
Abstract
Background:
Due to limitations in provision of prosthetic care in South Africa, a screening tool to select transfemoral prosthetic candidates has been implemented.
Objective:
To describe prosthetic services, use and mobility of people with transfemoral amputation, identified as prosthetic candidates through the Guidelines for Screening of Prosthetic Candidates: Lower Limb, and to identify variables that might influence prosthetic use and mobility.
Design:
Cross-sectional survey.
Methods:
The study population included all adults who received their first prosthesis from the Orthotic and Prosthetic Centre in the Western Cape between 1 June 2011 and 31 December 2014. Data were collected, with an adapted version of the Prosthetic Profile of the Amputee, from 43 participants, through telephonic interviews. Descriptive and inferential analysis, with the chi-square test, was done.
Results:
The majority of participants were older than 50 years (77%). Most participants (35; 81%) used their prosthesis; however, only 42% (18) used it daily. A significant association (p = 0.000) was found between prosthetic rehabilitation and self-reported prosthetic walking distance. Less than half of participants received prosthetic rehabilitation and only 10 (30%) could walk 500 steps and more without resting.
Conclusion:
Participants used their prosthetic leg, but experienced limitations in frequency of wear and mobility.
Clinical relevance
Current findings showed that participants’ prosthetic mobility was curtailed. In less-resourced settings, carefully selecting prosthetic candidates may be necessary to provide access to services. Prosthetic provision is advised to be followed up with prosthetic rehabilitation for favourable mobility outcomes.
Keywords
Background
The World Health Organization 1 estimates that more than 1 million limb amputations are done globally each year. Specific incidence and prevalence figures for lower limb amputation in Africa or South Africa could not be identified. Dunbar et al. 2 found that 1517 lower limb amputations were done at four public hospitals in Cape Town, South Africa, in 2009 and 2010. Diabetes was the main cause of amputation (69.6%) followed by vascular conditions (26.8%). 2 The incidence of lower limb amputations increases with age and mean ages of study participants are often above 60 years of age.2–5
A prosthesis can enhance mobility and physical function after amputation. 6 However, transfemoral prosthetic mobility can be challenging,7,8 and not all will be able to walk with a prosthesis.9,10 Due to the loss of the normal knee joint, transfemoral prosthetic mobility is more challenging than transtibial prosthetic mobility as energy demands increases, along with dynamic balance and strength demands.11–13 Hagberg and Branemark 14 showed that users of transfemoral prostheses can often only walk short distances before they have to stop and are often reliant on additional hand-held walking devices.14,15
Studies from developed countries reported that 75%–87% of participants used their prosthesis daily.13,14,16 From South Africa, De Klerk et al. 10 reported that 11.1% of participants used a prosthesis for mobility while a study from Nigeria showed that only 7% (56) of people used their prosthesis. 17
Prosthetic use and mobility may be affected by intrinsic factors, such as cause and level of amputation, condition, strength and mobility of the residual limb, cardiovascular fitness, dynamic balance and pre-morbid mobility.6,12 Prosthetic use and mobility may also be affected by extrinsic factors, such as type of prosthesis, prosthetic components, prosthetic fit, alignment and the environment in which prosthesis is used.18–21 The use of basic prosthetic components, prosthetic fit, suspension and alignment were challenges identified in studies in less developed settings.18,22 Prosthetic rehabilitation plays an important role in facilitating prosthetic function.18,23 However, access to prosthetic rehabilitation is limited in less developed settings, 24 including South Africa. 25 Challenges included transport, lack of knowledge about rehabilitation services and insufficient number of service providers.24,25 Finally, the environment in which the prosthesis is used in less developed settings often place high demands on prostheses and user.18,24
The realisation of the above described challenges in transfemoral prosthetic use, and the reasoning that prosthetic mobility is not always the most suitable mobility option after amputation, 9 led to the development of an evidence-based prosthetic screening tool, Guidelines for Screening of Prosthetic Candidates: Lower Limb. 26 This tool is used to guide pre-prosthetic rehabilitation pathways of persons with lower limb amputations and select prosthetic candidates 26 and has been implemented in certain settings of South Africa. 27 However, the prosthetic outcomes of clients identified as prosthetic candidates with this tool have never been assessed.
The aim of this study is to (1) describe the prosthetic services, use and mobility of people with unilateral transfemoral amputation, identified as prosthetic candidates through the Guidelines for Screening of Prosthetic Candidates: Lower Limb; and (2) to explore possible factors that might influence prosthetic use and mobility within the population.
Methods
A cross-sectional survey was done to describe prosthetic use and mobility of a selected group of persons with transfemoral amputation residing in the Western Cape Province of South Africa. The Province has a total population of 5,822,634, with sex ratio of 51% females compared to 49% males. 28 The major languages spoken in the province are Afrikaans (49.7%), followed by isiXhosa (24.7%) and English (20.2%). 28 The average household lives in a formal dwelling (80%), where most households (89%) have a land line and/or cell phone. 28
The Western Cape metro has one ‘Orthotic and Prosthetic Centre’ (OPC) that serves everybody who accesses public orthotic and prosthetic services. 29 The choice of prosthetic components in the public sector is limited and reflects components used in less resourced settings. 22 The knee and foot components used at OPC at the time of the study was a single-axis, single speed, hinge knee joint and a solid ankle-cushion heel (SACH) foot. Both these components are classified as basic, low level activity, and suitable for indoor and limited outdoor mobility.20,21 A quadrilateral socket and, as suspension, the Silesian belt with stump socks are commonly provided.
The study population was identified from OPC records and included all persons older than 18 years, with a unilateral transfemoral amputation, who had received their first prostheses at the OPC between 1 June 2011 and 31 December 2014, after screening with the Guidelines for Screening of Prosthetic Candidates: Lower Limb, 26 and according to hospital records, they were fluent in Afrikaans, isiXhosa or English. Twenty-nine variables that play a role in prosthetic use are assessed by the Guidelines for Screening of Prosthetic Candidates: Lower Limb. Variables relate to cause, number and level of amputations (2); health status (9); user expectations (1); mobility and balance (8); function (3); contralateral leg (1); and residual limb (8).26,27 Persons with major upper limb impairment, according to information in their hospital records, that could interfere with managing hand-held mobility assistive devices were excluded. The total population counted 88 people. From the population, seven had passed away, five had further amputations and one had no contact phone number. This left 75 people. A sample size calculation showed that a sample of 63 participants was required (CL 95%, CI 5%, population size 75 and response distribution 50%). Due to the small difference in number (12) between population and number of participants required, no sampling was done. Attempts were made to contact all 75 people. However, 32 persons could not be located due to a change in phone number, or unanswered phone calls or text message.
Data were collected through a questionnaire based on the Prosthetic Profile of the Amputee (PPA). 30 The PPA was selected as measuring instrument since it evaluates lower limb prosthetic use and the factors related to prosthetic use or disuse. The PPA is a self-reported measure; no clinical assessment was done to verify participants’ responses. 30 The original questionnaire was developed and demonstrated validity and reliability for an elderly Canadian population, 31 culturally very different from a South African setting. The PPA was therefore adapted (Figure 1), with approval of the author, to allow for questions that are more realistic and understandable within the different cultural and health setting. This adapted version of the PPA was not tested for validity and reliability, a recognised weakness. However, since no tool that measures the variables that addressed the study aim, and that was validated for the setting could be identified, the decision was made to use the adapted PPA. In broad terms, the following issues were addressed:
To facilitate understanding, certain Canadian language terms were changed to reflect South African English and context.
Original questions, not applicable to the current study population, were removed or altered.
Two questions applicable to current study setting and the study aims were added, namely: a question on date of amputation and date prosthesis received, and a question on whether participants received at least one session of prosthetic rehabilitation.
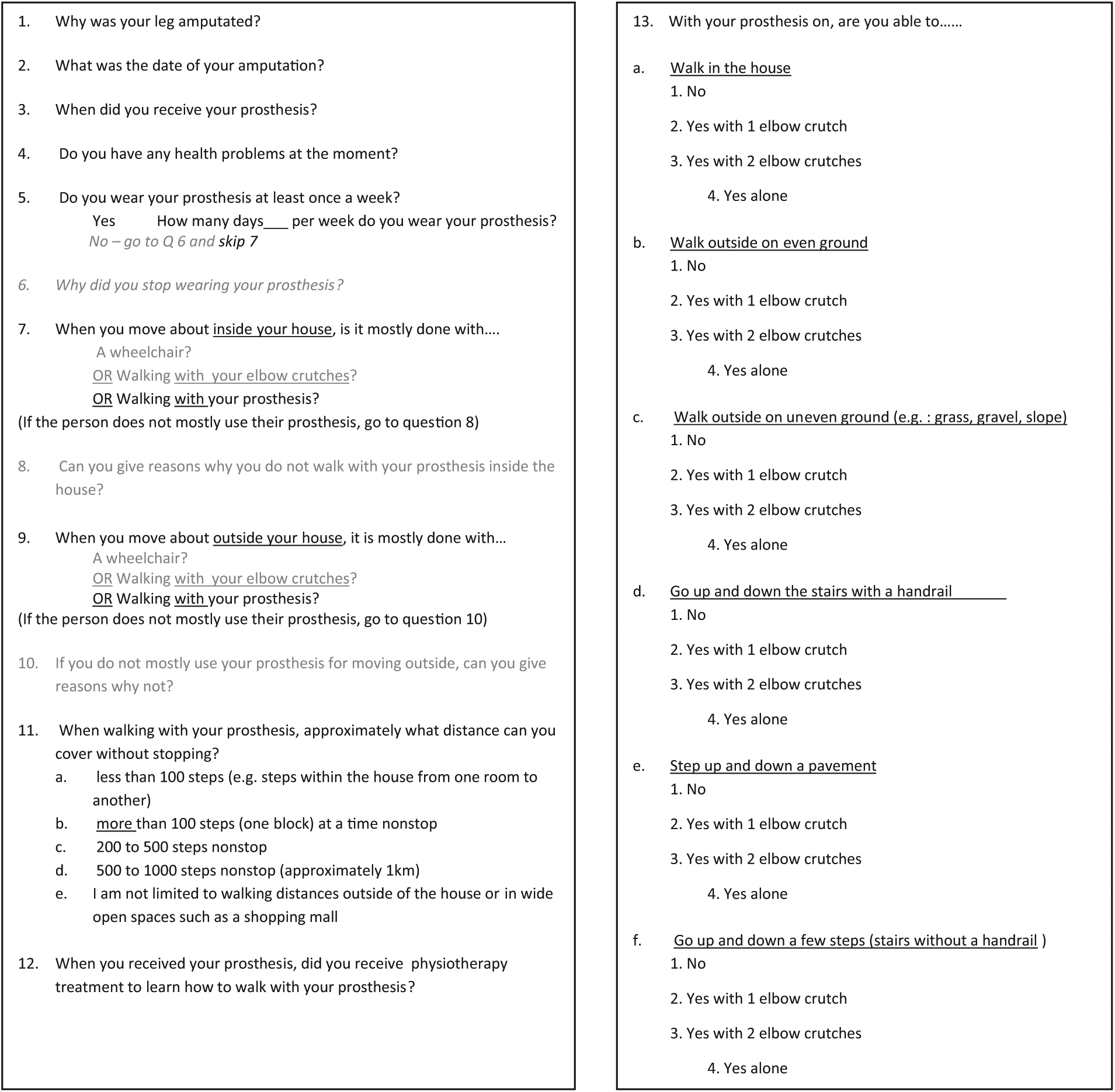
Questions in the adapted version of the Prosthetic Profile of the Amputee.
Translation to Afrikaans and Xhosa was done through professional language translators and back translation was checked by clinical experts. The final version was based on the opinion of the clinical experts as the few discrepancies noted were related to clinical terminology. The PPA was developed for self-administration, face-to-face interview or telephone interview. 30 To pre-empt transport challenges (in South Africa many people reliant on public health care services are dependent on public transport, which is notoriously inaccessible for persons with disabilities 32 ), the PPA was completed in May and June 2015 by means of a telephonic interview. The interviews were done by three research assistants fluent in English, Afrikaans or Xhosa, respectively. The research assistants were trained by the first author, focusing on the consistent application of the data collection instrument, followed by two pilot interviews.
Data from the questionnaire were coded and captured in an Excel spread sheet by the first author. Further analysis of the data was performed using the chi-square test, testing the following variables for significant relationships:
Prosthetic use: frequency of prosthetic wear, in relation to prosthetic mobility: (1) distances walked and (2) mobility with or without elbow crutches.
Prosthetic use in relation to demographic: (1) age, (2) time since amputation, medical: cause for amputation, and rehabilitation variables: attendance of prosthetic rehabilitation.
Prosthetic mobility in relation to demographic, medical and rehabilitation variables.
Significance level of alpha = 0.05 was determined.
Ethical implications
The proposed study was ethically approved by the Human Research Ethics Committee of the University of Stellenbosch (S14/10/215). Permission from Western Cape Department of Health and study settings was obtained. Participants were not exposed to risks. Participant’s personal details were kept confidential. All information was stored in electronic format and secured by means of a password. Participants were told that their participation in the study was on a voluntary basis and that refusing to continue, at any point, would not negatively impact future health care needs. Severe impaired cognition or psychological instability is a contra-indication for receiving prostheses in public services, in the Western Cape as walking with transfemoral prosthesis demands cognitive focus. Thus, these issues could not have impacted the consent process. Informed consent was obtained telephonically, recorded by a Dictaphone, and signed for by a witness.
Results
Demographic information
The ages of study participants ranged from 19 to 80 years, with a mean of 55.2 (SD, 14.25) years. The majority of study participants were men (34; 79%) with a male-to-female ratio of just below 3:1.
Cause of amputation and current health status
Vascular conditions (30; 70%) with or without diabetes caused the majority of amputations (Table 1). Nonvascular conditions included trauma (7; 16%), cancer (3; 7%) and infection (3; 7%). Hypertension (20; 47%) was the most common co-morbidity.
Summary of participant’s medical information.
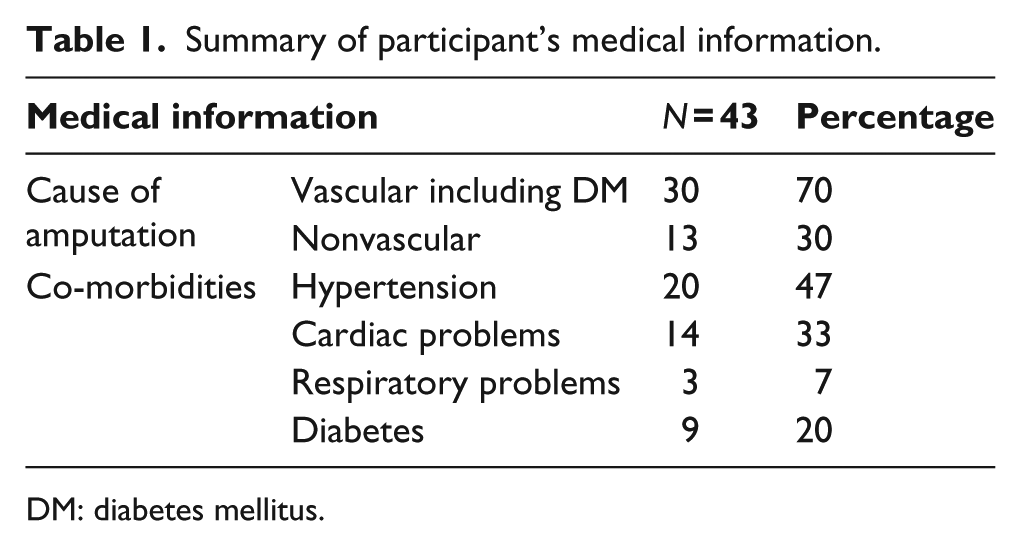
DM: diabetes mellitus.
Prosthesis and prosthetic services
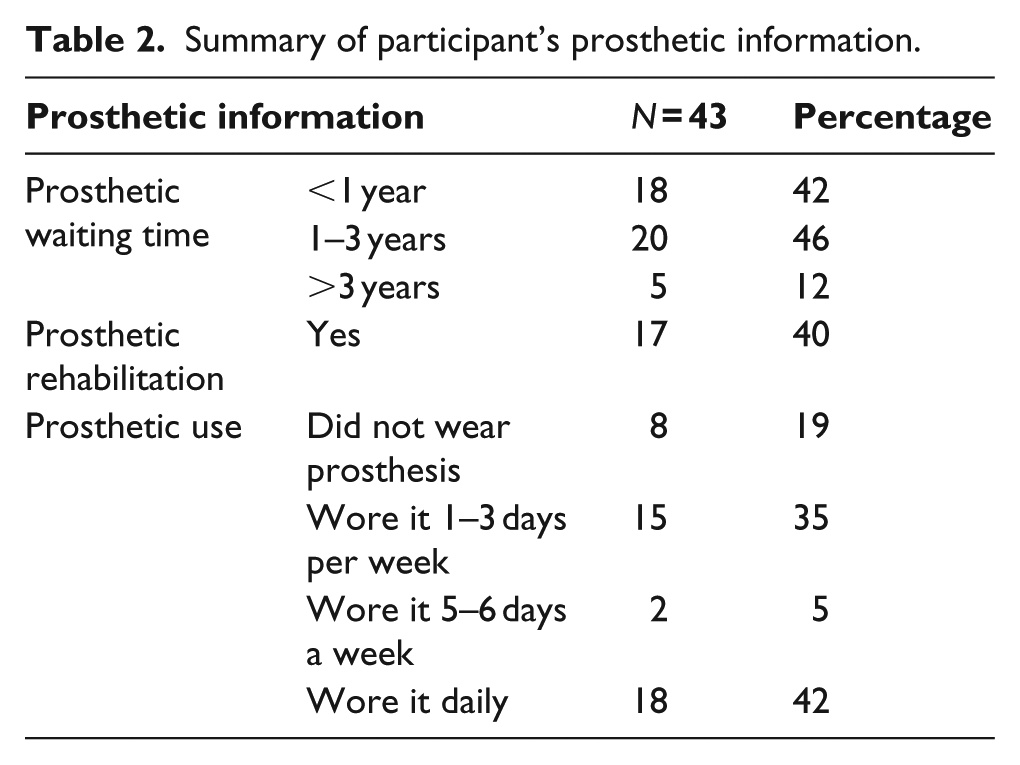
Forty-two percent (18) of participants received their prosthesis within a year of the amputation (Table 2). More than half of the participants (26; 60%) did not receive prosthetic rehabilitation.
Summary of participant’s prosthetic information.
Prosthetic use
Eighty-one percent (35) of participants reported that they wore their prosthesis at least once a week. Of this 35, 18 (42%) wore their prosthesis daily (Table 2). Prosthetic fitting problems (5) were the main reason given for non-use. Other reasons included walking with the prostheses is tiring and slow (4), fear of falling (2) and not knowing how to walk with the prosthesis (1).
Prosthetic use and prosthetic rehabilitation: Within the group who had received prosthetic rehabilitation, a higher percentage of participants (10; 59%) wore their prosthesis 5–7 days per week compared to those who had not received rehabilitation (10; 38%; Figure 2).
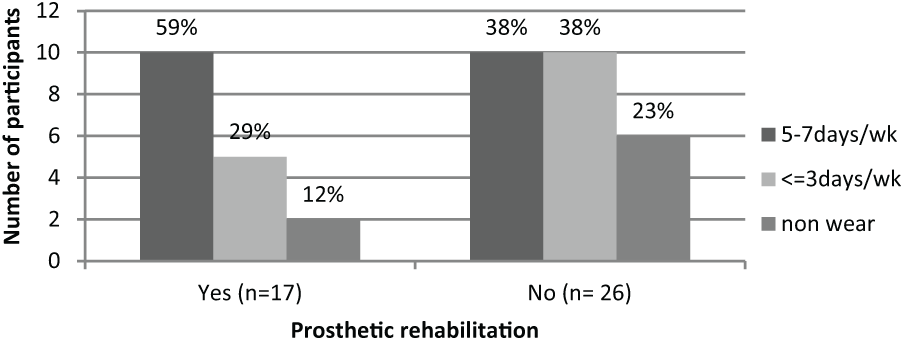
A comparison of the number of participants that used prostheses (in days per week) for people receiving prosthetic rehabilitation or not.
Prosthetic mobility
Walking distance
Just over half of the participants (19; 56%) reported that they walk less than 200 steps, and most (24; 70%) could not walk more than 500 steps without resting (Figure 3). Further analysis showed that those who received prosthetic rehabilitation could walk significantly longer distances than those who did not receive prosthetic rehabilitation (p = 0.000).
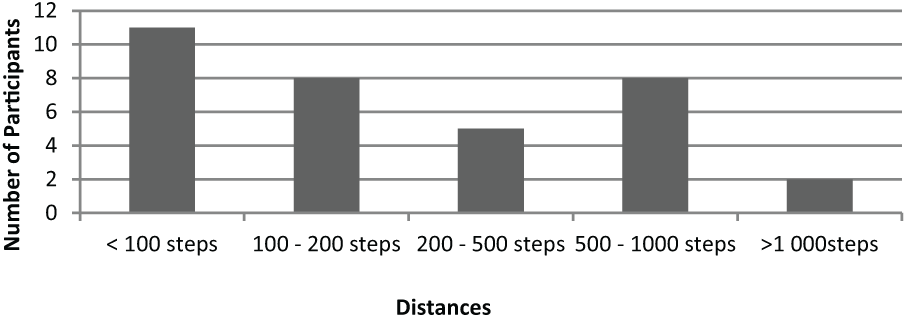
Self-reported walking distances with the prosthesis without stopping to rest.
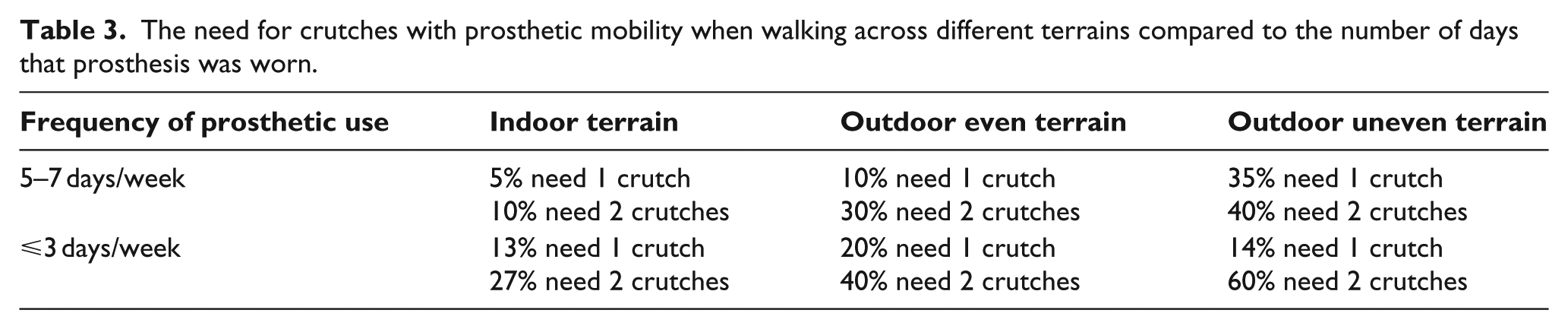
Use of elbow crutches with the prosthesis during walking
Table 3 shows that as the demands of the terrain increased, more participants used one or two crutches. Participants who used their prosthesis more frequently reported less dependency on two crutches.
The need for crutches with prosthetic mobility when walking across different terrains compared to the number of days that prosthesis was worn.
Discussion
Current participants were referred for prosthesis after being assessed by the Guidelines for Screening of Prosthetic Candidates tool. Even so they experienced challenges with prosthetic use and mobility. Prosthetic use frequency in this study was less than in developed countries among participants with similar characteristics,14,16,33 and overall self-reported walking distances with the prosthesis were also limited. These challenges might be related to not receiving prosthetic rehabilitation, the long time lapse between amputation and prosthesis, or other factors such as the prosthetic components used. However, one must also consider the validity of the tool within these constraints.
A concern to service provision is that only 40% of participants received prosthetic rehabilitation. Current and previous findings showed that prosthetic rehabilitation has a significant impact on prosthetic function distances. 34 However, the current findings agree with other South African studies that reported a lack of rehabilitation postamputation. 25 The importance of rehabilitation is underscored in the reasons that participants gave for not using their prosthesis.
The time lapse between amputation and receiving the prostheses is also concerning as previous studies34,35 demonstrated that the less time lost, the more positive the impact on prosthetic use and mobility. Participants in the study by Pezzin et al. 35 waited on average 165 days for their prosthesis where current study participants waited more than a year in 58% of cases.
Overall self-reported walking distances with the prosthesis were limited. While walking distance or steps taken per day were not assessed, one can deduct from the frequent need to rest that most participants probably experienced functional walking limitations. This is in accordance with findings from other studies18,23 and a review of the literature that explored physical activity of persons with lower limb amputations. 11
Prosthetic mobility was challenged when participants walked outdoors and on uneven terrain, as can be expected due to greater demands on balance and endurance. Therefore, the need for crutches increased. Current and previous findings showed that people who used their prosthesis more often tended to be less reliant on hand-held assisted devices.16,33
The limitations of the prosthetic components that were provided could also have played a role in the lower use figures and limited mobility. All participants received basic prosthetic components, with the aim to assist the masses, as opposed to addressing individual mobility needs. This is the dilemma of using cheaper durable prosthetic components in low- and middle-income countries. While longer lasting, these components are basic and essentially allow for indoor mobility at slower speeds. People, reliant on public health care services in the Western Cape, often need to walk long distances outdoor and often over uneven terrain to access services. Thus, they require a higher level of responsiveness from their prostheses, than what basic components can offer.17,18 They might especially hamper function of younger people and people in manual occupation. They might then choose not to use the prosthesis as elbow crutches will allow them to ‘walk’ faster and be more agile than a prosthesis manufactured with basic components.
Most people in the Western Cape Province have access to a telephone 28 so the manner of contacting potential participants through telephonic calls should not have caused bias. Other South African studies, however, have also shown loss of potential study participants when accessing health care records that are not updated. 17 The medical records show that the mean age of those who could not be traced was 10 years younger than that of study participants while the ethnic backgrounds of the two groups were similar. Thus, one should be able to generalise the results to the study population while remaining aware of these limitations.
Limitations of study
The questionnaire was administered telephonically. This excluded people who had changed contact numbers since last capture in hospital records. The questionnaire collects data on self-reported physical capabilities, including walking distance before needing to rest. This may result in over scoring or underscoring, influencing the study’s internal validity or reliability of results. Research has shown that people often do not report activity levels and walking distances accurately. 8 Furthermore, the adapted and translated versions of the PPA were not tested for validity and reliability. Interrater bias could have occurred between the research assistants. The first author listened to the recorded interviews to assess if trends occurred that might have led to interrater bias. No such challenges were identified. This procedure was not performed with the isiXhosa interviews as the author was not fluent in isiXhosa. Caution needs to be exercised in generalising results as the study participants do not represent all Western Cape persons who have received a transfemoral prosthesis.
Recommendations for future work
The provision of a prosthesis is but one aspect in functional prosthetic mobility. In less-resourced settings, prosthetic candidates may have to be carefully selected and optimal prosthetic components considered for the environment. The authors advise that the waiting time to rehabilitation and prosthetic services are minimised and that prosthetic provision is supported by prosthetic rehabilitation. In South Africa, especially in more urban settings such as the current study setting, all of these requirements can be met as the services are available. Research to explore factors that might influence the time delay between amputation date and prosthetic prescription date is recommended. Research that compares the impact of different prosthetic components on prosthetic mobility and use in less resourced settings will provide valuable evidence on which to base prescription of prosthetic components.
Conclusion
This study highlights the conundrum of prolonged time lapse between amputation and prosthesis, prosthetic components, and the lack of rehabilitation and how that could impact prosthetic use and mobility in less-resourced settings even with careful selection of prosthetic candidates. Most of the participants managed indoor prosthetic mobility without the need of crutches, but not being able to walk 500 steps or more without resting and being mostly dependent on crutches outdoor will challenge community mobility and subsequent integration into community activities.
Footnotes
Acknowledgements
The authors are indebted to the participants of this study, and acknowledge the contribution of the research assistants, and the staff at the Orthotic and Prosthetic Centre.
Author contribution
E.P. conceptualised the research, and collected and analysed the data. S.V. provided conceptual input into the research. All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The first author is a service provider in the Western Cape metro and has had contact in that capacity with some participants. Therefore, she did not do the data collection.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.