
Abstract
The aim of this study was to investigate the relationship between liner-related skin problems of the stump in patients with a lower limb amputation and impaired hand function. Sixty patients who were treated in a rehabilitation hospital from 1998–2006 were included in an historic cohort study. Data were collected concerning the amputation, skin problems of the stump, co-morbidity, hand function, the prosthesis, liner use and mobility score. The study population consisted of 50 trans-tibial and 10 knee disarticulation amputees, 43 male and 17 female, with a mean age of 62.3 years. The majority (63%) had a vascular reason for amputation. Blisters, folliculitis, rash and surface wounds on the stump were operationalized as being liner related. In patients with an impaired hand function, 70% had experienced liner-related skin problems of the stump, whereas 32% of the patients with a normal hand function had experienced skin problems (p = 0.035). This study shows that impaired hand function poses an increased risk for skin problems in the amputation stump in patients with a lower limb amputation and liner use in their prosthesis.
Introduction
An important part of the rehabilitation of the patient with a lower limb amputation is the training in the use of a prosthesis. The basis of this training is formed by the donning and doffing of the prosthesis with the goal of attaining independence in an adequate and safe donning technique. The ease of donning and doffing is a factor that significantly influences prosthetic wear and use (Gauthier-Gagnon et al. 1999). Different fitting and suspension methods, for example, the suction socket, Kondylen Bettung Munster (KBM) socket or liner socket, require different donning techniques and all require a proper hand function for an adequate and safe result.
Clinically the silicon liner socket is increasingly prescribed for reasons of better suspension, better cosmesis and socket comfort. However these claims are not substantiated in the literature (Baars and Geertzen 2005). With the increased use of the silicon liner in trans-tibial prostheses, following the years after its introduction (Kristinsson 1993), proper donning is even more essential to ensure adequate function of the prosthesis (Mak et al. 2001). Improper handling can result in skin problems as a result of an uneven distribution of liner material over the stump. Creasing in the liner can, for example, cause pressure points in the skin. Additionally air trapping under the liner can result in blistering of the skin (Wetz et al. 1992; Lake and Supan 1997). It is essential that the liner is evenly distributed over the stump with minimal elastic tension. Surprisingly little attention has been paid to study donning and doffing of the prosthesis or liners in view of the growing amount of liners prescribed. In a number of studies the donning and doffing is only briefly mentioned (Fillauer et al. 1989; Madigan and Fillauer 1991; Cluitmans et al. 1994; Datta et al. 1996; Hachisuka et al. 1998; Gauthier-Gagnon et al. 1999; Kapp 1999; Yiğiter et al. 2002; Tamir et al. 2003).
Skin eruptions at the proximal edge of the liner are said to occur in 10% of the patients using total contact socket interfaces (Lake et al. 1997; Stewart and Wilson 1999). No information however is provided about the donning technique and as a result it is not clear if the skin eruptions could be related to donning.
The aim of this study is to analyse, in a historic cohort, a possible relationship between impaired hand function and liner-related skin problems of the stump in trans-tibial and knee disarticulation amputees.
Methods
The medical records of trans-tibial and knee disarticulation amputees, who used a liner and were treated in ‘de Vogellanden’ Center for Rehabilitation in Zwolle in The Netherlands from June 1998 to May 2006, were retrieved from the archives. This sample included patients who had been amputated and received a prosthesis prior to 1998 as well as patients who had been amputated and received a prosthesis between 1998 and 2006. One physician (EB) treated all patients. Data were retrieved from the physician's notes and the correspondence in these records. The digital hospital records were used to verify completeness of the data. Data were collected concerning the following variables: Level, side and reason for amputation, co-morbidity, hand dominance, grip strength and hand function, and the Special Interest Group in Amputee Medicine (SIGAM) mobility score (Ryall et al. 2003). The SIGAM mobility score was scored based on information concerning the patient's mobility as written down in the records. Hand impairments were assessed during regular outpatient appointments while the patient dressed, and donned and doffed the prosthesis. These functional activities require fine coordination and sensitivity of the fingers and these activities show hand impairments if present. Hand impairments were operationalized as the loss of sensation, muscle strength or coordination of the hand and fingers, or contractures or amputations of one or more fingers (i.e., anatomical impairments). Grip strength of the patients was manually assessed by the physician and rated according to the Medical Research Council (MRC) scale (John 1984). Grip strength was rated diminished when it was less than MRC 4. Touch sense was assessed by lightly stroking the hand and fingers. Observed skin problems were operationalized as being liner related when it concerned blisters, folliculitis, rash and superficial wounds. Data were analysed in SPSS version 12.
Results
A total of 60 patient records were found who fulfilled the criteria of a trans-tibial amputation or knee disarticulation. Descriptive statistics of patients and amputations are summarized in Table I. In total 83% (n = 50) underwent a trans-tibial amputation, while 10 patients underwent a knee disarticulation. The most frequent reason for amputation was vascular (63%). Co-morbidity was present in 80% of the patients (Table I). Median time between amputation and the current study was 4.2 years (IQR 1.8–6.8). The majority of the patients were outdoor walkers (65%, n = 39). Most patients used a KBM type prosthesis (77%, n = 46). Liners were used in average, for a median period of 3.5 years (IQR 1.5–5.8). Seventy percent used a liner in their first prosthesis (Table II). The majority of these liners were made of silicon (83%). No reliable information concerning age or quality of the liners could be found in the records. As a result a relation between age or quality of the liners and the occurrence of liner-related stump skin events could not be explored.
Description of patients, type and reason for amputation, co-morbidity and SIGAM score (n = 60).
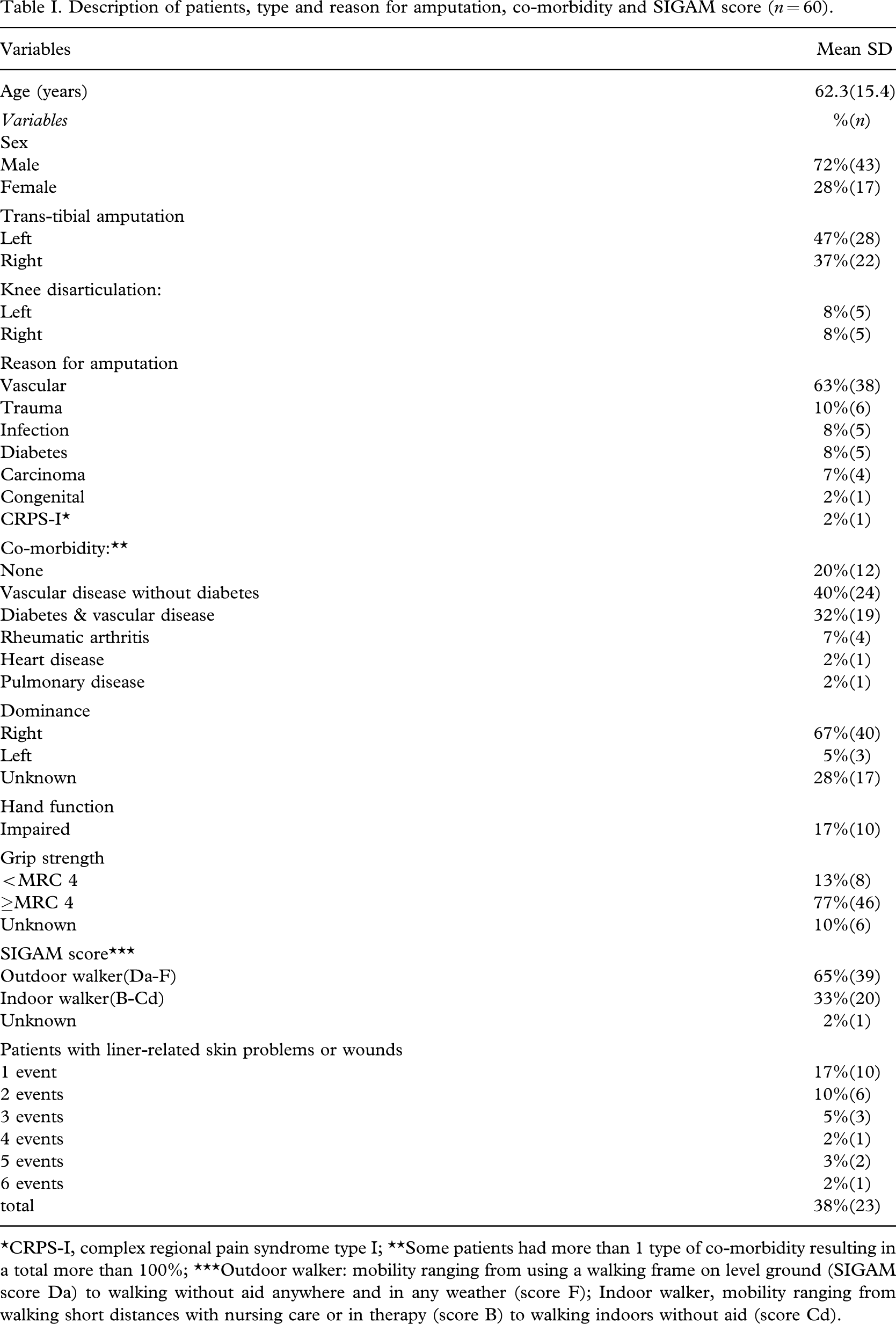
∗CRPS-I, complex regional pain syndrome type I; ∗∗Some patients had more than 1 type of co-morbidity resulting in a total more than 100%; ∗∗∗Outdoor walker: mobility ranging from using a walking frame on level ground (SIGAM score Da) to walking without aid anywhere and in any weather (score F); Indoor walker, mobility ranging from walking short distances with nursing care or in therapy (score B) to walking indoors without aid (score Cd).
Prosthesis specifications in the cohort (n = 60).
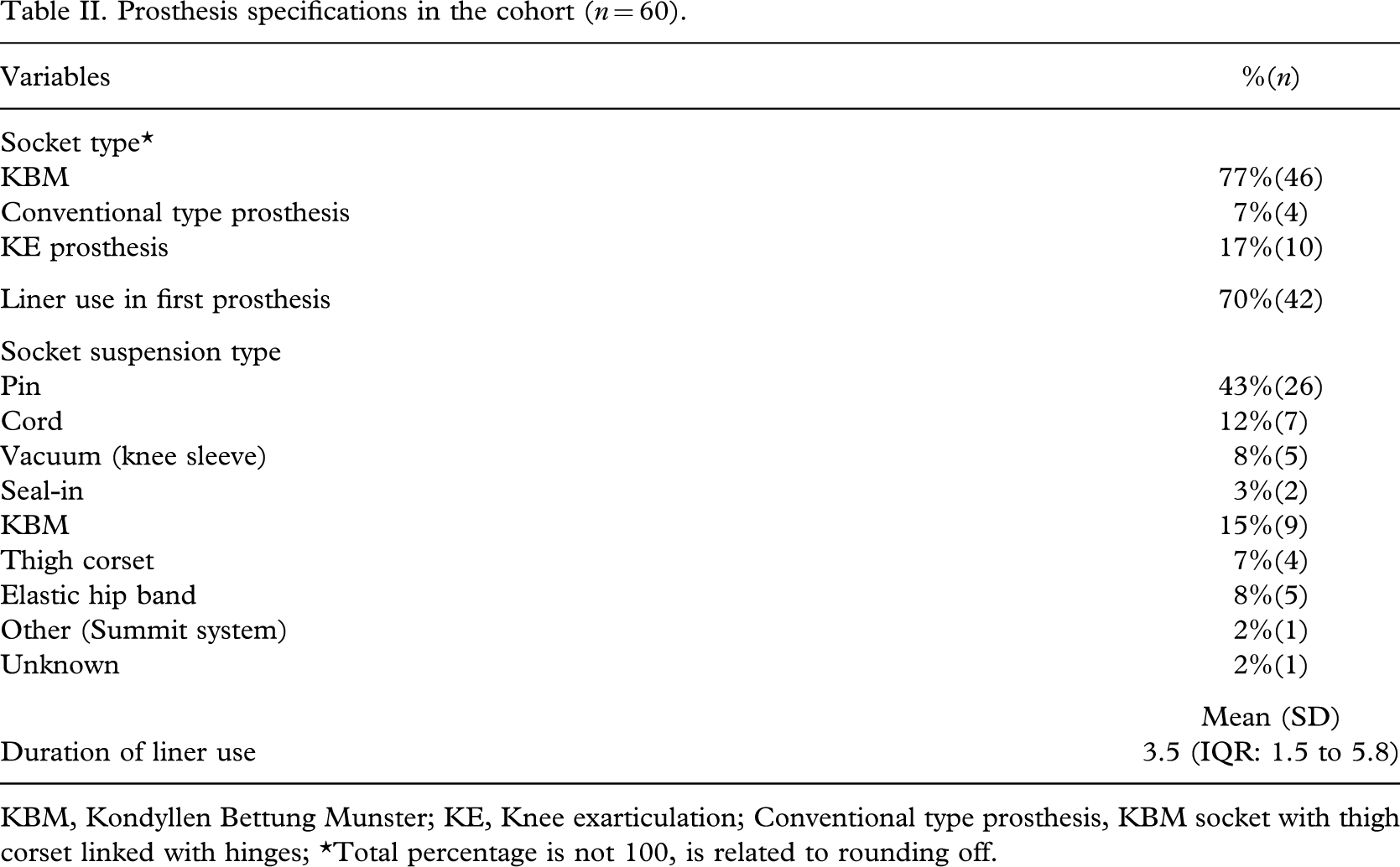
KBM, Kondyllen Bettung Munster; KE, Knee exarticulation; Conventional type prosthesis, KBM socket with thigh corset linked with hinges; ∗Total percentage is not 100, is related to rounding off.
Liner-related skin problems were present in 38% of the patients (n = 23). A total of 22% of the patients had two or more liner-related events in the study period. An impaired hand function was found in 17% of the patients (n = 10). Diminished grip strength was present in eight patients, diminished hand coordination was present in two patients and diminished touch sense was present in three patients. Several patients had more than one type of hand impairment, i.e., anatomical impairments and diminished grip strength. Most patients had similar hand impairments bilaterally because of diabetes or old age. Two patients with a CVA and hemiparalysis on the right side had diminished hand function on that side with diminished grip strength and coordination.
In the patients with an impaired hand function with diminished grip strength (n = 10), seven (70%) had liner-related skin problems whereas in the group of patients without impaired hand function (n = 50), 16 (32%) had liner-related skin problems (p = 0.035, Fischer exact two-tailed). A total of 13 blisters, four folliculitis, two rash and 41 superficial wounds was found in the cohort in this time period. Some patients had more than one liner-related stump skin event in this period. The exact location of the skin problems could not be found in the records.
Hand dominance could be ascertained in the medical records of 43 patients. No relationship was found between hand dominance and the occurrence of skin problems.
No other significant associations between liner-related skin problems or wounds and other potential risk factors were found. These factors included age, side and reason for amputation, the presence of co-morbidity and the level of mobility (SIGAM score) with the prosthesis. The type of prosthesis or type of socket suspension was not related to liner-related stump skin problems.
Discussion
An impaired hand function was significantly related to liner-related skin problems in the stump in patients with a trans-tibial amputation and knee disarticulation. About twice as high a percentage of liner-related stump skin problems were observed in patients with impaired hand function compared to those without. No relationship could be found between hand dominance and liner-related stump skin problems. From a clinical point of view it is clear that adequate hand function is a basic requirement for donning a prosthesis.
It is strange that the donning of the prosthesis and liner has received so little attention until now, because it has a direct effect on socket fit, suspension and function of the prostheses (Mak et al. 2001). Air trapping under the liner, for example, results in diminished suspension because the liner loses contact with the skin. Also the trapped air can cause skin burn and blistering when it is heated while the prosthesis is loaded.
All patients were treated in our hospital and were introduced to the liner in a similar fashion which means that they used the liner in increasing time periods to detect possible skin reactions before the actual prosthesis was made (see Appendix). By following this procedure the patient could practice the donning and doffing of the liner (Baars and Roosen 2006). Unfortunately clinically we have the experience that the liner is not always donned correctly. Misalignment of the pin in relation to the shuttle lock system in the socket, air trapping or use of material under the liner and rolling on with an extended knee (in case of trans-tibial amputees) are most frequently seen. These faults may result in insufficient suspension of the prostheses and stump problems, i.e., skin problems, wounds and pain. Because the liner can also diminish skin abrasion of the stump, caused by friction (Mak et al. 2001), this protective function can be compromised in cases where the liner is not handled adequately.
In the most extreme case the prosthesis cannot be used and a new concept must be made, i.e., KBM or a conventional type prosthesis without a liner. A conventional type prosthesis consists of a KBM socket linked with hinges to a thigh corset. The medical records were all obtained from the amputation department of the rehabilitation hospital and had a uniform design, facilitating data extraction.
The SIGAM mobility scale was included because more active patients have an increased risk for developing skin problems of the stump, i.e., folliculitis (Lake et al. 1997). This scoring system, while meant to score real time, uses systematic categories of mobility for the patient with a lower limb amputation. No relation between the level of mobility and the occurrence of stump skin problems of the stump was found in the current study.
This explorative study is the first to analyse liner-related skin problems and hand function. Before starting a prospective study it was deemed necessary to explore existing patient records for possible associations. This procedure resulted in a number of limitations. The quality of the data of the patient records depends on the precision and completeness of the records and these were interpreted retrospectively. No reliably information concerning age or quality of the liners could be found in the records. More detailed information about liner material was lacking. Thus possible relations between age and type of liner material and skin problems could not be explored. Probably minor stump skin problems were not all recorded. However skin problems that intervened in the use of the prosthesis and were alarming, were recorded because the patients usually sought medical attention in these instances. Information regarding hand dominance was missing in the records of 17 patients. Further hand function was not actually measured but assessed during dressing, donning and doffing and by manual grip strength assessment. Furthermore we assumed, based on our clinical experience, that blisters, folliculitis, rash and surface wounds were the most related to liner-related stump complications. However, no scientific literature is available to substantiate this assumption.
Future prospective studies are necessary to verify the findings of this explorative study. Based on the results of this study we conclude that liner-related skin problems of the stump are related to impaired hand function.