
Abstract
Background:
Individuals with proximal femoral focal deficiency (PFFD) present with a shortened femur. This report highlights the process used to determine prosthetic candidacy, a novel use of the International Committee of the Red Cross (ICRC) prosthetic materials, and subsequent rehabilitation when treating in rural Haiti.
Case Description and Methods:
An eight-year-old boy with PFFD whose goal was to walk ‘normally’ presented with a shortened right leg and typical foot/ankle. Concerns regarding ability to safely load the leg were mitigated after finding he could fully load his right limb, control motion, and had no fractures.
Findings and Outcomes:
A unique prosthosis incorporating a donated hinged ankle-foot orthosis, ICRC materials and a SACH foot was fabricated. Physical therapy followed for two weeks, progressing from static weight-bearing and gait training to dynamic balance activities. At discharge, the patient walked independently using the prosthosis and one forearm crutch.
Conclusion:
Through collaboration and innovation rehabilitation goals can be realized even when presented with limited resources.
Clinical relevance
Through collaboration and innovation novel prosthetic designs incorporating materials from the International Committee of the Red Cross can be created and rehabilitation goals can be realized even when presented with limited resources.
Background
Proximal femoral focal deficiency (PFFD) is a rare (~1 per 50,000 births) 1 congenital disorder, with an unknown etiology,2-3 resulting in shortening or complete absence of the proximal femur, malformation of the acetabulum, and a leg length discrepancy.2, 4 The typical presentation of PFFD is a short bulky thigh where the hip is held flexed, abducted and externally rotated. In PFFD, it is common that all the thigh muscles are present but smaller than expected. 5 Despite these osseous and soft tissue variations, the hip is generally painless and, in the presence of sufficient muscle power, stable during weight bearing activities.4-7
Treatment of PFFD is focused on achieving leg length equality and maximizing the patient’s potential for ambulation. 8 While surgery (e.g. limb lengthening, Van Ness rotational osteotomy, amputation) is often recommended, 9 prosthetic or orthotic intervention is also required in most cases. When surgery is not planned, fitting is typically implemented when the child stands or crawls. 4
The Republic of Haiti has a largely underdeveloped and understaffed healthcare system with almost no rehabilitation services. The Medical Teams International (MTI)-Advantage Program provides prosthetic, orthotic and rehabilitation services in the Les Cayes area of rural southern Haiti. Rehabilitation professionals serve as volunteers in various length rotations. The MTI-Advantage Program uses various methodologies, including the recommended guidelines for fabricating prosthetics and orthotics outlined by the International Committee of the Red Cross (ICRC). 10 This technology is durable, easy to learn, compatible in various climates, affordable and sustainable. 10
This case report describes the short-term management of a child living in Haiti with PFFD. We highlight the history, examination, evaluation, clinical decision-making process, novel use of ICRC methodology, and physical therapy follow-up despite limited resources.
Case Description and Methods
A shy boy, approximately eight years old presented with an obvious leg length inequality with his right foot situated just distal to his left knee (Figure 1a). The patient’s mother requested an evaluation to ‘see if anything could be done’ to enable her son to attain his goal of walking ‘normally’. The patient did not report pain in his right leg. He was able to rise to stand and stand to sit independently using his left leg. He ambulated independently with bilateral axillary crutches, non-weight-bearing through his right leg. Additionally, he demonstrated the ability to fully weight-bear through his affected right leg by walking without crutches utilizing left knee flexion to allow his right foot to contact the ground (supplementary online video 1). However, he infrequently ambulates in this manner.
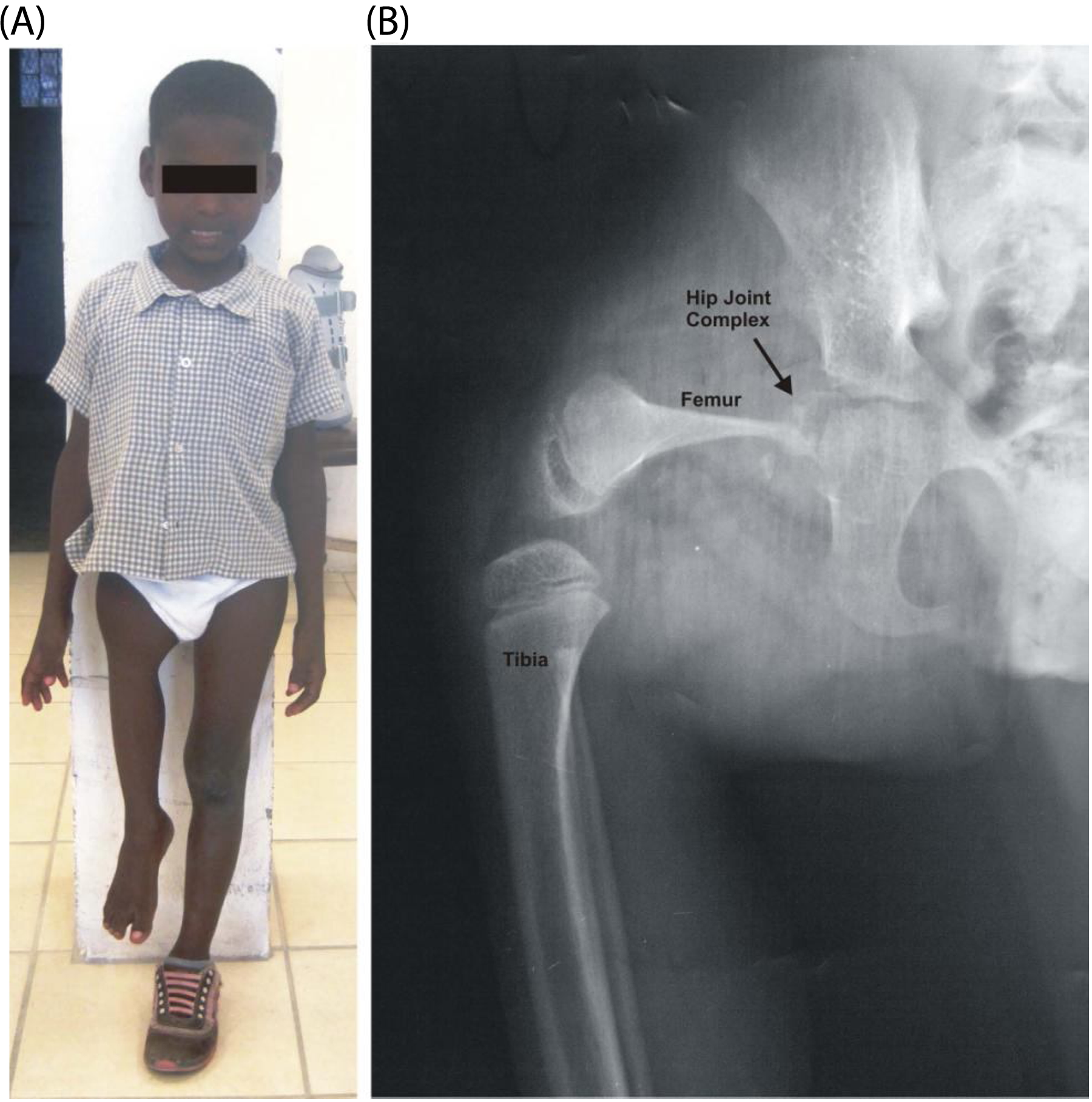
(A) Anterior view of the patient’s right leg affected by PFFD. (B) Anterior-posterior radiograph of the right hip and knee revealing shortened femur with thinned proximal portion.
Prior to intervention we needed to determine if weight-bearing through the femur could be tolerated. While magnetic resonance imaging, ultrasound, or computerized axial tomography scan would have been the preferred method,8, 11-12 this equipment was unavailable. Thus, he was referred for a radiograph assessment. As seen in Figure 1b there is a shortened and thinned right femur, an underdeveloped/absent femoral head, a malformed acetabulum, a tibio-femoral joint that appears to be without a patella, and a typical foot-ankle complex. Although the radiograph depicts femoral abduction this is not due to soft tissue contracture, but simply patient positioning by the technician.
Upon physical examination there were no complaints of pain or discomfort to touch. No sensory deficits were noted on either leg. A leg length assessment was performed with a tape measuring from the umbilicus to the medial malleolus. The right leg was 33% (22 cm) shorter than the left (Left: 67 cm; Right: 45 cm). The patient’s feet measured 17 cm heel to toe.
No motion restrictions of the left leg were noted during passive range of motion (PROM) testing. The right lower extremity PROM was visually estimated as: hip: >90° flexion, >10° extension, >45° abduction, >20° adduction; knee: >120° flexion and slight hyperextension; foot and ankle had no motion restrictions. Muscle strength was assessed using manual techniques and through observation of functional skills. Left lower extremity strength was grossly assessed as Normal. 13 Due to the atypical anatomy of the right hip and knee, the lack of access to a full orthopaedic assessment, and concern for the osseous integrity of the femur, the right hip and knee strength were assessed through active range of motion with no manual resistance. The patient moved the right femur through full available flexion against gravity. He was unable to move into full extension, abduction or adduction against gravity, but could achieve full range in gravity minimized positions. When against gravity he was unable to flex the right knee from full extension or achieve full extension from a flexed position. However, he could actively flex and extend the knee through available range when in a gravity minimized position. Muscle strength surrounding the right foot and ankle was graded to be at least Good. 13 Manual muscle testing is commonly used in a physical examination as it is a valid, reliable, and responsive measurement tool, especially when used by experienced clinicians. 14
Prior to developing a treatment plan it was essential to ensure that the right femur could support body weight. Ultimately, since the patient could ambulate by fully loading the right leg without pain and discomfort, had the ability to control motion around the hip and knee, no restrictions in PROM, and no apparent fractures, it was determined that he could participate in a rehabilitation program including fabrication of a hybrid prosthetic and orthotic device (prosthosis) and subsequent physical therapy.
Findings and Outcomes
Prosthetic/orthotic device
When this patient presented for evaluation the prosthetic/orthotic facility was relocating and not fully operational. Although fabricating a custom device would have been the optimal course of treatment most likely followed in a more developed country, this was not an option at the time the patient was treated. Suffice it to say, there is no ‘off-the-shelf’ device for a case presentation such as this. It is important to note that some decisions made would have been different if adequate materials and resources were available and the prosthetic clinic was fully operational.
After synthesizing the examination data and determining that controlled weight bearing through the limb was safe, the team, consisting of physical therapists and a certified prosthetist and orthotist trained in the ICRC method, determined that the best method to reduce the leg length inequality was to use a solid ankle-foot orthosis (AFO) combined with ICRC polypropylene prosthetic materials and a solid ankle cushion heel (SACH) foot (Figure 2a). This design is similar to one described by Devens. 15 Since we were unable to cast for a custom AFO, we searched the inventory of used, donated devices and found a pediatric hinged AFO approximately the correct size. Further, we searched for a 17 cm prosthetic foot but the smallest available measured 23 cm. The completed device is shown in Figure 2a.

(A) Materials used to fabricate the prosthosis, including the polypropylene components from the ICRC, a SACH foot, and a previously used hinged AFO. (B) Patient standing with prosthosis on right leg.
The hinged AFO was positioned with the foot plate in 1° of dorsiflexion and welded into place using polypropylene rod. A polypropylene convex disk, which is normally attached to the distal end of the socket when fabricating transtibial prostheses using the ICRC method, was welded to the bottom of the AFO. A hole was drilled near the heel and a bolt inserted through the disk and into the ICRC polypropylene pylon. A second bolt was inserted through the plantar side of the SACH foot through another convex disk and into a second pylon. The pylons were cut to size then welded so that the concave pylon would match with the convex disk and allow rotational and translational adjustments. 10 Once alignment was finalized a weld was placed and three straps were added to secure the prosthosis to the limb. The entire build took under one hour.
Rehabilitation protocol
The patient participated in physical therapy twice per day for two weeks. Each session lasted two to three hours. The frequency was based on the availability of physical therapists. The goals of treatment were to progressively increase weight bearing through the prosthosis, improve wearing tolerance, and perform functional and gait training on all surfaces.
On Day 1 the prosthosis was fitted (Figure 2b). The patient needed only minimal assistance to stand. Using one axillary crutch in his left and hand-held assist on the right, he ambulated 10 feet for two repetitions advancing the crutch and right leg together using a combination of a right hip hike, left lateral trunk lean and circumduction (supplementary online video 2). Following this initial walk, the device was removed and no integumentary issues were noted. The patient reported no pain or discomfort, but stated that his right leg ‘felt tired’.
As expected, minor adjustments needed to be made to the AFO since it was not custom made for this patient. Additionally, the shoe initially used had too much of a heel rise. Final adjustments were made and a different shoe was placed on the SACH foot. To improve comfort, padding was placed inside the AFO and added to the straps (Figure 2a).
The patient and his mother were instructed on how to assess the skin and how to don/doff the prosthosis. By Day 3, the patient was independent in these tasks.
A primary focus of treatment included weight-bearing through the prosthosis (Figure 3a) by participating in activities such as standing playing with play-doh, coloring books, blocks, and toy cars. Weight shifting activities were initiated including reaching in all directions as well as stepping onto a one-inch step with one leg then the other. Initially, the patient only tolerated approximately five minutes of standing before requesting to sit. By Day 4, he could tolerate 45 minutes of continuous standing.

(A) Various weight bearing and balance activities. (B) Dynamic balance and advanced gait activities.
Gait training using one axillary crutch was started on Day 1. On Day 3 a forearm crutch was introduced and gait training progressed to activities including inclines and stairs. Initially, when ascending or descending stairs the patient required contact guard due to loss of balance while advancing the right leg onto the next step. By Day 5 he was independent in ramp and stair negotiation (supplementary online video 3).
Higher level gait and balance activities (Figure 3b) were introduced by Day 3 including playing soccer, basketball, and gait training on paths encountered daily consisting of loose rocks. On Day 5 the patient walked ¼ mile down and then up a loose gravel hill independently using one loft strand crutch. During the walk up he completed the task while holding and eating an ice cup in his right hand, a task not previously possible (supplementary online video 4).
A continuation and progression of weight bearing and gait/balance activities were provided on Days 6 and 7. At the completion of Day 7 the patient went home with the prosthosis. He did not return on Day 8. On Day 9 he had no complaints and reported wearing the device the previous day around the home. Treatment on Days 9 and 10 focused on gait/balance and endurance. Supplementary Table 1 (available online) outlines treatment progression. Upon completion of Day 10 the patient was discharged with the prosthosis and one forearm crutch. He was advised to return for follow-up. To date, he has not yet returned and has been lost to follow-up, most likely due to lack of funds for the travel.
Discussion
This case report describes the clinical decision-making process used to determine prosthetic candidacy, and the resulting novel prosthetic management and short-term rehabilitation of a child with PFFD living in an underdeveloped country who expressed a personal goal to walk without crutches. Upon initial evaluation this young boy was able to ambulate independently, non-weightbearing through his right leg using bilateral axillary crutches but was unable to fully participate in playful activities with other children his age. While this ambulatory ability may be considered functional in most scenarios, this is not the case in a country like Haiti where many roads are unpaved and the terrain is uneven and difficult to manage on crutches. If treated in a developed country it is reasonable to suspect that he may have undergone surgery and rehabilitation; however, where this child was located in Haiti, surgery was not an option and rehabilitation care is extremely limited to visiting volunteering clinicians.
This report highlights how a used hinged AFO was modified and incorporated into the fabrication of a prosthesis using ICRC technology. To our knowledge, this technology has not been utilized to fabricate a device such as this. We understand that in optimal conditions, the prosthosis would be different to what was created (e.g. custom AFO, correct size foot) but the aim here was to create a device that would allow for upright ambulation with the limited materials and equipment available. While not cosmetically appealing, the final device allowed the patient to participate in two weeks of intensive gait/balance retraining. Ultimately, the provision of the prosthosis and use of a forearm crutch allowed the patient an opportunity to interact more fully in his environment. It is our hope that continued use will allow him to build the necessary bone and muscle strength required so that at a later date he can be fitted with a correctly sized and more ‘customized’ device. While continuous follow-up and monitoring are crucial to his continued ability to ambulate as he grows, the reality of Haiti reminds us that this follow-up is dependent on the presence of volunteering clinicians. In an effort to make this possible, full documentation and recommendations for future clinicians to follow were left in writing.
Conclusion
This case demonstrates how collaboration among a team can yield innovative and novel results and how a lack of resources does not have to be a limiting factor in the development and implementation of a treatment plan. A thorough understanding of the pathology that is PFFD, principles of orthotic and prosthetic development, creativity, and rehabilitation expertise allowed for the successful management of this case. Working with this patient taught all members of the team the importance of a willingness to try and the power of clinical decision making in helping a young boy gain improved functional independence despite the lack of resources.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.