
Abstract
This paper describes a new fabrication process for making low-cost transradial sockets using recyclable plastic soda bottles. Easy, fast, and inexpensive to fabricate, the resulting socket can be used as a temporary device for stump care. Multiple sockets can be made and individually incorporated with various terminal devices for light-duty self-care or functional activities, such as feeding, showering, typing, swimming, or gardening. The formed socket is lightweight and also suitable for use with a cosmetic passive hand prosthesis. This process has been developed as a potential cost-effective assistive technology appropriate for individuals with transradial amputation in resource-limited countries.
Keywords
Introduction
As a routine, upper limb prosthetic sockets are made of either thermoplastics or thermosetting resins. The traditional plaster-based procedure is a multi-step process; including casting of the amputation stump and modification of the positive model in order to vacuum form a prosthetic socket. The socket of a transradial prosthesis is usually joined with interchangeable terminal devices. Various terminal devices can be made and used with the same socket for different functional activities.
In countries with limited resources, Western technologies for upper limb prostheses are still being applied. However, many people with upper limb amputations are not being fitted with prostheses due to a lack of trained technicians able to provide the service, and a shortage of proper components or materials available for production of upper limb prostheses.1 One example of an attempt to improve the situation is the ‘socket-less’ forearm prosthesis, which was developed and used in 2000 for transradial amputees in Sierra Leone.2,3 Another type of technology, the CIR Casting System4 developed at the Center for International Rehabilitation (CIR) in Chicago, can also be used for individuals with transradial amputation. Seeking an alternative material for socket fabrication, it was found that recyclable plastic soda bottles can be reused to form transradial sockets.
The plastic soda bottle was invented and patented in 1973 by Nathaniel Wyeth,5 a mechanical engineer of DuPont Company This commonly used beverage container is made from polyethylene terephthalate (PET), which can withstand the pressure of carbonated liquids. The bottles are lightweight, translucent, virtually unbreakable, and have superior elastic properties. As they are formed by expansion in a negative mold,6 the plastic of the bottle retains a memory that will shrink when heat is re-applied. The degree of shrinkage is proportional to the intensity and duration of heat applied. In other words, it is possible to use a heat gun to shrink the soda bottle to produce non-uniform thickness and stiffness. By doing so, one can build rigid walls for structural support and flexible walls for a comfortable fit within the socket. The formed socket can be fabricated easily, quickly, and in a cost-efficient manner, and can be incorporated with different terminal devices for specific activities. Because it is flexible and lightweight, the formed socket is also suitable for use with a cosmetic passive hand prosthesis (Figure 1).
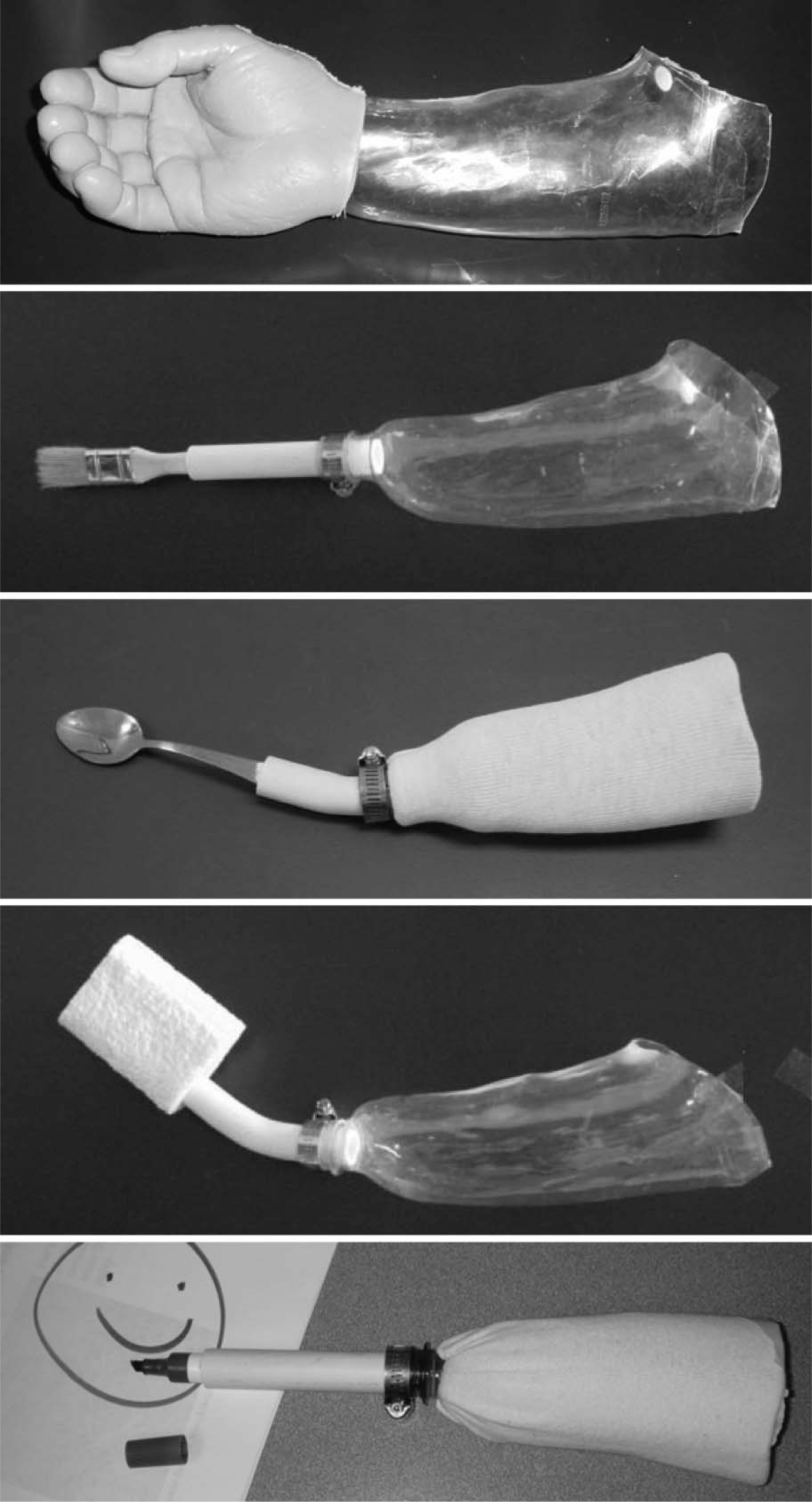
Low-cost sockets can be incorporated with various terminal devices for different functional activities.
Fabrication of low-cost transradial socket
For the purpose of describing the procedure, a modified plaster replica of the amputation stump is used (Figure 2). To provide structural support and a comfortable fit, the formed socket is made to have adequate thickness and strength. This is accomplished by varying the thickness of the plastic in different areas of the socket. The process for fabrication of a transradial socket includes five steps:6

Plaster model of an amputation stump for forming multiple transradial sockets using plastic soda bottles. The dotted area is where plastic can be made thicker for structural support in the socket.
Obtain a positive plaster model of the amputation stump using traditional plaster-based casting methods or the CIR Casting System. Provide necessary modification and pressure relief as is routinely done. Once the plaster is modified, identify the areas where structural support in the socket should be increased. Generally, this is from the proximal-posterior to distal-anterior aspect, as shown in Figure 2.
Prepare the plastic soda bottle socket
Once the plaster model is modified, cover it with a bottomless plastic soda bottle (Figure 3, top). Then, use a heat gun (Figure 3, center) to apply heat to the plastic bottle, making sure there is sufficient thickness in the dotted areas (Figure 2) to provide adequate support in the socket. When the plastic bottle has conformed to the shape of the plaster model, cut along the trim line as is traditionally done to form the socket (Figure 3, bottom). When necessary, a silicone end pad can be inserted inside the formed socket for added comfort.
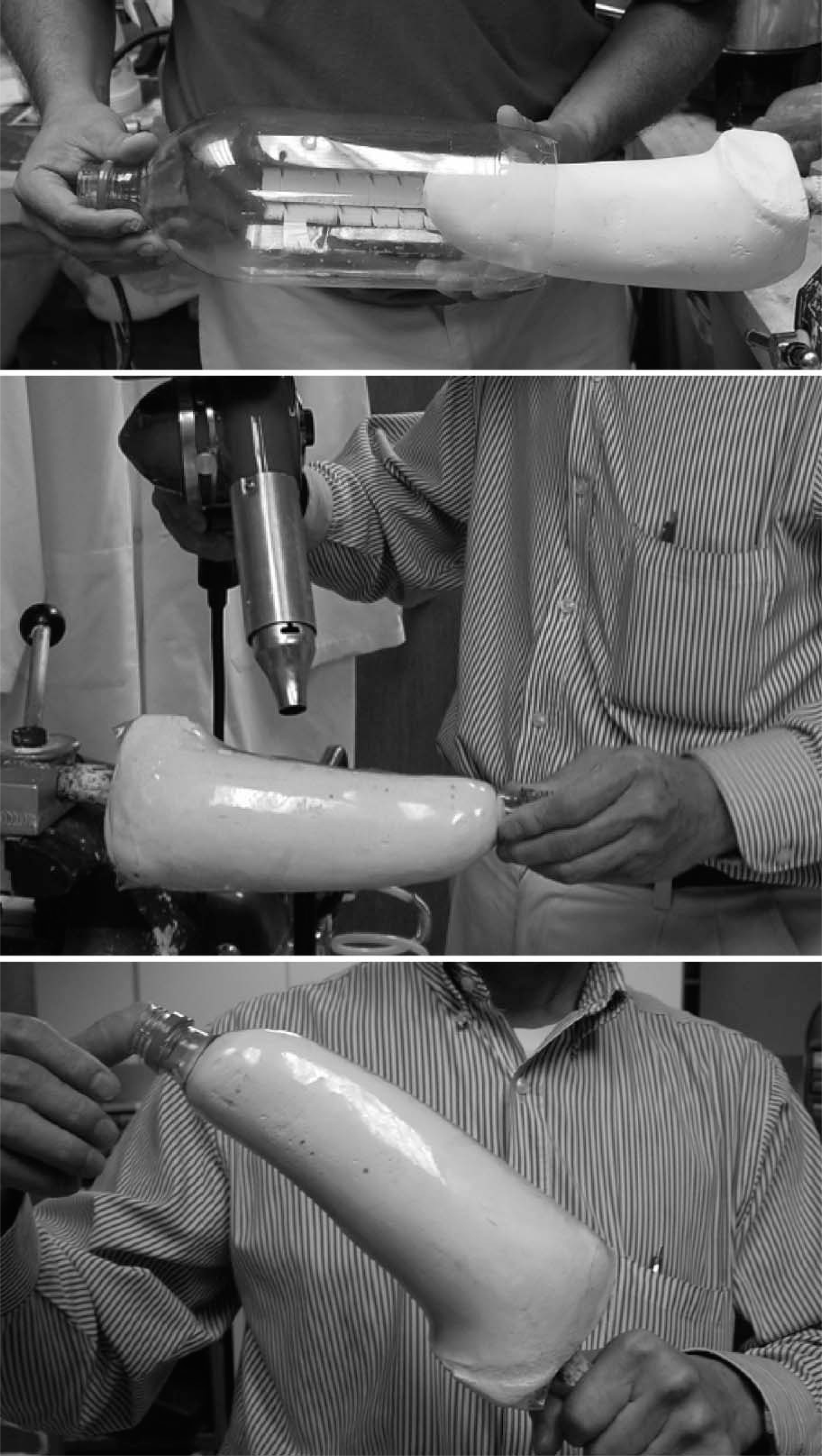
Place the bottomless plastic soda bottle over the plaster positive model (top) and use the heat gun to shrink the plastic (center) to form the socket (bottom).
To affix a terminal device, cut longitudinally across the thread portion at the top of the soda bottle (Figure 4, left). Use a hose clamp to tighten the connection after a ½ inch PVC pipe (21 mm outside diameter) is inserted (Figure 4, right). The PVC pipe can also be shortened and heated to allow it to be bent into proper position if needed. The terminal device is then attached to the end of the PVC pipe.

The bottle opening is cut across (left) for insertion of a ½ inch PVC (21 mm outside diameter) pipe. Use a hose clamp to tighten the connection (right).
Terminal devices, such as a spoon, fork, or paintbrush can be sanded and snugly fit into the PVC pipe. The gap between the terminal device and PVC pipe is then filled with plaster or cement for added stability. One can also glue a sponge over the PVC pipe for use while showering.
Suspension of light-duty transradial prosthesis
As it is very lightweight, the fabricated prosthesis may be suspended using either an elastic stockinet or inner tubing for tires, which is available in many countries where other materials may not be. If not allergic to latex, one can also use a large balloon with both of the ends removed, or a surgical glove with the digits removed to seal the opening between the socket trim line and the skin. In addition, use silicone to seal the distal end of the socket in order to create a suction suspension for the prosthesis. If necessary, a cuff at the level above the elbow made from a portion of another plastic soda bottle could also be attempted as a means for suspending the socket.
Discussion
Based on laboratory testing, the ability to reheat the plastic soda bottle to form flexible sockets easily and rapidly is clearly a technical potential and merit further exploration for clinical application.
Since plastic bottles are available in a range of sizes, one would expect that this method would present a viable alternative light-duty prosthetic device for self-care activities. They are suitable for both adults and children with transradial residual limbs that are shorter than the bottomless plastic soda bottle. In addition, it is possible for small children with transtibial amputations to use this device as a removable rigid dressing for stump management.
A simple test revealed that the socket with an over-hanging trim line above the olecranon is easily held on the rigid plaster model without additional suspension, even with an axial loading using two water-filled plastic soda bottles, which weigh approximately 4 kg, (Figure 5, left). This may not be true on the subject depending on the efficacy of suspension of the socket.

While on the plaster model without additional suspension, the prosthetic device tolerated axial loading of two water-filled plastic soda bottles, which weigh approximately 4 kg (left). Upon lifting, the prosthetic device tolerated same water-filled plastic soda bottles at a point 14 cm from the end of plaster model without creating any stress mark (right).
Upon lifting the load, two water-filled plastic soda bottles (about 4 kg) at a point 14 cm from the end of plaster model did not create any stress mark (Figure 5, right). When more were added to a total of five water-filled soda bottles (about 10 kg), there was a down shifting at end of the PVC pipe by 1.7 cm. Upon further up and down movement of these water-filled bottles, it caused the socket to buckle at its distal end. The exact amount of lifting tolerance by this type of prosthesis and by the residual limb can only be determined through future clinical study. However, for the aimed light-duty activities, such as feeding, showering, writing, etc. this prosthetic device is expected to tolerate the needed lifting loading well.
The concern of cosmesis was not addressed by the current design, but a procedure to incorporate low-cost acceptable cosmetic cover could be examined in the future. This technique of constructing a low-cost transradial socket offers an alternative or an addition to the traditional approach for transradial stump care or light-duty self-care training during the early phase of rehabilitation. Even in the developed world, where more technically advanced systems are available, this device would likely be the preferred device for simple light-duty functional activities, such as showering, in order to preserve expensive definitive prostheses for formal function. Being abundant and reusable, plastic soda bottles have the potential to be used to make prosthetic sockets, which can be applied as a protective stump dressing or training devices during early phase of rehabilitation, or as alternative devices for some light-duty self-care or functional activities even if a definitive prosthesis has been provided.
Conclusion
The procedure described utilizes a commonly available 2-litre plastic soda bottle to form a transradial prosthetic socket. As many areas of the developing world lack the resources required for prosthetic fabrication, reuse of the recyclable, durable, and abundant plastic soda bottles provides an alternative solution for making light-duty prosthetic devices to meet the functional need of many transradial amputees. The formed sockets can be assembled with various terminal devices for use as training devices or permanent tools for different light-duty self-care or functional activities. We believe that creative clinicians can use the unique features of the plastic soda bottle to develop other applications and variations of this technique to improve patients' function.
Footnotes
Acknowledgements
The contents of this presentation/publication were developed under a grant from the U.S. Department of Education, National Institute on Disability and Rehabilitation Research grant number H133E080009. However, those contents do not necessarily represent the policy of the Department of Education, and you should not assume endorsement by the Federal Government. The authors would like to thank Kate Jackson for her assistance with editing and posting the video presentation and valuable input during the preparation of this manuscript.