
Abstract
The past 40 years has seen the field of orthotics change from a craft-based industry into a modern clinical specialty. The author describes his personal view of some of the most important developments during this period in the areas of manufacturing and materials, patient/orthosis matching, biomechanics, joint design and standards. Some likely areas of future development are suggested.
Introduction
The author has enjoyed a professional career extending over almost 40 years, which has seen the field of orthotics transformed from a traditional craft-based industry into a modern professional clinical specialty. This paper represents a personal view of some of the most important elements of this process. It refers primarily to lower limb orthotics, however many of the subjects discussed apply to the field of orthotics generally.
The plastic revolution
The modern era of lower limb orthotics can reasonably be considered as having begun during the early 1970s. Prior to then the design and construction of lower limb orthoses had not changed substantially since the beginning of the century. Orthoses, in general, were assembled from metal components – some prefabricated some customized – with their body contact areas padded with felt and covered in leather by skilled craftsmen. The only significant change in practise in recent years had been the introduction of thermo-setting resins to produce plastic shells as, for example, in the PTB Brace (McIllmurray & Greenbaum 1958) and the UCLA Long Leg Brace (Scott 1971) both of which designs owed more than their material features to the rapidly developing field of prosthetics. The pioneering developments of Engen (1971) in Houston, and Lehneis et al. (1972) in New York, both of whom had recognized the enormous potential and opportunities for the use of thermoplastic materials in orthotic construction, can justifiably be described as revolutionary. During this first phase of innovative activity a variety of materials were employed, including polyethylene, PVC, ABS and polycarbonate, however it was polypropylene which quickly emerged as most versatile and most easily applied within the comparatively unsophisticated environment of a typical orthotic workshop. In the UK a comparatively unknown General Practitioner, after visiting Houston, published a brief article describing the use of polypropylene to fabricate below-knee braces for children with spina bifida and suddenly every parent was clamouring for ‘plastic braces’ for their child (Yates 1968).
During the years since that dramatic and exciting innovative phase, the methods of application and the uses of plastic have continued to evolve. Today, the majority of not only lower limb orthoses, but also upper limb and spinal orthoses are constructed using thermoplastic materials in their construction. Orthotists and technicians have learned how to vary the trim-lines, contour and cross-section of components and to use inserts to alter and control their mechanical properties and hence the functions they will provide. Some efforts have been made to design plastic joints, mostly unsuccessfully; hence even today most jointed orthoses which employ plastic interface components still use metal joints. The subject of the design and function of orthotic joints will be discussed later.
Patient/orthosis matching
One of the consequences of the sudden emergence of a whole new range of orthotic designs was to highlight the very poor quality of the existing guidance on orthotic prescription. The jargon phrase to describe this process was ‘patient/orthosis matching’. Virtually all the orthotic manuals and text books available (and there were precious few) tended to classify patients by reference to their medical diagnosis and routinely used terms such as ‘drop foot brace’ or ‘hemiplegic brace’ to describe both the devices and their clinical applications. These practises had many pitfalls and clearly a more logical approach to the description of both the orthosis user and their device was required if the goal of matching them was to be realized.
The orthosis user
The key to the evolution of the first of these objectives – a method for the description of the potential user of an orthotic device and their orthotic needs – was provided by Jacqueline Perry (1975). Perry described a model of normal physical activity and identified the body tissues and systems which contributed to each element of it. Using this model as a basis she then proceeded to propose a classification of ‘functional loss’ which completely eliminated the need for diagnostic labels to describe the disorder needing treatment.
A standard procedure for the systematic identification, description and recording of each patient's individual functional losses – the assessment process – already existed in the elegant set of forms developed by the American Academy of Orthopaedic Surgeons (McCullough 1970).
Orthotics was beginning to emerge as a modern clinical specialty and with this came the realisation that the supply of an orthosis was just the first element of an on-going process of patient care. Patients need to be reviewed to establish whether the prescription is achieving the desired effect. Patients change and as a consequence so do their needs. Orthoses deteriorate and require repair or replacement. Detailed records of all these changes, and the actions instituted, need to be maintained. Orthotists were now engaged in an ‘orthotic supply process’ rather than just making and fitting orthoses. Standards were laid down for the conduct of each part of the process defining precisely what should happen; who is responsible; and, where appropriate, the time scale for it to occur.
Interest in the description of the patient, or as it now more fashionable to say ‘the user’, waned over the ensuing two decades. It was not until 2003 that the Prosthetics and Orthotics Technical Committee of the International Standards Organization (ISO) devised and published a standard (ISO 2003) which formalized the original ‘Perry/AAOS’ approach and then proceeded to propose both the methods and the terminology to describe what are termed:
The clinical objectives of the supply of an orthosis; The functional requirements of an orthosis to achieve the clinical objectives.
The orthosis
Progress in the definition and description of the orthosis (the other half of the matching process) the prescription, was also slow. A first important step, attributable to the Committee for Prosthetic Research and Development in Washington and its far-sighted Director ‘Ben’ Wilson was the promotion of a classification of orthoses by reference to the body segments and joints which they encompass (Harris 1973). Such was the international popularity of this system that it was adopted by ISO as an international standard in 1989 (ISO 1989). Unfortunately this system tells us nothing about ‘the effect’ or ‘function’ of the orthosis. That required an understanding of orthotic biomechanics which was yet to emerge.
Orthotic biomechanics
The ‘direct’ effect of orthoses
It had always been appreciated by most people associated with the field of orthotics that the function of an orthosis was primarily dependent on the materials and components from which it was constructed and the manner in which the components were assembled and fitted to the user. Most of these individuals were also be aware that when a user donned his or her orthosis and engaged in some form of physical activity that this resulted in the generation of forces at the areas of contact between the orthosis and the user – the pads, bands and brims. Very few however, if any, of these individuals had a comprehensive understanding of the scientific principles governing the relationship between the mechanical properties of a particular design and the forces it was capable of creating. More importantly there was an almost total lack of understanding of how to optimise the design of an orthosis and to adjust it once fitted in order to achieve the most efficient and effective outcome for the user. Faced with this situation medical prescribers and orthotists were obliged to rely on trial and error (and clinical experience) when prescribing and fitting devices.
This absence of what might be termed a set of biomechanical principles of orthotic design and function was the most significant obstacle to the further advancement of the clinical practise orthotics. Fortunately, commencing in the late 1970s there was an upsurge in interest in the theoretical analysis of the contact forces between orthoses and their users. Using the free body analysis technique and applying Newton's Laws of Motion, it was possible to identify the optimal configuration of forces required to achieve a particular function. Referred to in the earlier literature, inaccurately, as ‘the 3 point force systems’, these have more recently been described as the ‘direct or internal force systems’. Significant publications on this topic include Lehmann and Warren (1976) and Condie and Meadows (1977). As a consequence of this knowledge the importance of utilizing the optimal lever arms, the desirability of distributing contact forces as widely as practicable and the need to pre-load soft tissues in order to minimize ‘lost motion’ soon became widely accepted and practised. Used in conjunction with the new widely available plastic technology, sophisticated cast rectification and device trimming practises quickly emerged.
The ‘indirect’ effect of orthoses
Most experienced orthotic practitioners were aware that orthoses could also exert biomechanical influence on the function of joints which they do not actually encompass. Saltiel (1969) and Glancy and Lindseth (1972) had both described the use of a below-knee brace to compensate for weakness of the knee extensors. Lehmann (1971) at the University of Washington had published the results of a biomechanical study of this orthotic application which demonstrated the importance of correctly setting the angle at which dorsiflexion is stopped to achieve the desired functional outcome. The implications of what was being referred to as the ‘ground reaction’ or ‘floor reaction’ effect for the design and application of lower limb orthoses was however largely unrecognized.
It was not until Meadows published his PhD Thesis on the influence of ankle-foot orthoses on the gait of children with CP, (Meadows 1984) that the full significance of this effect of orthoses was scientifically demonstrated. Biomechanical data obtained from a computerised gait analysis system revealed how, using AFOs with appropriate mechanical characteristics, both the point of application and the line of action of the ground reaction vector, throughout the gait cycle, could be modified or controlled with consequent improvements in the gait pattern attained generally. For example not only did these orthoses reduce any tendency to hyperextend the knee during mid-stance (Figure 1a), but also by encouraging hip extension, the orthoses enabled the user to generate more normal push-off forces (Figure 1b).
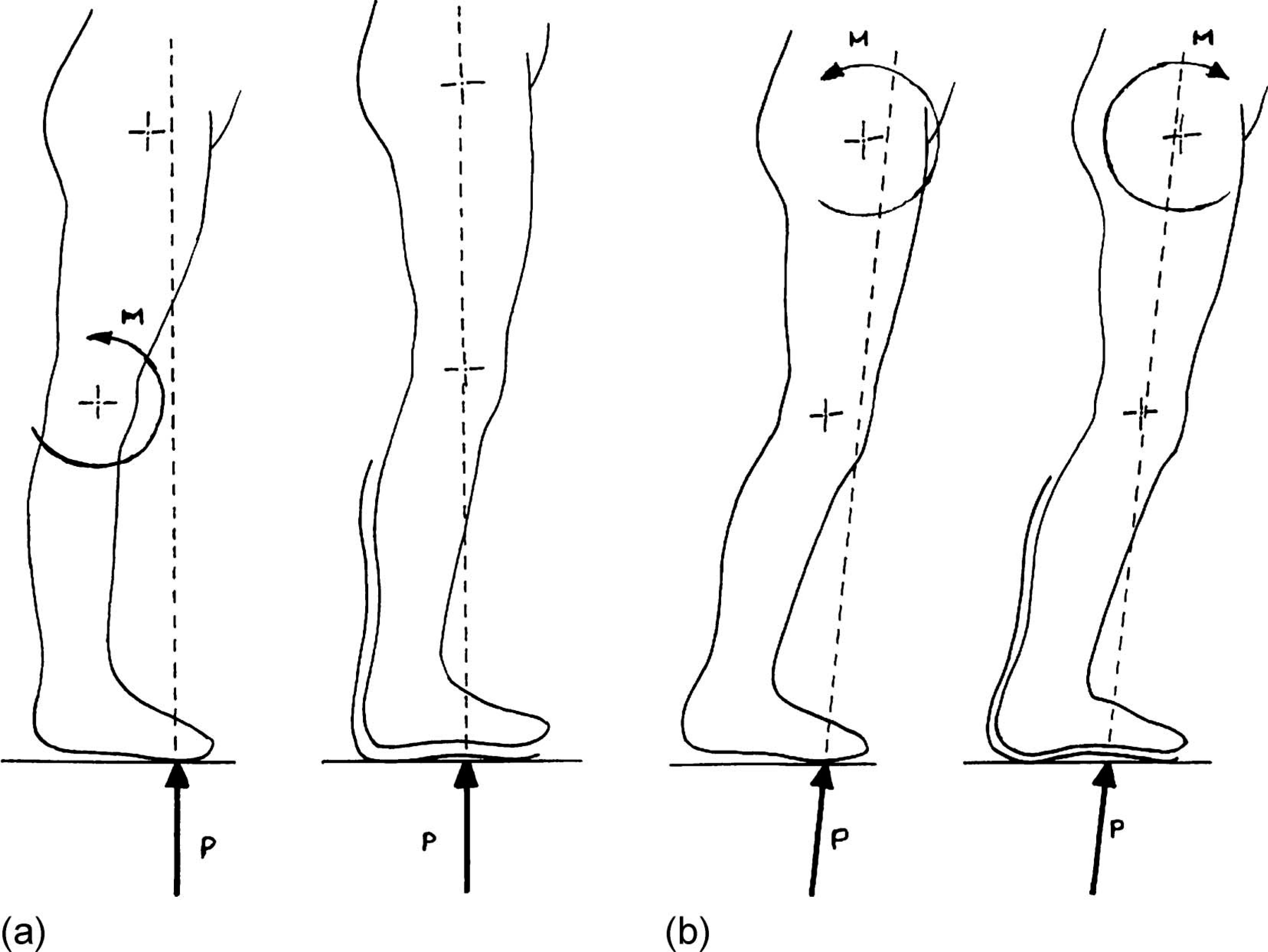
Influence of AFOs on the gait of children with CP. a) Knee biomechanics, b) hip biomechanics.
Just as with the earlier theoretical analyses of the direct biomechanical effects of orthoses this study also focussed attention on how to optimize the ‘ground reaction effect’ by adjusting the ankle angle at which the user was cast or by using various designs of footwear adaptation. Suddenly practitioners became aware that they had been using this effect in a whole range of orthotic applications ranging from simple shoe adaptations to control an unstable subtalar joint, through KAFOs employing offset knee joints all the way up to more complex designs of HKAFO used by paraplegic patients. Since the terms ground reaction and floor reaction had become synonymous with the original Saltiel/Glancy applications most authors have instead decided to use the terms ‘indirect’ or ‘internal’ when referring to this effect of orthoses.
Body assisted orthotic function
During the period of investigation and innovation being described several designs of orthoses emerged which attempted to use the power of an unimpaired joint or limb to complement the biomechanical properties of an orthosis. Probably the first example of this was the CARS-UBC Varus/Valgus knee orthosis (later renamed the Telescopic Varus/Valgus Support [TVS]) intended to be used to treat medio-lateral knee instability. This device incorporated a number of innovative design features including a novel knee strap or apron which uses the normal knee extension moment generated from initial foot contact until mid-stance to generate an abduction or adduction moment. Another design of knee orthosis marketed (briefly) by Donjoy for anterior cruciate laxity, used a unique knee joint design which converted the normal stance phase knee extension moment into a posteriorly directed force which was applied to the wearer through an anterior band positioned just below the joint.
Perhaps the most ingenious use of this concept is in the modern generation of HKAFOs designed initially for use by paraplegic children and subsequently used by some adults. The first example of this group of HKAFOs, which enabled this category of patients to achieve a reciprocal gait pattern, appeared as early as 1971 (Motloch 1971). To be followed by a number of increasingly sophisticated variants including the Hip Guidance Orthosis (HGO), (Rose 1979), the Reciprocating Gait Orthosis (RGO), (Douglas et al. 1983) and the Isocentric Orthosis. Certainly at the time of their first appearance the biomechanical explanation for the remarkable function which they bestowed on their users was far from clear. By 1981 however, as a consequence of the insights resulting from the previous ten years of scientific study and analysis, the simple elegance of their functional mechanisms were revealed (Major 1981).
All of these designs incorporate locks which hold the knees in full extension – using a system of directly applied forces. The hip joints of the HGO are free within a preset range while those of the RGO and the Isocentric are mechanically linked to one another so that they are obliged to move in a reciprocal manner. These features allow the user to stand freely using a walking aid (usually crutches) to maintain hip extension. But how does a person who has no lower limb muscle power achieve reciprocal gait using such a system? The answer lies in the manner in which the walking aid is used and may be explained by the application of Newton's Laws as follows for just one step (Figure 2).
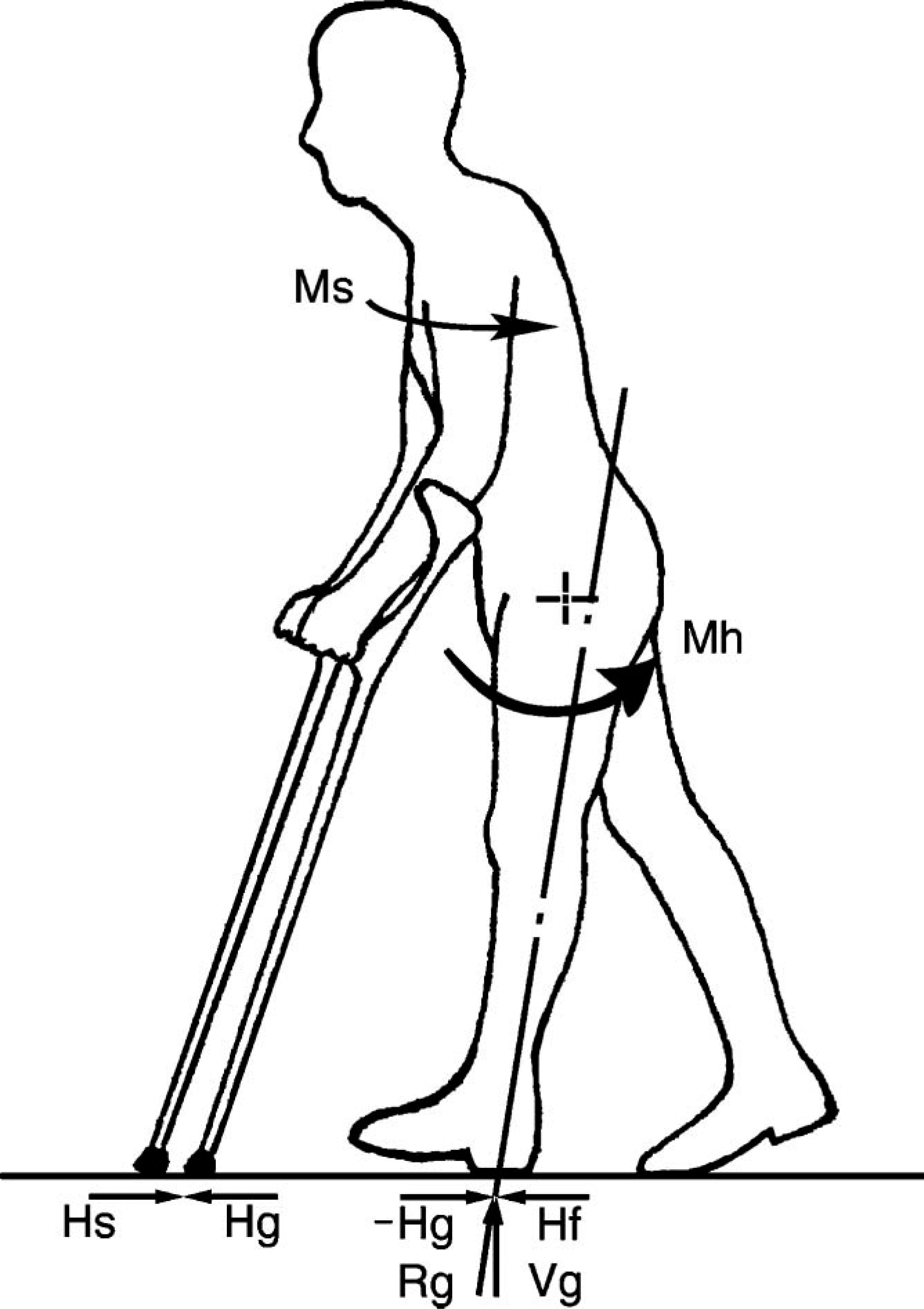
HKAFO biomechanics.
Firstly, the body must be tilted laterally, towards the leading leg to achieve clearance for the trailing leg. This action is achieved using elbow extension to push downwards with the contra lateral walking aid.
Secondly, the ipsilateral shoulder is extended forcefully. This action creates a horizontal posteriorly directed force between the crutch tip and the ground (Hs), which must (according to Newton's 3rd Law) result in an equal but oppositely directed anterior force exerted by the ground on the crutch (Hg). Equilibrium (according to Newton's 1st Law) requires that an identical pair of horizontal forces, −Hg and Hf (=−Hs), are generated between the ground and the leading foot which is already supporting body weight and as consequence is subject to a vertical ground reaction force (Vg). The line of action of the single (resultant) force (Rg) created by adding together −Hg and Vg passes behind the hip joint centre thereby creating an extension moment (Mh, Figure 2). This causes the hip to extend and the user to move forward over the supporting foot.
The function of virtually every ‘mechanical’ lower limb orthosis in use today may be explained either, by the ‘direct’ or ‘indirect’ force systems which they create, with or without the ‘assistance’ of power resulting from the action of an unimpaired joint or limb.
Our understanding of orthotic biomechanics has of course continued to grow. Two notable examples deserve mention here. Sakamoto at the 11th ISPO World Congress in Hong Kong (Sakamoto 2004) presented his preliminary findings from tests performed on patients suffering from muscle weakness using instrumented AFOs which both confirmed and challenged some of the long-standing beliefs regarding the nature of the direct force systems arising during the use of these devices.
Owen (2002) in her publication on the subject of tuning AFO/footwear combinations for children with cerebral palsy drew attention to the vitally important interaction between the cast angle selected for an AFO in order to produce particular direct and indirect effects and the resulting function of the two-joint gastrocnemius at the knee joint.
To date, only one book has been published which attempts to bring together all the known biomechanical theory relating to the function of orthoses (Bowker et al. 1983), this is now out of print. Hopefully the soon to be published 4th Edition of the Atlas of Orthotics and Assistive Devices (Hsu et al. 2008) will fill this vacuum.
Functional electrical stimulation
The categories of orthoses just described do not, of course, include functional electrical stimulators and hybrid orthoses. The first commercially available, and highly successful, FES system was the Ljubliana Functional Electronic Peroneal Brace (Gracinin 1972) and many practitioners predicted that this technology would revolutionise the design of orthotic systems for users whose functional loss was the result of an inability to control the muscles of the locomotor system. To date, the technique has only been applied to paraplegic patients, in isolation, and on a very limited basis with an inconclusive outcome and in conjunction with an orthosis as a hybrid, once again on a very limited basis (McClelland et al. 1987; Andrews et al. 1988). The hybrid HKAFO has been demonstrated to achieve an appreciable reduction in the energy cost of using the mechanical system alone (McClelland et al. 1987; Nene & Patrick 1990). It therefore goes without saying that the expected transformation of the field has to date not occurred.
Orthotic joints
The period under discussion has seen an explosion in the range of joints commercially available to orthotists, stimulated primarily by the demand for components which are compatible with thermoplastic fabrication techniques. In spite of this activity, the functions which they offer has continued to be confined to joints which allow free motion, joints which limit the range of motion permissible, joints which prevent all motion and joints which assist and/or resist motion. Furthermore, the vast majority of the joints which are in common use today may be described as ‘passive’, that is to say their biomechanical properties are set at the time of manufacture and fitting and do not vary thereafter. In contrast clinical experience suggests that there are many instances where an ‘active’ design of joint/orthosis would allow more effective treatment. The popular term used to describe such a design is ‘intelligent’, meaning that although its properties are still set at the time of manufacture they are capable of varying to suit the demands of the user and the activity being performed. It should be noted that the use of the term ‘dynamic’ to describe this capability is inappropriate since this adjective simply means ‘moving’.
The best known area of application of this concept are the so-called ‘stance control orthoses’ (SCOs) designed for use by patients with severe quadriceps weakness, which provide knee stability when loaded by body weight but which flex freely when unloaded as is the case during the swing phase of walking (Travolta 2002). The challenge of providing these conflicting functions has absorbed orthotic designers for many years. One of the earliest experimental designs of this type was the Rensberg Orthosis from Sweden and more recent examples include the UTX Swing from the Netherlands (Van Leerdam 1993) and the E-Knee developed by Becher Orthopedic in the USA. It would appear highly likely that with the ready availability of the microelectronic componentry ideally suited for their control systems that more examples of active or intelligent orthoses will reach the market before long.
Consensus conferences
It is ironic that virtually the first step taken in the development of a systematic, scientifically based process of patient/orthosis matching was the introduction of a system for describing the patient which consciously avoided reference to the pathology which presented. As experience in the assessment of potential users and the prescription of orthoses based on biomechanical principles has grown it has become apparent that on many occasions the conduct of this process specifically requires the consideration of a number of diagnostically related factors. For example; when dealing with developmental disorders the stage or phase of the disorder is clearly relevant. When dealing with disorders which are progressive or are characterised by flare-ups and remissions, the history and the current status of the disorder must be considered. In addition, where the potential user is currently receiving other treatment this will often have implications for the type orthotic treatment they might most appropriately receive.
So how has the field of orthotics attempted to collate and make generally available existing knowledge regarding these issues? The approach adopted and sponsored by ISPO has been to organize Consensus Conferences: Firstly on the topic of ‘The Orthotic Management of Cerebral Palsy’ (ISPO 1995), secondly on ‘The Management of Poliomyelitis’ (Jacobs 2001) and most recently on ‘The Orthotic Management of Stroke Patients’ (ISPO 2004). Expressed rather simply, these events bring together a carefully selected group of experts who are then required to review all the published evidence of the outcomes of the various treatments, including orthotics, (provided to the patient group under consideration) and agree upon recommendations regarding which treatments should be provided to which patients and at what times.
The American Academy of Orthotics and Prosthetics recently convened a State of the Art Workshop on the topic of KAFO and HKAFO applications with similar objectives (AAOP 2006).
An alternative method of arriving at a consensus regarding these matters which depends more on clinical experience rather than published evidence has been piloted by clinicians in the Netherlands (Hijmans & Geertzen 2006). It seems likely that with the high demand for clinical guidelines for the use of orthoses that this type of activity will become increasingly popular. Indeed ISPO has recently decided to convene a further conference to update the findings of their 1995 cerebral palsy conference (ISPO 1995).
Standards
Mention has been made on more than one occasion in this discussion to the subject of standards. Firstly, referring to the adoption of the CPRD system of acronyms to categorize orthoses in ISO 8549, and later when referring to ISO8551 which specifies a method and terminology for describing the user, the clinical objectives are of treatment and the functional requirements of an orthosis to achieve them.
The family of ISO orthotic terminology standards has recently been completed (for the present) by the publication of ISO 13404 which extends the scope of ISO 8549 by providing terminology for the description of the function of orthoses (which is compatible with ISO 8551) and to describe the components from which they are assembled (ISO 2007) (Figure 3).
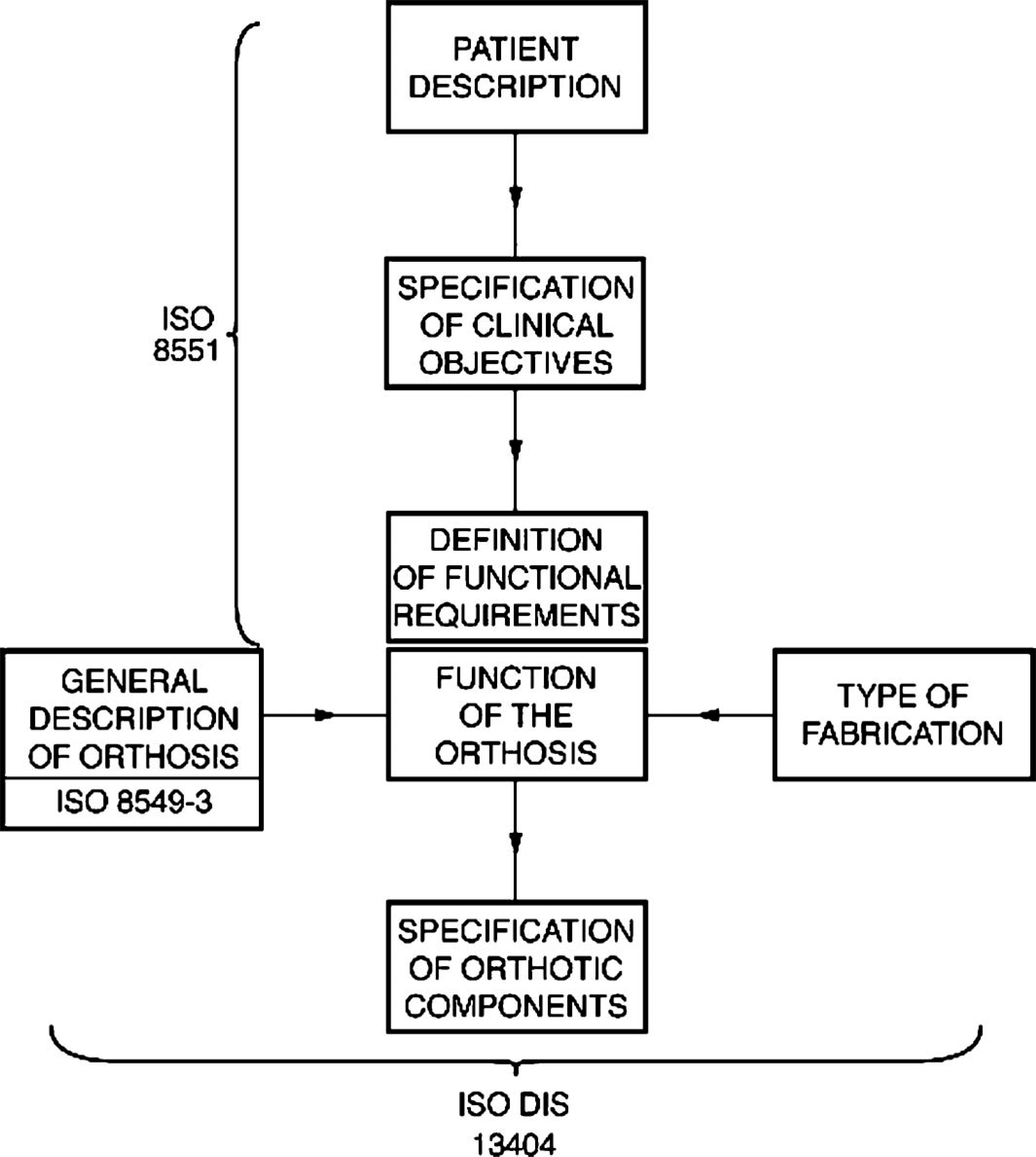
The current ‘family' of ISO orthotic terminology standards.
The future
It is possibly unnecessary to state that many of the developments referred to in this discussion would not have significantly changed clinical practise were it not for highly significant parallel advances in the training and education of both orthotic practitioners and the other members of the clinic team that have been achieved over the same period.
There is little doubt that the chemists and material scientists will continue to produce ever more convenient materials and manufacturing processes which will make the orthotists' task easier and more consistent. Designers equipped with these materials and the latest technology will inevitably continue to present clinicians with more ingenious and sophisticated devices.
The consensus and state of the art activities referred to earlier have all made valuable scientific contributions, however without doubt however the most important future challenge for the specialty of orthotics is to continue to assemble a body of scientific evidence of the biomechanical effects of orthoses and outcomes of their clinical application. The reasons why this is the case hardly need statement. The field of medicine generally has long accepted the need to measure the effects of treatment and thus provide justification for its implementation. Our sister field of prosthetics has fully embraced this philosophy. The individuals and organizations who pay for orthotic treatment whether government health services or private insurers, are demanding proof that their money is being spent in a worthwhile manner. Finally and perhaps most importantly, it is absolutely vital for the future development of the field that we learn both why and how effective our treatments are.