
Abstract
Background:
Few studies have examined the efficacy of trunk orthoses that support the upper trunk and a paretic limb in stroke patients. To improve stability and alignment of the trunk and pelvis in hemiparetic patients, we developed a newly designed trunk orthosis that provides resistive force through spring joints.
Objectives:
This study aimed to determine the newly designed trunk orthosis’s biomechanical effects during level walking.
Study design:
Before-after trials must be better.
Methods:
Measurements were taken for nine chronic-phase (>2 years post-onset) stroke patients using a three-dimensional motion capture system and force plates under three experimental conditions: self-selected gait speed without the newly designed trunk orthosis, with the newly designed trunk orthosis, and after newly designed trunk orthosis removal. We analyzed and compared spatiotemporal and kinetic parameters of the paretic and non-paretic limbs and kinematic parameters of the trunk and bilateral limbs.
Results:
Several pre-swing gait parameters (e.g. hip joint flexion moment and ankle joint plantar flexion angle) after newly designed trunk orthosis removal were significantly increased compared to those without newly designed trunk orthosis. Step length of the paretic limb tended to increase after newly designed trunk orthosis removal.
Conclusion:
The newly designed trunk orthosis effectively modified trunk alignment, but larger improvements in kinetic and kinematic parameters were observed in the bilateral limbs after newly designed trunk orthosis removal than with the newly designed trunk orthosis.
Clinical relevance
Stroke patients improved only trunk malalignment while wearing the newly designed trunk orthosis. Gait after newly designed trunk orthosis removal was better than with the newly designed trunk orthosis. Positive changes after removal were mostly observed in pre-swing of the hemiparetic limb. The newly designed trunk orthosis might be effective for gait training in stroke patients.
Background
Stroke is a major cause of disability in all industrialized countries. Stroke survivors are often left with persistent neurologic deficits. 1 Hemiplegia is one of the most common impairments after stroke and contributes significantly to reduced gait performance. 2 Although the majority of stroke patients achieve an independent gait, many do not reach a level of walking that enables them to perform all their daily activities. 3 Gait performance in persons with stroke is typically characterized by spatiotemporal asymmetry between sides, decreased walking speed, and problems with trunk–limb, interlimb, and intralimb coordination.4–6 Gait recovery is a major objective in the rehabilitation program for stroke patients. For many decades, hemiparetic gait has been studied and methods for the development of gait analysis and rehabilitation have been developed. 7
Several types of gait training focusing on rehabilitation of the paretic limb in persons with stroke can improve gait performance. In addition, orthoses for paretic lower limbs—ankle–foot orthoses (AFO) and knee–ankle–foot orthoses (KAFO)—are often prescribed and enhance the effects of gait training. A previous study reported that stroke patients showed a persistent decrease not only in functions of the paretic lower limb but also in the level of trunk performance compared with age- and sex-matched healthy individuals, even in the non-acute and chronic phase after stroke. 8 Verheyden et al. 9 reported that trunk performance, as measured by the Trunk Impairment Scale and Trunk Control Test, contributed to gait performance. Hence, some exercise therapies are often applied to improve or maintain the function of trunk muscles in stroke patients. However, orthoses to assist and enhance trunk stability are rarely prescribed for gait training in stroke patients, and therefore, very few studies have reported the effects of orthoses on improving gait performance in these patients. Maguire et al. 10 showed an immediate effect of a corset with elasticated strapping to guide the hip joints on increasing hemiplegic hip abductor activity. Thijssen et al. 11 reported an immediate effect and an effect after 3 weeks of familiarization with a corset with elastic straps to guide the major joints of the affected limb (i.e. the hip, knee, or ankle) on the energy cost and spatiotemporal parameters of level walking. Although these studies showed improved gait performance, the corsets they used would have affected the functions of both the paralyzed trunk and lower limb. To our knowledge, no previous studies have reported significant effects of wearing a trunk orthosis without a brace or straps on paretic lower limb control during level walking in stroke patients.
In light of these limitations, we developed a newly designed trunk orthosis (NDO) with joints providing resistive force (Figure 1). The NDO was designed to improve trunk and pelvis stability and alignment by providing resistive force through the use of joints stabilized with springs. The resistive force produces a resistive moment to rotate the trunk backward and the pelvis forward, and the moments are controlled by adjustable screws. The NDO can thus effectively modify malalignment in stroke patients. Therefore, the purpose of this study was to examine, through biomechanical analysis, the effect of the NDO on the gait of stroke patients. We hypothesized that this NDO would effectively modify trunk malalignment and thus improve the kinetic and kinematic parameters of the lower extremities in stroke patients during level walking.
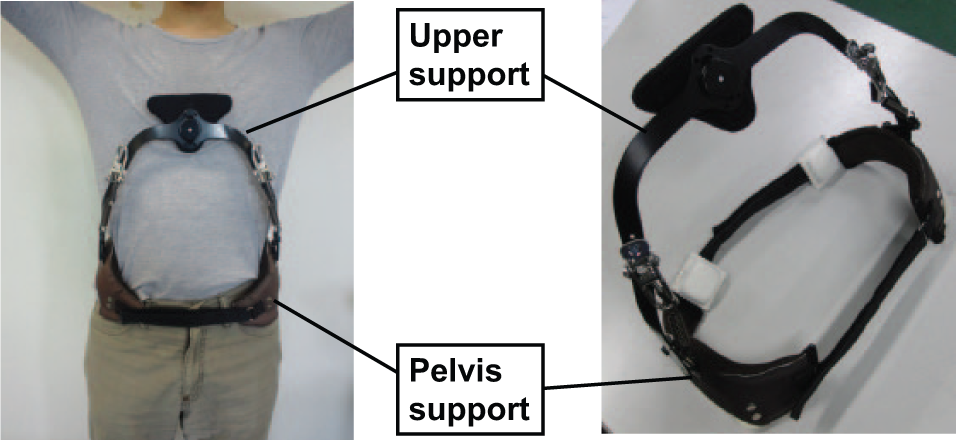
Appearance of the newly designed trunk orthosis.
Methods
Features of the NDO
A pelvic and upper support is positioned on the ilium and sternum, respectively, and joints are connected to an upper support made of stainless steel with a nylon pad and a pelvic support (Figure 1). The joints produce resistant force by extension springs (Figure 2), and a link mechanism translates spring-generated tension into resistive force on the chest. The NDO range of motion is 40°. While wearing the NDO, the upper support initially inclines backward to provide resistive force on the chest. The NDO has release mechanics using tension levers, with resistant force released by pulling tension levers downward. Adjustment screws control the magnitude of spring-generated resistive force.
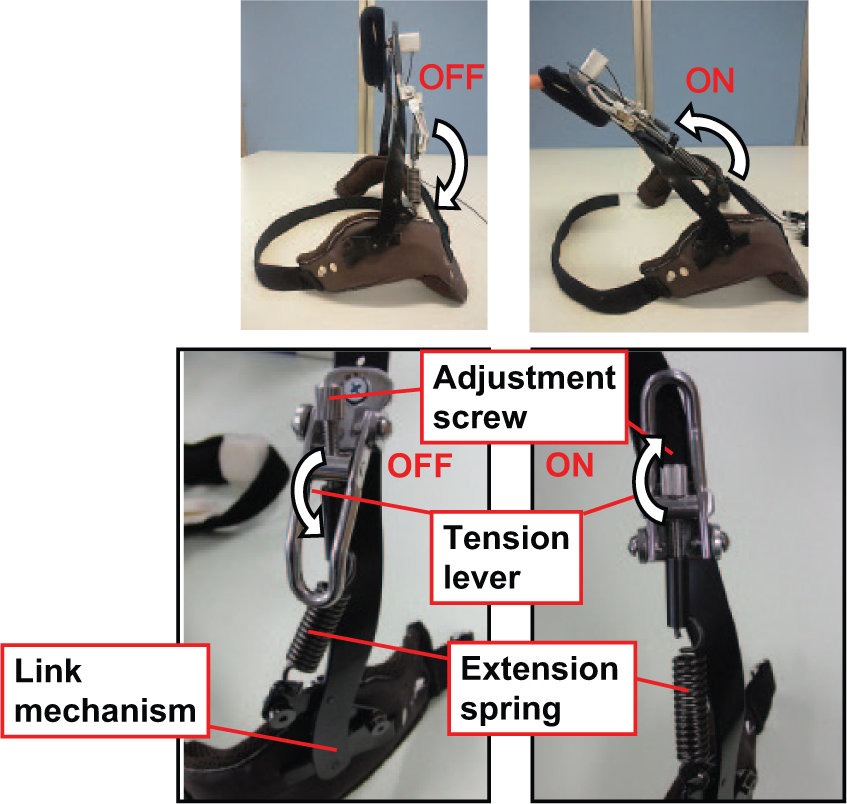
Details of functions of the newly designed trunk orthosis.
Figure 3 shows the functions of the NDO. The compositional center of gravity (COG) of the head, arm, and trunk (HAT) positions is at about mid chest level and a gravitational force vector passes somewhat forward of the low back joint (see L4/5 joint in Figure 3). A trunk extension moment is needed to maintain an upright position. The NDO can produce resistive force by means of the joints on the chest. The resultant force vector is composed of both gravitational and resistive forces to incline the trunk backward. Accordingly, wearing the NDO decreases the low back extension moment and increases the abdominal moment. Resistive force on the chest effectively extends the trunk backward. We previously reported that wearing an NDO prototype could increase abdominal muscle activity and decrease back extensor muscle activity during level walking in healthy young adults. 12
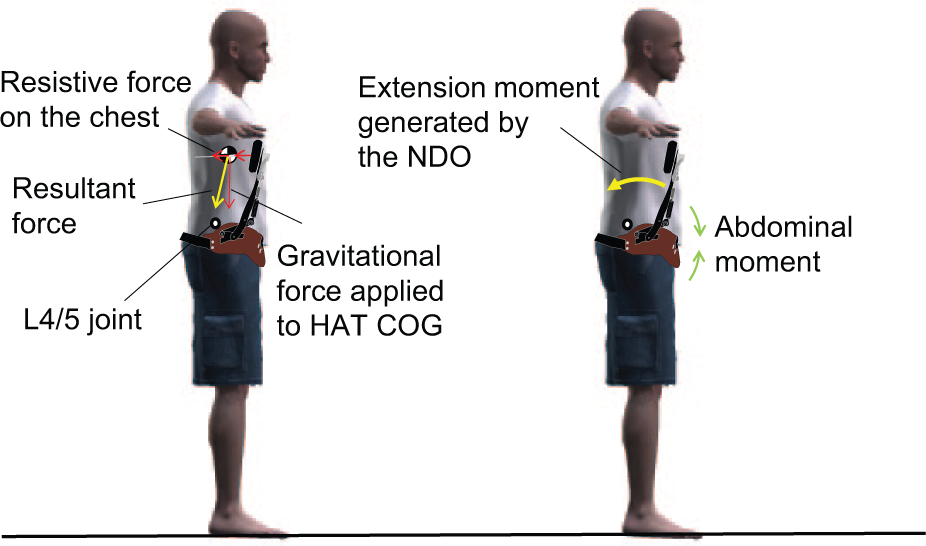
Biomechanical effect of the NDO.
Patients
Participants were nine stroke patients in the chronic phase (>2 years post-onset) who we selected due to the steady state of their gait, because the recovery curve plateaus at approximately 6 months after stroke onset. 13 The inclusion criteria were a diagnosis of hemiparesis and the ability to walk at least 10 m without an AFO. Exclusion criteria were non-concurrent pathologies affecting the central nervous system or neuromuscular system, communication problems, or severe spasticity and proprioceptive sensory impairment. Table 1 shows the participants’ profiles. The institutional ethics committee approved all procedures, which were consistent with the Declaration of Helsinki. We obtained informed consent from all patients prior to their participation in the study.
Patient profiles.
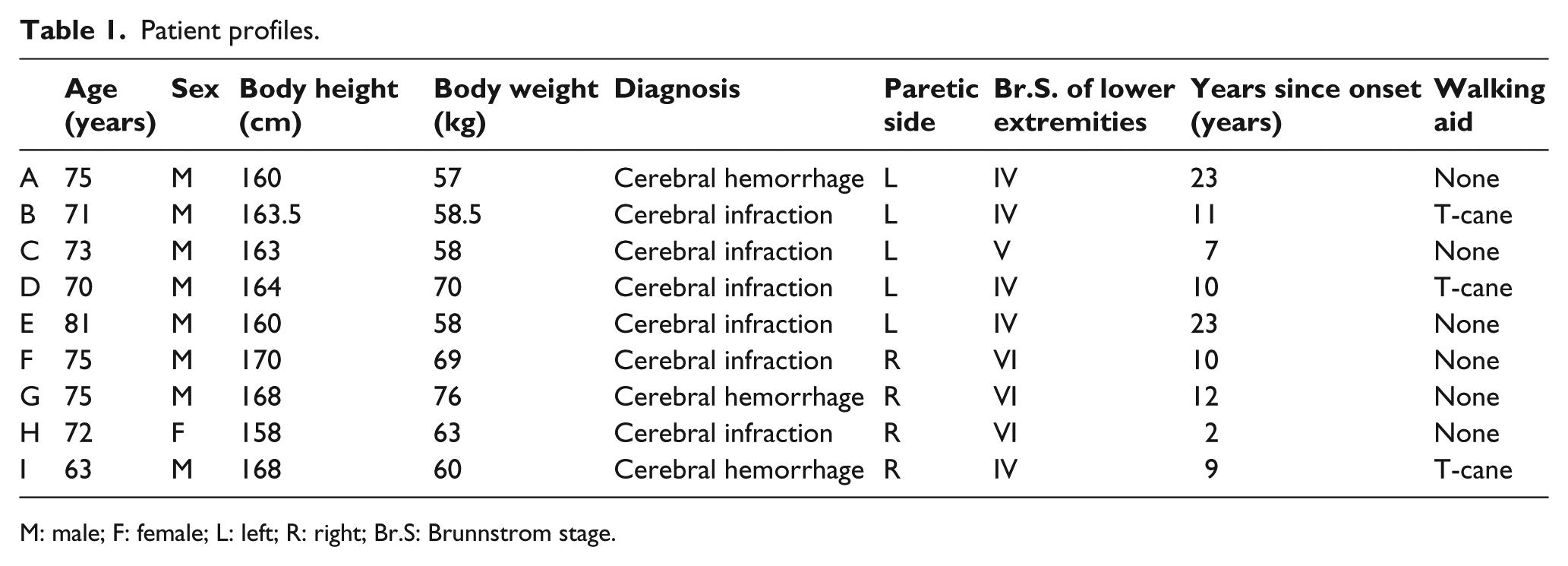
M: male; F: female; L: left; R: right; Br.S: Brunnstrom stage.
Study protocol
We recorded gait data using a three-dimensional (3D) motion capture system consisting of four force plates arranged in two rows of two. The patient stepped onto the right-hand plates with the right foot and the left-hand plates with the left foot. Fifteen reflective markers were attached to the following landmarks: posterior aspect of the iliac spine, bilaterally on the acromion process, trochanter, elbow, wrist, lateral epicondyle of the knee, lateral malleolus, and fifth metatarsophalangeal (MP) joint. We measured the markers’ trajectories and force plate data at a sampling frequency of 100 Hz. During all measurements, patients were barefoot and used canes when needed. First, we measured gait without the NDO at the patient’s selected speed and repeated these measurements three times. Next, after the patient put on the NDO and practiced using it for 10 min, we measured gait with the NDO. Before doing so, we set the resistive force magnitude to 20 N during static standing based on preliminary experiments. We measured tuning of the resistive force with a strain gauge embedded into the NDO’s upper support and transferred the measurement to a personal computer using Bluetooth. After this measurement, the patient removed the NDO and we recorded gait immediately after removal using the same protocol. Consequently, we took measurements for each patient under three conditions: without the NDO, with the NDO, and after NDO removal.
Data processing
We processed the obtained physical coordinates and ground reaction force data with a 6 and 18 Hz low-pass filter, respectively. 14 The link segment model consisted of 11 segments: the trunk including the head, upper arms, forearms, thighs, shanks, and feet. We calculated COG and joint centers using anthropometric data for each segment of the model. We calculated joint kinematics and kinetics based on previous studies using similar marker placements.14,15 This model was developed primarily to analyze kinetics and kinematics in the sagittal plane. From these data, we detected (per gait cycle in each patient under each condition) the spatiotemporal parameters and peak values of joint angles and joint moments in the sagittal plane, and the vertical, anterior, and posterior components of the floor reaction force in the paretic and non-paretic limb that were examined in previous studies.16–19 Body mass normalized joint moments, floor reaction force, and power. We calculated COG sway by subtracting leftward COG displacement from rightward COG displacement. Altogether, we obtained 32 gait kinetic and kinematic parameters for analysis. As analytic values, we extracted the maximum and minimum values of the bilateral kinetic and kinematic parameters at the time of (a) initial contact (IC), (b) loading response (LR), (c) pre-swing (PS), (d) stance, and (e) swing phase. We extracted only the peak values of the forward trunk angle and backward bending angle in one gait cycle of the paretic limb because of the overlap in gait cycle phases for bilateral legs.
Statistical analysis
Gait parameters were determined and averaged for two selected trials out of three measured trials without missing markers under each of the three experimental conditions. To exclude the outlier effect in this small test group, we performed non-parametric statistical analysis. First, we conducted a Friedman analysis to identify any significant differences between the three conditions. When a significant difference was found, we made further comparisons between the without the NDO and with the NDO conditions, and between the without the NDO and after NDO removal conditions. Statistical significance was established at a p-value of 0.05 for the Friedman analysis, and a Wilcoxon signed-rank test with Bonferroni correction was applied to reduce the likelihood of obtaining false-positive results. We used SPSS version 20 for Windows (IBM Corp, Armonk, NY) for all statistical analyses.
Results
Table 2 shows that all spatiotemporal parameters and kinematic and kinetic parameters significantly differed among the three conditions. Friedman analysis showed significant differences in the step length of the paretic limb and in the kinetic and kinematic parameters of the bilateral limb and trunk forward flexion angle during all phases except IC. Significant changes while wearing the NDO were reflected by an increased peak ankle joint plantar flexor moment in LR and decreased minimum values of the non-paretic knee flexion angle in PS and peak flexion moment in LR in the non-paretic limb. The peak trunk forward flexion angle in LR and the stance and swing phases significantly decreased when wearing the NDO.
Mean and SD for gait parameters of three walking conditions (N = 9) and results of statistical analysis.
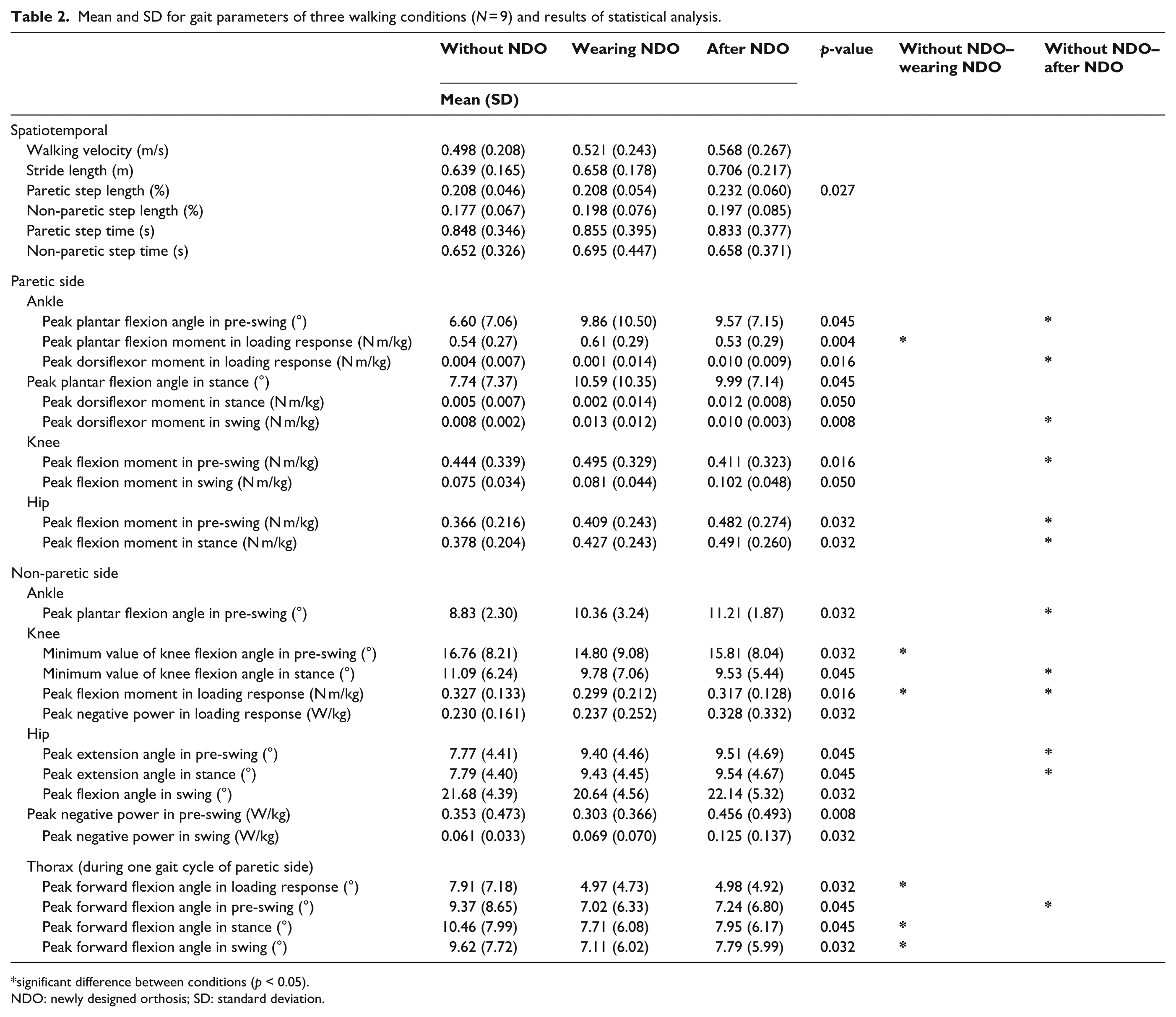
significant difference between conditions (p < 0.05).
NDO: newly designed orthosis; SD: standard deviation.
After NDO removal, we observed further significant changes in kinetic and kinematic parameters not only in the non-paretic limb but also in the paretic limb. Friedman analysis revealed a tendency for significant differences to increase (p = 0.05) after NDO removal in paretic step length among the three conditions. We observed a significant decrease in forward trunk flexion angle only during PS after NDO removal. Regarding the hip and knee joints in the paretic limb, we observed significant increases in the hip joint flexion moment in PS and in stance and a significant decrease in the peak knee joint flexion moment in PS. With regard to the ankle joint in the paretic limb, we observed a significant increase in the peak plantar flexion angle in PS and in the peak dorsiflexor moments in the LR and swing phases. With respect to the non-paretic limb after NDO removal, we observed a significant increase in the peak ankle joint plantar flexion angle in PS and in the peak hip joint extension angle in PS and in stance, as well as a significant decrease in the minimum value of the knee flexion angle in stance and in the peak flexion moment in LR.
Discussion
Effects of wearing the NDO
We hypothesized that the NDO would effectively modify trunk malalignment and thus improve the kinetic and kinematic parameters of the lower extremities in stroke patients during level walking. However, our findings did not support this hypothesis. As expected, trunk alignment during LR and in the stance and swing phases improved the most with the NDO, which produced moments for trunk extension by applying a spring-generated resistive force on the chest (Figure 3). However, wearing the NDO affected only three lower limb kinetic and kinematic parameters. These parameters showed significant differences, although the differences were within only about 1° for the knee flexion angle in paretic PS and 0.01 N m/kg for the peak flexion moment in non-paretic LR. If we consider the biomechanical features of normal gait, 20 an increased ankle plantar flexor moment of the paretic limb in LR would not reflect a positive change in abnormal gait in stroke patients. We previously reported the negative effect of an NDO prototype that restricted pelvis rotation during level walking in healthy young adults. 21 The reasons for the lack of improvement in kinetic and kinematic lower limb parameters when stroke patients wore the NDO in this study might have been due to this restriction of pelvis rotation. Although trunk alignment was effectively modified by wearing the NDO, the restriction of the pelvis rotation, which contributes to increased step length and walking speed, decreased the positive effect of modified trunk alignment. However, as we did not attach reflective markers to the pelvic girdle, we could not investigate the effect of restricted pelvis rotation by the NDO in this study. Further investigation is needed to examine the effect of restricted pelvic movement on abnormal gait in stroke patients.
Improvements after NDO removal
We anticipated that improvements in both alignment and gait parameters while wearing the NDO would disappear after NDO removal. However, we observed many more significant changes in gait parameters immediately after removing the NDO than while wearing it, especially in PS.
Ankle and hip joints contribute to the swing limb in level walking, and ankle plantar flexors contribute to forward propulsion and swing initiation. 4 In PS, the ankle joint plantar flexion moment increases with an increased plantar flexion angle to push the lower limb off the ground. Hip flexors also contribute to the initiation of leg swing.6,22 Experimental studies on hemiparetic walking have indicated several abnormalities during paretic PS.4,23 Nadeau et al. 4 found that weakness in the plantar flexors correlated with gait speed limitations in hemiparetic subjects and suggested that they could compensate for these deficits and achieve faster walking speeds via the paretic hip flexors. Although we found a significant increase in paretic hip flexion moment in PS after NDO removal, the ankle plantar flexion moment did not change. Consequently, the tendency for the paretic step length to increase (p = 0.05) could have been caused by the increase in the hip flexion moment in PS after NDO removal, which in turn would have been caused mainly by the significant decrease in trunk bending angle during the same phase. In addition to the spring-generated resistive force on the chest, the posterior limb generated the forward component of the ground reaction force, which in turn generated an inertial force applied to the upper trunk in PS (Figure 4(a)). Subjects wearing the NDO needed to maintain an upright position to resist the trunk extension moment that was generated by the spring-generated resistive force and the inertial force by exerting the trunk flexion moment. 12
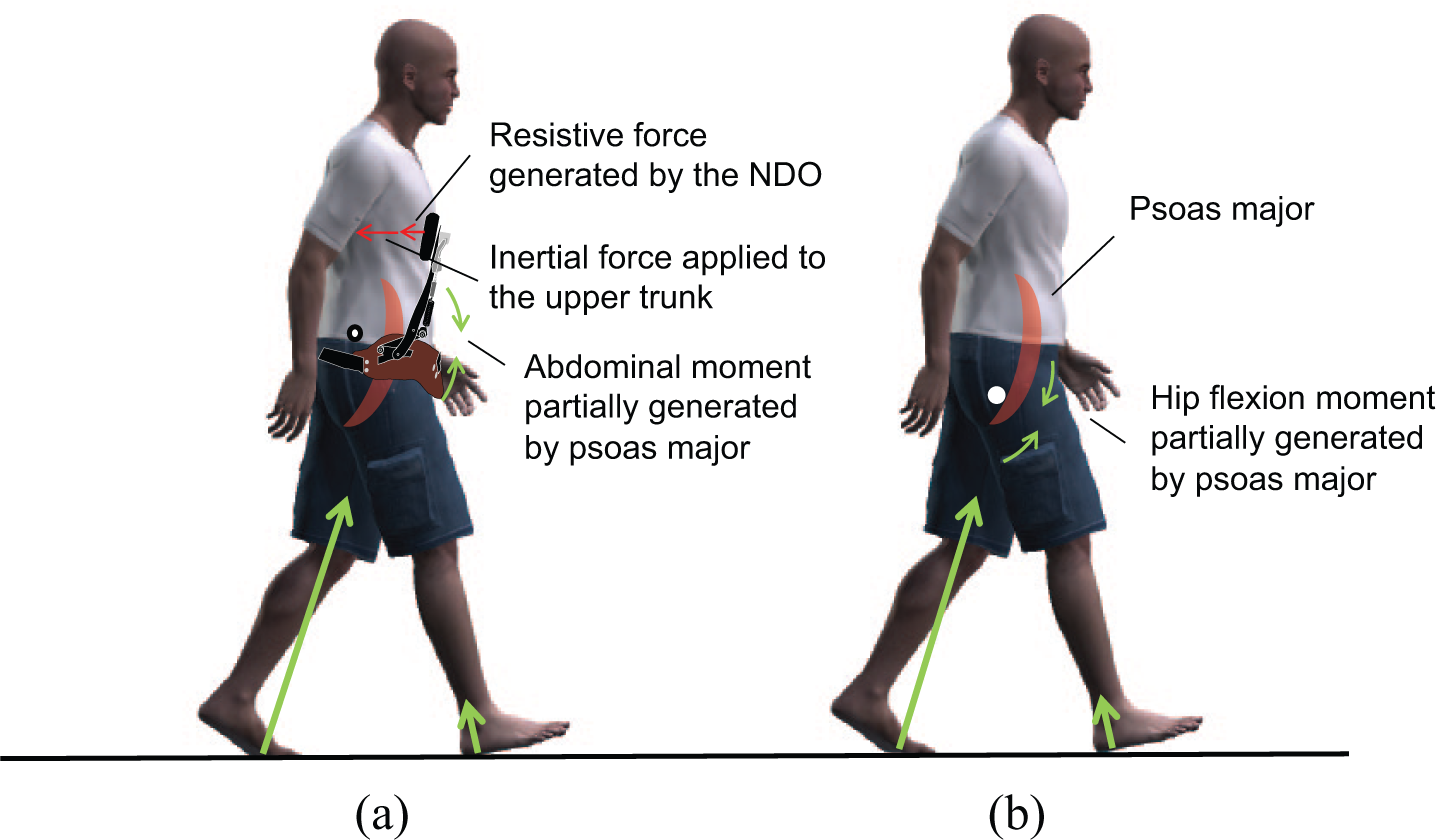
Biomechanical effect of the NDO (a) while wearing it and (b) after its removal in the pre-swing phase.
The abdominal and hip joint flexion moment might include the activity not only of the superficial muscles, but also the deep muscles (i.e. iliopsoas), since the activity of the iliopsoas muscles contributes to generate the hip flexion moment in PS.6,22 Matsubayashi et al. 24 observed increased activity of the psoas major during PS on ultrasonography. The primary action of the psoas major might have been to resist the spring-generated resistive force on the chest to maintain an upright posture while wearing the NDO, and the residual action of the psoas major might have contributed mainly to the increased hip flexion moment and swing limb, which improved the stroke patients’ trunk bending posture and gait in PS (Figure 4(b)). Forced extension of the upper trunk by the NDO might have served as a training effect on the trunk muscles. However, we could not confirm this action while the subjects were wearing the NDO because the inter-segmental forces between the thigh, pelvis, and trunk generated by the psoas major were difficult to analyze.
Moreover, the improved trunk bending posture might have contributed to an increase in ankle plantar flexion angle and a decrease in knee extension moment after NDO removal in PS. Saha et al. 25 examined the effect of trunk bending on the gait of able-bodied subjects and found that the ankle plantar flexion angle significantly decreased while walking with a deliberately increased trunk bending posture compared with walking upright. In our study, a nearly upright posture after NDO removal in PS did not significantly affect the ankle plantar flexion moment, although it might have caused a significant increase in the ankle plantar flexion angle. Kinetically, forward inclination of the trunk positions the COG forward, and the ground reaction force vector readily passes in front of the paretic knee and hip joint. Hence, this posture causes excessive knee extension and an increased knee flexion moment. In this study, the knee flexion moment in PS significantly decreased after NDO removal, suggesting that a decrease in trunk bending angle might have contributed not only to an increased hip flexion moment but also a decreased knee flexion moment in PS.
Limitations
This study has several limitations. Other factors might have contributed to the improved gait after NDO removal. The simplest explanation is that subjects were walking under laboratory conditions; NDO removal was the last step of the experiment, and the adjustments made in the laboratory might have caused larger improvements after NDO removal compared with wearing it. We cannot say whether the immediate positive changes after NDO removal were due to the adjustments made in the laboratory or the training effect of wearing the NDO, and therefore, comparative verification is needed using a control group wearing another type of trunk orthosis. In addition, because this study involved a small sample population recruited from a single institution, further investigation is needed with a larger and more diverse patient population.
Conclusion
Stroke patients improved only their trunk bending alignment while wearing the NDO. However, gait after NDO removal was better than gait with and without the NDO. Positive changes after removal were mostly observed in PS of the hip flexion moment of the hemiparetic limb and thus increased the paretic step length.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
None declared.
Funding
This work was supported by a KAKENHI (No. 23700619) Grant from the Japan Society for the Promotion of Science.