
Abstract
The aim of this study was to compare hip strength in sports-active transtibial (TT) amputees, sedentary TT amputees and sports-active non-amputees. Three ‘active’ (exercising recreationally at least three times per week) TT amputees, four ‘inactive’ or sedentary TT amputees and nine ‘active’ able-bodied persons (AB) underwent concentric and eccentric hip flexion and extension strength testing on both limbs on an isokinetic dynamometer at 60 and 120°/s. Little strength asymmetry was noted between the limbs of the active TT amputees (8% and 14% at 60 and 120°/s, respectively), their residual limb being slightly stronger. Inactive TT amputees demonstrated up to 49% strength asymmetry, their intact limb being the stronger. Active TT amputees demonstrated greater peak hip torques (Nm/kg) for all conditions and speeds compared to inactive TT amputees. Peak hip torques (Nm/kg), were greater in the active TT amputees' residual limb compared to AB. While inactive TT amputees and AB had similar flexion/extension ratios, active TT amputees exhibited a lower ratio indicating overdeveloped hip extensors with respect to their hip flexors. It is not known whether this is due to the demands of sport or exercise with a prosthetic limb, or remaining residual thigh atrophy.
Introduction
It is observed, both in practice and in scientific studies, that thigh muscle atrophy and a reduction in thigh muscle strength is common following transtibial amputation.[1-3] Strength differences between limbs, measured as flexion and extension torques at the knee[1], 1,2,, 4,, [5] or hip isometric strength,[6] have previously been reported of up to 47% in sedentary transtibial (TT) amputees, the residual limb being weaker than the intact limb. These studies are in agreement that the quadriceps tend to be more atrophied and weaker than the hamstrings. Muscle atrophy and a reduction in muscle strength, though, is associated with inactivity and can be reversed with training or exercise.
After rehabilitation, few amputees become involved in sport or take regular exercise. The most common reasons for this are an inability to run or jump, becoming easily fatigued, having decreased speed of movement and decreased endurance,[7] which paradoxically, can all be improved with training. Training studies for TT amputees have been found in the literature aimed at increasing either isokinetic knee strength[2] or residual limb (stump) volume,[8] but none have been found targeting any other lower limb muscles.
It is known that lower limb amputees compensate at the hip (in terms of increased range of movement and torque) during walking, running and jumping.[9-11] Thus greater demands are made on the muscles surrounding the hips for prosthesis users than for able-bodied persons. In addition, authors have suggested that a deficiency in hip muscle strength may contribute to poor walking ability12,, [13] and an inability to run or walk quickly would be expected to be a result of inadequate training of the hip flexors.[6] Thus it appears that for lower limb amputees, the important muscle groups for good walking or running, and thus ability to be sports-active, are the muscles surrounding the hip joint. To date, no published studies have either investigated the amount of hip flexion or extension strength asymmetry or, in a training study, tried to increase hip strength in lower limb amputees in order to investigate whether this improves their walking or running or ability to be sports-active.
To successfully take part in sports or exercise, one needs to be in fairly good condition and be sufficiently strong in the appropriate muscles. This is achieved in itself via progressive training of the cardiovascular system and muscles. Unilateral TT amputees at elite level have run 100 m in 10.91 s, jumped 6.79 m in the long jump and cleared 2.11 m in the high jump (current World Records) which is beyond the performance of many non-amputees. As success in these events require strong lower limb muscles, it is clear these athletes cannot have the same degree of residual limb muscle atrophy or loss of muscle strength as has been reported in sedentary TT amputees. Thus it can be inferred that lower limb amputees are able to train their muscles to a degree that will allow them to compete in sport at the highest level. However, whereas few amputees have the ability or inclination to train to elite level, a greater number would like to be able to return to participating in sport or exercise on a recreational level. Understanding strength requirements for lower limb amputees to participate in sport at this level would be of interest for practitioners and coaches working in this field. As nothing has yet been reported about strength requirements or strength magnitudes in sports-active lower limb amputees at any level, it is necessary to first determine how strong recreational exercisers are compared to those who do not exercise. The aim of this study is to compare hip strength in sports-active TT amputees, sedentary TT amputees and sports-active non-amputees.
Method
Subjects
Subjects' characteristics. Individual characteristics are given for all TT amputees, while group means ± SD are given for the able-bodied (AB) persons.
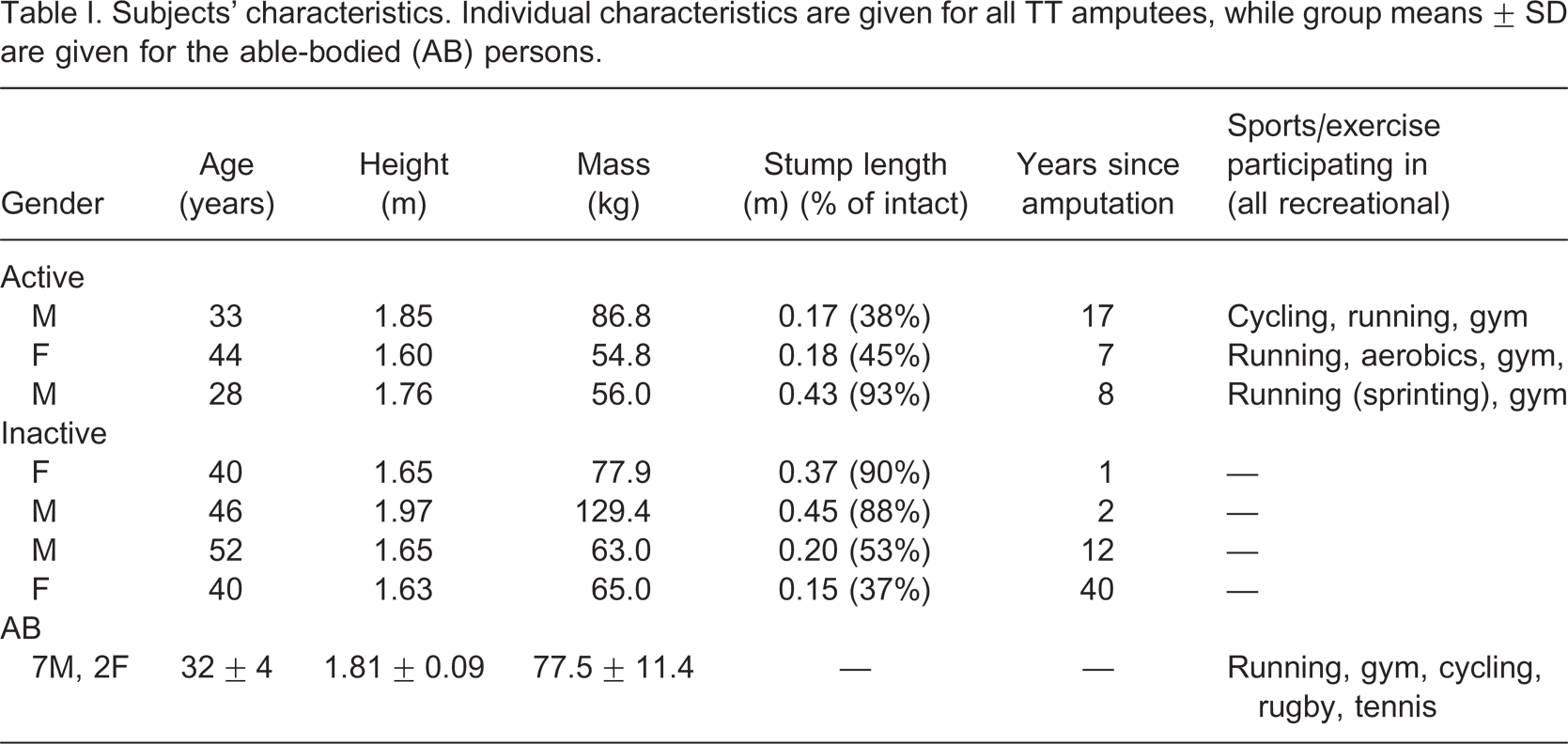
Able-bodied participants were recruited from a Physical Education College in Sweden. The amputee participants were initially contacted by a physiotherapist or prosthetist with general information about the study and those interested in participating were requested to contact the author for more information and the possibility of volunteering. Due to ethical requirements, the author was not allowed to make initial contact with potential amputee participants. Ethical approval was given by the institutional ethics committee and written informed consent was obtained from all participants.
Apparatus
An isokinetic dynamometer,[14] controlled by a PC, was used to measure hip flexor and extensor strength during concentric and eccentric actions with the subjects lying prone. A custom made cuff to be placed around the most distal part of the thigh was constructed. Pilot work determined the best type of cuff to minimize errors in strength measurement due to pain or discomfort. The hip range of motion, selected to include hip range of motion during running at all speeds up to sprinting, was from 10° hip extension to 70° hip flexion. The dynamometer was set with a 5° ramp, i.e., it took 5° to reach the selected speed, and 5° to slow down. Thus the range 5° hip extension to 65° hip flexion was guaranteed to be at the selected speeds. The isokinetic dynamometer was calibrated prior to each testing session.
Procedure
The subject lay in a prone position and the dynamometer was adjusted so that the hip joint centre corresponded with the position of the axis of rotation of the lever arm. The cuff was placed around the thigh of the limb being measured, as distally as possible, adjusting the lever arm length for each subject. The free limb and lower back were strapped down to try to isolate hip flexion and extension movement (see Figure 1 for an example of the set-up). Hip strength in both limbs was measured, intact limb first, with measurements on the residual limb being made without a prosthesis.
An example of the isokinetic dynamometer set-up for testing hip strength in the right limb of an able-bodied subject. For testing hip strength in the left limb, the subject lies on the right bench and the free leg support and cuff with lever arm are transferred to the right side. The set-up is identical for the TT amputees with the exception of when the amputated leg is the free leg, a pillow is provided for use between the residual stump and the leg support.
Each subject underwent a warm-up. This consisted of flexing and extending the hip throughout the measuring range of motion. Each trial required progressively more effort until the subject was ready to perform a maximal movement. The subjects then completely relaxed and an initial flexion/extension trial was collected to determine the torque due to gravity and the mass of the leg.
Maximal concentric and eccentric flexor and extensor strength measurements at 60°/s and 120°/s were performed in random order with verbal encouragement. Two trials, each trial consisting of one flexion and one extension movement, for each condition were performed so as not to fatigue the subjects, particularly the inactive amputees. A short rest period of at least 60 s was allowed between each trial. For the eccentric strength actions, the subjects were allowed several practice trials at both speeds to familiarize themselves with the movement. Output angle (degrees) and torque data (Nm) for each trial was collected on a second computer, sampled at 100 Hz, using a Powerlab® data acquisition system (AD Instruments Ltd, Oxfordshire, UK).
Data analysis
Five degrees were removed from the start and the end of the range of motion prior to further processing (resulting in −5 to 65°) to ensure the correct speed was present throughout the whole range of motion. Of the two trials for each condition, the trial showing the largest peak torque was chosen for further analysis. The gravity torque was then taken from, or added to, the flexion and extension trials, respectively, to take into account the effect of gravity and the mass of the leg when lying in the prone position.
Peak torque, during the analyzed range of motion (−5 to 65°) was calculated for concentric hip flexion, concentric hip extension, eccentric hip flexion and eccentric hip extension at both speeds. All values were normalized to body mass for each individual. An asymmetry index was used to indicate peak torque differences between the residual and intact limbs of the TT amputees where amount of asymmetry (ASI):[15]

In order to determine the relative strength of the hip flexors to the hip extensors, a flexion extension ratio (peak flexion torque/peak extension torque) was calculated for each contraction type (concentric or eccentric) and for each speed.
Statistical analysis
For the able-bodied persons, a paired t-test, with level of significance set to p < 0.05, was performed to determine any differences between left/right limb peak torques for all speeds and conditions. None were found and so an average of the left and right limbs were calculated for all able-bodied individuals to avoid reporting either dominant or non-dominant limb values as the basis of a comparison value for the TT amputees. Due to having so few TT amputees in each group, n = 3 and n = 4, only descriptive statistics, such as group means, standard errors and percentage asymmetry, calculated using the mentioned asymmetry index, could be presented.
Results
Muscle contractions at 60°/s
Asymmetry
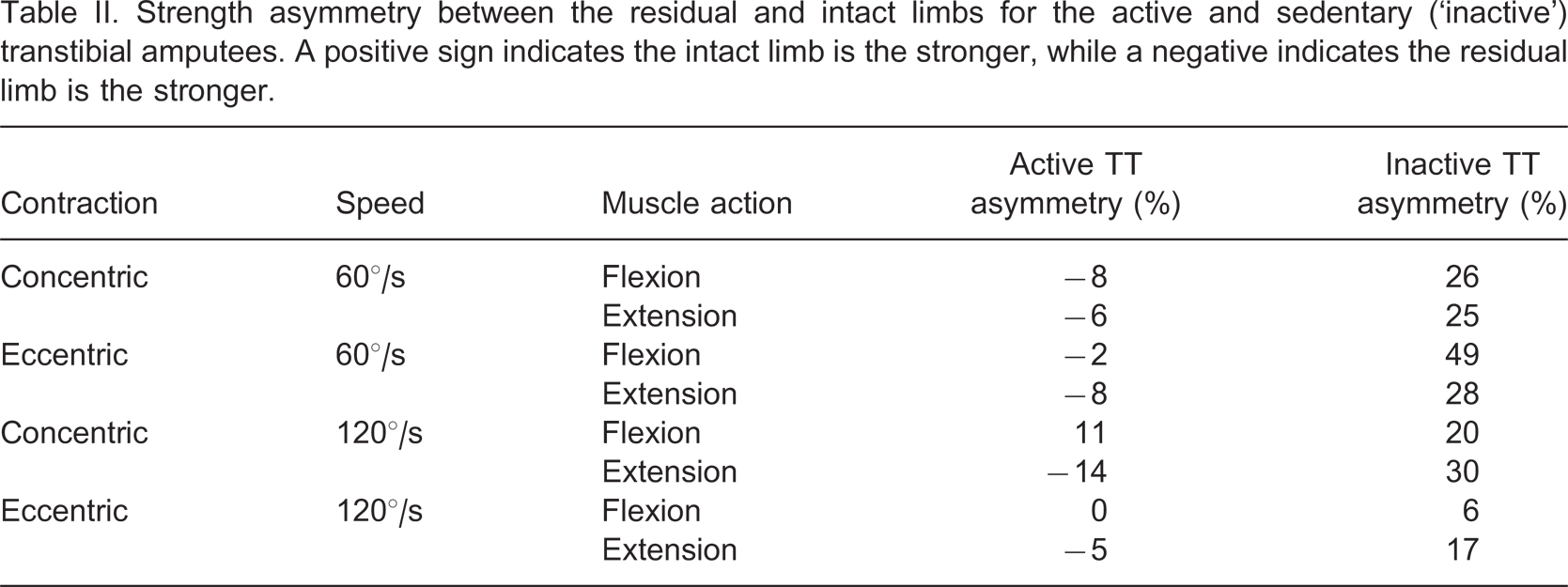
Strength asymmetry between the residual and intact limbs for the active and sedentary (‘inactive’) transtibial amputees. A positive sign indicates the intact limb is the stronger, while a negative indicates the residual limb is the stronger.
Concentric flexion and extension peak torques
Figure 2 shows peak concentric hip flexion and extension torque at the slower speed of 60°/s. Both active and inactive TT amputees had smaller hip flexion peak torques than the AB group, with the active amputees being stronger than the inactive (13% stronger intact limb, 59% stronger residual limb). What is particularly interesting is the active amputees had greater hip extensor peak torques than the able-bodied persons (12% greater on the residual limb, 6% greater on the intact limb). Peak hip extension torque differences were seen between the active and inactive persons, the active TT amputees having 53% stronger intact limb and 109% stronger residual limb than the inactive.
(A) Concentric hip flexion and (B) extension strength, normalized to body mass, at 60°/s. Mean (+ SE) values shown for active (black) and inactive (grey) TT amputees. Solid block indicates intact limb, striped block residual limb. The corresponding able-bodied value (average of both limbs) is indicated by the white block.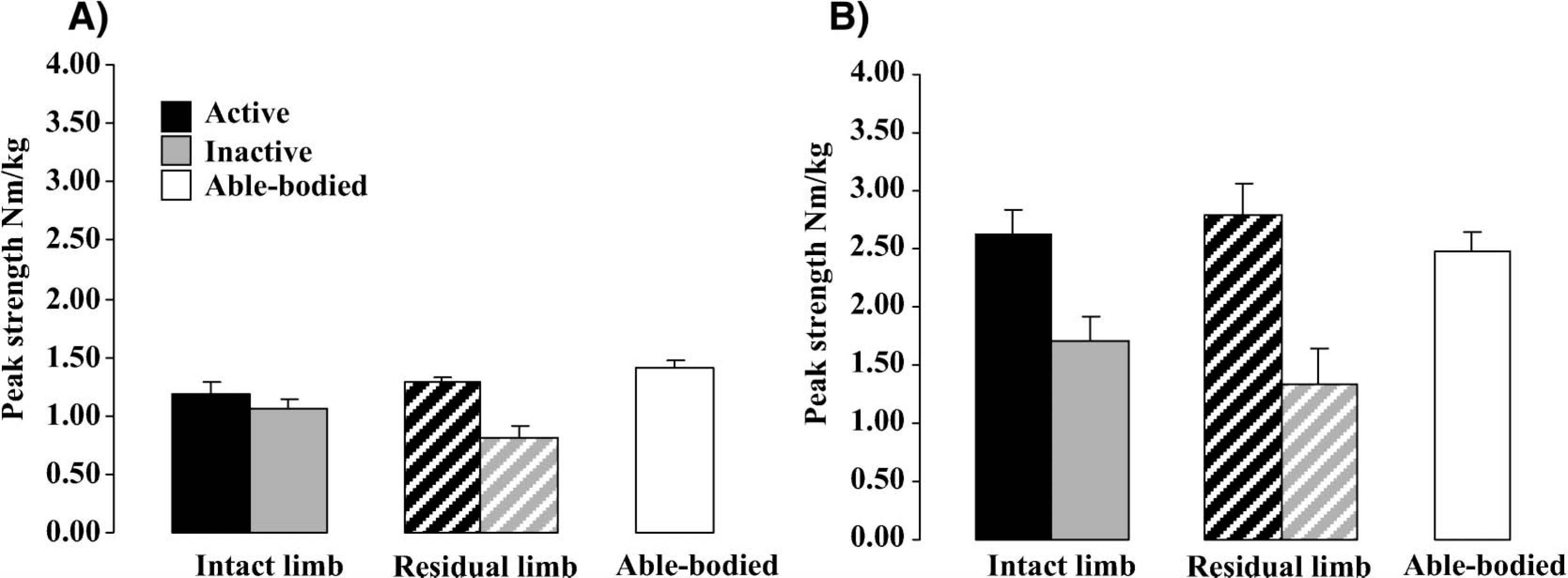
Eccentric flexion and extension peak torques
Eccentrically, the active amputees were again stronger than the inactive amputees (Figure 3). The active individuals exhibited similar magnitude hip flexion peak torques in both their residual and intact limbs, while the inactive individuals had a much smaller residual hip flexion peak torque compared to their intact limb. Comparing the TT amputee groups, the active persons produced a 91% greater eccentric hip flexion peak torque in their residual limb than the inactive persons.
(A) Eccentric hip flexion and (B) extension strength, normalized to body mass, at 60°/s. Mean (+ SE) values shown for active (black) and inactive (grey) TT amputees. Solid block indicates intact limb, striped block residual limb. The corresponding able-bodied value (average of both limbs) is indicated by the white block.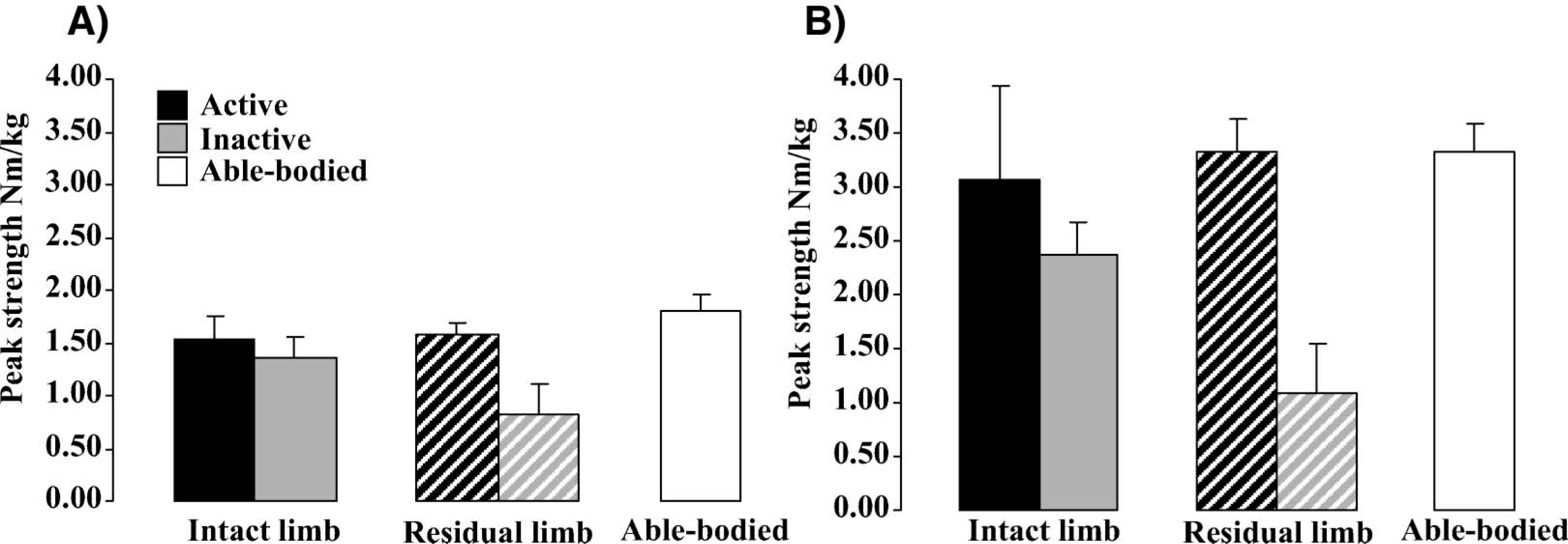
While all amputees exhibited weaker smaller hip flexion peak torques than AB persons, the active individuals had a similar magnitude hip extension peak torque in their residual limb compared to the AB group. Again for the active persons, their residual limb hip muscles were stronger than their intact limb hip muscles, and this is where the difference between the active and inactive individuals was seen clearest (active amputees had a 187% greater residual limb eccentric hip extension peak torque than inactive).
Muscle contractions at 120°/s
Asymmetry
Looking at Table II, a little more asymmetry was seen between the limbs of the active amputees for concentric contractions at this speed than for the slower speed. Maximum asymmetry at 120°/s, regardless of muscle action (flexion or extension) or contraction (concentric or eccentric) was −14%, indicating a greater peak torque was produced by the residual limb than the intact limb for all muscle actions and contractions except concentric flexion. For the inactive amputees, up to 30% asymmetry was seen between the limbs, where in all cases a greater peak torque was produced by their intact limb compared to their residual limb.
Concentric flexion and extension peak torques
At the faster speed of 120°/s, both active and inactive TT amputees had smaller concentric hip flexion peak torques than the AB group (Figure 4). Comparing the TT amputee groups, the active individuals were stronger, producing a 25% greater peak torque on their intact limb and a 36% greater torque on their residual limb compared to the inactive individuals. For concentric hip extension peak torques at this speed, active amputees had a similar magnitude intact limb peak torque, but greater residual limb peak torque (16%) compared to the able-bodied group. Again, hip extensor torque in the residual limb was where the largest difference was seen between the active and inactive amputees, the active persons having a 124% greater hip extension peak torque than the inactive.
(A) Concentric hip flexion and (B) extension strength, normalized to body mass, at 120°/s. Mean (+ SE) values shown for active (black) and inactive (grey) TT amputees. Solid block indicates intact limb, striped block residual limb. The corresponding able-bodied value (average of both limbs) is indicated by the white block.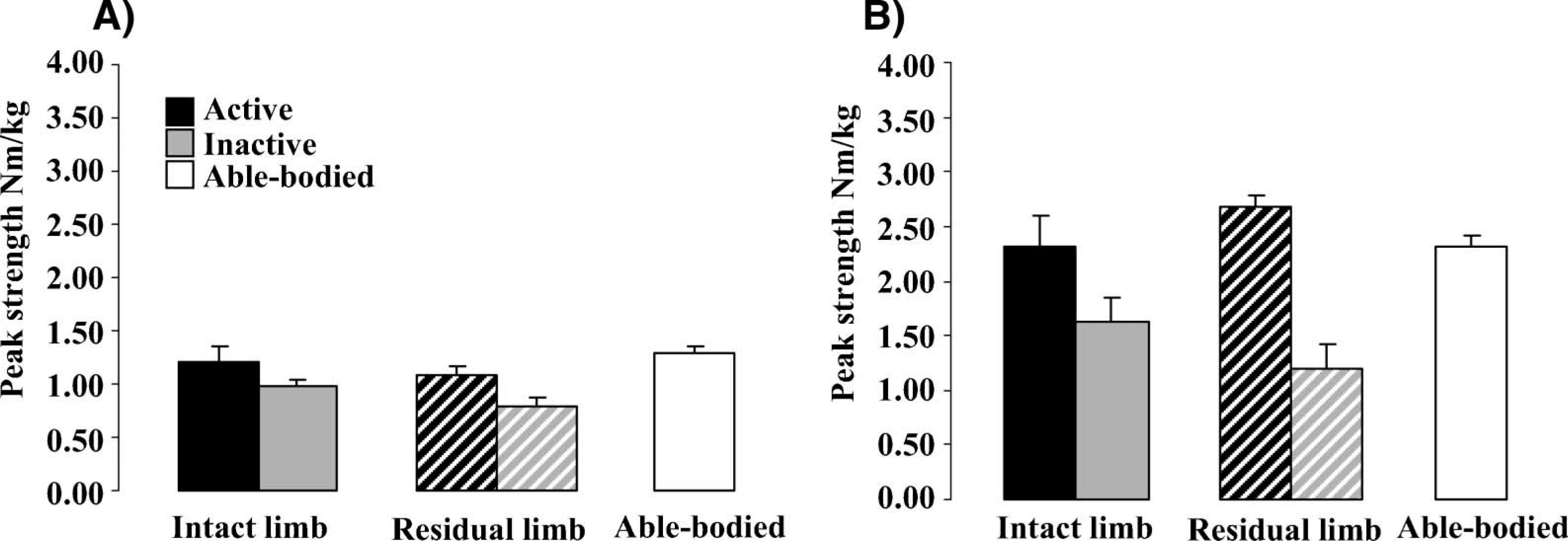
Eccentric flexion and extension peak torques
The active amputees were again stronger than the inactive amputees (Figure 5). The able-bodied persons exhibited a greater peak hip flexion torque than the amputees. However, for hip extension, the active amputees produced a greater peak torque than the able-bodied persons in both their intact limb (20%) and residual limb (26%). In addition, eccentric hip extension at the fast speed of 120°/s is where the largest difference in peak torque was seen between the active and inactive amputees. In the intact limb, the active persons produced an 80% greater peak torque and in the residual limb they produced a 123% greater peak torque than those amputees who did not exercise.
(A) Eccentric hip flexion and (B) extension strength, normalized to body mass, at 120°/s. Mean (+SE) values shown for active (black) and inactive (grey) TT amputees. Solid block indicates intact limb, striped block residual limb. The corresponding able-bodied value (average of both limbs) is indicated by the white block.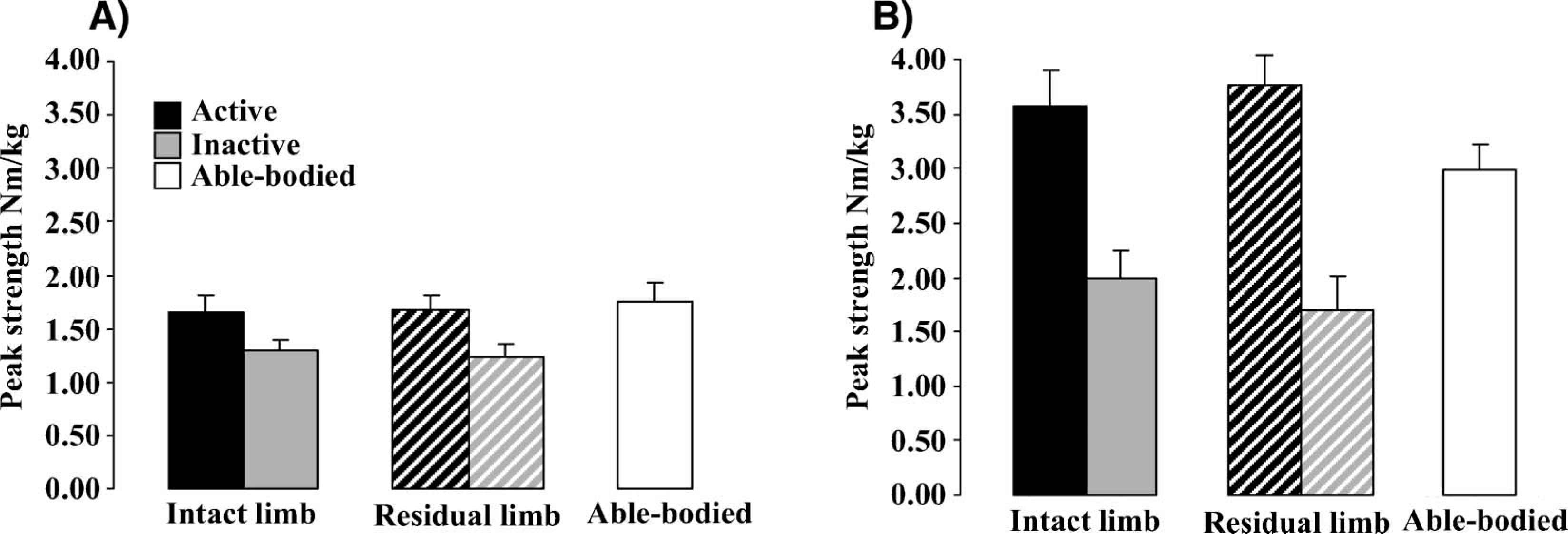
Flexion/extension ratio
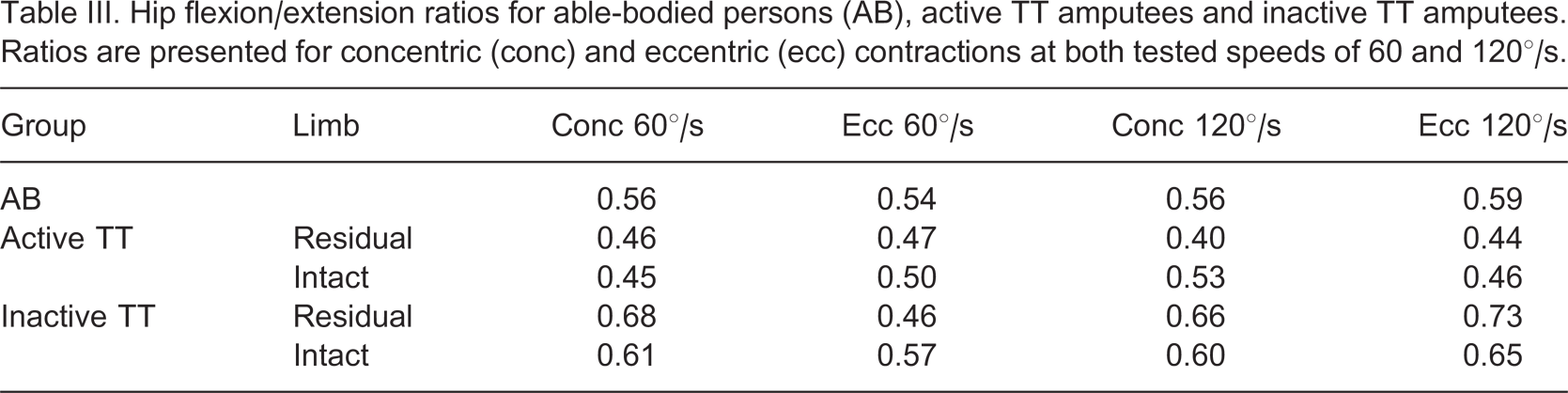
Hip flexion/extension ratios for able-bodied persons (AB), active TT amputees and inactive TT amputees. Ratios are presented for concentric (conc) and eccentric (ecc) contractions at both tested speeds of 60 and 120°/s.
Discussion
On comparing the three groups descriptively, it is clear from the results that active TT amputees have stronger hip muscles than inactive amputees, as is to be expected. The inactive amputees tested were on average a little older than the sports-active group (mean ± SD age 44.5 ± 5.7 and 35.0 ± 8.2 years, respectively), which could have accounted for some strength difference, but the differences between these two groups are so large that it cannot be only due to age.
More interestingly, the active TT amputees have as strong or stronger (depending on limb, contraction type or speed) hip extensor muscles than active able-bodied persons. In particular, residual limb concentric hip extensor torque at both speeds and both the residual and intact limb eccentric hip extensor torque at the faster speed, were 12–26% stronger than the able-bodied group. To the author's knowledge there are no published studies on isokinetic hip torque in sports-active unilateral TT amputees, and so there are no values to compare these findings to. The able-bodied persons and active TT amputees recruited for the present study all claimed to regularly exercise at least three times per week at the time of testing, but no measurements were performed to assess their general level of fitness, nor to question their training intensity. Thus it could be, although it is not known, that the active TT amputees exercised more than the AB persons and that could account for their stronger hip muscles. Thus in future studies of this nature it is recommended that training intensity as well as training duration and frequency are recorded. On the other hand, the problems associated with performing sports with a prosthetic foot may force active TT amputees to become so much stronger in their residual limb hip compared to both their intact limb hip and to the hips of AB persons as many studies have reported that TT amputees compensate at the hip during walking, running and jumping.[9-11] Whatever the reason, this study illustrates descriptively that TT amputees, despite residual limb atrophy following amputation, can strengthen their hip muscles to a level that surpasses age-matched sports-active AB persons. Thus in terms of limb strength, there should be no barriers to sports participation for healthy TT amputees. Further study is needed to determine if these amounts of hip strength are the necessary minimum for lower limb amputees to participate in sport or exercise at recreational level. This information would provide a basis for the development of effective and efficient training programmes for currently sedentary amputees.
On looking at the descriptive results of inter-limb symmetry within each group, for each contraction type, speed and muscle action, the inactive TT amputees displayed the most asymmetry. The large asymmetry values were seen as much larger hip peak torques on their intact limb than their residual limb. Similar findings for sedentary TT amputees have been reported previously for thigh strength (knee torque) measured at the same speed as the present study2,, 4,, 5,, [16] although no comparable studies have been found reporting hip strength torques. In the present study, the differences between the limbs of the inactive TT amputees were seen as large amounts of asymmetry, regardless of muscle action, contraction or speed, of up to 49%, which is comparable with previous studies reporting, either by measuring isokinetic knee strength or isometric hip strength, inter-limb asymmetry of up to 47%.1,, 2,, [4-6] As residual limb atrophy is less pronounced in the hamstrings than quadriceps,[3] hip flexion asymmetry should be greater than hip extension asymmetry. This was true for the present study's inactive persons for both eccentric and concentric contractions at the slower speed, but not at the faster speed where the opposite was true. This could have been due to the speed of motor unit recruitment in untrained persons. Muscle fibre type has been found to differ in the residual limb thigh of inactive TT amputees compared to their intact limb thigh.2,, [3] A greater percentage of Type II fast twitch fibres and reduced percentage of Type I slow twitch fibres compared to the intact limb were found in the vastus lateralis, which interestingly was redressed with training.[2]
While these results are only descriptive due to the small group numbers involved, these findings suggest that active TT amputees exhibit the opposite of the inactive TT amputees in terms of inter-limb asymmetry. In all measurements except concentric flexion at 120°/s, their residual limb hip muscles were stronger than their intact limb hip muscles. Indeed inter-limb asymmetry at the slower contraction speed was 8% or less regardless of contraction type or muscle action, and there was no pattern of the hip flexors being more asymmetrical than hip extensors or vice versa. Thus, the results for the active TT amputees show, and these are not elite athletes but individuals who exercise on a recreational level, it is not only possible to redress muscle atrophy and reduced strength in the residual limb, but also to have greater residual limb strength than in both their intact limb, and in the limbs of sports-active AB persons. Further study needs to be done to determine whether the use of sport or exercise is an effective tool to help reduce the levels of muscle and gait asymmetry commonly seen in lower limb amputees.
For all able-bodied persons, and all amputees in this study, regardless of whether active or inactive, hip extensor muscles were stronger than hip flexor muscles both concentrically, eccentrically, and at both contraction speeds. This is in agreement with previous studies.[17-21] On comparing how strong the hip flexors are relative to the hip extensors in an able-bodied population, authors have reported isokinetic (concentric and eccentric) hip flexor/extensor ratios of 0.58–0.75.[20], 20,21 The able-bodied persons in the present study exhibited a concentric flexion/extension ratio of 0.56 and an eccentric ratio of 0.54–0.59 indicating this group is at the lower end of the reported AB range. Bäcklund et al.[6] reported isometric hip extension strength was greater than isometric hip flexion strength in sedentary TT amputees, and proposed that this was due to the fact that hip flexors are less exercised than hip extensors. Hip extensor muscles function as antigravity muscles and thus are naturally exercised more than hip flexor muscles. In the present study, the hip flexion/extension ratio for the active TT amputees was 0.40–0.47 for their residual limb and 0.45–0.53 for their intact limb. While these results are only descriptive due to the small group numbers involved, these findings suggest much weaker hip flexors with respect to extensors in both limbs, particularly in the residual limb, compared to the able-bodied population. For the inactive TT amputees, the ratios were higher; 0.46–0.73 for their residual limb and 0.57–0.65 for their intact limb indicating similarities with the able-bodied population. Thus while the active TT amputees in this study were stronger than the inactive amputees, their hip extensor muscles were excessively strong compared to their hip flexors. It may be that either their chosen sports demand high levels of hip extension strength, or that hip flexor strength cannot be increased much more than this, particularly in the residual limb as atrophy of the hamstring muscles is less pronounced than for the quadriceps muscles.[3] Perhaps due to this, active amputees need to ‘overdevelop’ their hip extensors in compensation, resulting in the need to be stronger than able-bodied persons in order to perform similar sport or exercise movements. Further study is needed to determine the effect of hip flexor strength training in a similarly active TT amputee population.
A limitation of the study was, as with all isokinetic or maximum strength testing studies, knowing whether or not the subjects were performing maximum effort on the strength tests. Fear, particularly for the inactive group on the residual limb tests could have been a factor, and reproducibility was not tested in order to avoid fatigue. However as much as possible was done to reduce this particular limitation such as acclimatising and warming up using the same movements as in the test, and also testing the intact limb first. In addition, the cuff of the isokinetic dynamomenter was placed on the distal end of the thigh and thus nothing was touching the stump, avoiding excess pressure or discomfort.
The low numbers of sports-active amputee subjects available was the limiting factor of group size. Due to ethical requirements, the author was not allowed to approach any potential amputee participants and thus cooperation from prosthetists and physiotherapists treating these amputees was required. Due to this fact, it is not known how many amputees were informed about the study and how many of these were interested enough to take it further. The strict inclusion criteria, not least that all should be trauma or congenital amputees, limited further the group numbers as two sports-active amputees had to be rejected because they were competitive athletes. It was thought that including competitive athletes could skew the results somewhat as it is expected they will be stronger than those exercising recreationally. Due to these constraints, it was not possible to include more subjects within the time period for the study. With these small group sizes all results are presented on a descriptive level and the findings cannot be generalised to all TT amputees. However, the standard error for measured variables in this group was small so it may be that other young, healthy, sports-active TT amputees with amputations resulting from trauma could show similar findings to the present study.
Conclusion
Little hip strength asymmetry was seen in the limbs of the three active TT amputees, where their residual limb was slightly stronger than their intact. The opposite was found for the four inactive TT amputees who displayed up to 49% inter-limb asymmetry, where their residual limb was weaker than their intact.
The sports-active amputees had more than double the size hip extensor peak torques on their residual limb compared to inactive TT amputees, and were also up to 26% greater than similarly sports-active AB persons. However, their flexion/extension ratio was much smaller than both the other groups indicating their hip extensors were overdeveloped compared to their hip flexors. It is not known if this is due to the demands or sport or exercise with a prosthetic limb resulting in the need to be stronger than able-bodied persons in order to perform similar sport or exercise movements, or remaining amounts of thigh muscle atrophy. However, these are preliminary findings due to the low subject numbers in the study. Further research needs to be undertaken in this area.
Footnotes
Acknowledgements
The author gratefully acknowledges the help of Socrates Deligeorges, and financial support from CIF (Centre for Sport Research, Stockholm) and Allmänna Arvsfonden (Stockholm, Sweden).