
Abstract
Purpose: There are around 800 lower limb amputations performed each year in Scotland, however one unpublished study showed that 20% of fitted transtibial amputees do not use, and 20% only occasionally use, their prosthesis at one-year follow-up. This finding has implications for patients' well-being and healthcare cost efficiency. Leventhal's common sense self-regulation model (CS-SRM), a social cognition model in health psychology, was used to determine if psychological variables would predict prosthetic use and activity limitations in lower limb amputees.
Method: A longitudinal study recruited 166 peripheral arterial disease amputees (aged: 50+ yrs). The illness perception questionnaire-revised (IPQ-R) assessed psychological variables at 3–4 weeks post-operatively. Items from the functional measure for amputees (FMA) assessed prosthetic use and the locomotor capabilities index (LCI) evaluated activity limitations at 1-month and 6-months post-discharge. Outcome variables were entered into multiple regression equations with predictor variables.
Results: Significant CS-SRM regression models emerged for predicting prosthetic use, with timeline cyclical (perceptions of symptoms fluctuating) and treatment control (beliefs about treatment efficacy) being the most influential variables. Their effects were stronger at 6-months than at 1-month. The same variables were influential for predicting activity limitations at both 1-month and 6-months. Emotional representations (distressing thoughts) were also influential at 1-month.
Conclusions: Knowledge of how psychological variables determined prosthetic use and activity limitations is valuable because it raises the prospect of being able to identify patients whose psychological profiles render them more at risk of not rehabilitating successfully with a prosthesis, in this case those who perceived symptoms as fluctuating and treatment to be ineffective. Such information could also inform the formulation of elements of psychological care aimed at increasing the number of patients making effective use of their prosthesis and achieving improved activity post-discharge from hospital.
Introduction
The overall number of limb amputations performed each year in Scotland has steadily increased since records began in 1992, peaking at 831 in 2004, however there was a sharp and sudden decrease to 731 in 2005. The mean age of amputees has remained consistent at 69 years, as has the ratio of male vs. female amputees with a typical 65/35 (male/female) distribution. The main cause of amputation is peripheral arterial disease (PAD), which consistently accounts for nearly 90% of cases each year. On average, between 40–45% of PAD cases have concomitant diabetes. Trauma (including burns) and orthopaedic factors are typically the next largest reported causes of amputation, followed by tumour, congenital deformity, drug abuse, venous disease, blood infection and renal failure. Transtibial amputations account for around half of all cases, closely followed by transfemoral amputations. Knee, hip and ankle disarticulations are next most common levels of amputations, followed by transpelvic amputations. On average, only around 40% of all lower limb amputees are fitted with a prosthesis. Transtibial amputees have more chance of being prescribed with a prosthesis (i.e., around 60%) compared to transfemoral amputees (i.e., around 25%) (Condie et al. 2007).
Prosthetic use is an important consideration in amputee rehabilitation because it facilitates reduced activity limitations, which, in turn, assists engaging in daily functions and social participation that may influence mood and quality of life. In Scotland, however, one study revealed that around 20% of fitted transtibial amputees do not use their prosthesis, and a further 20% only occasionally use their prosthesis, at one-year follow-up (Sockalingam et al. 1998). Moreover, prosthetic construction and development, as well as prosthetic patient rehabilitation, are expensive commodities and services that require to be utilised efficiently. Consequently, identifying predisposing variables that influence prosthetic use and activity limitations would be beneficial both to patients and healthcare organisations. Most prediction and correlation studies with amputees have focussed primarily on identifying contextual (Grise et al. 1993), socio-demographic (Taylor et al. 2005) or clinical (Neumann et al. 1998) variables associated with these outcomes. Although less well represented, some studies have supported the influence of psychological variables on amputee outcomes, such as cognitive impairment (Larner et al. 2003), depression (Barnfield 1997) and self-efficacy (Lowther et al. 2002), however drawbacks in study designs and methodology have rendered the role of psychological influences both unclear and unsatisfactory. For example, most studies employed a cross-sectional design, with inherent difficulties in identifying causal direction, while others used relatively small sample sizes, presenting confidence difficulties for inferring results back to the target population. Further, clinical (Cansever et al. 2003) and socio-demographic (Ahmad et al. 1996) variables are known to discriminate between amputee outcomes, however, such variables were seldom controlled during the sampling procedures or analyses in these studies.
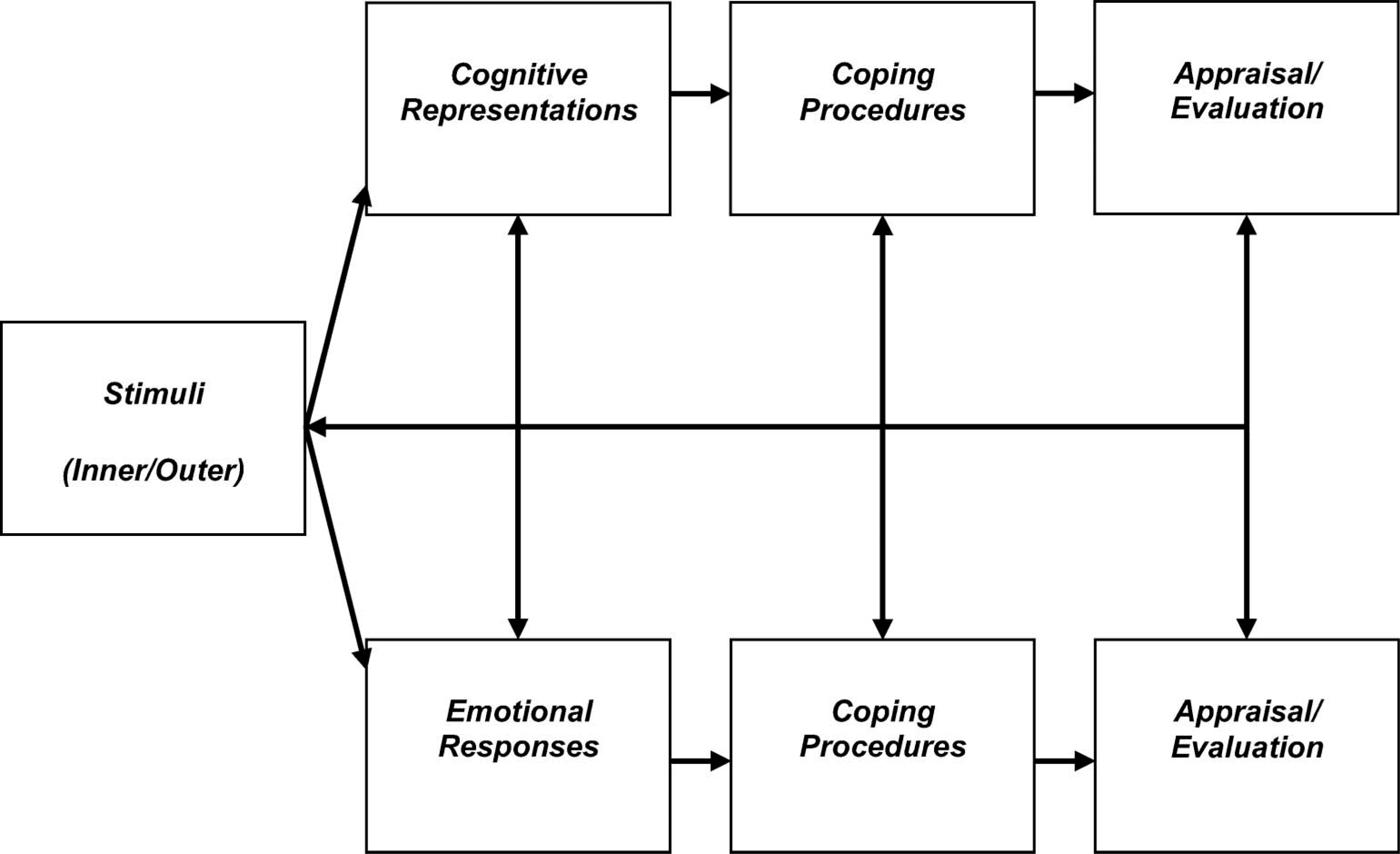
Social cognition models (SCMs) are theoretical models used in health psychology that incorporate how psychological processes influence behaviours. These provide a clear theoretical background and standardised framework for research. Specifically, they guide the selection of variables to measure and further knowledge and understanding of how these variables combine to determine and predict health behaviours and outcomes. Figure 1 provides a schematic representation of a prominent SCM called the common sense self-regulation model (CS-SRM: Leventhal et al. 1980, 1984). According to the CS-SRM, inner (e.g., somatic sensations) or outer (e.g., symptomatic diagnosis) stimuli are reasoned to simultaneously trigger cognitive representations and emotional responses. Cognitive representations are categorized into a number of logical dimensions. These include identity (the number of symptoms the patient associates with the illness), timeline-acute/chronic (perceived duration of the condition), timeline-cyclical (perceptions of symptoms fluctuating), consequences (expected effects and outcomes of the condition), personal control (beliefs that one's condition is self-controlled), treatment control (beliefs that one's condition is controlled by treatment), illness coherence (how much the patient understands or comprehends their condition) and causal attributions (personal ideas about the aetiology of the condition). The model also incorporates emotional representations (emotional responses generated by the condition). Emotional responses typically entail negative affect variables such as fear, anger, worry, stress and distress. In some cases, however, positive affect variables such as relief and determination may be experienced. Cognitive representations and emotional responses, in turn, are reasoned to initiate their respective coping procedures. Those triggered by cognitive representations involve either a) appraisal-focussed coping (e.g., logical analysis) or b) problem-focused coping (e.g., learning new skill such as prosthetic use), while those triggered by emotional responses involve emotion-focussed coping (e.g., denial, acceptance). Coping procedures are then appraised to evaluate their effectiveness. Finally, each construct within the CS-SRM model is reasoned to have the potential to influence any other component within the framework.
The CS-SRM has been applied successfully within a broad range of rehabilitation settings to several physical conditions, such as cancer (Donovan 2004), diabetes (Eiser et al. 2002), multiple sclerosis (Jopson and Moss-Morris 2003), Addison's disease (Heijmans 1999), rheumatoid arthritis (Scharloo et al. 1999), psoriasis (Fortune et al. 2002), osteoarthritis (Orbell et al. 1998) and chronic fatigue syndrome (Moss-Morris et al. 1996). Some studies have explored coping procedures as outcomes, while others have explored activity limitations. Therefore, the CS-SRM was used to determine if psychological variables would predict prosthetic use and activity limitations in lower limb amputees. Specifically, the research questions asked if cognitive representations and emotional responses within the CS-SRM predicted prosthetic use and activity limitations, at 1-month and 6-months post-discharge from inpatient rehabilitation therapy, following lower limb amputation.
Methods
Participant recruitment
A 12-month cohort of transtibial and transfemoral lower limb amputees undergoing post-operative rehabilitation therapy was recruited from eight hospitals in Scotland. Participants were required to be over fifty years of age, fluent in English, and to pass a screening test for cognitive and communication problems. The primary aetiology of their amputation was required to be peripheral arterial disease (PAD).
Measures
Cognitive screening was undertaken using the information and orientation sections of the Clifton Assessment Procedures for the Elderly (CAPE: Pattie and Gilleard 1979). Psychological variables within the CS-SRM were assessed using the illness perception questionnaire - revised (IPQ-R: Moss-Morris et al. 2002). Additional principle components analyses on the IPQ-R data resulted in the development of two causal attribution sub-scales relating to risk factors (i.e., diet or eating habits, one's own behaviour, overwork, alcohol and smoking) and emotional/psychological factors (i.e., stress or worry, mental attitude – thinking about life negatively, family problems/worries; emotional state – feeling down, lonely and personality). Levels of prosthetic use were evaluated using dependent variable items from the functional measure for amputees (FMA: Callaghan et al. 2002). Activity limitations were operationalised by locomotor function (i.e., levels of mobility and personal independence) and were measured using the locomotor capabilities index (LCI: Gauthier-Gagnon et al. 1998).
Procedure
Following approval from relevant research ethics committees, participants were recruited and interviewed by a Senior Physiotherapist or Research Fellow at recruitment between 3- and 4-weeks post-operatively, during inpatient rehabilitation, using the predictor measure. A baseline retrospective measure was also taken for 6-months pre-operative activity limitations. In addition, socio-demographic and clinical details were recorded for both consenting and non-consenting patients. At 1-month and 6-months post-discharge from the rehabilitation hospital, patients were visited in their homes by a trained amputee volunteer, who assisted them to complete the outcome measures. The volunteers (n = 10) were members of the Murray Foundation, which was established as a support service for individuals and their families who have been affected by limb loss or absence in Scotland.
Statistical analyses
Percentages were calculated for categorical variables, while means, standard deviations and ranges were calculated for continuous variables. The socio-demographic and clinical variables were compared between consenting and non-consenting patients using Chi-square analyses for categorical data and two-sample t-tests (or Mann-Whitney U statistics if Kolmogorov Smirnov analyses for normal distribution was significant) for continuous data. MANOVA and post hoc analyses (i.e., Tukey HSD) tested for differences in the LCI measure over time. To develop models for the role of psychological variables in predicting prosthetic use and activity limitations, the outcome variables were entered into multiple linear regression equations with the predictor variables.
Results
At recruitment 166 participants were interviewed, with no patients being lost as a result of cognitive screening. At 1-month follow-up post-discharge from rehabilitation therapy 143 participants were interviewed (86.1% of original sample), and at 6-months follow-up 120 participants were interviewed (72.3% of original sample, and 83.9% of 1-month follow-up sample). The average length of inpatient stay in hospital post-operatively was 65 days (SD = 52, range = 386). Age, amputation level and gender data relating to participants at each interview time are summarized in Table I.
Summary of the means, standard deviations and ranges for age with percentages for amputation level and gender ratios at each assessment time.
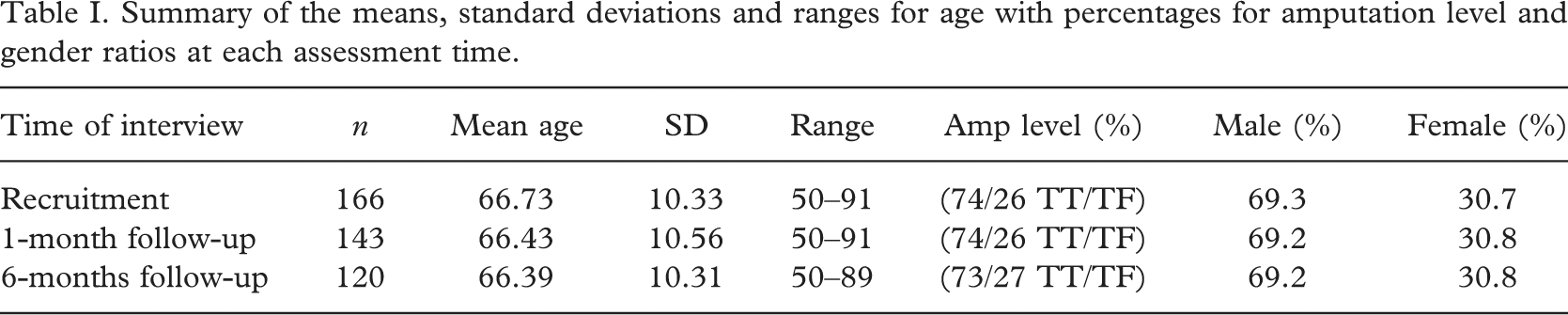
The consent rate at recruitment was 70.9% (i.e., consenters = 166, non-consenters = 68). Comparisons between consenting and non-consenting patients on demographic and clinical variables revealed significant differences in age (Mann-Whitney U = 3515.000, N1 = 165, N2 = 67, p < 0.001, two-tailed), level of amputation (Chi-square = 1.598, df = 1, p < 0.001) and Scottish index of multiple deprivation (SIMD, 2004) scores (Mann-Whitney U = 4659.000, N1 = 164, N2 = 68, p < 0.05, two-tailed), but not in gender or unilateral/bilateral status. That is, at recruitment, consenting patients were younger, more likely to be transtibial amputees, and lived in less deprived areas than non-consenting patients.
There were significant differences in overall activity limitations over the three assessment periods according to the MANOVA analyses (F 2, 216 = 20.334, df = 2, p < 0.001). In particular, significant differences were found, following post hoc analyses (i.e., Tukey HSD), between 6-months pre-operative levels and 1-month follow-up (p < 0.001) and between 6-months pre-operative levels and 6-months follow-up (p < 0.001).
Descriptive data for prosthetic use at 1-month follow-up related to percentage of moves made indoors (mean = 49.12, SD = 39.82, range = 100), percentage of moves made outdoors (mean = 41.90, SD = 44.62, range = 100), hours per day (mean = 8.82, SD = 4.98, range = 19) and days per week (mean = 6.20, SD = 2.01, range = 7). At 6-months follow-up, data again related to percentage of moves made indoors (mean = 55.46, SD = 41.45, range = 100), percentage of moves made outdoors (mean = 53.96, SD = 46.40, range = 100), hours per day (mean = 10.01, SD = 4.86, range = 22) and days per week (mean = 6.37, SD = 1.91, range = 7). There were improvements on all four prosthetic use outcome variables between 1-month and 6-months follow-up (Figure 2).
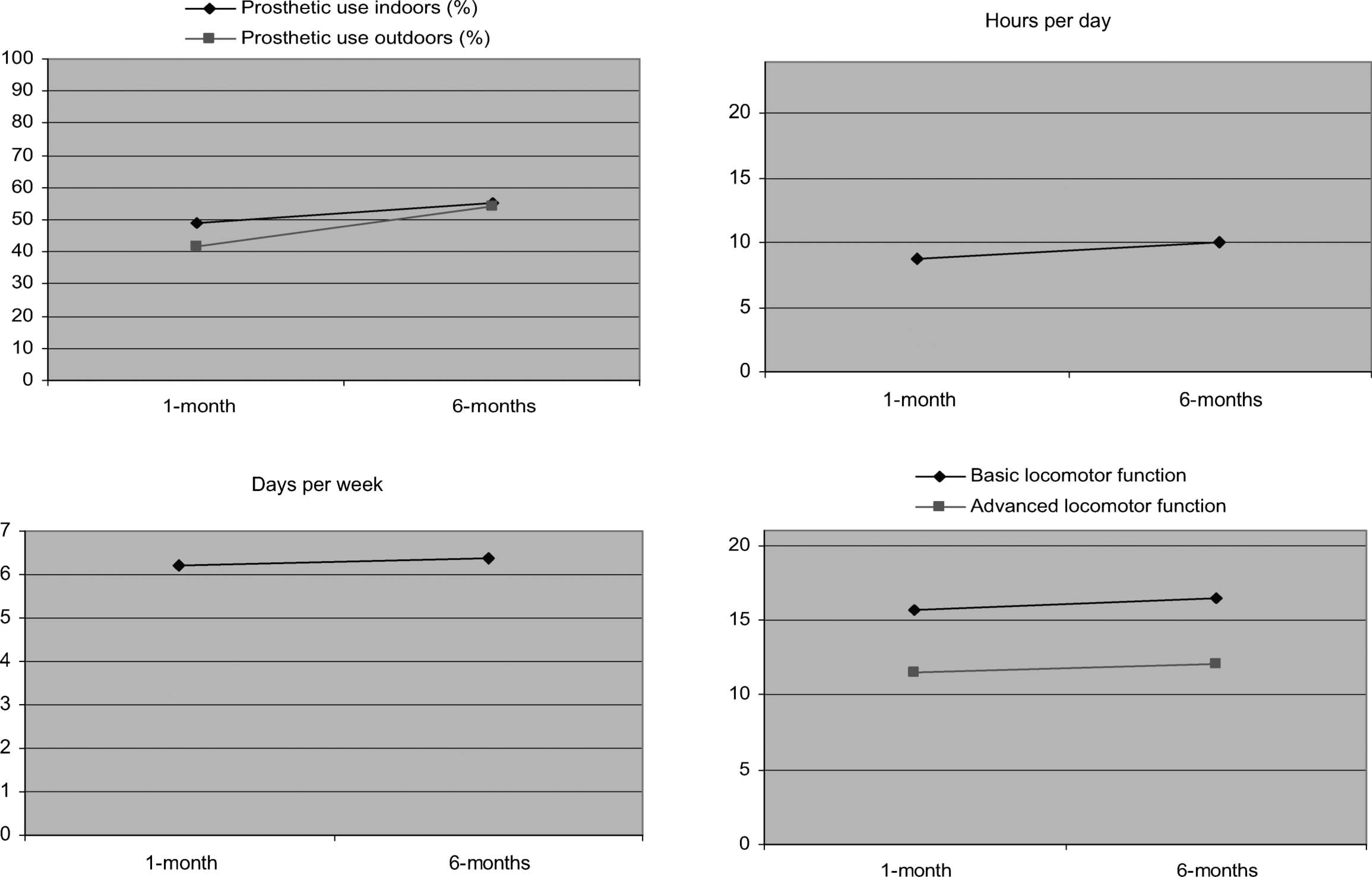
Improvements in prosthetic use and activity limitations between 1-month and 6-months follow-up.
Descriptive data for activity limitations at 1-month follow-up related to basic function (mean = 15.74, SD = 6.77, range = 21) [possible = 0–21] and advances function (mean = 11.49, SD = 7.61, range = 21) [possible = 0–21]. At 6-months follow-up, data again related to basic function (mean = 16.47, SD = 6.73, range = 21) and advanced function (mean = 12.13, SD = 7.70, range = 21). There were improvements on both levels of the activity limitations outcome variable between 1-month and 6-months follow-up (Figure 2).
Table II illustrates the results for CS-SRM psychological predictors of prosthetic use. A significant CS-SRM model emerged for predicting indoor prosthetic use at 1-month. Timeline (cyclical) emerged as the sole significant predictor variable within the model, while treatment control and causal attributions (risk factors) approached significance. Despite having higher beta coefficients than timeline (cyclical), the confidence intervals of the latter two variables passed through zero, indicating non-significance. Within this model, therefore, amputees who perceived during rehabilitation that their physical symptoms fluctuated less, used a prosthesis more indoors at 1-month post-discharge.
Summary of CS-SRM psychological variables prediction of prosthetic use at 1 and 6 months post-discharge: Results of multiple regression analyses with four dependent variables on each occasion.
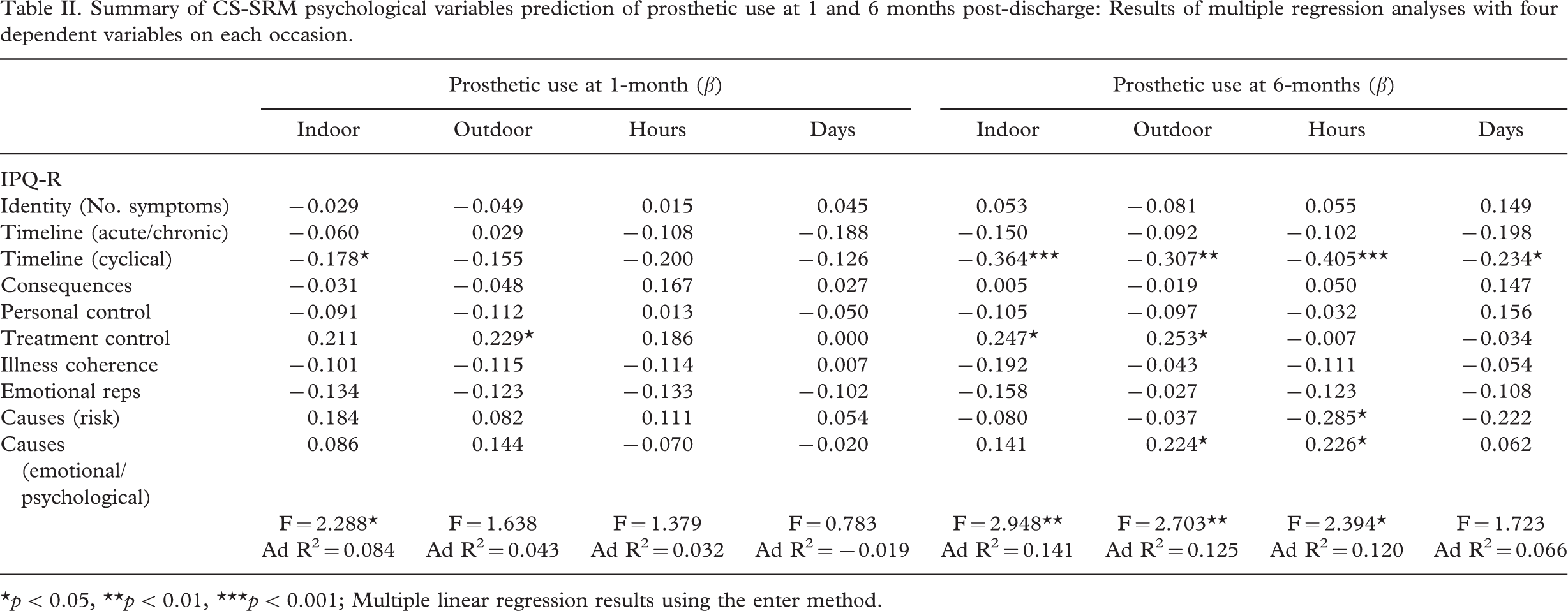
∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001; Multiple linear regression results using the enter method.
At 6-months, a significant CS-SRM model also emerged for predicting indoor prosthetic use. Timeline (cyclical) and treatment control emerged as significant predictor variables within this model. This meant, that amputees who perceived during rehabilitation that: (a) Their physical symptoms fluctuated less, and (b) Their treatment would be effective in controlling their condition, used a prosthesis more indoors at 6-months post-discharge.
A significant CS-SRM model also emerged for predicting outdoor prosthetic use at 6-months. Timeline (cyclical), treatment control, and causal attributions (emotional/psychological) emerged as significant predictor variables within the model. Therefore, amputees who perceived during rehabilitation that (a) their physical symptoms fluctuated less, (b) their treatment would be effective in controlling their condition, and (c) their condition was caused by emotional/psychological factors (e.g., stress, mental attitude, personality, etc.), used a prosthesis more outdoors at 6-months post-discharge.
A CS-SRM model also significantly determined hours per day of prosthetic use at 6-months, with timeline (cyclical) and causal attributions (risk factors and emotional/psychological factors) emerging as significant predictor variables within the model. That is, amputees who perceived during rehabilitation that (a) their physical symptoms fluctuated less, (b) their condition was not caused by risk factors (e.g., diet, overwork, smoking, etc.), but was caused by emotional/psychological factors (e.g., stress, mental attitude, personality, etc.), used a prosthesis more hours per day at 6-months post-discharge.
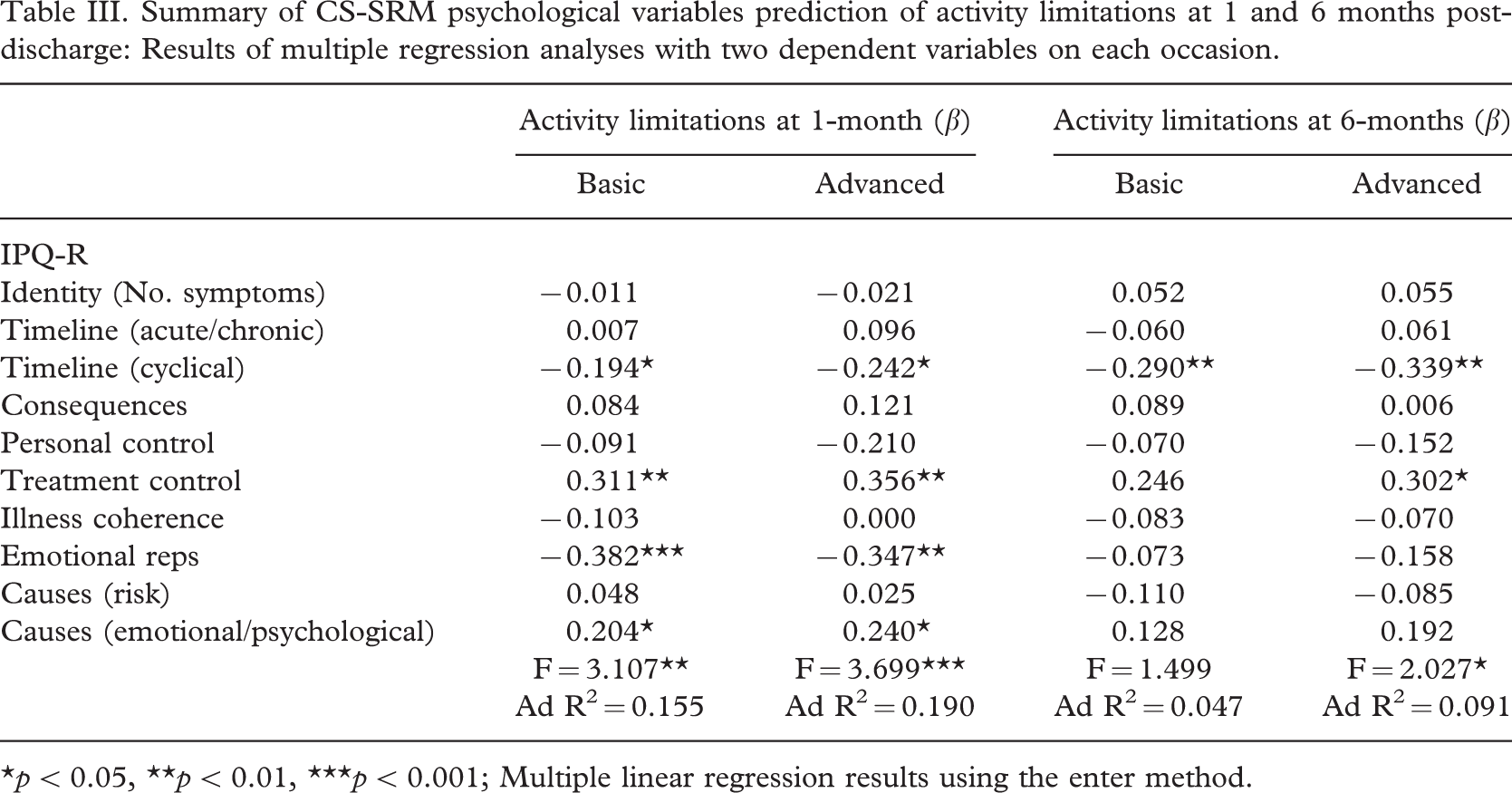
Table III illustrates the results for CS-SRM psychological predictors of activity limitations. A significant CS-SRM model emerged for predicting both basic and advanced activity limitations at 1-month. Timeline (cyclical), treatment control, emotional representations, and causal attributions (emotional/psychological) emerged as significant variables within both models. Therefore, amputees were more mobile and independent (basic and advanced) at 1-month post-discharge if they perceived during rehabilitation that: (a) Their physical symptoms fluctuated less, (b) Their treatment would be effective in controlling their condition, (c) they had less negative emotional representations about their condition (e.g., worried, angry, afraid, etc.), and (d) their condition was caused by emotional/psychological factors (e.g., stress, mental attitude, personality, etc.).
Summary of CS-SRM psychological variables prediction of activity limitations at 1 and 6 months post-discharge: Results of multiple regression analyses with two dependent variables on each occasion.
∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001; Multiple linear regression results using the enter method.
Finally, a significant CS-SRM model emerged for predicting activity limitations (advanced only) at 6-months. Timeline (cyclical) and treatment control emerged as significant predictor variables within the model, meaning that amputees had better advanced mobility and independence at 6-months post-discharge if they perceived during rehabilitation that (a) their physical symptoms fluctuated less, and (b) their treatment would be effective in controlling their condition.
Discussion
Around 20% of fitted transtibial amputees in Scotland do not use their prosthesis, and a further 20% only occasionally use their prosthesis, at one-year follow-up according to one Scottish study. This finding has implications for patients' well-being and healthcare cost efficiency, however the reasons for this non/limited prosthetic use are unclear. Prosthetic use impacts directly on activity limitations, which, in turn, has the potential to influence mood, social participation and quality of life outcomes. Most studies have examined how physical, socio-demographic and clinical variables have influenced prosthetic use and activity limitation outcomes in amputees. A small section of the amputation literature has explored how psychosocial variables have correlated with prosthetic use or activity limitations, however, these studies have had methodological limitations. The current study improved upon previous methodology by using a longitudinal predictive design and a relatively large sample size, and by recruiting peripheral arterial disease amputees over 50 years of age, as traumatic (Cansever et al. 2003) and younger (Ahmad et al. 1996) amputees are known to systematically influence outcome variables. Moreover, this study employed the common sense self-regulation model (CS-SRM: Leventhal et al. 1980, 1984), which is a prominent social cognition model in health psychology, to guide the investigation.
The loss of no patients after cognitive screening may have been due to the onsite healthcare staff not recruiting individuals from the outset that they deemed to be incapable of participating in the study. The loss of just over a quarter of the original sample at 6-months follow-up may have had implications because the multiple linear regression analyses excluded cases for which there were incomplete data sets. Consequently, it is reasonable to assume that amputees with poorer function post-discharge were lost at follow-up and, hence, less likely to have been represented by these results. Moreover, significant differences were found in certain socio-demographic and clinical variables between the consenting and non-consenting patients at recruitment. Although patients were required to be over 50 years of age, the reasons for these observations are likely to be due to a disproportionate amount of younger, healthier transtibial amputees taking part in the study, compared to older, more cognitively impaired transfemoral amputees. Accordingly, it is arguable that the sample was not strictly representative of a new cohort of Scottish lower limb amputees, and any subsequent interventions resulting from this study may not be applicable or effective with more vulnerable patients.
Prosthetic use
Encouragingly, improvements on all prosthetic use outcome variables were noted between 1-month and 6-months follow-up. Moreover, excluding cases lost at 6-months, who may arguably have been those more likely to have decreased or abandoned prosthetic use after the first month, improvements were still found on all four prosthetic use outcome variables, with outdoor prosthetic use (t = − 3.16, p < 0.01) and hours per day of prosthetic use (t = − 2.71, p < 0.01) achieving statistical significance. Of further note in relation to these data, however, are the large standard deviations observed on the percentage of moves made using a prosthesis indoors and outdoors. This was probably because participants had a tendency to report using their prosthesis for either none (0%) or, alternatively, all (100%) of their transfers.
The CS-SRM cognitive representations of timeline (cyclical) and treatment control were the predominant underlying psychological variables within the models that determined prosthetic use, both at 1-month and 6-months post-discharge from rehabilitation (especially at 6-months). Timeline (cyclical) relates to the perception that one's physical symptoms fluctuated on a regular basis. Patients who perceived that their symptoms were coming and going during rehabilitation experienced less favourable prosthetic use outcomes. The most frequently reported physical symptoms in the current sample related to pain (i.e., phantom pain/sensation, stump pain, general pain). Cognitive beliefs about pain, particularly catastrophising, have been found to impact on quality of life outcomes in chronic pain patients (Lame et al. 2005), and cognitions have also been found to influence self-reported phantom limb pain, as well as physical and psychosocial dysfunction, in amputees (Hill et al. 1995). Treatment control relates to beliefs that one's treatment would be effective in curing or controlling their condition. Those patients who held such beliefs experienced better prosthetic use outcomes. It may be then, that having had more confidence in the efficacy of their therapy, these patients were more eager to follow the advice of the allied healthcare professions involved in their rehabilitation and, consequently, they may have adhered more closely to, and engage more readily in, their prescribed treatment regimes with a prosthesis.
Both of the CS-SRM causal attribution cognitive representations (i.e., risk factors and emotional/psychological factors) were influential in determining prosthetic use at 6-months, but not at 1-month post-discharge. Notably, there was a negative beta coefficient denoting the significant relationship between risk factors and prosthetic use, as opposed to a positive beta coefficient denoting the significant relationship between emotional/psychological factors and prosthetic use. In effect, this meant that patients who held beliefs that their condition was not caused by variables such as diet or eating habits, their own behaviour, overwork, alcohol and smoking (i.e., risk factors) used their prosthesis more, whereas patients who held beliefs that their condition was caused by variables such as stress or worry, mental attitude – thinking about life negatively, family problems/worries; emotional state – feeling down, lonely and personality (i.e., emotional/psychological factors) used their prosthesis more. Accordingly, it may be the case that patients who never smoked, had healthy diets and had always led a low risk lifestyle in general, were more inclined to look after themselves and have a positive determined outlook on life and, hence, perhaps they persevered more with using a prosthesis. Or, such patients could have been experiencing some degree of denial, as a coping procedure for emotional responses, and may, therefore, have been more able to ignore the negative aspects of their lives, such as losing a leg, and adopt a more positive approach by simply getting on with matters (e.g., using a prosthesis, engaging in activities). Conversely, it may be the case that patients who were more stressed, worried and experienced more negative affect in general during inpatient rehabilitation, used their prosthesis more post-discharge as a coping mechanism to manage such poor emotional/psychological dispositions. Or, they may have felt that they needed to compensate for having held such negative thoughts which, in their view, led to requiring an amputation in the first instance, by becoming more positive about their rehabilitation and, subsequently, they engaged in more prosthetic use.
Notably, the effects of all the prominent CS-SRM cognitive representations were significantly stronger for determining prosthetic use at 6-months rather than at 1-month follow-up. Thus, the influence of psychological variables on prosthetic use did not diminish but, in fact, increased in strength as a factor of time since discharge from rehabilitation. Also, within the CS-SRM framework, cognitive representations are reasoned to influence problem-focussed coping procedures, of which prosthetic use may conceptually be regarded, while coping procedures are also reasoned to impact on emotional responses. To this end, some additional analyses revealed that more hours per day of prosthetic use at 1-month significantly predicted less anxiety (r = − 0.28, p < 0.01) and less depression (r = − 0.27, p < 0.01) at 6-months, while more days per week of prosthetic use at 1-month also significantly predicted less anxiety (r = − 0.28, p < 0.01) at 6-months. Psychological distress variables were measured at both follow-up times using the hospital anxiety and depression scale (HADS: Zigmond and Snaith 1983). Moreover, levels of anxiety and depression did not significantly increase or decrease over this period of time. These additional prosthetic use findings would further seem to support the theoretical framework of the CS-SRM. That is, using a prosthesis undoubtedly increased mobility, independence and participation in activities, all of which are subjectively important factors for amputees (Callaghan and Condie 2003), which, in turn, impacted positively on emotional outcomes.
Activity limitations
There were marginal improvements in both basic and advanced activity limitations between 1-month and 6-months follow-up, although, these may have been influenced by less active individuals dropping out of the study after the first month. Nevertheless, improvements on both levels of the activity limitations outcome variable were still observed when such cases were excluded, although these did not achieve statistical significance. Having taken a baseline retrospective assessment of 6-months pre-operative activity limitations at recruitment, however, significant differences were found between 6-months pre-operative levels and 1-month follow-up and between 6-months pre-operative levels and 6-months follow-up. This latter result demonstrated that although activity levels with a prosthesis steadily improved between the two follow-up assessment times, they had not significantly returned to pre-operative levels of activity.
In relation to predicting activity limitations, the CS-SRM cognitive representations of timeline (cyclical) and treatment control were again the predominant psychological predictor variables within the model for determining activity limitations. This was, perhaps, not unexpected considering that these constructs also significantly predicted prosthetic use. As with predicting prosthetic use, the influence of the CS-SRM timeline (cyclical) and treatment control variables on activity limitations was evident at both 1-month and 6-months post-discharge. Again, within the dynamics of the CS-SRM framework, it is feasible to view prosthetic use as a problem-focused coping procedure, which facilitated amputees being more active (i.e., mobile and independent) in their environments, which, in turn, could potentially impact on mood and quality of life outcomes. That is, improved activity limitations may be appraised or evaluated by individuals as a positive consequence of this coping procedure (i.e., engaging in prosthetic use), which may, subsequently, influence other constructs within the model, such as emotional responses. In support of this position, additional analyses revealed that overall activity limitations at 1-month significantly predicted both anxiety (r = − 0.25, p < 0.05), and depression (r = − 0.27, p < 0.01) at 6-months.
CS-SRM emotional representations, and to a lesser extent causal attribution cognitive representations (emotional/psychological), also contributed towards the prediction of activity limitations, but only at 1-month follow-up. That is, the influence of the emotionally related CS-SRM cognitive variables (i.e., emotional representations and emotional/psychological causal attributions) was lost at 6-months follow-up on activity limitations. This finding suggested that emotionally orientated cognitions influenced activity limitations, but that the effect was ephemeral because it was not sustained to influence activity limitations at 6-months post-discharge from hospital.
The influence of a control-related predictor variable, in this case treatment control, on activity limitations is consistent with earlier studies of other physical conditions (e.g., Moss-Morris et al. 1996; Orbell et al. 1998; Eiser et al. 2002), however, perceptions of symptoms fluctuating have less often been found to demonstrate a significant effect on outcomes. Moreover, the hypothesis that such perceptions may simply have served as a proxy for patients who were more ill was not supported, due to a non-significant correlation between the timeline (cyclical) variable and transfemoral cases in this study. Finally, activity limitations have sometimes been predicted by perceived consequences in other physical conditions (e.g., Moss-Morris et al. 1996; Orbell et al. 1998), however, this particular cognitive representation was not a significant determinant of prosthetic use or activity limitations with the current sample of amputees.
Knowledge gained from the present study is valuable in that it has identified the predictive relationships between specific psychological variables and rehabilitation and health outcomes in amputees, using a valid social cognition model. Knowledge of these predictive relationships can impact on NHS service delivery in several ways. Firstly, it may be used to identify patients whose psychological profile renders them at more risk of: (a) not rehabilitating as successfully with a prosthesis, and (b) not achieving favourable activity limitation and psychological distress outcomes, in this case those who predominantly perceived symptoms as fluctuating and treatment to be ineffective. Secondly, it raises the prospect of being able to formulate new psychotherapeutic interventions, or adapt existing cognitive behavioural therapies, aimed at influencing these psychological variables with the goal of increasing the numbers of patients: (a) making effective use of a prosthesis, and (b) achieving successful long term rehabilitation and health outcomes, on physical, behavioural, and psychological levels.