
Abstract
Keywords
Youth suicide is currently the second leading cause of premature death among young Australians. The identification of young people at risk of suicide is often complicated by coexisting psychosocial stressors, psychological [1] and/or physical morbidities [2]. It therefore remains unclear as to which particular antecedents are necessary and sufficient factors to result in a suicide attempt.
The presence of psychiatric disorder [3–7], particularly depression [8–11], has been the most frequently identified risk factor for attempted suicide and death by suicide. From their analysis of depressive comorbidity studies, Angold et al. [1] concluded that the likelihood of comorbidity in the presence of depression exceeded the likelihood of depression in the presence of another psychiatric disorder. For example, attention deficit hyperactivity disorder and anxiety were more common in depressed than in non-depressed children and adolescents [1]. However, Gould et al. [12] found that school-related problems and stressful life events increased the risk of death by suicide among adolescents, even after accounting for psychiatric disorders.
Other factors contributing to suicide risk have included a family history of either suicide [7] or psychiatric disorder [9,13,14]; unemployment among older youth [15]; a history of sexual abuse [16,17] and a previous suicide attempt [18,19]. Chronic medical conditions such as type 1 diabetes mellitus [20], asthma [21] and epilepsy [2] have also been implicated. One study found that a history of a medical condition independently predicted repeated suicide attempts [22].
Despite the vast body of knowledge on suicidal behaviours, primary suicide prevention efforts may never reach their target audiences. For some young people, contact with the health services may only ever occur with a presentation to an emergency department after having already attempted suicide [23]. Within the 12 months following a suicide attempt the risk of suicide or another attempt has been estimated to be as high as 100 times greater than those who have never made an attempt [24].
However, most young people who attempt suicide do not re-attempt or die by suicide. Thus, risk factors associated with a one-off suicide attempt may differ from factors associated with repeated suicide attempts. The current exploratory study was undertaken as a first step in the development of a critical pathway for the management of attempted suicide among adolescents admitted to hospital following a suicide attempt. The primary purpose of this study was to delineate factors associated specifically with repeated suicide attempts among adolescents.
Methods
Attempted suicide is defined as either the ingestion of drugs in excess of the recommended therapeutic dosage, and/or self-inflicted injury, with some intention of ending one's life. A comprehensive psychosocial and psychiatric assessment by the on-call psychiatric registrar is mandatory at the study hospital (Royal Prince Alfred Hospital) for all patients assessed by nursing or medical staff as having attempted suicide. Some presentations may have been deemed a suicidal act by the assessing clinician or other appropriate health professional, even though the patient may have been ambivalent about, or denied their intention of suicide. These assessments are documented in the medical records. Cases are then routinely coded according to the International Classification of Diseases (ICD-9) coding system.
The sample for this study was identified with a central hospital inpatient database search, using the ICD-9 E-codes E950.0 to E959.0 for attempted suicide. Potential subjects included all adolescents (13–20 years, n = 118) admitted to an inner-city teaching hospital during a 36-month period between 1994 and 1996, and who received an E-code for attempted suicide. A high inclusion rate was obtained (95%, n = 112). Reasons for exclusion included death soon after hospital admission (n = 1), missing file (n = 1) and patient not waiting for psychiatric assessment (n = 4). An unknown number of cases that might have been incorrectly diagnosed or coded, have also been unintentionally excluded from this study.
When a patient had been admitted to hospital following an attempted suicide on more than one occasion, the first admission during the study period was taken as the index attempt. Subsequent attempts within the following 12 months were also documented. A database search was also conducted at the Coroner's Court in order to establish if any of the patients included in the current sample had died as a result of suicide since their last hospital admission for a suicide attempt.
Study variables
The variables of interest were selected on the basis of data available in the medical records and factors previously shown to be associated with self-harming or suicidal behaviours. The demographic parameters included age, sex, occupation, living arrangements and ethnic origin. The variable ‘psychiatric disorder’ included disorders which had previously been diagnosed (and which were still clinically relevant) and disorders provisionally diagnosed at the index attempt.
Other variables included a history of sexual abuse, chronic medical conditions/illnesses, previous and subsequent suicide attempts, and the context of the index attempt. Whether or not alcohol had been consumed at the time of the index suicide was based on self-report.
A chronic medical condition was defined as a medical condition which was not of finite duration and which was associated with the need for continuous medical treatment and/or regular medical review (e.g. physical disability with recurring problems, asthma, epilepsy or diabetes). Psychiatric disorders were categorised as follows: depressive disorders (e.g. major depression, manic episode and dysthymia), non-affective psychotic disorders (e.g. schizophrenia, schizophreniform, schizoaffective and delusional disorders and atypical psychosis), personality disorders (e.g. borderline, dependent, antisocial and unspecified), adjustment disorder with or without brief depressive reaction (e.g. acute stress reaction and post traumatic stress disorder) and substance abuse or dependence disorders.
A history of rape was understood as including any single episode of unwanted sexual intercourse. Child sexual abuse (CSA) was defined in accordance with the New South Wales Child Protection Guidelines [25] which include any sexual act or perceived threat imposed on a person under the age of 18 years by an older person, as stipulated in Section 3 of the Children (Care and Protection) Act 1987 [25].
Data coding
Due to the retrospective nature of inquiry, it was not always possible to distinguish between nonexisting conditions and missing data. Data that were not routinely collected during assessment, or which were likely to be under-reported, included information about sexual abuse, chronic illnesses, alcohol intoxication and previous and subsequent suicide attempts. Responses for these variables were coded as either ‘yes’, or ‘no/uncertain’.
Statistical analysis
Data were analysed using
Results
Sample characteristics
The sample was comprised of 36 male and 76 female adolescents. The mean age for males (18.6 ± 1.4 years) was significantly higher than for females (17.5 ± 2.0 years; t = 3.07, p = 0.003). The average length of hospital stay was 3.5 ± 9.4 days (Range: 1–78 days).
The majority of adolescents were identified as being born in Australia (63.4%; 17% unknown). There were no significant differences between the distribution of males and females for living conditions, classification of occupation or for the presence of at least one chronic medical condition/illness (asthma = 26%, epilepsy = 4%, other = 12%). However, female adolescents (34%) were significantly more likely than males (14%) to have reported a history of sexual abuse (χ2 = 5.04, p = 0.025).
Seventy-nine per cent of adolescents had attempted suicide in the context of a relationship break-up or a dispute with a family member or partner. The precipitating event was unknown for 12% of patients. Poisoning by solids or liquids was the most frequently used method for suicide attempts (87%), followed by cutting/piercing (9%). Two patients attempted suicide by jumping, one with a firearm, and two used a combination of poisoning and cutting/piercing. A significantly greater proportion of males (33%) compared with females (5%) had consumed alcohol at the time of their suicide attempt (χ2 = 15.34, p < 0.0001).
According to the medical records, 39% of the sample had attempted suicide on more than one occasion. There were no statistically significant differences between the proportion of males and females who had attempted suicide prior to (males: 28%, females: 21%) or within 12 months of (males: 31%, females: 25%) the index suicide attempt.
Psychiatric morbidity was present for 76% of adolescents at the time of the index attempt. Depressive disorders were most prevalent (46%) followed by alcohol abuse/dependence (35%), drug abuse/dependence (27%), adjustment (24%), non-affective psychotic (16%) and personality disorders (9%). Comorbidity was present for 38% of adolescents. Personality, non-affective psychotic and substance abuse disorders often co-occurred with depression (64%, 50% and 59%, respectively). Personality disorders also tended to co-occur with substance abuse disorders (64%). Males were more likely than females to have been abusing drugs (χ2 = 14.1, p < 0.001) or alcohol (χ2 = 6.0, p = 0.01), and to receive a comorbid psychiatric diagnosis (χ2 = 11.02, p < 0.001).
Five patients (4.5%) had died by the end of the study period. One male with schizophrenia and one female with borderline personality disorder died by suicide within one year of the index attempt. Both these adolescents had drug abuse disorders. Within 2 years of the index attempt, two more females were deceased. One of these, for which the mode of death was undetermined, was diagnosed with adjustment disorder in the context of a relationship break-up. The second of these females was diagnosed with borderline personality disorder and the mode of death was determined to be suicide. Within the third year, a fifth female adolescent had died following an accidental overdose. Although this patient had a lengthy history of recurrent major depressive disorder and affective psychosis, no diagnosis was given at the time of death.
Variables associated with subsequent suicide attempts
Chi-squared analyses were conducted for all categorical variables, except age, using suicide re-attempt within 12 months of the index attempt as the dependent variable. At the probability level of 0.05, subsequent suicide attempts were univariately associated with personality and substance abuse/dependence disorders, and the coexistence of two or more disorders (Table 1).
Univariate analysis of psychiatric disorders based on whether or not patients had re-attempted suicide within 12 months of the index attempt (n = 112)
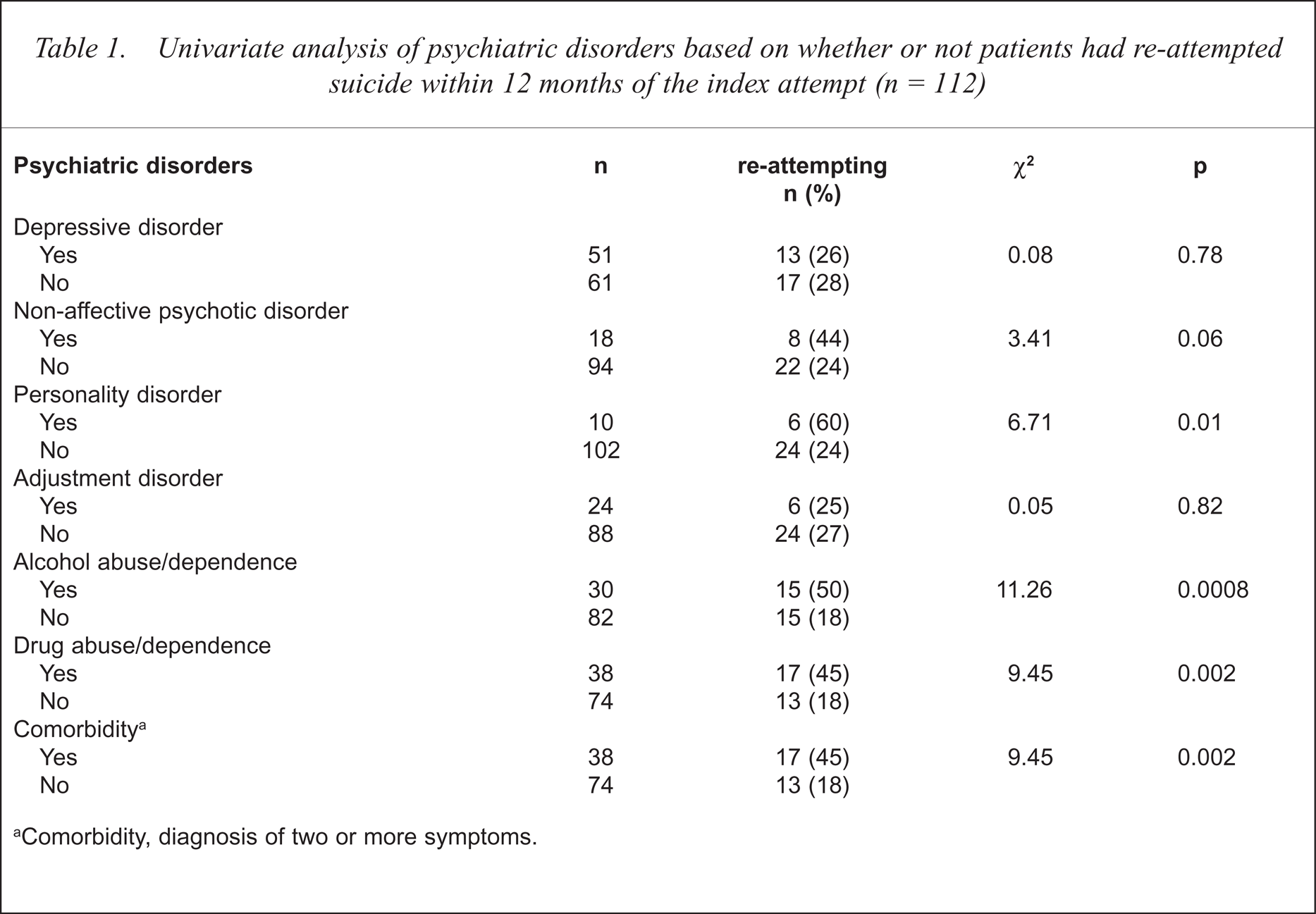
Comorbidity, diagnosis of two or more symptoms.
The age distribution was negatively skewed. Consistent with this graphical assessment, the Kolmogorov-Smirnov statistic was highly significant (Lilliefors significance p = 0.0001), indicating that age was a non-normal variable. Therefore, the non-parametric analogue of regression, logistic regression, was conducted for the variable age. However, age did not distinguish between patients who had or had not re-attempted suicide within 12 months (OR = 1.16, 95% CI = 0.92–1.47, p = 0.21). Other variables not univariately associated with subsequent suicide attempts at p < 0.05 were sex, living arrangement, classification of occupation, sexual abuse, chronic medical condition/illness and prior suicide attempts (Table 2).
Univariate analyses of patients' characteristics based on whether or not they had re-attempted suicide within 12 months of the index attempt (n = 112)
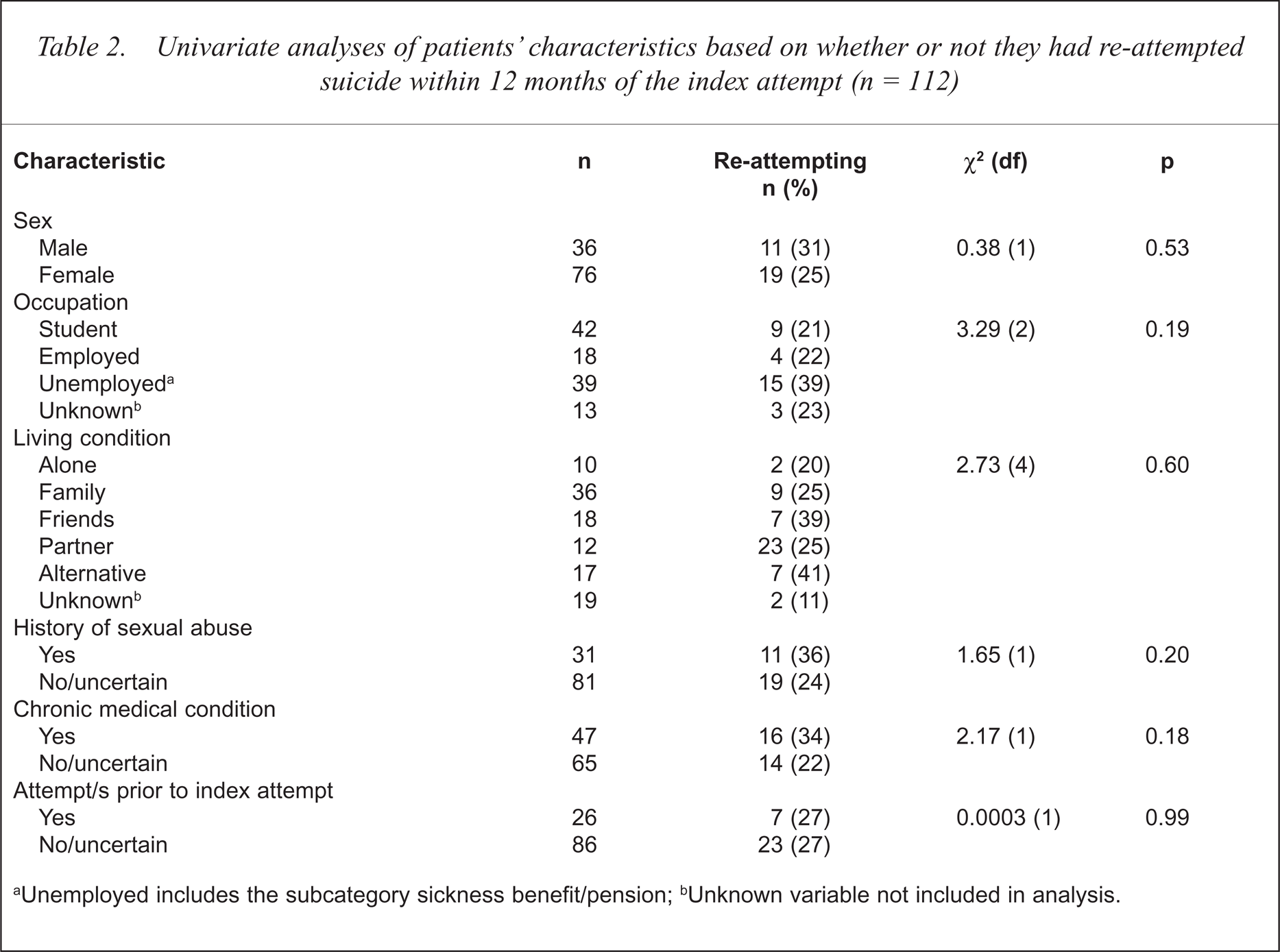
Unemployed includes the subcategory sickness benefit/pension;
Unknown variable not included in analysis.
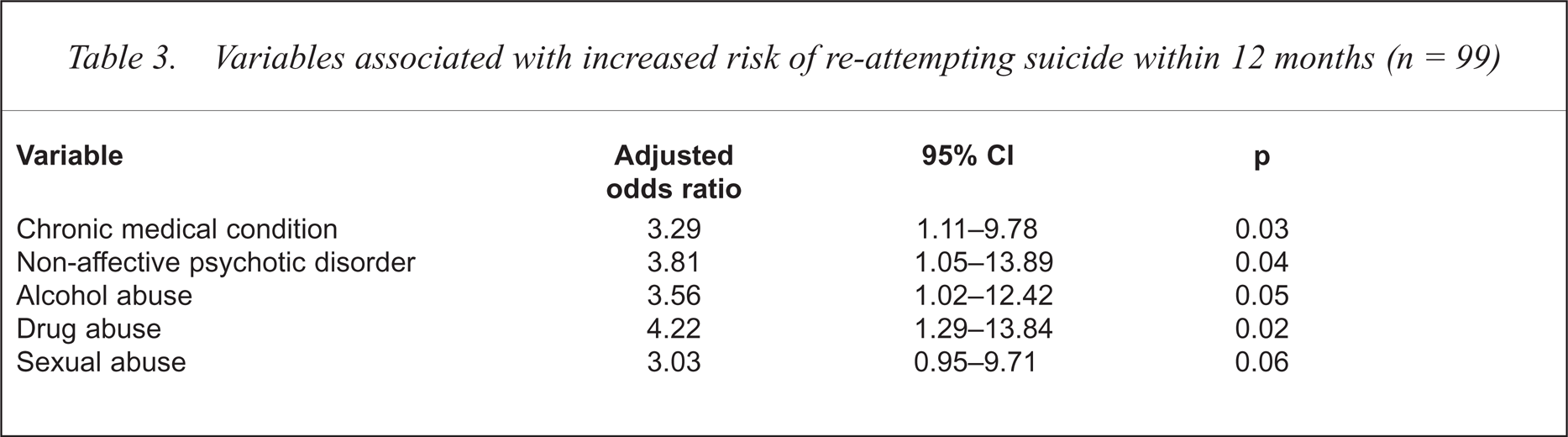
The eight variables selected for entry into the multivariate analysis included age, classification of occupation, sexual abuse, chronic illness, non-affective psychotic disorder, alcohol and drug abuse/dependence disorders and comorbidity of any of these eight variables. Although a diagnosis of a personality disorder was significantly associated with repetition of suicide (Table 1), an insufficient proportion of the sample were affected by this disorder. Therefore, personality disorder could not be meaningfully modelled. Thirteen cases were rejected due to missing data for occupation, and therefore the regression analysis was based on 99 cases. The adjusted odds ratios and 95% confidence intervals for the five variables retained in the final solution are shown in Table 3.
Variables associated with increased risk of re-attempting suicide within 12 months (n = 99)
Discussion
The main objective of this study was to identify factors associated with repeated suicide attempts among adolescents who were hospitalised after attempting suicide. Consistent with previously reported sex ratios, twice as many females as males were hospitalised for attempted suicide during the study period [18,29]. However, the 1-year repetition rate did not differ significantly between male and female adolescents [30,31].
Sexual abuse was most likely underestimated among the current sample due to non-reporting and non-documentation in the medical records. Exploring issues around sexual abuse presents clinicians with a particularly delicate situation as young people are unlikely to reveal abuse during a one-off initial assessment in the emergency department. Despite this, the prevalence of reported sexual abuse among our sample was considerably higher than in other published literature for either adolescents [32] or adults [16,17] found by other workers. A history of sexual abuse was almost a significant predictor (p = 0.06) for repeated suicide attempts among our sample, after adjusting for other factors. A history of CSA, in particular, has been found to more strongly predict self-destructive behaviour than individual characteristics and other negative childhood and adult stressors [17]. Furthermore, cycles of self-destructive behaviour among survivors of childhood victimisation may be exacerbated by the use of substances such as alcohol, presumably as these decrease inhibition [33].
The high rate of self-reported asthma in our study is surprising. Within the current study hospital's Area Health Service, an adult health survey showed that 14% of the general community had at some stage been diagnosed with asthma. Of these, only 9% were currently asthmatic while 5% had a history of asthma [34]. It is therefore possible that asthma has been over-diagnosed in the study group and that the respiratory symptoms are related to anxiety and hyper-ventilation syndrome. Excessive and inappropriate use of readily available beta adrenoreceptor agonist inhaler therapy, in an attempt to alleviate symptoms, may exacerbate anxiety and behavioural sequelae. Our review of the literature failed to locate previously published studies examining the association between asthma and repeated suicide attempts among adolescents. Allard et al. [22] reported that a history of medical problems (but not current medical problems) predicted repeat suicide attempts. However, as approximately 50% of patients were over the age of 30 years, and neither the types of illnesses nor their chronicity were specified by the authors, the study is not entirely comparable to ours. The presence of a medical condition was also included for analysis in Goldstein et al.'s [27] predictive study, but was not retained in their final model.
Consistent with previous studies, psychiatric morbidity was highly prevalent among the current sample. Our finding that depressive disorders were not significantly associated with subsequent suicide attempts has been previously reported among samples across the age span [19,22]. Nonetheless, caution should be exercised when interpreting our results. The association between depression and repetition may be confounded in the first instance because suicidal ideation is one of the diagnostic criteria for depressive disorders. A diagnosis of a depressive disorder may in part be an artefact of diagnostic criteria [35,36], and therefore result in its over-diagnosis and low predictive utility. The extreme opposite is also possible. In their review of 23 studies, Goldney and Pilowsky [37] found that, when using objective rating scales, depression was diagnosed at double the rate compared with when clinical judgement was used. As a diagnosis of depression in the current study was based on clinical judgement, an underestimation of its prevalence is also a possibility.
It is also important to consider that some patients may not have been diagnosed with depressive disorder, yet depressive symptoms may have been a predominant feature at the time of diagnosis of other disorders. This is particularly the case in adjustment disorder with depressed mood, which in many ways clinically aligns itself with depressive disorder. In fact, Gotlib et al. [38] reported that adolescents who exhibited high levels of depressive symptoms without fulfilling the diagnostic criteria for major depressive disorder (MDD), did not differ significantly from those who were diagnosed with MDD on most measures of previous and subsequent psychosocial dysfunction.
Depressive disorders may also be associated with longer-term risk not accounted for over our 1-year follow-up period. For example, Kovacs et al. [39] reported some interaction effects between childhood/adolescent depression, adult depression and attempted suicide during adulthood. Merikangas et al. [40] found a strong association between repeated suicide attempts and the severity of depression over the longitudinal course.
A larger than would be expected proportion of our sample was diagnosed with a non-affective psychotic (18%) or personality (9%) disorders. Even so, it is important to recognise that such disorders may be in evolution during adolescence and clear symptomology may not manifest until late adolescence or early adulthood. Non-affective psychotic and personality disorders are therefore likely to be under-diagnosed among adolescents. Nevertheless, the presence of non-affective psychotic disorders such as schizophrenia significantly increased the likelihood of repetition among the current sample of adolescents, as found by van Aalast et al. [19]. Personality disorders also demonstrated a strong univariate association with suicide reattempts. Although we were unable to account for personality disorders in a multivariate analysis, the risk posed by such disorders has previously been reported [22].
Independently, non-affective psychotic or personality disorders might present greater risk of suicide repetition than depression, because such disorders tend to be more longstanding and the most likely to be associated with substance abuse and with severe to extreme levels of psychosocial stress [7]. Consequently, excessive cognitive disorganisation and disruption to psychosocial functioning are likely to result. The impairment to daily functioning caused by mental illness itself, coupled with the need of adolescents to accomplish normal developmental tasks, may exceed their coping capacity and therefore present significant risk of suicide.
In the current study, both drug and alcohol abuse independently posed significant risk of repetition. While substance abuse is common among those who attempt or die by suicide [5,9,22,36], the association between substance abuse and repetition is less clear. Alcohol abuse among depressed adolescent in-patients has been associated with both increased frequency of suicide attempts and greater medical morbidity associated with the attempt [41]. Allard [22] found that drug, but not alcohol, abuse predicted subsequent suicide attempts. In another study, while drug abuse was correlated with a previous suicide attempt, neither type of substance abuse was associated with subsequent attempts [19]. Nevertheless, substance abuse is likely to intensify long-standing social and interpersonal difficulties [42], and to be associated with severe to extreme levels of psychosocial stress [7].
It is interesting that in our final statistical model, a previous suicide attempt was not a predictive risk factor for a suicide attempt. A suicide attempt may increase the risk of suicide beyond the extent which would be found in an at risk group who have never attempted suicide [24]. However, contrary to previous studies [19,22,27,36] repetition within 1 year was not associated with past suicide attempts. It is, however, possible that the risk of repetition is related directly to the actual number of previous suicide attempts rather than their mere occurrence. Indeed, Goldstein et al. [26] found that the likelihood (odds ratio) of repetition increased proportionately to the number of previous suicide attempts. Similarly, De Moore and Robertson [43] found that more than one suicide attempt within 1 year predicted suicide within the next 18 years. Nevertheless, given that a previous attempt was not a distinguishing risk factor, the risk among adolescents presenting with attempted suicide for the first time should not be underestimated.
The reliability of the study data is limited by the possibility that the medical records contained incomplete or inaccurate psychiatric, medical or psychosocial histories, and, in particular, information about previous suicide attempts [44]. Also, subsequent suicide attempts were only acknowledged if the adolescent returned to the study hospital. Moreover, we can not draw any firm conclusions regarding causality as we can not be certain that identified risk factors preceded repeated suicide attempts [18]. There were some significant differences between males and females, and therefore the data are also limited by the small proportion of males in the study which precluded the viability of separate modelling for each sex.
There are likely to be many other important psychosocial risk factors [18] that were not documented in the medical records, and therefore, not investigated here. It appears however, that the risk of repetition may be relative to the level of dysfunction associated with certain types of psychiatric disorders or adverse life events. Risk factors which are known to be associated with high levels of dysfunction, such as those predictive factors identified in this study, tend to be multifaceted in their nature and identification of ongoing risk and acute care is likely to be complicated. Nevertheless, discerning the extent to which adolescents are able to function within their environment, might be a valuable indicator for risk potential and could form part of the clinical assessment in the emergency department. Further research on the relationship between psychosocial dysfunction, specific types of psychiatric morbidity, psychosocial stress and repeated suicide attempts is needed to test the worthiness of our assertion.
There were also many adolescents who presented with an attempted suicide and who did not exhibit risk of repetition as measured by the identified predictor variables. Yet a substantial proportion re-attempted suicide within the following year. Clearly, all suicide attempts warrant serious attention regardless of whether or not psychiatric morbidity is a prominent feature and regardless of how trivial the reasons for attempted suicide may initially appear. All young people who have attempted suicide should receive an extensive mental health and psychosocial assessment, with a follow-up appointment being arranged prior to leaving the emergency department. Given the array of characteristics and potential risk factors that adolescents may present with, a broad-based, multidisciplinary intervention approach is strongly recommended.
Acknowledgements
The authors thank the Commonwealth Department of Health and Family Services for funding under the National Youth Suicide Prevention Strategy, and note that the views expressed in this paper are those of the authors, and not necessarily endorsed by the funding body. We also thank Malina Gattellari (Research Psychologist, the University of Sydney) for her assistance with the data analysis.