
Abstract
Moving beyond Disability was the theme of the 12th World Congress of the International Society for Prosthetics and Orthotics. This paper is a reflection of one of the keynote lectures discussing the International Classification of Functioning, Disability and Health (ICF). Multicultural aspects in disability and sexuality in amputees will be discussed within the ICF perspective. Finally, Internet and research in the light of having a disability are positioned within the theme.
Introduction
What does ‘Moving beyond Disability’ mean? Is it possible to dream while sitting in a wheelchair up a tree? Can one still be able to read a book, while completely paralyzed? Are you able to swim with your friend who is a child with CP? Will you be able to participate in sports following an amputation? Can a person have a sexual relationship when they are severely disabled? In a world which has truly moved beyond disability, the answer to these questions would be ‘Yes!’
Questions to be considered regarding the theme are:
What is a disability? What does a disability mean for a disabled person? Is disability the same for a disabled person as for a non-disabled person? What is Quality of Life? Can we measure Quality of Life?
In this paper the following items will be discussed. The International Classification of Functioning, Disability and Health (ICF) will be introduced in relation to Disability and Quality of Life (QoL). Multicultural aspects and sexuality will be elaborated in respect of the ICF. The influence of the Internet and science on Moving beyond Disability will be considered. Finally some conclusions will be drawn.
Classification of Functioning, Disability and Health (ICF)
The Classification of Functioning, Disability and Health (ICF) (World Health Organization [WHO]2001) provides a standard language and a universal and globally accepted framework and classification that comprehensively addresses human experience in relation to functioning and health. The ICF is the successor to the International Classification of Impairment, Disability and Handicap (ICIDH) (WHO 1980). The ICIDH was a result of the traditional medical model of thought. A disease leads to impairment and subsequently to disability and handicap. The disadvantage however was that there was no causal relationship shown in this sequence. The diagnosis of the disease alone does not explain what patients can do, what their prognosis is and what their needs are. There was a requirement for a unified and standardized international language for describing and classifying health domains and health-related states. There was also a need to provide a common framework for health outcome measurement, for both individual as well at population level. With respect to the patient, the ICIDH was a negative model, whereas the ICF has a positive approach by classifying health by accounting for function. In short: There was a transition from the biomedical model (ICIDH) to a bio-psycho-social model (ICF). Advantages of the ICF are as mentioned the common language (internationally), common terminology (in publications), and the possibility for data research and for benchmarking (code-system for information for insurance companies). An example of the common language of the ICF is, for instance, assessing the expectations of the patient and also of the rehabilitation team during the rehabilitation process. This is practical in goal setting but also in the reviewing and evaluation of the rehabilitation process, and in setting renewed goals. There are several levels of severity of impairment, activity or participation (with the help of a special designed figure code).
Examples: a5101.2: moderate difficulty in the capacity to bathe
or a5101.1: minor difficulty in the performance to bathe.
The ICF framework consists of three components. The first component is body functions and structures which refers to physiologic functions and anatomical parts. The loss or deviations from normal body functions and structures are referred as impairments. The second component is activity which refers to task execution by the individual. Activity limitations are difficulties the individual may have in executing activities. Finally, the third component, participation, refers to involvement in everyday situations. Participation restrictions are problems the individual may experience with such involvement. These three components are summarized under the umbrella terms: Functioning, Disability and Health. The three components are related to and may interact with the Health condition and to the Personal factors and Environmental factors (Figure 1).
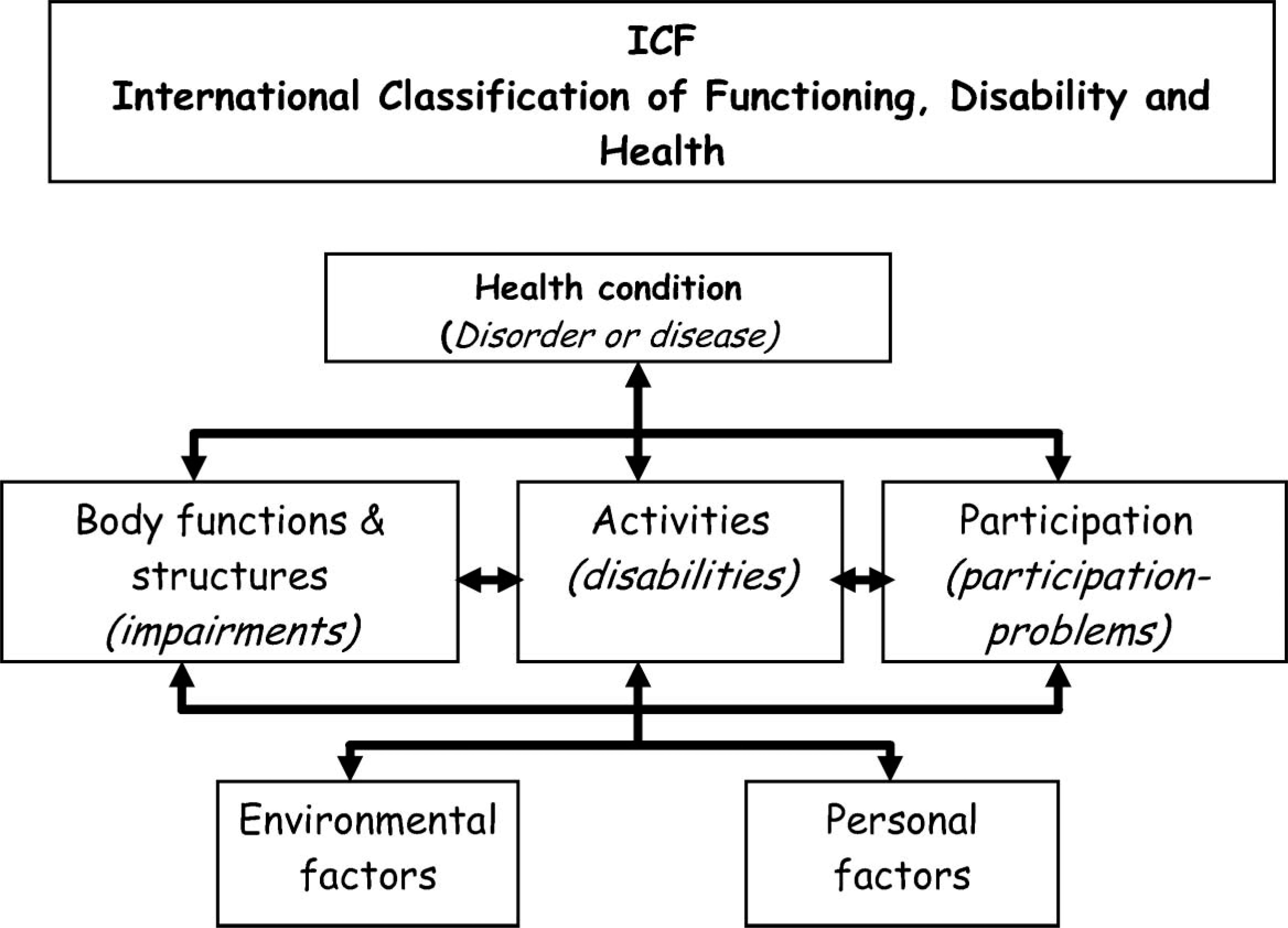
ICF Framework.
The ICF has also some disadvantages such as the existence of more than 1400 components. It is too difficult to work with such great detail in daily practice. The ICF was, however, in the first place not intended as a clinical tool. There are several groups in the world who are developing short core sets for daily practice (Stucki and Melvin 2005; Grimby et al. 2007). A special ICF checklist has been developed for clinical practice and is a practical tool to elicit and record information of the individual (www.who.int/classifications/icf/site/checklist).
Looking at the ICF-model and bringing this in daily practice, there is still a difference between what one should or can expect, regarding a person with(out) a disability and what the person really does, expects and experiences, depending on personal and external factors. In other words; there is a distinction between capacity and performance. Capacity is what we can do under the best circumstances. Performance is that what we actually do in our day to day life. Performance includes the choices we make about we do and how we do it; and this performance might not equal capacity. This is the same for both disabled and for non-disabled persons.
Disability and Quality of life (QoL)
Disability means any limitation in performing tasks, activities, and roles to levels expected within physical and social contexts. As defined by the World Health Organization, a disability is a restriction or lack of ability to perform an activity in the manner or within the range considered normal for a human being (www.who.int/classifications/en). About six hundred million people (10% of the world population) live with disabilities of various types, and the number is increasing due to the rise of chronic diseases, injuries, falls, car crashes, violence and other causes such as ageing. Of this total, 80% live in low-income countries; most are poor and have limited or no access to basic services, including rehabilitation facilities (www.who.int). Disability is located in the individual with an emphasis on individual coping and acceptance: capacity and performance.
Moving beyond Disability suggests a change in focus from disability or impairment to the broader perspective of the overall health of individuals with disabilities, the so-called holistic approach of the individual. This holistic approach is the approach in which all members of the rehabilitation (multidisciplinary) teams work with the goal of a better QoL for their patients. This is in line with the ICF. Rehabilitation Medicine is committed to reduce the burden or consequences associated with health conditions in people who experience, or who are at risk of disability in their immediate environment, by enabling them to achieve and maintain, optimal functioning implicitly compatible with the ICF. While Rehabilitation Medicine is working with ICF concept it is not as explicit as it is in the ICF framework. To acquire a better QoL for the patient is the goal of Rehabilitation Medicine. But what is Quality of Life? QoL is defined as the patient's ability to enjoy normal life activities (http://www.medterms.com). But again there are many definitions of QoL; there are even complete books and journals devoted to this subject (Fayers and Machin 2000; Hays). QoL is very complex and measuring QoL is even more difficult. Mostly in science we measure the mean Health Related QoL. But is the mean of Health Related QoL the same as the personal QoL? How can we judge what the QoL is? Can we judge for a disabled person if he/she has a good QoL? Can we even judge QoL for ourselves?
Environmental and Personal Factors
Environmental factors is the first component of contextual factors in the ICF. Environmental factors have an impact on all components of functioning and disability and are organized in sequence from the individual's most immediate environment to the general environment (individual and social level). These factors form the physical and social surroundings in which people live such as products and technology (e.g., excessive high technology versus appropriate levels), relations, attitudes, systems and policy, and finally natural surroundings. Natural surroundings in the ICF set is about animate and inanimate elements of the natural or physical environment, and components of that environment that have been modified by people, as well as characteristics of human populations within that environment (e.g., accessibility).
Another example is policies. Policies are constituted by rules, regulations, conventions and standards established by governments at the local, regional, national, and international levels, or by other recognized authorities (human rights; equal rights).
Personal factors is also a component of Contextual factors but they are not classified in the ICF because of the large social and cultural variance associated with them. Examples are age, race, gender, experience, personality and characteristics, abilities, physical fitness, style of living, upbringing, social background, independency, coping, profession and schooling. For instance: Job reintegration is successful in 80% of lower limb amputees, but this is mainly related to age, wearing comfort of the prosthesis and level of education (Schoppen et al. 2001).
Mostly there is a combination of the environmental and personal factors and activity (disability) and participation problems. There is a division in the framework but not in reality. In the WHO-ICF book activity and participation are even mentioned in the same chapter (WHO 2001).
Examples
Multi-cultural aspects
Multicultural aspects are something we are confronted with in daily life because the world is effectively becoming smaller. Travelling has become easier and people migrate more and more for socio-economic or political reasons. An additional impact is the ability of individuals to make international contacts through progressively easier access to the Internet, so there a greater mixture of cultures. The multi-cultural aspects of the ICF framework affect not only the borders on national activities or participation, or the environment but also personal factors. Aspects of gender, religion, society, economy, education, security and relation should be considered. Working with the ICF gives clinicians a broader and different view of a patient's problem. The Krukenberg construction of a stump is ‘accepted’ in many countries in the World, but finds little acceptance in Western Europe (Freire et al. 2005). However, European clinicians are seeing more patients with a Krukenberg construction due to greater emigration into Europe. So as a prescriber, we have to adapt another attitude.
During the 11th ISPO World congress, Professor Seishi Sawamura gave the Knud Jansen lecture with the following title: Culture-sensitive innovations for quality living of lower amputees (Sawamura 2004). He described the toilet facilities in East Asia; the alternative praying positions, the need for sitting cross-legged, the need for the possibility to sit with legs folded to one side, etc. These other needs of the East Asian people made the Western orthopaedic industry produce for this market extra adaptations (rotators). Nowadays in the Western World we are using this knowledge and input from industry for our patients coming around of the world.
Sexuality
With sexuality and the need to express one's sexuality, there is no different between able and non-disabled persons. Everybody (mostly) has the same needs and rights. But in many countries there is still a taboo on the discussion of sexuality and speaking about a disabled persons' sexuality is an even greater a taboo.
Reading the ICF we can find aspects of sexuality in chapter 6 (Functions): Functions of urogenital system and reproductive functions. The different aspects are very well described in detail. The social aspects of sexuality are described in chapter 7 (Activity and Participation) under the sub-paragraph: Interactions and relations (d770 romantic, intimate and sexual) (WHO 2001).
One of the advantages of the ICF was the common language not only in patient treatment but also in research. At our department a systematic review was performed on the topic: ‘Amputation and sexuality’ (Geertzen et al. 2008). The preliminary conclusions were that the finally selected papers were of low quality. The terminology with respect to sexuality was not comparable, because every author used different terms without explaining what they meant. In most papers, in the discussion section, it was mentioned that there was no, or almost no, experience in rehabilitation teams concerning sexuality in relation to amputation. In some teams this was a taboo subject and in other teams it was not considered taboo at all. But the truth is: It is an issue for the amputees and their partners.
The first publication that deals with satisfaction of amputee patients with their sexual life was that of Ide et al. (2002). Thirty percent of the amputees surveyed were not satisfied with their sexual life (Ide et al. 2002). A few of his conclusions and observations were:
There was a need for medical professionals to set up opportunities for psychological support for amputees; It was regrettable that no respondent in the study talked about sexual issues with (medical) professionals.
We have to consider, working as professionals with amputees, if we should discuss sexuality in our consultation room with our patients. If we do, we must consider in what sense: In general terms or do we ask whether a patient has intercourse and is he/she satisfied with his/her sexual life? My conclusion is that there is still a taboo on sexuality in amputees and that rehabilitation teams are not trained enough to deal with this easily. Finally, we should use the same ICF terminology of sexuality in teams but also in research.
Internet and Science
Electronic accessibility, or E-Accessibility, is the ease of use by people with disabilities of information and communication technologies (ICT) such as the Internet. What is the role of the internet regarding the theme? In 2006 the theme for the International Day of Disabled Persons was ‘E-Accessibility’. The use of ICT is rapidly becoming an essential part of the economic, educational and social life of many people today, both able and disabled. Internet activity brings a new world with possibilities to interact. Websites of interest for people with a disability (e.g., amputees) are those of the orthopaedic industry, patient organizations, governments, insurance companies, P and O facilities etc. There are also chat rooms for persons with disabilities on the pages of patient organizations. This not only facilitates the ready exchange of information, but also allows discussion of questions of self-management or insurance problems. These sites are interesting for professionals providing background and inside information which can be used in daily practice for the benefit of their patients.
Research is necessary to bring knowledge further and so in order to move the patient beyond their disability. Research can be fundamental, practical, patient bound, technical and or translational, (that is the translation of insights from fundamental research to clinical applications). Science should be more focussed on the patients needs and patient organizations must be involved in writing research grants or on the advisory boards of granting bodies.
Conclusions
Having a disability, you have the same hopes, dreams and wishes as a person without a disability. In daily practice one has the possibility to explore these with the patient and rehabilitation team. The ICF can be a tool in this exploration and in setting goals. Starting the implementation of the ICF in daily work and research seems to be logical.
Future directions and opportunities for ISPO are, for example, our input in developing a core set for amputees and if finalized implementing the core set in guidelines. Finally we should use the ICF terminology as well as ISO terminology in professional journals.