
Abstract
Objective:
Previous research has found an alarmingly high rate of psychosis in Indigenous1 patients from remote communities of Cape York and the Torres Strait with the treated prevalence of psychosis four times higher than that found for the Australian population. This study assesses comorbid illness and risk factors among this same cohort of psychosis patients.
Methods:
Data were collated from a clinical database that contains complete psychiatric records from 1992 to 2015, extracted for all Indigenous patients who received treatment for a psychotic disorder from the Remote Area Mental Health Service. Descriptive analysis and logistic regression models explored differences across subgroups of ethnicity and sex, and relationships between co-morbid disorders and risk factors. All multivariate models included variables of age, year of birth, sex and ethnicity.
Results:
Sixty per cent of participants (n = 256) experienced a comorbid mental or substance use disorder. Forty-five per cent (n = 192) of participants experienced a physical comorbidity. The most frequent physical health outcomes were injury (29%, n = 93), diabetes (18%, n = 58) and cardiovascular disease (21%, n = 68). Risk factors considered to play a potential biological or neurodevelopmental role in the development of psychosis were approximately three times more likely in Aboriginal (odds ratio = 3.2; 95% confidence interval = [2.0, 4.9]) versus Torres Strait Islander patients, and those born after 1980 (odds ratio = 2.5; 95% confidence interval = [1.6, 3.9]) versus those born prior to 1980. Environmental or contextual factors were associated with significantly greater risk among Aboriginal (odds ratio = 3.8; 95% confidence interval = [2.4, 6.0]) compared with Torres Strait Islander patients.
Conclusion:
Our data expose the perinatal and early environment of Indigenous children who later developed a psychotic disorder. As risk factors for schizophrenia may be cumulative and interactive, both with each other and with critical periods of neurodevelopmental vulnerability, our results suggest possible causes for the increasing prevalence of psychotic disorders between 1992 and 2015.
Introduction
Despite well-documented inequality in physical health between Indigenous and non-Indigenous Australians (Vos et al., 2009), with more than twofold the disease burden in the former, the inequality in Indigenous mental health has received less attention. Jorm et al. (2012) reported a threefold excess in prevalence of self-reported psychological distress in Indigenous adults compared to the general community with mental and substance use disorders accounting for 19% of the total Indigenous burden(Australian Institute of Health and Welfare, 2018; Jorm et al., 2012). However, the immense health disadvantage of those affected by both physical and mental illness living in remote areas has not been well documented. In this paper, one in a series of articles investigating psychosis in communities across one region of remote Indigenous Australia, we assess comorbid mental and physical diseases, injuries and risk factors affecting Indigenous people living with psychosis.
In our first study (Gynther et al., 2019), we reported on data collated from a unique clinical database that contains complete psychiatric records of all Indigenous patients from remote communities of Cape York and the Torres Strait who were treated for psychotic disorders from 1992 to 2015. This database was maintained by psychiatrists from the Remote Area Mental Health Service (RAMHS, Queensland Health). We found alarmingly high rates of psychosis with the age-standardised treated prevalence of psychosis five times higher in men and three times higher in women than that found for the Australian population (Morgan et al., 2011), with the highest treated prevalence being 4% in Aboriginal men in 2015.
During our 23-year study period, we also found a steady increase in treated prevalence of schizophrenia and schizoaffective disorder in addition to significantly higher prevalence of psychosis among Aboriginal people compared to Torres Strait populations. In contrast, the prevalence of bipolar and depressive psychosis remained unchanged over time in both populations and was similar to those in the general Australian population. We also found an increase in mortality risk among Aboriginal men and women, and Torres Strait women living with psychosis, compared to the Queensland Indigenous population. Social and historical events that may have resulted in an increase in environmental and neurodevelopmental risk factors for psychosis among Aboriginal people in Cape York were suggested (Gynther et al., 2019), but more information is required to explain these results.
This study assesses multimorbidity data for mental, substance use and physical disorders among the same Indigenous cohort. In addition, we present simultaneously collected precipitating and risk factors that may contribute to the extremely high rates of psychosis in this cohort.
Methods
Full details of this study’s methods have been described elsewhere (Gynther et al., 2019). In brief, approximately 0.5% of Queensland’s population resides in the Cape York and the Torres Strait region (Office of Economic and Statistical Research, 2012). The RAMHS clinical database was established in 1992 using Filemaker Pro. In 1998, all records were transferred to and then maintained on Microsoft Access. The database contains the complete psychiatric clinical records of RAMHS, with documentation of the assessment, diagnosis and ongoing management of patients. For this study, one investigator and RAMHS psychiatrist (B.G.) extracted data from the database for all Indigenous patients who received treatment from RAMHS between 1992 and 2015 for a psychotic disorder meeting the following International Classification of Diseases, 10th Revision (ICD-10) diagnostic codes (World Health Organization, 1993): organic-related – F06; substance use-related – F10-19; schizophrenia-related – F20-22; acute and transient psychoses – F23; mood disorder-related – F25, F30-33. The majority of the data were obtained from documentation of comprehensive clinical assessments undertaken at first diagnosis, but data were also extracted from progress notes.
Data were extracted from clinical notes maintained on the RAMHS database and included demographics (such as ethnicity, sex and age at first diagnosis of psychosis) and patient history (such as harmful substance use and other comorbid mental or physical disorders). We also assessed comorbid mental or substance use disorders which met clinical diagnostic criteria (Diagnostic and Statistical Manual of Mental Disorders [DSM] or ICD), as well as substance use which did not necessarily meet the threshold for a clinical diagnosis (American Psychiatric Association, 2000). Substance use other than alcohol or cannabis were categorised in ‘other substances’ and included amphetamines, cocaine, inhalants and solvents (e.g. petrol and paint) and psychedelics (e.g. lysergic acid diethylamide).
Comorbid physical conditions were grouped as per global burden of disease categories of non-communicable diseases (NCDs) (diabetes, cardiovascular, respiratory, renal and neurological), communicable diseases (sexually transmitted infections [STIs]) and injuries (excluding self-harm).
Factors that have been implicated in the involvement of the acute onset of psychosis were examined. Individual factors were also grouped with consideration of which risks could potentially be reduced with available interventions. These were as follows:
Biological and neurodevelopmental factors, including mother drinking during pregnancy, family history of serious mental illness, family history of suicide, low birth weight, failure to thrive, developmental delays, infections (in utero or childhood) and hearing impairment, obstetric complications, born premature, history of seizures and intellectual impairment;
Environmental and contextual factors, including childhood trauma or abuse (physical and/or sexual), intimate partner violence, family violence, physical trauma as an adult (other than intimate partner violence or self-harm), loss of a family member or close friend, adoption/separation from parents at a young age, family history of heavy substance use, parental separation/family breakdown and incarceration prior to diagnosis;
Behavioural factors, including previous alcohol use, previous cannabis use, previous other substance use, patient self-harm or suicidality, conduct or behavioural disorders.
For the purpose of modelling, risk factors and comorbid disorders were considered to be present if they were mentioned by the treating psychiatrist in the clinical notes. It was not possible to extract data regarding the relative severity of risk factors. The percentages with different numbers of co-morbid disorders and risk factors were compared between Aboriginal and Torres Strait Islanders and between sexes. The mean and standard errors of total comorbid disorders and risk factors were also presented.
Logistic regression models were then used to compare comorbid substance use (any alcohol, any cannabis, both alcohol and cannabis) between Aboriginal and Torres Strait Islander patients and between sexes. Similar models assessed the percentages with injuries and specific non-communicable and communicable diseases, as well as selected biological/neurodevelopmental, environmental/contextual and behavioural risk factors.
Level of substance use (none, alcohol only, cannabis only, alcohol and cannabis, and other substances) was assessed as an independent variable in multivariate models. All models included variables age (15–29, 30–39, 40+), year of birth (pre- and post-1980), sex and ethnicity (Aboriginal or Torres Strait Islander). Statistical analyses were undertaken in Stata 15 (College Station, 2015; StataCorp. 2015).
In the papers in this series, the terms Aboriginal and Torres Strait Islander are used when specifying the respective, discrete groups, Indigenous (capitalised) when either or both are being referred to, and indigenous (non-capitalised) for First Nations peoples globally.
Ethics
Ethical approval for this study was obtained from Far North Queensland Human Research Ethics Committee and the University of Queensland. Approval for the research was also obtained in accordance with the Queensland Public Health Act 2005.
Results
Between September 1992 and December 2015, 426 patients were treated for psychosis by RAMHS. Approximately two-thirds were Aboriginal (n = 259) and a similar proportion were from Cape York (n = 270). Females constituted 34% (n = 146) and males 66% (n = 280).
Comorbid mental and substance use disorders
Of our sample, 74% had a comorbid mental, substance use or physical condition (n = 315); 86% of Aboriginal (224 of 259) and 53% (70 of 131) of Torres Strait Islander patients.
Sixty per cent of participants (n = 256) experienced a comorbid mental or substance use disorder which met clinical diagnostic criteria (in addition to psychosis); of these, 241 were diagnosed with a comorbid substance use disorder. The majority of these participants experienced one additional comorbid diagnosis. Nearly three-quarters (73%) of the Aboriginal sample experienced a comorbid mental or substance use disorder (compared with 37% of Torres Strait Islanders) and had more than twice the average occurrence of comorbid disorder than did the Torres Strait Islander patients (Table 1). Males were diagnosed with comorbid mental or substance use disorders more frequently than females (66% and 49%, respectively).
Frequency of comorbid disorders among those with psychosis.
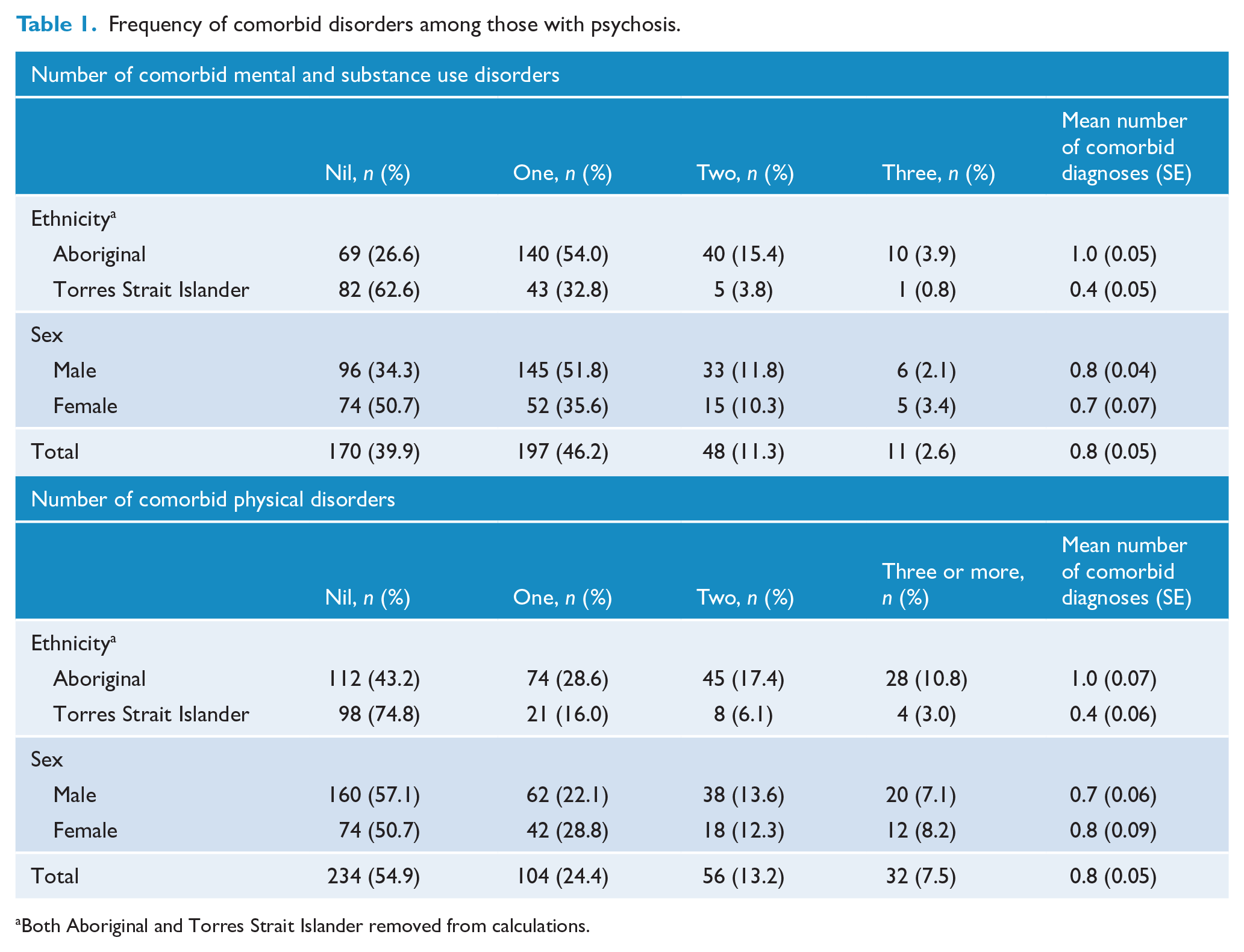
Both Aboriginal and Torres Strait Islander removed from calculations.
Comorbid physical conditions
Forty-five per cent (n = 192) of participants experienced a physical comorbidity. Comorbid physical conditions were reported in almost 60% of Aboriginal compared with approximately 25% of Torres Strait Islander patients, with a mean of 1.0 and 0.4 comorbid conditions, respectively (Table 1).
The most frequently documented physical health outcomes for this cohort were injury (29%, n = 93), diabetes (18%, n = 58) and cardiovascular disease (21%, n = 68) (Figure 1). These causes were followed by STIs, respiratory illness, seizures and renal disease. NCDs accounted for over half of the comorbid physical conditions (58%, n = 188). Injury and STIs increased markedly from pre-2005 to post-2005 (19–25% and 6–14%, respectively; Supplemental Figure S1).
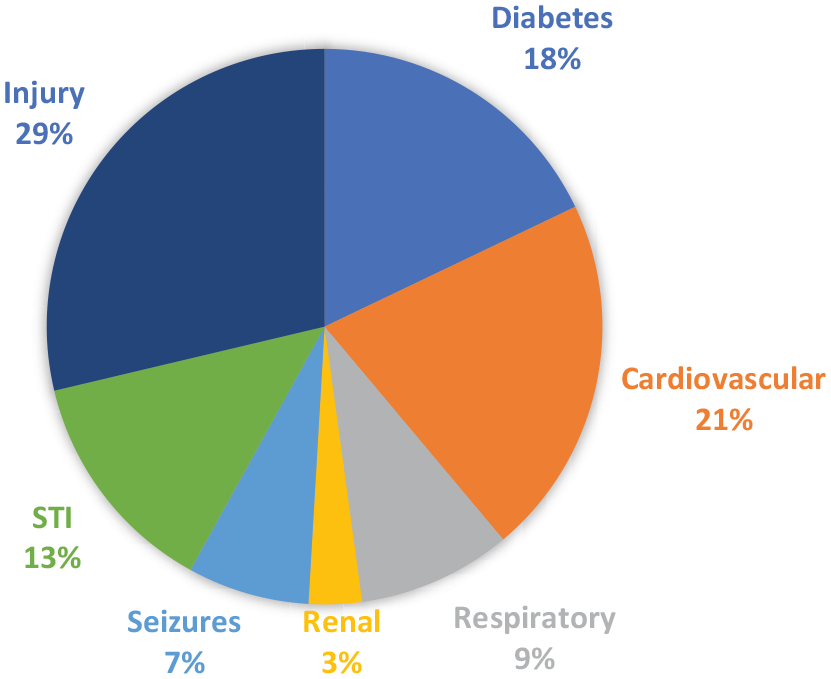
Distribution of comorbid physical conditions as a proportion of total number of comorbid physical conditions in those living with psychosis.
Significant substance use was documented in patients even when an official substance misuse diagnosis had not been attributed. Of 426 patients, 337 (79%) experienced comorbid substance use. Frequencies and odds ratios of comorbid substance use are presented in Table 2. Overall, comorbid alcohol use was 8.3 times more likely in Aboriginal than Torres Strait Islander patients, cannabis use 3.5 times more likely, and both alcohol and cannabis use 4.6 times more likely. Overall, males were two to three times more likely to use alcohol or cannabis than females.
Comorbid substance use in those with psychosis.
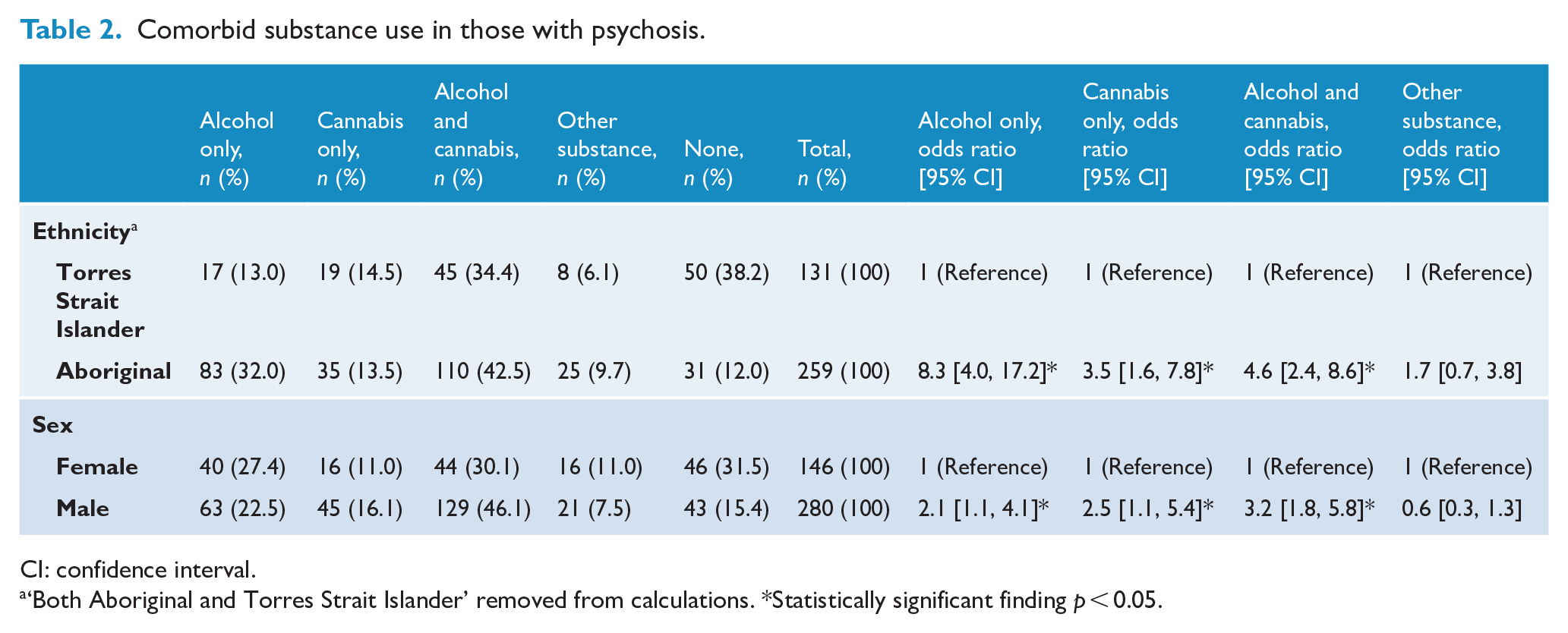
CI: confidence interval.
‘Both Aboriginal and Torres Strait Islander’ removed from calculations. *Statistically significant finding p < 0.05.
Injury was significantly more likely among Aboriginal (32%) compared to Strait Islander patients (2%; odds ratio [OR] = 18.5; 95% confidence interval [CI] = [5.5, 62.2]; Table 3), as was also the case for respiratory illness, STIs and infections. Differences in physical comorbidity between males and females were not apparent, except for injury where the odds were three times higher in males (OR = 2.7, 95% CI = [1.4, 5.2]) and STIs which were two times more likely in females (OR = 0.5, 95% CI = [0.2, 0.9]).
Risk of comorbid physical conditions among those with psychosis, by ethnicity, sex and substance use (odds ratio [95% CI]).
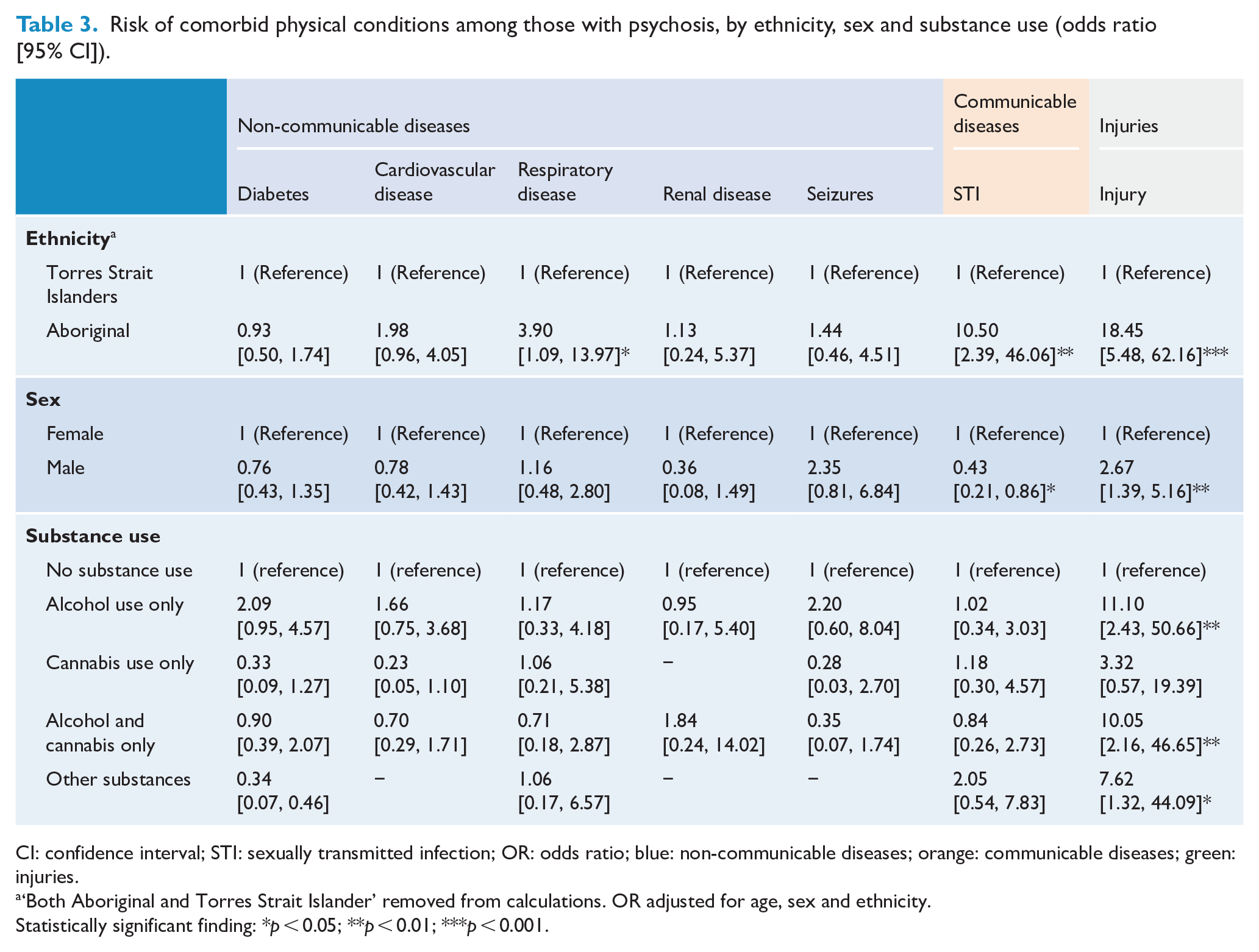
CI: confidence interval; STI: sexually transmitted infection; OR: odds ratio; blue: non-communicable diseases; orange: communicable diseases; green: injuries.
‘Both Aboriginal and Torres Strait Islander’ removed from calculations. OR adjusted for age, sex and ethnicity.
Statistically significant finding: *p < 0.05; **p < 0.01; ***p < 0.001.
Given the prominence of substance use and certain physical conditions in this cohort, we examined associations between these comorbid conditions (Table 3). The most notable findings were that alcohol use, combined alcohol and cannabis use, and use of other drugs led to increased odds of injuries. The rate of injuries in those who do not use substances is low (3.4%). This percentage is increased for all substance use groups, but especially in those who use alcohol or alcohol and cannabis (41% and 27%; not shown). No other links between substance use and increased risk of comorbid physical health outcomes were observed.
Risk factors
Relatively high frequencies of a range of potential risk factors are observed across the lifespan (Figure 2). These include a family history of serious mental illness and substance use (32% and 37% of the cohort, respectively), childhood trauma or abuse (27%), separation from parents at a young age (19%), loss of a loved one (20%), family violence (22%) and alcohol use (25%). On average, participants experienced three risk factors (Supplemental Table S1). Aboriginals experienced a mean of 3.6 risk factors compared with 1.7 for Torres Strait Islanders, and females experienced slightly more risk factors than males (mean of 3.3 and 2.8, respectively).
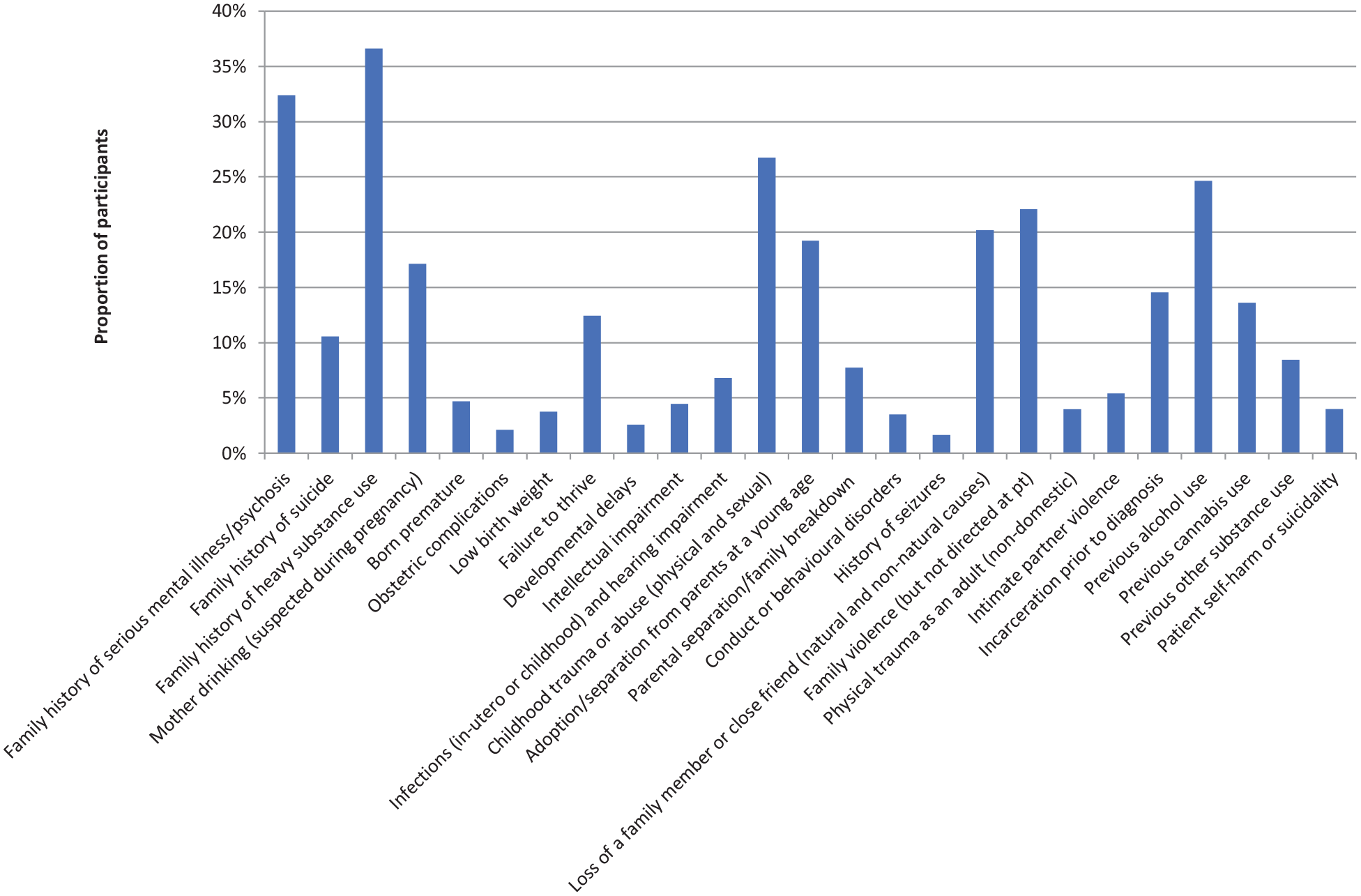
Proportion of sample experiencing risk factors in chronological order across the lifespan (n = 426).
Overall, risk factors considered to play a potential biological or neurodevelopmental role in the development of psychosis were approximately three times more likely in Aboriginal (OR = 3.2; 95% CI = [2.0, 4.9]) versus Torres Strait Islander patients, and those born after 1980 (OR = 2.5; 95% CI = [1.6, 3.9]) versus those born prior to 1980 (Table 4). A family history of suicide demonstrated a statistically significant association with being of Aboriginal descent (OR = 5.5; 95% CI = [1.9, 15.7]); while there was a greater risk of a family history of serious mental illness (OR = 2.3; 95% CI = [1.5, 3.6]), premature birth (OR = 14.6; 95% CI = [3.3, 65.3]) and failure to thrive (OR = 4.8; 95% CI = [2.5, 9.4]) if the participant was born after 1980. Having a mother drinking during pregnancy and childhood infections or hearing impairment were strongly and statically significantly associated with both Aboriginal descent (OR = 14.5; 95% CI = [4.4, 47.8] and OR = 15.2; 95% CI = [2.0, 114.0], respectively) and being born after 1980 (OR = 4.2; 95% CI = [2.4, 7.6] and OR = 3.3; 95% CI = [1.4, 7.6], respectively).
Odds ratios of biological/neurodevelopmental risk factors (odds ratio [95% CI]).
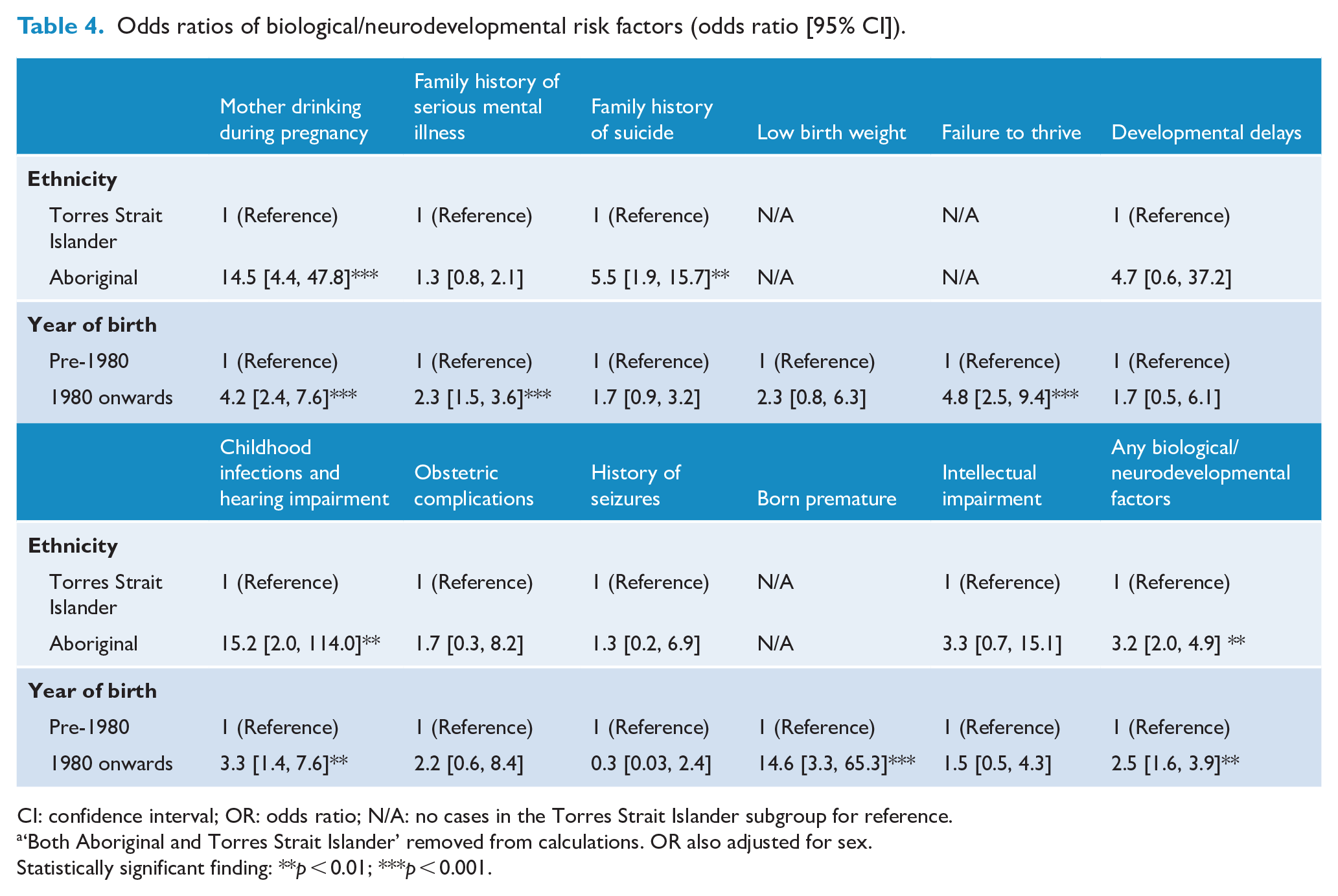
CI: confidence interval; OR: odds ratio; N/A: no cases in the Torres Strait Islander subgroup for reference.
‘Both Aboriginal and Torres Strait Islander’ removed from calculations. OR also adjusted for sex.
Statistically significant finding: **p < 0.01; ***p < 0.001.
Environmental or contextual factors were associated with significantly greater risk among Aboriginal (OR = 3.8; 95% CI = [2.4, 6.0]) compared with Torres Strait Islander patients (Table 5), as was being incarcerated prior to a psychosis diagnosis (OR = 2.1; 95% CI = [1.0, 4.3]). Childhood trauma or abuse (OR = 2.0; 95% CI = [1.3, 3.2]) and family violence (OR = 2.3; 95% CI = [1.4, 3.7]) demonstrated greater risk among those born after 1980. Loss of a loved one, separation from parents at a young age and a family history of heavy substance use demonstrated statistically significant greater risks for Aboriginal patients and those born after 1980.
Odds ratios of environmental/contextual risk factors (odds ratio [95% CI]).
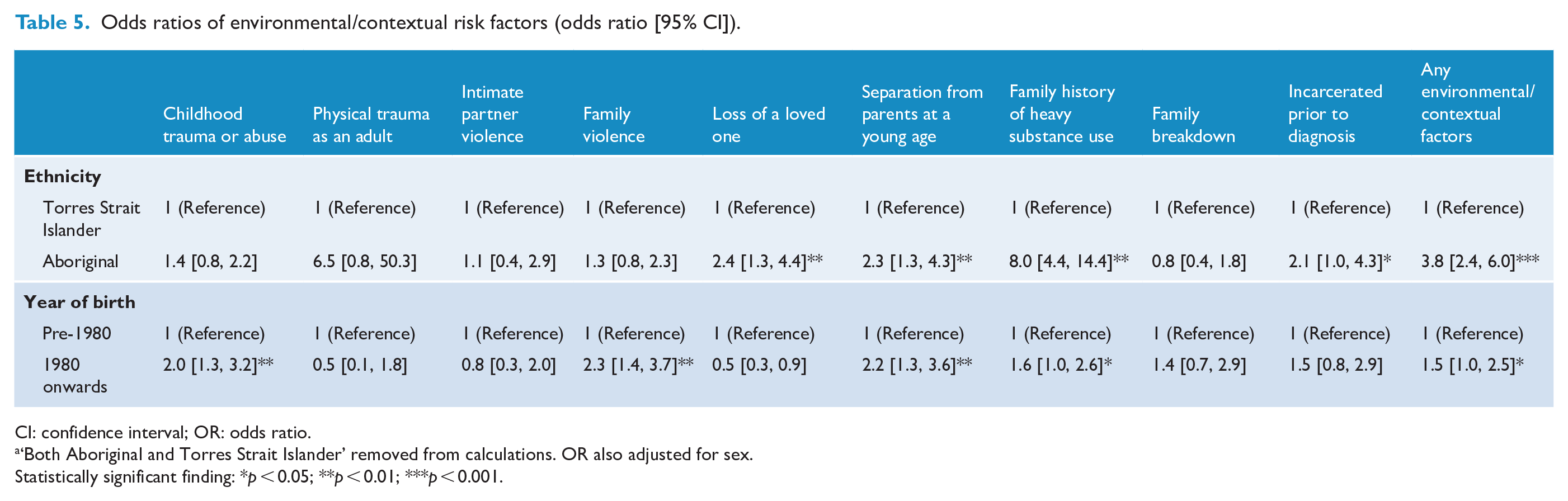
CI: confidence interval; OR: odds ratio.
‘Both Aboriginal and Torres Strait Islander’ removed from calculations. OR also adjusted for sex.
Statistically significant finding: *p < 0.05; **p < 0.01; ***p < 0.001.
Behavioural risk factors which demonstrated significant associations were previous alcohol use (OR = 3.1; 95% CI = [2.0, 4.9]) and self-harm (OR = 8.0; 95% CI = [1.0, 61.8]) among Aboriginal patients, and previous cannabis use (OR = 5.7; 95% CI = [3.5, 9.2]) and other substance use (OR = 7.7; 95% CI = [3.2, 18.2]) in those born after 1980 (Table 6).
Odds ratios of behavioural risk factors (odds ratio [95% CI]).
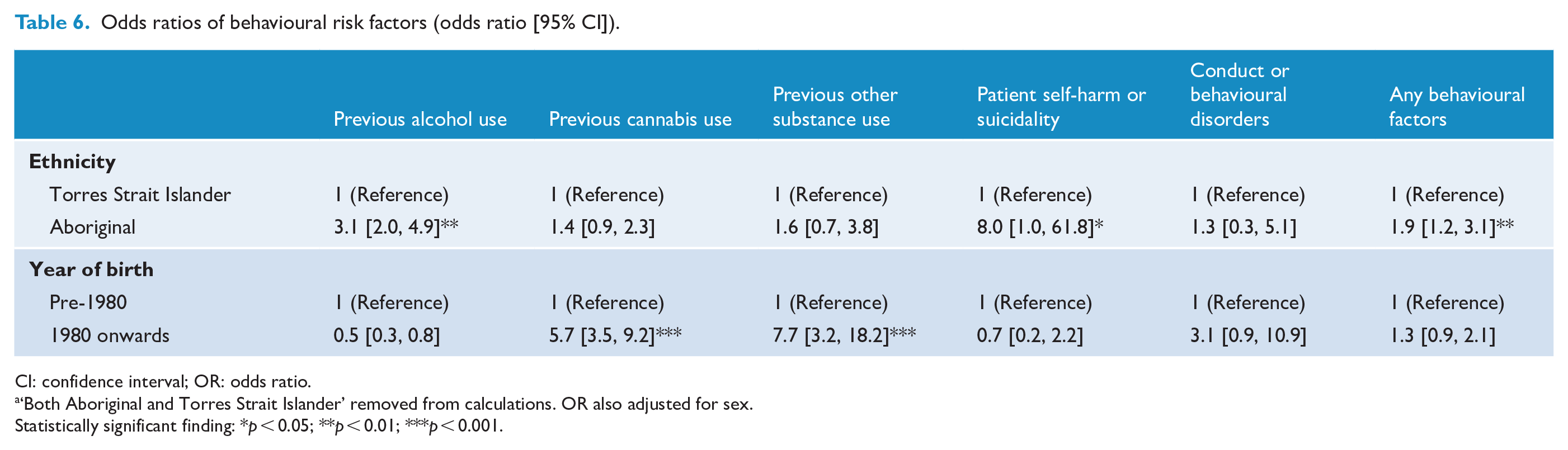
CI: confidence interval; OR: odds ratio.
‘Both Aboriginal and Torres Strait Islander’ removed from calculations. OR also adjusted for sex.
Statistically significant finding: *p < 0.05; **p < 0.01; ***p < 0.001.
Further examination of ‘mother drinking during pregnancy’ revealed this as one of the most influential, yet highly correlated, risk factors (Supplemental Figure S2). After adjusting for ethnicity, sex and birth year, the following risk factors demonstrated significant associations with ‘mother drinking during pregnancy’: family history of suicide, failure to thrive, intellectual impairment, childhood infections or hearing loss, childhood trauma, separation from parents at a young age, cannabis use, other substance use and a history of family substance use.
Given the prominence of injury as a comorbid physical condition, we further explored the relationship between injury and risk factors. After adjusting for ethnicity, sex and birth year, the following risk factors demonstrated significant associations with injury: mother drinking during pregnancy, low birth weight, failure to thrive, childhood infections or hearing loss, alcohol use and family substance use (Supplemental Figure S3).
Acute antecedent factors
Substance use was identified as a potential acute precipitating factor in the onset of psychosis (around 60% of the patients). For patients for whom data were available on the age of initiation of substance use (n = 100), almost all began using prior to the onset of psychosis (96%, mean age of 14.6 years). Other factors reported and identified as potential precipitating factors included family conflict and/or domestic violence (n = 50), and death of a loved one or being a witness to death (n = 47) (Supplemental Table S2).
Discussion
Our findings contribute to an increasing body of knowledge on the effects of social adversity and related environmental stressors on the development of psychosis, in this case in Indigenous populations of Cape York and the Torres Strait Islands.
This study builds upon previous research demonstrating extremely high prevalence rates of psychosis, increasing prevalence over a 23-year period in the Indigenous populations of Cape York and the Torres Strait Islands and differences in the distribution of psychosis between the two groups (Gynther et al., 2019). We proposed that those observations suggested an aetiological role of environmental and neurodevelopmental factors and discussed possible risk factors for psychosis that have been documented in scientific literature. Risk factors may be cumulative and interactive, both with each other, and with critical periods of neurodevelopmental vulnerability (Davis et al., 2016). Here, we have explored the relationships of psychosis with comorbid health conditions and the potential roles of a range of risk factors.
In line with the differences we observed in the prevalence of psychosis, we also observed comparable differences in the distribution of comorbid health conditions and risk factors: 74% of our sample had a comorbid mental, substance use or physical condition; 86% of Aboriginal patients had some degree of comorbidity. Aboriginal and male patients experienced greater comorbidity across all mental and substance use disorders. However, differences in physical comorbidity between males and females were less apparent. Literature on excess physical health comorbidities in people with schizophrenia is well documented, as is the disproportionately high burden of chronic disease in Indigenous people in Australia (Smith et al., 2013; Stubbs et al., 2016).
High frequency of comorbidity was largely driven by two conditions: injuries and substance use. These conditions also stood out in terms of unequal distributions between our sample subgroups. Aboriginal and male patients demonstrated large, statistically significant risk for both outcomes with the Aboriginal risk of injury a staggering 18-fold that of Torres Strait Islander patients. We explored this relationship further and noted a high correlation between injury and substance use – a dominating issue, particularly in the Aboriginal males in our sample. The rate of injury in those who do not use substances was very low. Our data also show an increase in injury in our population by 6% between 2005 and 2015 which may be linked to ongoing challenges that undermine liquor restrictions, particularly widespread and continued access to illicit alcohol. These findings should be contextualised, with research demonstrating increasing rates of traumatic brain injury between 2007 and 2015 in the wider Indigenous populations of northern Queensland (Clough et al., 2017).
Substance use disorders constituted the most frequent comorbid condition, as well as the most prevalent predisposing and precipitating risk factors for psychosis. Whereas the Torres Strait Islander cohort had prevalence rates comparable with a recent meta-analysis of substance use disorders in people experiencing schizophrenia spectrum disorder (Hunt et al., 2018), the Aboriginal cohort had two to three times these rates. The increase in cannabis use among this cohort, particularly from the early-2000s following the introduction of legal restrictions to alcohol in Indigenous communities, is of particular significance, as there is existing evidence for a dose–response relationship between level of use and risk for psychosis (Marconi et al., 2016).
We observed high frequencies of a range of potential risk factors across the lifespan. Six of these occurred in more than 20% of our cohort – family history of serious mental illness, family history of substance use, childhood trauma or abuse, loss of a loved one, family violence and alcohol use. Participants typically experienced multiple risk factors, and the frequency distribution and magnitude of risk factors across all three categories (biological or neurodevelopmental, environmental or contextual, and behavioural) were skewed with a greater burden among Aboriginal patients. However, in contrast to some of our other outcomes where males typically fare worse, females slightly more often experienced a combination of multiple risk factors than males.
Of particular interest are the observed temporal trends of several key risk factors, with those born after 1980 at greater risk compared to those born prior to 1980. These risk factors include mother drinking during pregnancy, family history of serious mental illness, failure to thrive, childhood infections and/or hearing impairment, born premature, childhood trauma or abuse, family violence, separation from parents at a young age, family history of heavy substance use, previous cannabis use and previous use of other substances. With the exception of previous cannabis use and previous use of other substances, all of these risk factors occur during the early developmental years of a child’s life.
We found ‘mother drinking during pregnancy’ as one of the most highly correlated risk factors – particularly among Aboriginal patients and those born after 1980. Alcohol exposure in pregnancy has been associated with a variety of outcomes in the offspring including psychotic symptoms in adolescents (mothers consuming > 21 units weekly) (Zammit et al., 2009). Although our results cannot establish a causal link between alcohol consumption in pregnancy and later development of schizophrenia, alcohol use in this sensitive period has ramifications that are likely inter-related and cumulative with other potentially amplifying factors and is likely to convey an increased risk for Aboriginal children through complex, interactive pathways.
Our findings support those of several other studies. A recent investigation in Western Australia found both maternal schizophrenia and obstetric complications are independently and significantly associated with psychosis in offspring and, after adjustment for exposure to other environmental stressors, the hazard ratio decreased substantially for familial liability but did not change for obstetric complications (Morgan et al., 2019). Previous research has found childhood infection is associated with a nearly twofold risk of adult schizophrenia (Khandaker et al., 2012), hence there is a likely link of increased vulnerability through infections and increased psychosis rates in the Aboriginal cohort.
Meta-analysis found that childhood adversity, including physical and psychological maltreatment, abuse and neglect, increases the risk of developing psychosis almost threefold (McGrath et al., 2017; Varese et al., 2012). Other reviews and meta-analyses consistently converge evidence of adversity including loss, witness to domestic violence, parent death or separation, single motherhood and bullying, with risk of psychosis (Matheson et al., 2013; Trotta et al., 2015; Velikonja et al., 2015). Importantly, exposure to multiple adversities is associated with a linear increase in risk of developing psychosis (Morgan et al., 2020).
The particular vulnerability of Aboriginal compared to Torres Strait Islander residents treated for a psychotic disorder demonstrated in this study underscores the salience of social adversity – broadly and across the lifespan – that is reflected in the higher prevalence rates for the Indigenous populations of this area as a whole compared to non-Indigenous Australians. That intra-group differential (Aboriginal > Torres Strait Islander) is also readily apparent in a wide range of health and social outcomes in the wider Indigenous populations of Queensland that we have drawn on in interpreting findings in the earlier papers in this series (Office for Aboriginal and Torres Strait Islander Partnerships, 2006). The origin of these differences can be found in the distinct histories of Cape York Aboriginal people and Torres Strait populations since colonisation. In our previous paper (Gynther et al., 2019), we discussed how significant social change which occurred in Cape York, peaking through the mid-1980s and 1990s led to social instability, increased alcohol and drug use and violence, with consequences for community and family stability. Our current findings reinforce the increasing research lode demonstrating the importance of social determinants, and the importance of nuanced research methodologies capable of both drawing on real-world clinical data and making sense of the interplay of risk factors (risk amplification) within vulnerable populations.
Limitations
A major limitation of our study is the lack of comparison groups of non-psychotic Indigenous people and non-Indigenous people from Cape York and the Torres Strait. Owing to the unique social, environmental and historical context of Cape York and the Torres Strait Islands, our results may not be generalised to other Aboriginal populations. Furthermore, we have, in previous publications in this series, drawn attention to the particular history and circumstances of the Aboriginal communities of Cape York which we believe not only inform Aboriginal versus Torres Strait Islander vulnerabilities, but which are likely to complicate extrapolation to Aboriginal settings where those factors do not pertain.
As a retrospective study using data from clinical records, the results are influenced by the thoroughness of documentation and the possibility of clinician bias in diagnosis. Risk factors, particularly those arising in the perinatal and early childhood periods, may not have been known or documented by the treating psychiatrist. The psychiatrists usually had access to general medical clinical notes, but these may not have extended back to birth. The judgement by RAMHS psychiatrists of the clinical significance of risk factors was subjective and may have varied between psychiatrists. Due to the clinical focus on the treatment of psychosis, stress-related disorders such as post-traumatic stress disorder (PTSD) and depression may have been underreported. Foetal alcohol spectrum disorder (FASD) lacked uniformly accepted diagnostic criteria up until 2016 (Alcohol and Drug Foundation, 2017, accessed 18 January 2021), which is after the period of this study. Personality disorder is likely to have been underreported on account of the difficulty of making an accurate diagnosis because of cultural differences and in the presence of widespread social upheaval.
The presence of other potential confounders as risk factors, including social disadvantage, age and smoking, has not been included in our analysis.
Conclusion
Our data powerfully expose the perinatal and early environment of Indigenous children who later developed a psychotic disorder. We have identified higher rates of risk factors for psychosis in those born after 1980, a period marking enormous social change across these populations. As risk factors for schizophrenia may be cumulative and interactive, both with each other, and with critical periods of neurodevelopmental vulnerability (Davis et al., 2016), our results suggest possible causes for the increasing prevalence of psychotic disorders between 1992 and 2015.
Supplemental Material
sj-pdf-1-anp-10.1177_0004867420984832 – Supplemental material for Multimorbidity and vulnerability among those living with psychosis in Indigenous populations in Cape York and the Torres Strait
Supplemental material, sj-pdf-1-anp-10.1177_0004867420984832 for Multimorbidity and vulnerability among those living with psychosis in Indigenous populations in Cape York and the Torres Strait by Fiona Charlson, Bruce Gynther, Karin Obrecht, Michael Waller and Ernest Hunter in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The clinician authors of this paper (B.G., E.H. and K.O.) are indebted to the Aboriginal and Torres Strait Islander patients and their families who have enriched their understandings of cultural diversity and strengths, and resilience in the face of adversity.
Author Contributions
E.H., K.O. and B.G. undertook data collection. F.C., E.H. and B.G. were responsible for study design. F.C. and M.W. undertook statistical analyses. F.C., B.G., E.H. and K.O. were responsible for interpretation of results. All authors were responsible for writing and editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors report grants from Mental Health Branch, Queensland Health, during the conduct of the study. Queensland Health who are the custodians of this database funded this study. The funder had no role in study design, data analysis, data interpretation, writing of the report or submission for publication. All authors had full access to all the study data. The corresponding author had final responsibility for the decision to submit for publication. F.C. is supported by an Australian National Health and Medical Research Council (NHMRC) Early Career Fellowship (APP1138488).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.