by the formula weight divided by height squared, and for girls, the presence of menstrual irregularity. Eating Attitudes Test (EAT): This is a tool developed by Garner and Garfinkel for the purpose of screening eating disorders in adolescent girls and young women. It can be used for people over 11 years of age, which contains 40 questions with six graduated answers in Likert style [19]. In 1989, Erol and Savaşır confirmed the validity and reliability of this tool in Turkey [20]. Rosenberg Self-Esteem Scale (RSES): This is a measure of selfevaluation using 63 multiple-choice questions [21]. The scale has 12 subcategories. The first 10 subcategories were used to measure selfesteem for our research goal. The scale's reliability and validity in our country was tested by Cuhadaroglu [22] and the level of internal reliability was found to be r = 0.71 and test–retest reliability was r = 0.75. Structured Clinical Interview for DSM-IV axis I Disorders (SCIDI), Clinical Version Childhood Abuse and Neglect Questionnaire Form (CANQF): This form examines childhood abuse and neglect with incidents of physical, sexual and emotional abuse, neglect and incest. Brown and Anderson's definitions were used for physical abuse, sexual abuse and incest [25]. Childhood physical abuse is defined as physical violence against a person under 16 years old, by someone at least 5 years older or by a family member at least 2 years older than the victim. Close confinement, such as being locked in a closet is also included. The victim perceives it severe, but should not consider this maltreatment as sibling rivalry. Quarrels between friends that do not include any physical contact are not accepted as physical abuse. Childhood sexual abuse is defined as involvement of a person younger than 16 years old in any kind of sexual activities, such as genital fondling, an adult exhibiting his or her genitalia to a child, forcing the child to exhibit himself or herself to the adult or the child to have sexual intercourse with someone at least 5 years older or with a family member (incest) at least 2 years older than the victim. Questions about emotional abuse and neglect were based on the descriptions of Walker et al. [26]. Emotional abuse involves the use of excessive verbal threats, ridiculous and personally demeaning comments, derogatory statements and threats against the young person to the extent that a child's emotional and mental wellbeing will be jeopardized. Neglect refers to acts of omission in which the child is not properly cared for physically (nutrition, safety, education, medical care etc.) or emotionally (failure to bond, lack of affection, love, support, nurturing or concern). Family Assessment Device (FAD): This self-report device was developed by Gülerce [27] for the purpose of measuring a family's internal relationships, needs, family structure and total functioning. There are 36 items that comprise seven subtests: communication, unity, management, perfection, emotional attachment, individuality and satisfaction. Answers are marked on a separate form using a 10-step Likert scale that ranges between ‘just like ours’ and ‘exactly opposite ours’. The lowest score for each question is 1 and the highest is 5. A high FAD score means ‘good and healthy adjustment’.
The device was tested on 100 university students by 1-month interval and the Pearson's product–moment correlation was 0.79, Stanley correlation coefficient was 0.85. Kuder–Richardson 20-coefficient test of internal stability total score was approximately 0.70. The correlation between the FAD scores and the Beaver Timber Lawn family assessment scores was found as 0.78 (statistically significant) and also the correlation between the FAD scores and the Minnesota Multiphasic Personality Inventory (MMPI) family relationships subtest scores was 0.69 (statistically significant) [27].
Procedure
This research was carried out on the campus of Cumhuriyet University. Subjects were selected using the simple random sampling method. Previously identified university classrooms were entered. The sociodemographic information form and EAT were given to 980 students who agreed to participate and gave informed consent. The SCID-I was used to interview the students who scored higher than the cutoff score of 30 on the EAT for diagnosis. The control group was matched with the students having ED in respect of the number and sex and was consisted of classmates who had a score on the EAT below the cutoff score and did not have an eating disorder using SCID-I. The control group was selected by using simple random sampling method. The control group was consisted of 18 females and three males. The difference among characteristics such as gender, age, BMI and income level was not found to be statistically significant (p < 0.05). Both groups were given RSES, FAD and CANQF. The data obtained were evaluated using the SPSS statistical package program. Quantitative data evaluation was done with Mann–Whitney U-test and qualitative data were evaluated with chi-squared test. Results at the p < 0.05 level were considered statistically significant.
Results
Seventy-one of the 951 students (492 female, 459 male) who correctly filled out the EAT had a score above the cutoff level of 30 or higher. Of these 71 students, 21 (2.20%) were found to have an eating disorder based on the SCID-I. No subjects were found to have AN. Eighteen of the 21 subjects were female. Of these 18 female students 15 (1.57%) were found to have BN and three (0.31%) were found to have BED. All of the three male subjects were diagnosed with BED (0.31%). The age range for the study and control group was 18–24 years old and the mean age for the study group was 20.0 ± 1.60 and for the control group was 21.1 ± 1.72.
Sociodemographic data
A statistically significant difference (p < 0.05) was not found between the study and control groups regarding age, sex and economic situation. The study group had significantly higher menstrual irregularity for females (χ2 = 4.50, p = 0.03). The data for both groups are shown in Table 1.
Sociodemographic data, history of childhood abuse and neglect in the study and control group
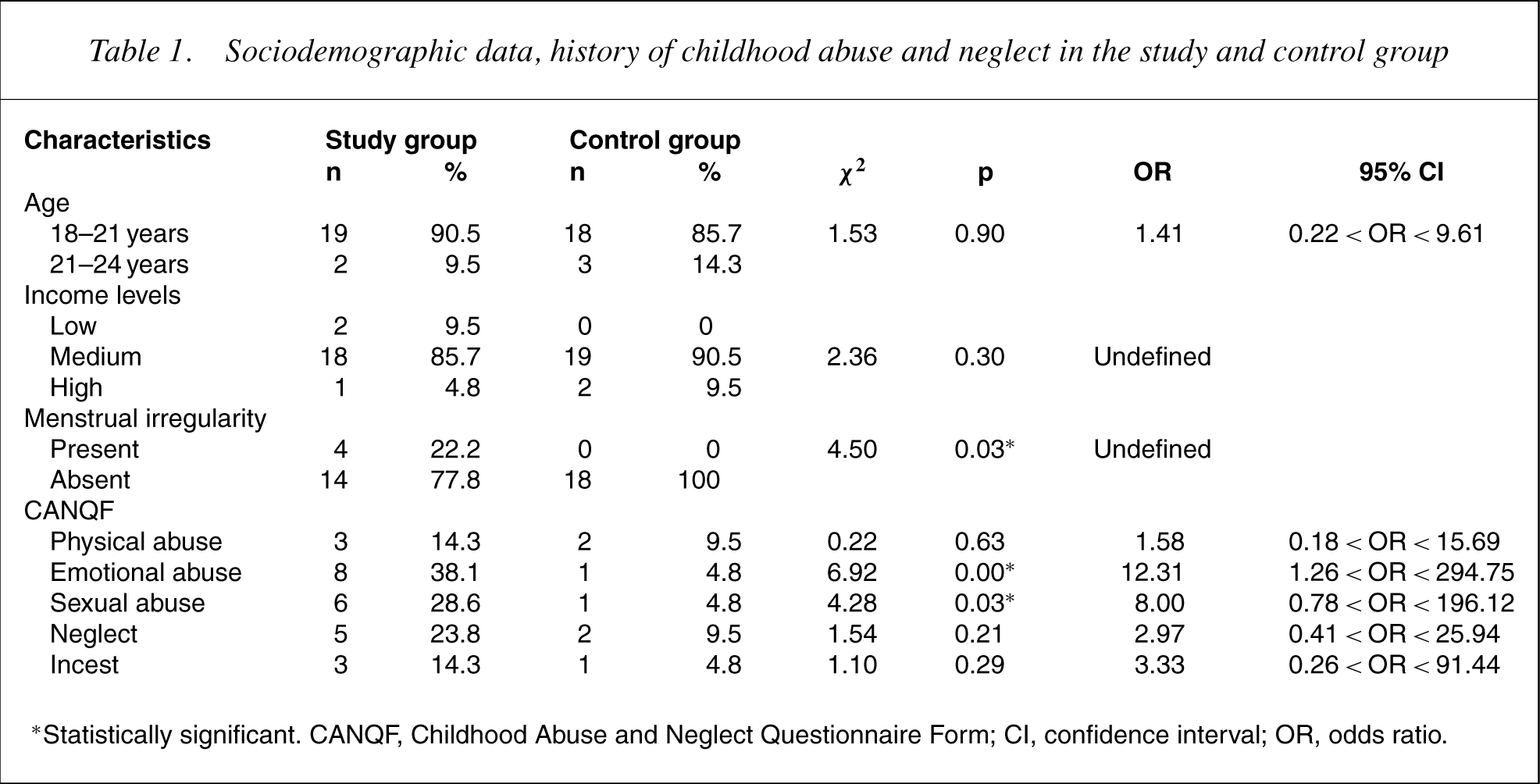
∗Statistically significant. CANQF, Childhood Abuse and Neglect Questionnaire Form; CI, confidence interval; OR, odds ratio.
Physical measurements
There was no statistically significant difference between the study (21.02 ± 2.62) and control groups (20.86 ± 2.63) regarding mean height, weight, and BMI, which is determined by the formula weight, divided by height squared (p < 0.05).
Self-esteem
The self-esteem scores of the study group were found to be significantly lower than those of control group (χ2 = 33.4, p < 0.001).
History of childhood abuse and neglect
The incidence of physical, emotional and sexual abuse in the study group was 14.3% (n = 3), 38.1% (n = 8) and 28.6% (n = 6) respectively; however, the incidence in the control group was 9.5% (n = 2), 4.8% (n = 1) and 4.8% (n = 1) respectively. The incidence of neglect was 23.8% (n = 5) in the study group and 9.5% (n = 1) in the control group; the incidence of those in the study group subjected to incest was 14.3% (n = 3) and 4.8% (n = 1) in the control group. Although 4.8% (n = 1) of the study group had attempted suicide, there was no history of suicide attempts in the control group but the difference between the two groupswas not found to be statistically significant (χ2 = 0.35, p = 0.54). The frequency of childhood emotional and sexual abuse was significantly higher in eating disorder group than the control group (χ2 = 6.92, p = 0.00; χ2 = 4.28, p = 0.03 respectively). The mean scores of child abuse and neglect for both groups are shown in Table 1.
Family roles
When the scores for study group and control group were compared for the FAD's seven subtests, the scores for communication in the family, family unity and emotional attachment in the family were found to be statistically significantly lower in the study group (z = −3.91, p < 0.001; z = −2.72, p < 0.001; z = −5.59, p < 0.001 respectively). The scores for both groups on the FAD subtests are shown in Table 2.
The FAD's subtests mean scores of study and control groups
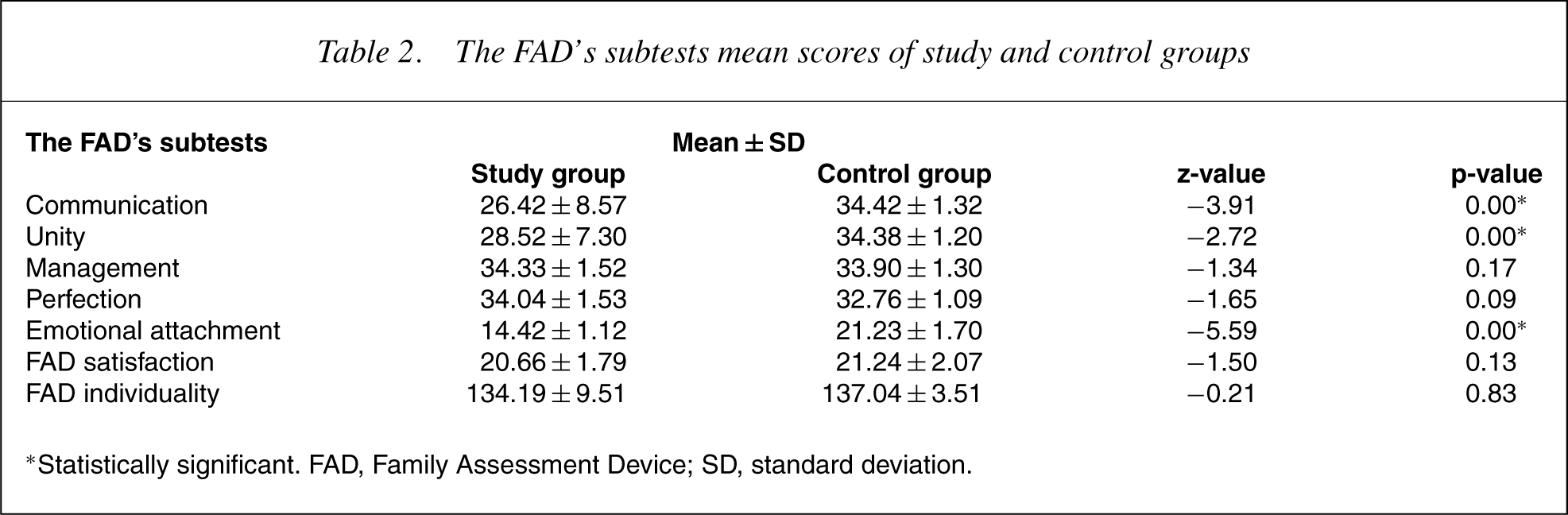
∗Statistically significant. FAD, Family Assessment Device; SD, standard deviation.
Discussion
In our study, the frequency of EDs was found to be 2.20% in university students in a rural area of Turkey. Of this, the percentage of BN was 1.57% and the percentage of BED was 0.31% for females. The particularly interesting aspect of this research is the BN frequency so similar to Western countries. No cases of AN was not found. Similar to our study two other studies done in our country did not find any AN [4, 18]. AN occurs approximately 1–2 in a thousand in Western samples, so not detecting AN in small epidemiological samples is the norm in the Western samples. The results in our study are similar to those of studies done both in Western societies and in our country [3, 18,28–33]. In Western societies the physical appearance of women is emphasized in their sexual role and being excessively thin is the ideal for acceptance and success in society. Although earlier having a thin body appearance has been evaluated as unhealthiness and weakness especially in rural areas of Turkey, in the last decades this idea has been changed by the increasing effect of the media so that being thin is accepted as the sign of the beauty. Furthermore, it is not surprising that the prevalence of ED even in rural areas of Turkey is the same as Western countries.
Low self-esteem has been identified as an important risk factor for EDs [5]. Silverstone suggested that low self-esteem is a frequent finding in BN, and EDsmight be the result of chronic low self-esteem [6]. Low self-esteem is also an important sign that shows the bad prognosis of ED [7]. In this study, the self-esteem of the study group was found to be significantly lower than the control group. Body image is important for a woman's self-perception and determining self-esteem [34]. Men, however, are at lower risk for EDs because they do not define their selfesteem and self-worth by external appearance [35]. In this study neither AN nor BN was found in men. Moreover, 18 of the 21 subjects in the study group were female and the study group had lower self-esteem than the control group supports this theory.
There are a number of studies in Western societies on the subject of whether or not a history of childhood abuse and neglect is a risk factor for EDs [8–11,36–38]. It has been reported that the history of childhood sexual abuse can be a risk factor for bulimic behaviours [9, 36, 37]. In 2000, a study by Kent et al. showed that the influence of childhood emotional abuse on EDs is more than that of sexual and physical abuse [10].
In this study, a history of childhood sexual and emotional abuse was found significantly more frequently in the study group than in the control group. The findings obtained in this study regarding childhood abuse and neglect correspond with studies done in Western societies, which has found this relationship [8–11,39]. Because in our country there are no other studies available on this subject, it is very difficult to make a good evaluation. Nevertheless, it can be said that it is necessary to study the history of childhood abuse and neglect as the risk factors for EDs in these subjects.
It is reported that there is a disorder of family functioning in people with EDs [12–14,40]. It has been observed that compared to healthy families in families of patients with BN there is more enmity between parents and daughters, less love, more blaming, rejection and neglect in relationships. On one side the patient lives with conflict and from the other side a compulsory relationship that does not allow clarification of conflict [41]. In another study, it was reported that the relationships in families of bulimic patients have unmet needs for interest, empathy and support and thus vomiting is the result of the feelings of enmity, rejection and restriction against own family [42].
In 1999, Tachi et al. studied family roles in patients with BN and BED as diagnosed according to DSM-III-R criteria. Relationships were found between disengaged, rigid family environment and purging type of BN; rigid and chaotic family environment and purging symptoms in BED [43]. In our country a recent study with high school students found that study group subjects had a higher frequency of having criticism in the family, blaming, incompatibility history in the family and witness to physical violence in the family [18].
In our study, the scores, which show FAD communication, unity and emotional attachment, were significantly lower in the study group than the control group. These results reveal that the students in the study group perceive their family more problematic regarding expressing themselves in the family freely, enmeshing or irrelevancy of the family members, and the feelings of love, peace and sympathy within the family environment, compared to the control group. The findings of this study related to family roles are consistent with the results of other studies, which shows that there is a disorder in family roles of patients with BN [12, 13, 18,40–43]. But because there is very limited number of studies on this subject in our country, we think that is necessary to approach these results with precaution.
Conclusions
Eating disorders are seen more frequently in Western societies than in other societies. However, in this study the rate of incidence that was found did not show a clear difference from the incidence in Western societies. Research carried out that shows EDs are particular to the culture should be examined again, and it is necessary to study the risk factors in those with EDs of low selfesteem, childhood abuse and family roles. There is very limited research in our country about the frequency and characteristics of EDs. This situation limits the possibility of making good evaluations of research.
In Turkey, there is a need to expand research using wider samples from the general population in different regions of the country, outpatient and inpatient patients, and adolescents and young adults identified as at risk. Such research would assist in identifying the frequency and characteristics of these disorders, increase the awareness of these disorders and improve methods of treatment. However, the results of this study showthat it is necessary to pay attention to levels of self-esteem, family functioning and a history of childhood abuse in the treatment of EDs. It is thought that it is correct to consider the factors that are able to affect treatment.