
Abstract
Background:
Vacuum-assisted suspension systems provide better suspension than non-vacuum systems, but data are limited on whether they improve physical activity levels and quality of life for people with amputation.
Objectives:
To compare the physical activity and quality of life levels of people with transtibial amputation using PIN/LOCK suspension system or vacuum-assisted suspension systems with those of able-bodied controls and to investigate parameters associated with physical activity levels.
Study design:
A cross-sectional observational study.
Methods:
Fifty-one people with amputation and 51 controls participated. The International Physical Activity Questionnaire Short Form and Short Form 36 were used to measure the physical activity and quality of life, respectively.
Results:
The total physical activity and Short Form 36 scores were significantly lower in the participants with amputation than the controls. There were no significant differences between the two types of suspension systems in terms of physical activity levels and quality of life. The vacuum-assisted suspension system users reported significantly more bodily pain on the Short Form 36 questionnaire than the controls (p = 0.003). The only parameter that correlated significantly with the total physical activity was the Short Form 36 physical functioning subscale (r = 0.302, p = 0.031).
Conclusion:
Contrary to our expectations, vacuum-assisted suspension system users compared to PIN/LOCK users did not report greater levels of physical activity or improved quality of life or levels closer to comparable controls.
Clinical relevance
A better understanding of the effects of different prosthetic suspension systems on physical activity and quality of life may help clinicians when prescribing prostheses, as well as setting appropriate prosthetic expectations. This study suggests that vacuum-assisted suspension systems and PIN/LOCK suspension systems provide equal benefit to users with regards to physical activity and quality of life.
Keywords
Background
The number of individuals with lower limb amputation increases daily. 1 People with amputation experience many physical, psychological and social challenges throughout their lives. 2 Collectively, these challenges often resulted in reduced levels of physical activity (PA) compared to people without amputation. 3 Restoring mobility and PA are primary functional goals for the amputation rehabilitation team, in addition to the overall goal of improving the individual’s quality of life (QoL). 4 PA and QoL have been reported to be related, both in people with amputation 4 and able-bodied individuals. 5
The first step towards achieving these goals is to choose an appropriate prosthesis and train the individual to use it. However, performance of a prosthesis is primarily determined by the suspension system that secures the socket to the residual limb. 6 Poor suspension can lead to excessive limb pistoning, skin irritation and discomfort, thereby limiting mobility of the user.6,7
Several prosthetic suspension systems are available for people with transtibial (TT) amputation. 6 Two widely prescribed systems are the PIN/LOCK suspension system and the vacuum-assisted suspension system (VASS). The PIN/LOCK system uses a liner with a pin attached to its distal point in which the prosthesis is suspended with a locking mechanism. The VASS system uses a pump to extract air from the socket via a one-way valve, which creates a negative pressure between the liner and socket.8,9 Studies have shown that, compared to non-vacuum suspension systems, VASS reduces fluctuations in limb volume during gait, levels of peak socket pressure, pistoning, and reported frequency of skin problems.10–12 These advantages may help to maintain a better socket fit, increase PA and improve QoL. However, the effect of VASS on PA and QoL compared to non-vacuum suspension systems is not fully understood owing to a limited number of studies, many of which had small sample sizes and did not compare the results with the corresponding data from able-bodied controls.10,11,13,14
The present study aimed to compare self-reported QoL and PA levels of people with traumatic TT amputation using PIN/LOCK suspension system or VASS with those of able-bodied controls. Furthermore, the study aimed to investigate the parameters associated with the level of self-reported total PA in people with amputation. Based on previous studies,3,15 we hypothesized that the people with amputation would have lower PA levels and QoL than the able-bodied controls. Based on limited data,11,12 we also hypothesized that VASS users would report greater levels of PA and increased QoL compared to PIN/LOCK users. We also expected that VASS users would report PA closer to comparable individuals without amputation.
Methods
Participants
A cross-sectional observational study was conducted to assess PA and QoL in lower limb prosthesis users with respect to controls without amputation. Convenience sampling was used to identify employed individuals who had undergone unilateral TT traumatic amputation, and had used either a PIN/LOCK or VASS socket suspension system for at least a year. Participants were recruited from a tertiary hospital that is a major referral centre for prosthetic services in our country. Able-bodied controls (i.e. individuals who were of similar age and doing similar jobs) were recruited from among the families and friends of participants with amputation.
The two suspension types investigated in this study were the PIN/LOCK system, comprising a silicone liner and integrated locking pin, and the VASS, which comprised a silicone liner, a suspension sleeve and an air evacuation pump. To prevent any bias from foot component on the results, the study included only participants who used a non-articulated dynamic foot (e.g. 1D10, Otto Bock, Duderstadt, Germany; ORT-08H10, Ortotek Orthopedics, Ankara, Turkey) that provides shock absorption at heel strike and a regular transition from heel strike to toe off. The other inclusion criteria were as follows: currently employed, aged 18–65 years, Medicare functional classification level K3 (i.e. unlimited community ambulator) or higher, 16 wore the prosthesis for at least 8 h a day, no history of falls within the past year and ability to walk with the prosthesis at a freely selected speed for at least 10 min without assistance. The inclusion criteria for the able-bodied controls were aged 18–65 years and the ability to walk without assistance. People with amputation and controls were excluded from participation if they had significant cognitive impairment or a medical history of balance, orthopaedic, neurological or general health problems that limited their ability to ambulate in the home and community.
All participants were informed about the study procedures and provided written consent to participate in this study. The study was approved by the local ethics committee of Ankara Numune Training and Research Hospital. (Protocol E-18-1870).
Assessments
Demographic and clinical data were recorded for each participant, including age, sex, body mass index (BMI), cause of amputation, smoking status, packs of cigarettes smoked a year, prosthesis type, time since amputation and duration of use of their most recent prosthesis. The participants with amputation were asked about any prosthetic-related skin problems and to grade the severity of their residual limb pain on a visual analog scale (VAS) from 0 to 10, with 0 indicating no pain and 10 indicating very severe pain.
PA levels were evaluated using the self-administered International Physical Activity Questionnaire Short Form (IPAQ-SF), which has shown to have evidence of reliability and validity in a Turkish population. 17 This was selected as it is one of the few reliable and valid self-report measures of PA levels that have been applied to both healthy individuals and those with limb loss.18–20 The IPAQ-SF comprises seven questions and evaluates the intensity and duration of walking, moderate-intensity activity and vigorous activity over the previous 7 days. The weekly total PA was calculated as the total of the number of minutes declared for each activity intensity weighted according to the estimated metabolic equivalent (MET) energy expenditure, in accordance with the IPAQ guidelines. MET is a physiological value indicating the energy cost of a given level of PA relative to resting energy expenditure. The IPAQ scoring procedure assigns the following MET values: 3.3 METs for walking, 4.0 METs for moderate-intensity activity and 8.0 METs for vigorous activity. 21 Each individual’s total weekly PA was categorized as sedentary (<600 MET-min/week), low (600–3000 MET-min/week) or meeting recommended levels (>3000 MET-min/week). 22
The QoL of each participant was evaluated using the Turkish-validated version of the Short Form 36 (SF-36). This comprises 36 questions related to eight different subscales, physical functioning, bodily pain, role limitations due to physical health problems, general health perceptions, vitality, energy and fatigue, role limitations due to emotional problems, social functioning and general mental health, which covers psychological distress and well-being. Each of eight subscales is scored between 0 and 100, with higher scores indicating a better QoL.23,24
Data analysis
A power analysis was performed using G*Power 3.1.9.2 software (Heinrich Heine University, Düsseldorf, Germany) to detect differences between two independent groups (group with amputation vs control group). Results of the power analysis (with α = 0.05, β = 0.20, effect size = 0.50 and a one-tailed test) indicated that a sample size of ⩾102 participants (51 in each group) was required. All the other statistical analyses were performed using SPSS for Windows v 18 (SPSS Inc, Chicago, IL, USA). The normality of data distributions was tested with the Shapiro–Wilk test, and data are summarized as mean ± standard deviation, median (range) or number (percentage), as appropriate. The Mann–Whitney U, Student’s t and chi-square tests were used to evaluate comparisons between groups of continuous and nominal variables. One-way analysis of variance was used to compare continuous variables between three groups, with post hoc multiple comparisons using the Bonferroni test for unequal samples.
Results
The study included 51 individuals with TT amputation (45 men (88%): mean age, 48 years; range, 18–65 years; BMI, 26.45 ± 5.08) and 51 able-bodied controls (41 men (80%): mean age, 44 years; range, 26–65 years; BMI, 28.10 ± 5.01). There was no significant difference between the two groups for age (p = 0.115), sex ratio (p = 0.276) or BMI (p = 0.070). Of the participants with amputation, 26 (51%) used the PIN/LOCK system and 25 (49%) used the VASS. The demographic and clinical variables of the two lower limb prosthesis user groups and controls are shown in Table 1. There were no significant statistical differences in these characteristics among the three groups (all p > 0.05).
Group comparisons for the demographic and clinical characteristics
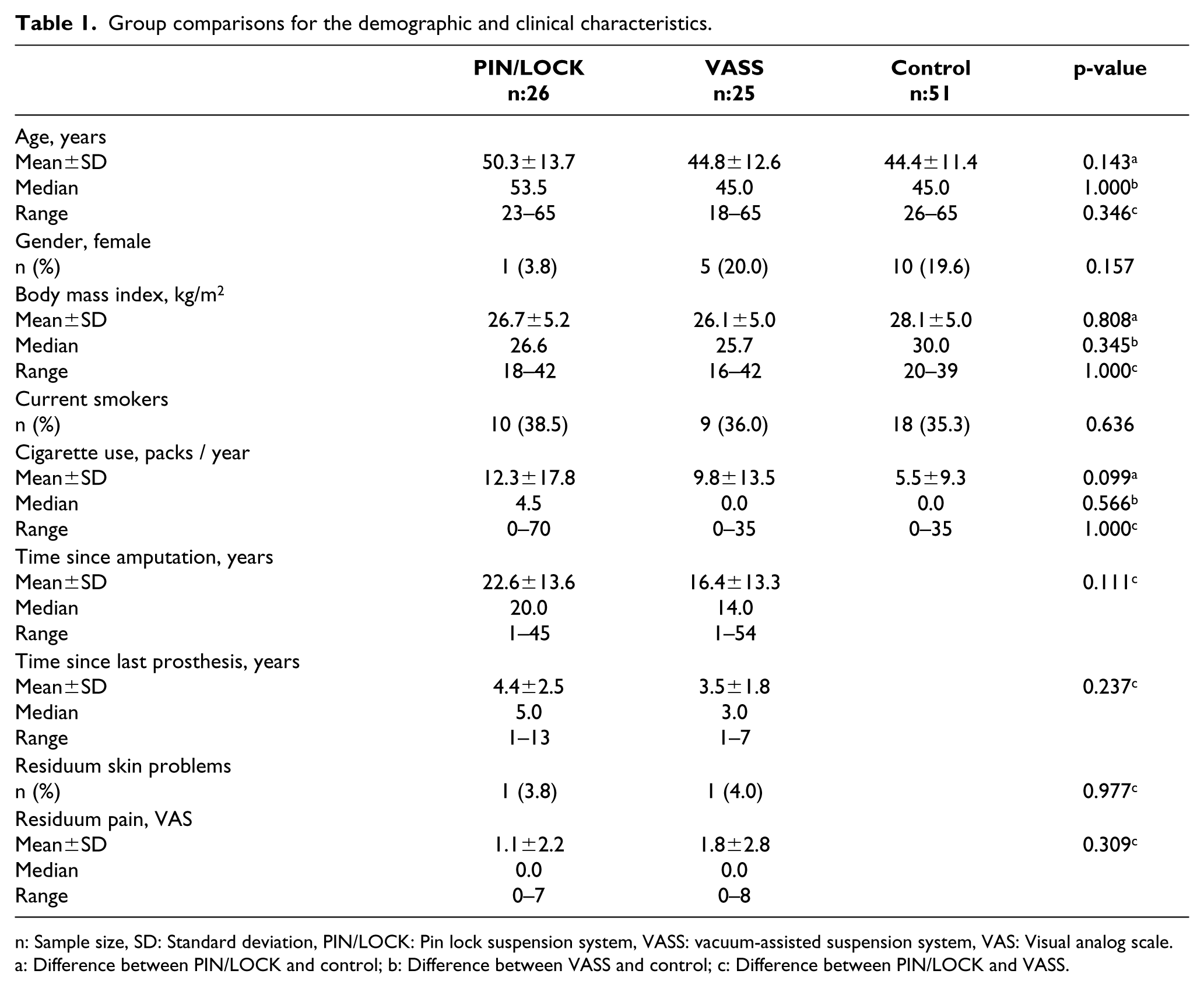
n: Sample size, SD: Standard deviation, PIN/LOCK: Pin lock suspension system, VASS: vacuum-assisted suspension system, VAS: Visual analog scale.
a: Difference between PIN/LOCK and control; b: Difference between VASS and control; c: Difference between PIN/LOCK and VASS.
All participants with amputation were graded by their managing prosthetist as unlimited community ambulators (i.e. Medicare Functional Classification Level K3). The most common cause for the amputation was a road traffic accident (n = 27, 53%) followed by industrial accidents (n = 8, 16%), construction accidents (n = 6, 12%), burns due to fire or electrocution (n = 6, 12%) and firearm accidents (n = 4, 8%). The mean period since amputation was 19.6 years, and the mean number of years using the existing prosthesis was 4.0 years. These parameters were similar between the two suspension groups, as were reports of residuum pain and skin problems.
Three participants with amputation (6%) and 13 controls (26%) reported >3000 MET-min/week of PA, and 25 participants with amputation (49%) and 14 controls (35.9%) reported <600 MET-min/week. The mean total PA levels for the PIN/LOCK, VASS and control groups were 1387.23 ± 2352.24, 1014.12 ± 978.98 and 1879.35 ± 1260.20 MET-min/week, respectively. The walking, moderate activity and total PA scores for the group with amputation were lower than those of the controls (p < 0.001, p = 0.001 and p < 0.001, respectively), but there was no statistically significant difference with regard to vigorous PA (p = 0.253). Figure 1 summarizes the PA scores of the group with amputation and controls. The scores for all SF-36 QoL domains were lower for the group with amputation than for the controls (p < 0.01 for all subscales, Figure 2).
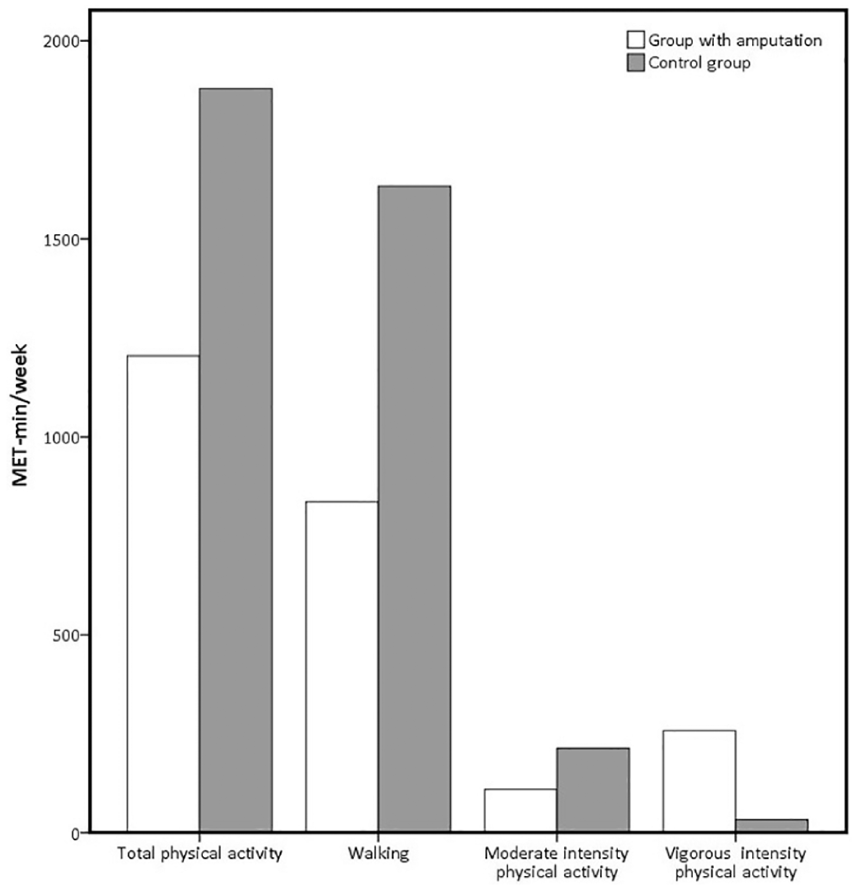
Comparison of mean scores (MET-min/week) of IPAQ-SF between groups with amputation and able-bodied controls.
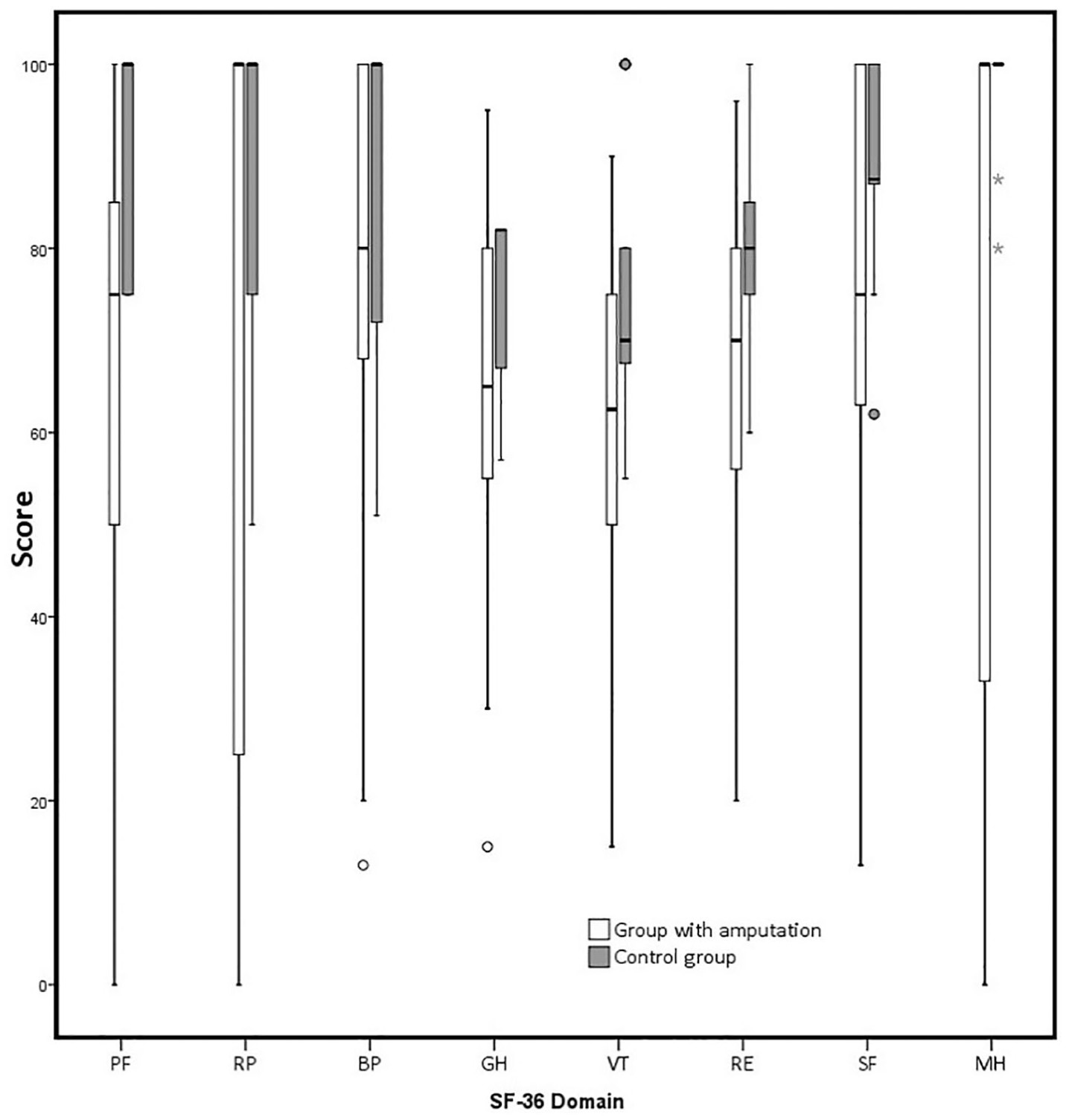
Comparison of SF-36 scores between groups with amputation and able-bodied controls. Box limits indicate the 25th and 75th quartile and the whiskers show the maximum and minimum scores. The line within boxes is the median. Circle and star indicate outlier data.
Table 2 summarizes the IPAQ-SF and SF-36 scores for the three groups. There were no significant differences in any of the PA components between the two prosthesis user groups. The walking scores were significantly lower for the two prosthesis user groups than for the control group. Although not statistically significant, the mean total PA of the PIN/LOCK group was more similar to that of the control group than the PA of the VASS group. Although there was no significant difference in any SF-36 subscale between the two lower limb prosthesis user groups, the bodily pain subscale score of the SF-36 was significantly lower in the VASS group than the controls (p = 0.003).
Comparisons of the IPAQ-SF and SF-36 scores between the two lower limb prosthesis user groups and the able-bodied controls
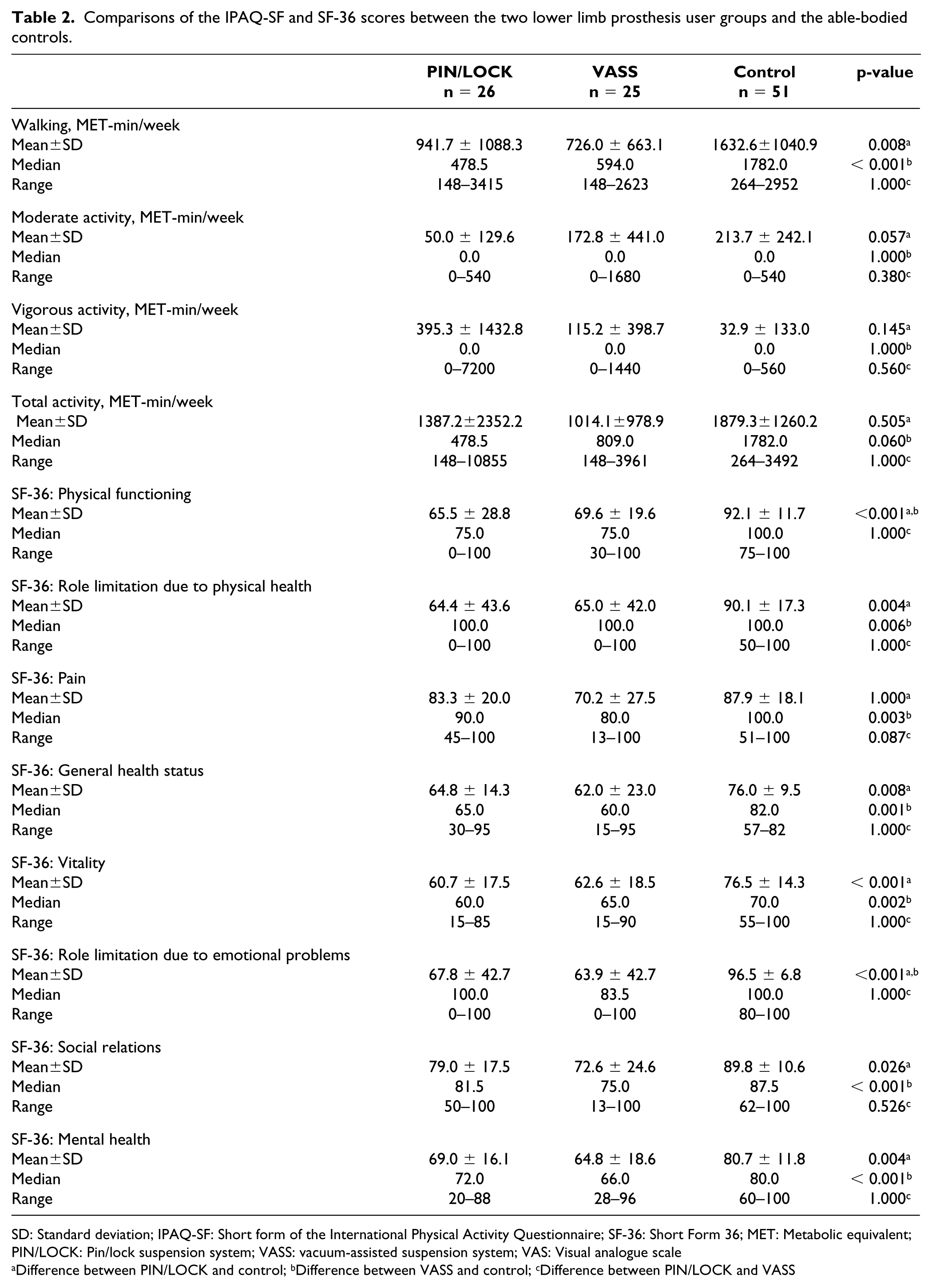
SD: Standard deviation; IPAQ-SF: Short form of the International Physical Activity Questionnaire; SF-36: Short Form 36; MET: Metabolic equivalent; PIN/LOCK: Pin/lock suspension system; VASS: vacuum-assisted suspension system; VAS: Visual analogue scale
Difference between PIN/LOCK and control; b Difference between VASS and control; c Difference between PIN/LOCK and VASS
The correlation analysis is summarized in Table 3. The only parameter with a significant correlation with PA was the SF-36 physical functioning subscale (r = 0.302, p = 0.031).
Relationship between total physical activity and clinical characteristics and quality of life in participants with amputation.
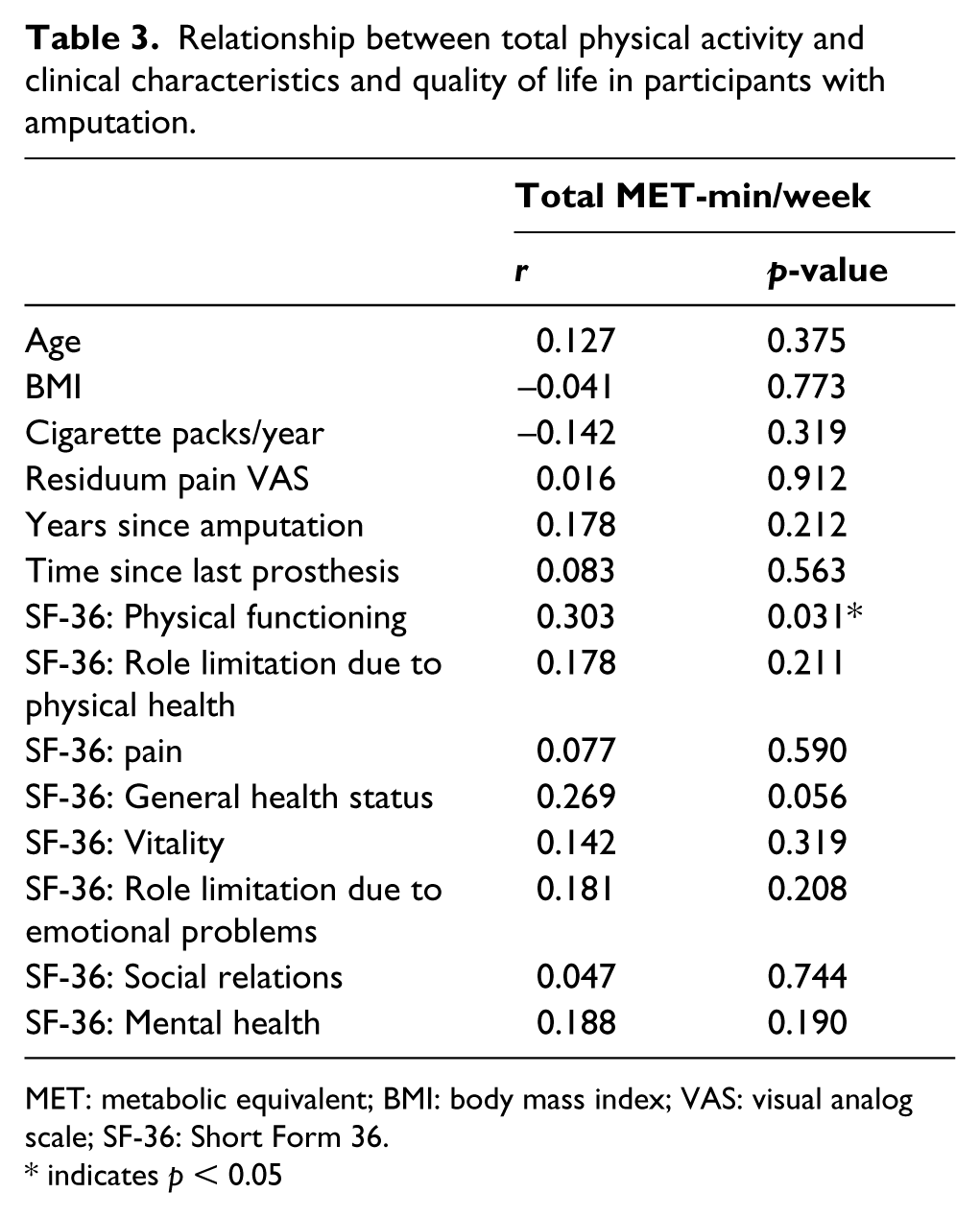
MET: metabolic equivalent; BMI: body mass index; VAS: visual analog scale; SF-36: Short Form 36.
indicates p < 0.05
Discussion
This study compared self-reported PA and QoL levels of people with amputation using PIN/LOCK suspension system or VASS with those of able-bodied controls. Results showed that the group with amputation reported significantly lower PA levels and QoL scores than the controls, but there were no significant differences between the two types of suspension systems in terms of these variables. The participants with amputation using the PIN/LOCK system reported SF-36 bodily pain scores and total PA levels more similar to those of the controls than those using VASS. We also found that PA level of participants with amputation showed a significant correlation only with the SF-36 physical functioning subscale.
Compared with their peers without amputation, the participants with amputation reported significantly less PA overall (confirming our first hypothesis), including less walking and moderate activity. The recommended 3000 MET-min/week of total PA 22 was not met by 94% of the participants with amputation and 76% of the controls. Furthermore, 49% of the participants with amputation and 29% of the controls were classified as sedentary (<600 MET-min/week). Consistent with these results, a study with 43 participants with lower limb amputation that used the IPAQ-SF found that only 9% of participants met the 3000 MET-min/week recommendations, with 51% undertaking less than 600 MET-min/week. 19 In addition, Bussmann et al., in a study that measured PA using step activity monitors, found that individuals with unilateral traumatic TT amputation were less active than healthy controls. 25
We evaluated QoL with SF-36, which has been reported to be a valid and reliable tool for measuring health outcomes in both people with15,26–28 and without amputation. 29 The participants with amputation had lower QoL scores than the controls on all the SF-36 subscales. Our results are consistent with those of other studies, which showed that amputation is a major life transition that can impact QoL many years after the incident.15,26,28 The SF-36 scores of the participants with amputation in the present study were similar to those of previous studies of participants with amputation, but there were some differences in the scores.15,26–28 This discrepancy may be due to different inclusion criteria for the participants. Among the previous studies, the SF-36 scores of the amputation group in the study by Tekin et al. 27 may be the most comparable with the scores in the present study because the participants with amputation in the two studies had similar demographic and clinical characteristics. Comparing SF-36 scores between the present study and their results showed similarities in physical functioning (67.54 ± 24.64 and 66.50 ± 17.33, respectively) and general mental health (67.04 ± 17.30 and 65.20 ± 8.65 respectively); however, there were differences in other subscale scores, perhaps because SF-36 is a self-reported questionnaire and QoL that can be affected by many other factors (e.g. phantom-limb pain, comorbidities, employment status). 15
Contrary to our second hypothesis, participants with amputation using the PIN/LOCK suspension system reported much closer total PA scores to the controls than did those using VASS. Although VASS has been comprehensively investigated in recent years, demonstrating several benefits, 12 only a few studies have compared vacuum-assisted and non-vacuum systems in terms of PA and QoL.11,13,14 Consistent with our results, Klute et al. 13 used activity monitors to compare step counts between VASS and PIN/LOCK groups and found that the participants using the PIN/LOCK system took almost twice as many steps. In contrast, Ferraro 11 found that the participants reported increased activity levels with the VASS system. However, in Ferraro’s study, participants were asked to compare activity levels between their old prosthesis (using a PIN/LOCK system) and their current prosthesis (using VASS). Comparing a new prosthesis with prosthesis at the end of its lifespan may result in bias. One possible explanation for our result is that in addition to the advantages of VASS, some disadvantages such as loss of vacuum, heavier weight and difficulty with doffing and donning the prosthesis may adversely affect PA.6,8,9,12 Although we tried to include the participants who were homogeneous in terms of factors that might affect PA, perhaps the main reason for the lack of significant difference between the two prosthesis user groups in this study was that many other factors (e.g. prior low activity level, reduced self-worth and self-efficacy, lower wealth) can have a greater influence on PA than suspension type. 3
The two prosthesis user groups had similar SF-36 scores; these were significantly lower than those of the controls for all subscales except the bodily pain scale, which was lower only for the VASS group and not the PIN/LOCK group. However, the residuum pain VAS scores were similar between the two prosthesis user groups. The SF-36 pain subscale evaluates general pain. The residuum pain VAS score may, therefore, be more informative for comparing pain associated with each suspension system during prosthesis use. On the other hand, general musculoskeletal pain is frequent in people with limb amputation and may affect PA and QoL and may be associated with prosthetic components. 30 So, future studies that assess the relationship between musculoskeletal pain and different suspension types through questionnaires specific to people with lower limb amputation would be beneficial.
The only parameter found to be significantly associated with total PA levels was the SF-36 physical functioning subscale; this may be because the physical functioning subscale includes several questions related to PA level. Total PA levels were not associated with age, BMI, the amount of cigarettes smoked, residual limb pain, time since amputation, duration of prosthetic use or any of the other SF-36 subscales. Although we observed no relationship between PA and the emotional component of SF-36, Da Silva et al. 20 reported that PA was positively correlated with psychological QoL, and several previous studies have shown that psychological well-being positively affects PA.3,31 However, it should be borne in mind that patients with mental health problems, such as depression, may underestimate PA levels in self-reported questionnaires. 32
Our study had some limitations. First, it is used as a self-reported questionnaire to measure PA. Direct measurements should be used in future studies to obtain more objective data. Self-reported questionnaires may be incorrectly answered due to a participant’s inability to recall experiences or events, or an inability to interpret the question as the developers intended. Nevertheless, previous studies have shown that total PA as evaluated with IPAQ-SF is related to objective assessments. 18 Second, an individual with a physical impairment, such as a lower limb amputation, generally consumes more energy when performing PA compared to a non-impaired individual. PA levels were estimated based on MET values and were not specific to people with a functional impairment; the PA levels of the participants with lower limb amputation in this study may therefore have been underestimated. Finally, another limitation of this study was that other factors that may affect user outcomes, such as the specific make or model of the prosthetic components, socket fit or prosthetic alignment were not adequately addressed.
Conclusion
Our findings showed that VASS compared to PIN/LOCK did not provide benefit to users regarding PA and QoL. Moreover, participants using PIN/LOCK also reported total PA (not statistically significant) and SF-36 bodily pain scores more closely to those of the controls than those using VASS. The findings, therefore, may improve our understanding of the effects of different prosthetic suspension systems on PA levels and QoL, and guide the clinician when prescribing prosthesis. However, additional studies which include direct measurement of PA, condition-specific measures of QoL and address potential confounders are needed to confirm the findings from the present study.
Footnotes
Acknowledgements
We would like to thank Enago for the English language review.
Author contribution
All authors contributed equally in the preparation of this article.
Associate Editor: Brian Hafner
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.