
Abstract
The human–prosthesis interface is one of the most complicated challenges facing the field of prosthetics, despite substantive investments in research and development by researchers and clinicians around the world. The journal of the International Society for Prosthetics and Orthotics, Prosthetics and Orthotics International, has contributed substantively to the growing body of knowledge on this topic. In celebrating the 50th anniversary of the International Society for Prosthetics and Orthotics, this narrative review aims to explore how human–prosthesis interfaces have changed over the last five decades; how research has contributed to an understanding of interface mechanics; how clinical practice has been informed as a result; and what might be potential future directions. Studies reporting on comparison, design, manufacturing and evaluation of lower limb prosthetic sockets, and osseointegration were considered. This review demonstrates that, over the last 50 years, clinical research has improved our understanding of socket designs and their effects; however, high-quality research is still needed. In particular, there have been advances in the development of volume and thermal control mechanisms with a few designs having the potential for clinical application. Similarly, advances in sensing technology, soft tissue quantification techniques, computing technology, and additive manufacturing are moving towards enabling automated, data-driven manufacturing of sockets. In people who are unable to use a prosthetic socket, osseointegration provides a functional solution not available 50 years ago. Furthermore, osseointegration has the potential to facilitate neuromuscular integration. Despite these advances, further improvement in mechanical features of implants, and infection control and prevention are needed.
Introduction
For more than 40 years, the International Society for Prosthetics and Orthotics has contributed to knowledge in the field of prosthetics by sponsoring the journal, Prosthetics and Orthotics International. In a paper published in the first edition of Prosthetics and Orthotics International in 1977, Dr Sidney Fishman
1
emphasised the need for institutional training and education to ensure that every prosthetist and orthotist demonstrated minimum competencies for the provision of safe and effective care. One of the competencies Dr Fishman considered necessary was biological sciences. He stated,
The mechanical product (machine) which the prosthetist-orthotist fabricates must be integrated with a biological entity (the human being). It must be fitted and worn in the closest intimacy to the body of the wearer for the purpose of improving the physical resources of that individual.
He further pointed out that, ‘the adequacy of efforts at physical restoration’ requires learning new science, such as biomechanics, which can enable understanding of soft tissue mechanics and behaviour under load. 1 In the intervening four decades, research has led to a better understanding of tissue mechanics and the human–device interface. It remains, however, one of the most complicated challenges facing the field of prosthetics.
A successful interface must provide a stiff coupling between the user’s skeleton and the rest of the prosthesis in order to facilitate control without causing pain or discomfort. The socket remains the most common mechanism of attaching the prosthesis to the user’s skeleton via residual limb soft tissue. However, estimates suggest that up to 50% of people with transtibial amputation do not regularly use their prosthesis, primarily due to socket problems.2 –4 The disuse rate is even higher in people with transfemoral amputation. 5 The main complaints about prostheses relate to socket discomfort, and problems with socket fit that cause skin problems.4,6 These issues may be compounded by short- and long-term residual limb volume fluctuation, 7 and heat and perspiration caused by the enclosed socket environment. 8 In current clinical practice, the process of prosthetic manufacturing remains empirical rather than data-driven; the process is iterative, labour-intensive, wasteful of material, and dependant on the prosthetist’s skill and experience with input from the person with amputation. However, a significant advancement of the last few decades is that, in select individuals with amputation who cannot tolerate a prosthetic socket, osseointegration (OI) has become available, providing prosthesis users with improved functionality, mobility and quality of life. However, use of OI remains limited by infection, and other major complications, for example, implant failure or osteomyelitis.9,10
Integrating a prosthesis with the human body poses a great challenge, and many studies have been conducted in the last 50 years in an attempt to disentangle its complexities. Accordingly, in celebrating the 50th anniversary of the International Society for Prosthetics and Orthotics, this review aimed to explore how the human–prosthesis interface has changed over the last five decades; how research has played a role in shaping our understanding of mechanics of interfaces; how clinical practice has been informed as a result; and potential future directions.
Literature search
For this narrative review, electronic databases such as AMED, MEDLINE, EMBASE, CINAHL and PsycINFO were searched using a combination of database-specific keywords pertinent to ‘lower limb’, ‘amputation’, ‘prosthesis’, ‘socket’, ‘design’, ‘biomechanics’, ‘manufacturing’, ‘material’, ‘computer model’, ‘finite element analysis’, ‘human–machine interface’, ‘osseointegration’, ‘bone-anchored’, and ‘soft tissue mechanics’. The databases were searched from their inception to July 2020; however, only studies published in the last five decades that reported on design, manufacturing and evaluation of lower limb prosthetic sockets and OI were considered. Forward and backward searches of citations from included literature reviews were also conducted to identify any potential studies not found by the database searches. Although alignment and other prosthetic components influence interface mechanics, these were not discussed here as the focus was on the interface itself. Further, the emphasis of this review was on lower limb prosthetic sockets; upper limb prosthetic sockets were not considered.
Since the first issue of Prosthetics and Orthotics International, there has been a plethora of research on user–prosthesis interfaces. As one of the leading journals in the field of prosthetics and orthotics, Prosthetics and Orthotics International has made a substantial contribution to the growing body of knowledge in human–prosthesis interfaces. The journal is among the top three journals that published top-cited articles in orthotics and prosthetics. 11 In the current review, articles published in Prosthetics and Orthotics International account for the highest number of articles cited from a single journal (16.9%, n = 37), followed by the Journal of Rehabilitation Research and Development (10.0%, n = 22), journals from the Institute of Electrical and Electronics Engineers (6.4%, n = 14), and the Journal of Prosthetics and Orthotics (5.9%, n = 13) (Figure 1). Journals that contributed between two and seven articles to the references accounted for 28.8% (n = 63) of the citations, while the remaining journals were cited only once (32.0%, n = 70). There appears to have been an exponential growth in the body of literature in recent decades. Although commenting on the increase in the number of studies is not practical given the large number of studies retrieved through the database search (~3000 records after removal of duplicates), the number of published literature reviews may give an idea; 69.7% (n = 46) of the literature reviews identified were published in the 2010s, 19.7% (n = 13) in the 2000s and 10.6.0% (n = 7) in the 1990s (Figure 2).
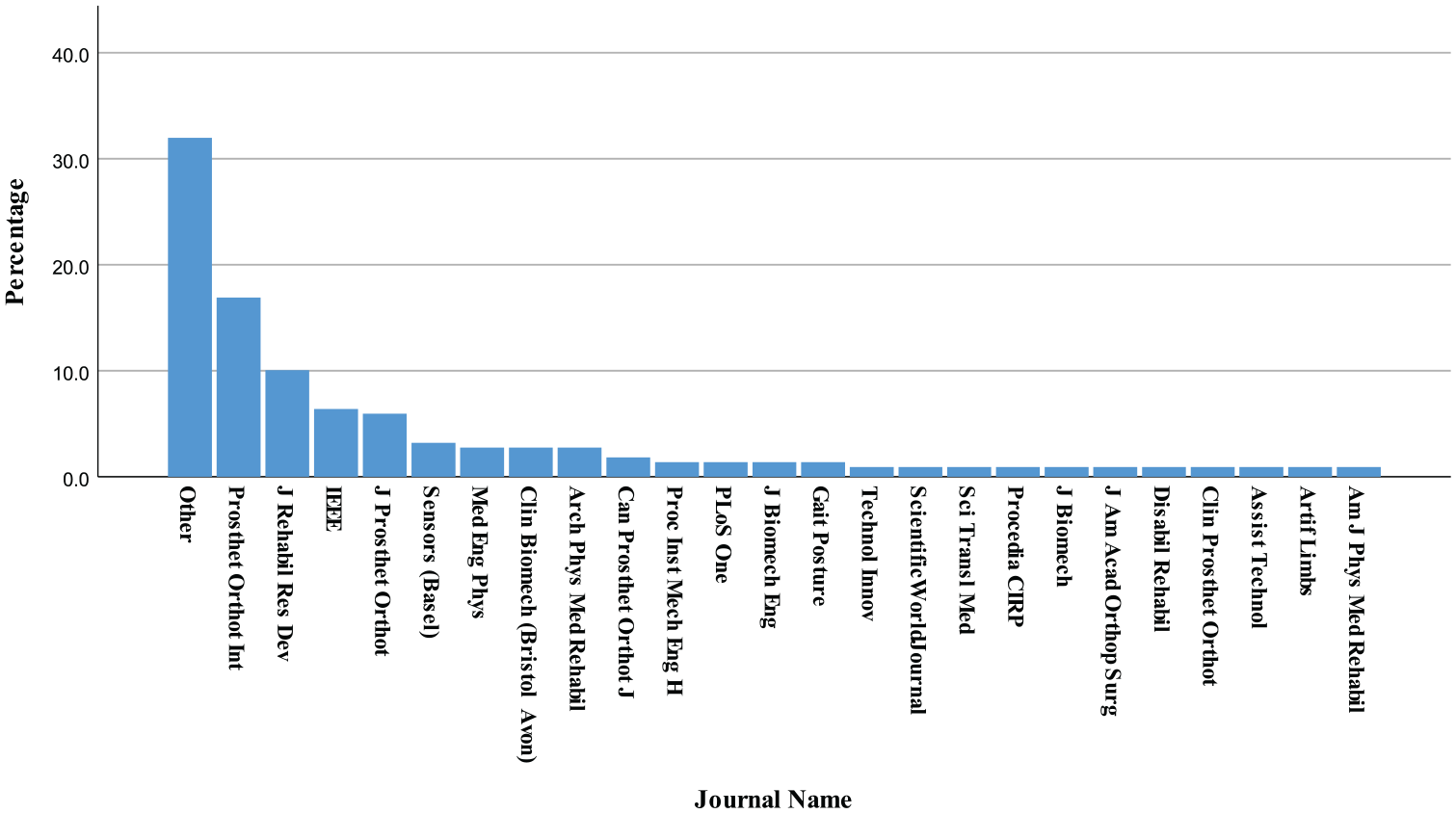
Percentage of articles published in each journal cited in the current review.
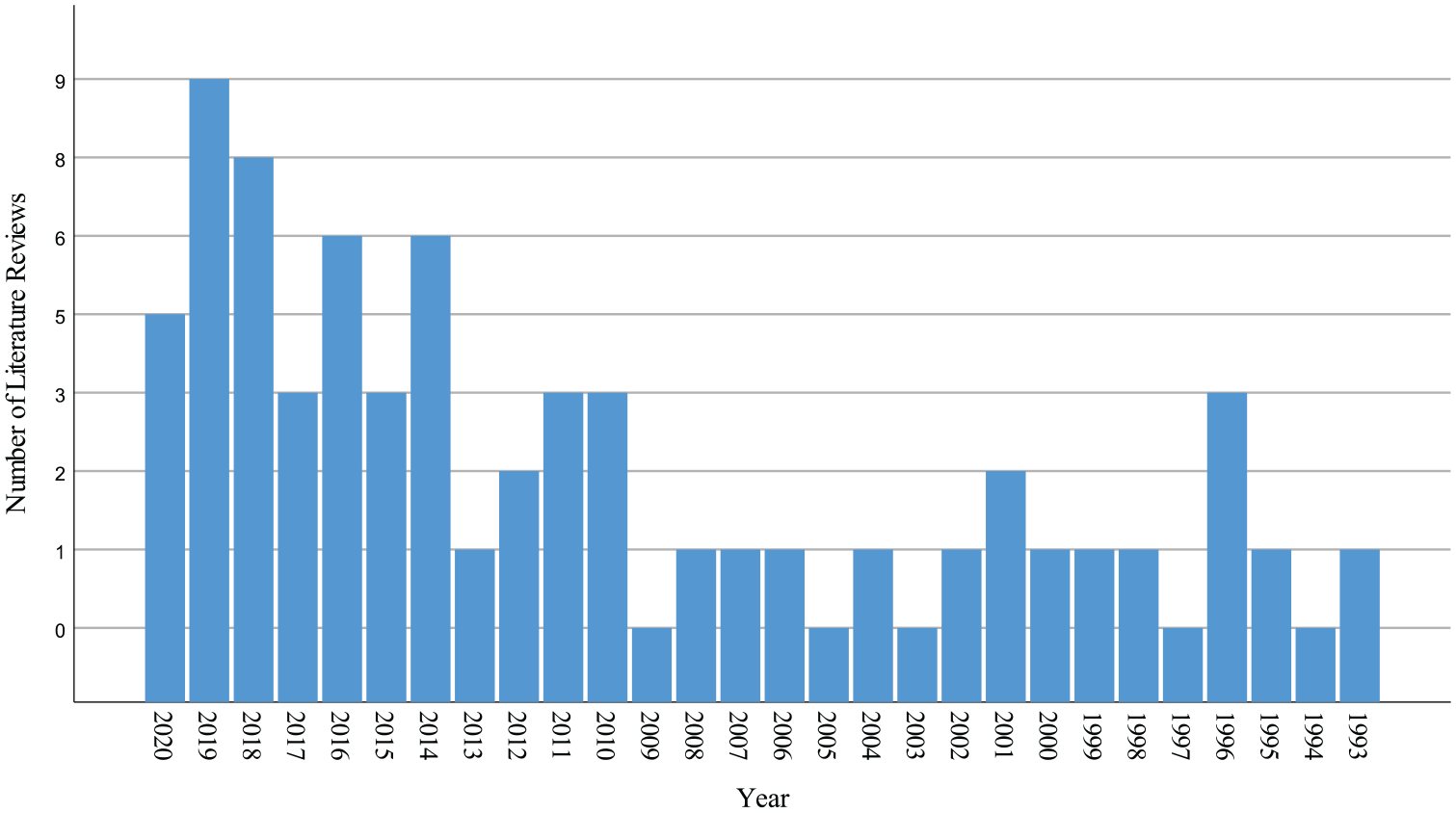
Number of literature reviews published per year on the user–prosthesis interface.
Advances in socket design and evaluation
Owing to advances in technology and material sciences, new socket designs have evolved and become clinically available in the last 50 years, and clinical studies have improved our understanding of the benefits and drawbacks of these designs. Also, interface pressure and in-socket residual limb displacement studies have examined the effects of different socket designs and suspension mechanisms. In addition, new methods of residual limb shape capture have been developed and evaluated. Various methods have also been developed for measurement and management of residual limb volume fluctuation, heat and perspiration. Moreover, sensing technologies have been proposed for smart monitoring of residual limb–socket mechanics outside of the clinic. In the succeeding sections, these advances will be discussed, followed by suggestions for potential future research.
Prosthetic socket designs and suspension mechanisms of the last 50 years
In the 1960s, the patellar tendon bearing (PTB) socket, was introduced by Radcliffe based on the biomechanics of gait and tissue load tolerance. 12 The PTB socket is shaped to load ‘pressure tolerant’ areas of the residual limb, while providing load relief to more sensitive areas. More than two decades later, Staats and Lundt 13 introduced the total surface bearing (TSB) socket concept, stating that areas previously thought sensitive could be loaded to some extent. With the advent of silicon liners, the modern-day TSB socket and the so-called ‘Hydrostatic’ socket (HS) provide better load equalisation based on the flow properties of the silicon materials.14,15 Variations of TSB/HSs based on method of residual limb shape capture, including air bladder casting, pressurised water casting, or vacuum casting, have also become available.16,66
The two primary transfemoral socket designs are the quadrilateral socket (Quad-S) introduced in the 1950s 17 and the ischial containment socket (ICS) introduced in the 1980s.18 –20 The primary difference between them is that the Quad-S has a posterior horizontal brim and a narrow proximal anterior–posterior socket dimension that helps keep the ischial tuberosity on the horizontal brim for weight-bearing; whereas the ICS encloses the ischial tuberosity and ramus in a curved posterior–medial socket wall for weight-bearing. In the ICS, support is further supplemented by hydrostatic weight-bearing as a result of the relatively smaller socket volume, and a narrow proximal medial–lateral socket dimension improves coronal plane stability. A variant of ICS introduced in the early 2000s is the Marlo Anatomical Socket (MAS), 21 which achieves coronal plane stability by containing only the ischial ramus and lowering other trim lines to allow greater range of hip motion. Another design, introduced in the last decade, is the High-Fidelity (Hi-Fi) socket, 22 which has struts that compress the soft tissues of the thigh to achieve femur stabilisation, allowing excess tissue to flow through openings between the struts. 22 Sub-ischial sockets, based on the TSB/hydrostatic weight-bearing concept, that eliminate all contact with the pelvis to improve user comfort without loss of function have also been introduced in the past decade.23 –25
The advent of suction suspension and elastomeric liners led to improvements in suspension. Early skin-fit suction suspension was introduced in the 1970s.23,26 In current clinical practice, an airtight environment between the liner and the socket is generated by expelling air via a distal one-way valve. Air infiltration is prevented by either gaskets on the outer surface of a liner that conform to the internal socket walls (e.g. Iceross Seal-In®; Össur, Sweden) or a sleeve worn over the proximal end of the socket (e.g. Alps EasySleeve™; Blatchford, UK). Pin-lock suspension, introduced in the late 1980s, 14 used a pin attached to the distal end of the liner to engage a locking mechanism fitted into the socket. Vacuum-assisted socket suspension (VASS), introduced in the 1990s, uses a pump to apply active suction between the liner and socket. 27 While initially used for persons with transtibial amputation, VASS has more recently been successfully used in persons with transfemoral amputation and sub-ischial sockets.25,28,29 Although VASS was originally developed to improve suspension, it has since demonstrated other advantages in terms of more even socket pressure distribution, control of residual limb volume fluctuation, and improved residual limb health.30 –34 These will be discussed further in the following sections.
Clinical effectiveness research
There have been many studies in the last 50 years evaluating the effects of transtibial socket designs and materials on various functional, biomechanical and patient-reported outcomes aimed at developing a better understanding of socket design. This body of evidence has spurred a number of recent reviews that help identify benefits and limitations of available prosthetic socket designs, socket materials and suspension mechanisms.30 –39 The findings of these reviews have been summarised in clinical guidelines40,41 and are highlighted below.
Overall, studies indicate that TSB sockets incorporating elastomeric liners may lead to improved satisfaction and greater activity among active and younger people with amputation, and with comparable manufacturing and fitting costs to PTB sockets.32,35 Compared to PTB sockets, TSB sockets with elastomeric liners may decrease dependence on walking aids, improve suspension and load distribution, decrease pain, and improve comfort.30,32,33 A TSB socket with VASS provides the least pistoning, followed by a TSB suction socket (Seal-In), a TSB socket with sleeve suspension, and a TSB socket with a pin-lock liner. 33 The least suspension is provided by a PTB socket with sleeve suspension or a PTB socket with supracondylar suspension.33,34 A TSB socket with VASS may also decrease residual limb volume loss, improve balance, increase physical function, and help with skin health compared to non-vacuum suspension mechanisms.30 –34 Despite these advantages, VASS requires more maintenance, user cognitive ability, and compliance; therefore, it is not recommended for all adults with amputation. 31
Comparative study of transfemoral sockets has drawn less attention from researchers than transtibial sockets. Compared to the Quad-S, the ICS results in a lower energy cost of walking, 42 increased walking speed and stride length, 43 more even interface pressure distribution, 44 improved comfort, 45 and less restriction of hip motion. 46 Sub-ischial sockets appear to be comparable to ICS in coronal plane stability and vertical movement, but with lower peak pressure at the proximal–medial brim during gait.24,47,48 Greater socket comfort and a narrower base-of-support during gait were reported for the sub-ischial socket compared to ICS due to its lower proximal trim line.24,47 A literature review of transfemoral socket suspension systems concluded that in addition to suspension enhancement, use of liners and inner flexible socket walls improves function, and comfort, and may reduce the rate of skin problems. 49
The main concern with the available evidence is the low methodological quality of clinical studies. There is a lack of sufficiently powered randomised controlled trials assessing the benefits and harms of available socket designs. Heterogeneity of intervention, study population and outcome measures makes meta-analysis impossible. In addition, the inter-related and aggregate performance of factors such as socket design, liner properties, suspension mechanisms prosthetic alignment, and components other than the socket precludes measurement of the isolated effect of these factors on fit, comfort, and function. Questionnaires assessing patient-reported outcomes operationalise constructs differently, adding to the complexity of comparison of the effects of the various prosthetic sockets. 38 Furthermore, long-term cost-effectiveness studies of these sockets, in particular VASS, are needed. 41
Vacuum level in Vacuum Assisted Suction Suspension
As noted earlier, previous studies highlight potential benefits of VASS, but may be dependent on the vacuum level. Studies indicate that there is a correlation between the amount of vacuum and prosthetic socket fit, residual limb volume fluctuation and distal displacement; moreover, this relationship is affected by the type of tissue, size and shape of the residual limb, and the swing and stance phases of gait.50 –52 Residual limbs with firmer tissues exhibit higher pressure fluctuations compared with limbs with medium firm tissues for a given magnitude of pistoning. 51 The effect of muscle contraction on pressure is larger in residual limbs with firmer soft tissues than those with medium firm tissues. 51 For a given vacuum level, firmer tissues result in less pistoning than medium firm tissues. 51
Pressures created by electrical elevated vacuum pumps are reported to range between −27 and −85 kPa.50,52 –59 A few studies have evaluated the performance of different VASS pumps, highlighting differences in maximum pressure and time to achieve a desired vacuum level.31,58 –60 Variability in performance of a mechanical vacuum pump in a transtibial socket was tested by logging socket air pressure over time during functional tasks. 61 The socket showed a decrease in socket air pressure of −34.6 ± 7.7 kPa over 10 gait cycles during a 2-min walk test, but no significant difference in task performance was observed between vacuum and suction conditions, perhaps due to the short test duration. 61 A study by Xu et al. 62 revealed that higher vacuum levels in transtibial VASS sockets (50–67 kPa) appeared to be more comfortable and improved loading of the intact limb, but also increased hip and knee external adduction moments, potentially increasing the risk of knee osteoarthritis on the amputated side; while lower vacuum levels adversely affected gait symmetry. Whether vacuum in VASS sockets was active or inactive was shown to have a small but significant effect on a few gait parameters. 63 In particular, gait was affected when the vacuum pumps were off for an extended period of time possibly due to increased residual limb volume fluctuation and poor socket fit. 63 While much has been learned about vacuum over the last two decades, future studies are needed to systematically evaluate and compare different vacuum systems, to study use of vacuum over longer periods of time, to explore the effect of vacuum during different activity levels and functional tasks, and to explore the effect of vacuum in patients with varying characteristics, such as residual limb geometry and tissue type.
Residual limb geometry quantification
Accurate and reliable quantification of residual limb geometry is a fundamental step in socket manufacturing, and long-term evaluation of shape and volume is needed for continuous clinical decision-making. Numerous measurement techniques have been developed to measure shape and volume, including the water displacement method (i.e. submerging the residual limb in water and measuring the volume of displaced liquid), anthropometric measurement, contact methods (casting or probes), optical or laser scanning, ultrasound (US), computerised tomography (CT), magnetic resonance imaging (MRI), and bioimpedance.7,64 –66 Although US, CT, and MRI provide useful internal and external structural data, their clinical application has not proved feasible for routine residual limb imaging due to high cost, potential hazards (e.g. ionising radiation in CT and risk of projectiles in MRI), and long scanning time. Shape capture in current clinical practice mainly involves plaster casting, surface scanning, and anthropometric measurement.
Load distribution in the HS is a result of the synergistic effect of casting method and flow properties of the liner material. Hence, to evaluate the isolated effect of hand-casting and pressurised water–casting methods on the outcome, PTB and hydrocast sockets were compared using pelite liners. 67 Participants reported a lower socket comfort score after 1 month of hydrocast socket use compared to the PTB socket. 67 However, in another study, where the sockets were used for a longer period (5 months), the hydrocast socket resulted in improved temporal gait parameters; hence, increased loading of the prosthetic limb. 68 Nevertheless, no significant differences were found in functional capacity, mobility, or satisfaction between sockets. 68
Studies have shown that the pressure-casting approach results in greater repeatability than the hand-casting method.69,70 However, the overall inter-cast volume difference was not considered clinically meaningful (i.e. smaller than the volume of a sock over the residual limb). 70 Both casting methods showed inconsistency regarding the shape of the cast. Interfacial pressure measurements highlight that the HS does not result in uniform pressure distribution, contrary to hydrostatic theory; however, it produces a pressure distribution with less of a variation, potentially resulting in less of a pressure gradient and hence lower shear stress. 71 Socket interface pressure distributions in PTB TSB/HSs during gait do not fully comply with the biomechanical assumptions proposed by Radcliffe.12,71,72
The Omega Tracer (Ohio Willow Wood, Mt. Sterling, OH, USA) structured light surface scanner was used to scan residual limb models and was shown to be a reliable method for measuring residual limb volume.73,74 The TT Design (Otto Bock, Germany) photometric scanner, the Omega Tracer laser line scanner, the BioScanner (BioSculptor, Hialeah, FL, USA) laser line scanner, and the Rodin4D (Rodin4D, France) infrared scanner were all used to scan residual limb models and were reported to be reliable (error variance of 3%) and repeatable in volume measurement. 75 Comparing structured light scanners such as Go!SCAN (Creaform, Levis, QC, Canada), the second generation Sense and the iSense/Structure Sensor (3DSystems, Rock Hill, SC, USA) with the hand-cast method on residual limbs, Dickinson et al. 76 concluded that the Go!SCAN was more reliable than hand-casting in volume and perimeter measurements, while the iSense and Sense scanners both had larger deviations than hand-casting.
Despite the successful application of commercial scanners in capturing a three-dimensional (3D) models of the residual limb for socket manufacturing, they have seen limited use in inter- and intra-session geometric evaluations because they do not provide internal structure data. Their application for out-of-socket volume/shape measurements is also limited due to relatively long scanning times that make them ill-suited to quantifying volume changes that occur within minutes of socket removal. Bioimpedance analysis has been developed as a method for in- and out-of-socket residual limb volume measurement for inter- and intra-session volume change measurement during static and dynamic situations. 77 However, bioimpedance is limited to measurement of residual limb fluid content and has been employed for research purposes only. More recently, a high-resolution multi-camera system (up to 40 cameras) has been developed for instantaneous in vivo measurement of residual limb shape, volume and strain. 78 Also, a mechanised water tank with an US transducer, in combination with a structured light–based 3D camera for motion compensation, was developed and tested on a residual limb model. 79 The system generated a safe and adequately accurate 3D image of the residual limb in approximately 2–3 min, while enabling the gathering of internal and external residual limb geometric data.
Surface scanners have reached a high level of reliability and speed for geometric quantification of residual limbs. However, the main unresolved challenge is the lack of knowledge as to what constitutes an accurate residual limb shape and volume for comfortable and functional socket manufacturing. Until now, the closest shape to a residual limb within a socket we can capture is the shape defined in a pressure cast during static loading. Casting during dynamic loading may be a possible avenue to further explore the behaviour of the loaded soft tissue in relation to the underlying bone.66,80,81
Management of residual limb volume fluctuation
The residual limb experiences both short- and long-term volume fluctuations, which cause socket fit to deteriorate, resulting in excessive shear and normal load over the residual limb, socket pistoning, and gait deviations.7,54,82 Various methods have been proposed for evaluation of residual limb volume changes (see the previous section and review by Sanders and Fatone 7 ).
Many attempts have been made to develop solutions for residual limb volume fluctuation including active adjustable sockets that regulate volume based on measurement of in-socket sensors. Examples include inflatable inserts using the F-socket system (Tekscan, Inc., South Boston, MA, USA) or inflatable pressure actuators,83 –86 a fluid bladder with a mechanically controlled circuit, 87 controlled magneto-rheological (MR) fluid bladders for both volume adjustment and socket stiffness control, 88 sockets with panels adjusted either manually or by a motor, 89 motor-actuated adjustable panels via a control system based on data collected by an inductive sensor,90,91 and VASS with variable vacuum pressure as a surrogate measure of volume change reflecting pistoning during walking. 51 Additionally, a few adjustable socket systems are commercially available. For example, the Infinite Socket™ adjustable, custom-moulded, four-strut design combined with a textile brim and tensioner (LIM Innovations, San Francisco, CA, USA) and the RevoFit™ manual adjustable socket (RevoFit™, Steamboat Springs, CO, USA) both for transfemoral residual limbs, and the immediate fit socket system (iFIT Prosthetics, Pewaukee, WI, USA) for transtibial residual limbs. 92
A series of studies by Sanders et al.93 –96 reveal interesting findings that may be used to develop a practical active panel socket for volume management without adversely affecting socket fit and comfort. The findings show that standing and low-intensity activity result in volume loss. 94 In transtibial sockets with pin suspension, intermittent doffing (i.e. eliminating liner pressure) may provide volume accommodation.93,94 Using an adjustable panel, the researchers demonstrated that small continual adjustment within a user’s accepted socket size range (i.e. ±5% residual limb volume changes from the neutral socket volume) may be used to adjust and possibly maintain residual limb fluid volume and limb position within the socket. 95 Finally, using inductive sensors and a socket with motorised adjustable panels, it was shown that limb fluid changed proportionally to changes in the socket volume within an optimal socket size setting. 96
In another study, increase in posterior residual limb fluid volume was demonstrated by creating negative pressure on the residual limb using a socket with three adjustable panels that were pulled outwards via a motor mounted to the outside of the socket. 97 Residual limb in-socket volume fluctuation was measured using bioimpedance while the person with amputation wore either VASS or suction suspension sockets during a 5.5-h protocol that included multiple activities performed at specified intervals. 98 Although the overall volume change was not significantly different between sockets, the results indicated that the rate of fluid volume in at least one residual limb region was increased when using VASS. 98 The authors also noticed an intra-individual variation in the magnitude of overall residual limb fluid difference between VASS and suction sockets, and suggested that a tuning system could be employed for a personalised optimisation of vacuum level because effectiveness varied between individuals and daily activities. Vacuum pressure measurement using microprocessor-controlled VASS was sensitive enough to detect differences of 1.5% or smaller in global volume. 52 These results indicate that active monitoring and adjusting of vacuum pressure may be achieved using a single controller as a method for both measurement and management of residual limb volume fluctuations.
Work is underway developing electroactive polymer (EPA) networks capable of actively expanding or contracting at low voltages, offering impact resistance and pressure sensing. 99 It has been suggested that EPA can be used in liners or sockets for automatic socket volume adjustment. 99 Also, a ferrous polymer can be used as an inductive sensor (0.50 mm thickness) and as a magnetically permeable target to measure socket wall and liner distance, and decrease socket volume by approximately 2.1%. 100 Overall, VASS with a controller and the active panel socket with an in-socket sensor appear to be viable clinical options for management of diurnal residual limb volume fluctuation; though, further developments are needed to make them commercially available.
Socket–liner material
The advent of elastomeric liners resulted in substantial improvements in residual limb loading and efficacy of prosthetic suspension systems.14,15,101 Liner material properties have been studied ex vivo under tension, compression, shear, and friction loading conditions.37,102 –106 The results indicated that soft liners improve cushioning over bony prominences, protect skin against breakdown, and provide better suspension.37,101,103 Polyethylene, closed cell liners showed better durability but had a lower coefficient of friction compared to silicon or polyurethane. 102 Stiffer liners provide a faster response to movement and would be preferred for residual limbs with excessive soft tissue. 103 Thicker liners can distribute the load more evenly across the residual limb and reduce peak pressure over bony areas (e.g. the fibula head); however, they may compromise the user’s stability during functional activities. 107
Despite the existence of literature reporting the experience of individuals with amputation with different liners,101,108 confounding factors, methodological rigour and issues with validity and reliability of outcomes preclude meaningful clinical decision-making. 36 The findings of ex vivo tests need to be confirmed by human subject experiments to establish liner prescription clinical guidelines. Furthermore, changes in liner properties, as a result of wear and tear or prolonged exposure to perspiration and body heat, have yet to be explored. 37 Future studies are also needed to explore additive manufacturing (AM) and subsequent evaluation of customised elastomeric liners.109 –112 Manufacturing multi-material liners with variable stiffness and/or thickness could also be explored once advances in AM technology emerge.
Heat and perspiration management
The use of elastomeric liners to improve load distribution over the residual limb comes at the cost of increased heat build-up inside the socket. Thermal discomfort and perspiration are common problems for prosthesis users that can result in skin problems and adversely affect socket–residual limb mechanics.8,113,114
Recent strategies explored to mitigate heat and perspiration inside the socket include perforated silicon liners,115,116 an automatic system consisting of a cooling pipe dissipating the heat to an external heat sink, 117 AM of a socket incorporating helical cooling channels and an air pump, 118 a heat pipe with fluid and wicking system, 119 a smart thermoregulatory system using a thermoelectric heat pump,120,121 phase change material (PCM),122,123 and a PCM liner in combination with an air pump in a proof of concept additive manufactured socket. 124 Finally, a vacuum was created between proximal and distal regions of the socket using a pump and electromagnetic control system to create airflow between the liner and the skin expelling heat and perspiration. 125
Williams et al. 126 compared thermal conductivity of a liner made of thermally conductive silicon, a plain silicon liner, and a hybrid liner in a controlled laboratory setting, and found no significant difference between liners. The authors concluded that passive heat transfer may not mitigate heat unless a higher thermally conductive liner or an active heat-dissipating system can be made. 126
Aside from perforated liners (e.g. Silcare Breathe, Blatchford, UK) and PCM liners (SmartTemp®; Ohio Willow Wood, Mt. Sterling, OH, USA), none of the above-mentioned strategies has yet been developed sufficiently to be clinically feasible. VASS appears to be a promising solution and further development is needed to adapt the current VASS system to incorporate a heat and moisture dissipating mechanism; a potential approach may include a perforated PCM liner coupled with VASS.
Interface pressure and shear stress
Excessive and or prolonged interface stresses result in tissue breakdown. 105 A primary objective of interface stress measurement studies has been comparing different prosthetic socket fit and comfort, assessing the effect of socket design parameters, inputting data into finite element analysis (FEA) to predict interface stress and or to understand the interface biomechanics, and assessing the effects of alignment and components other than the socket on interface stress.39,105,127 –133
Four main types of sensors have been utilised to measure interface stress: (1) strain gauges such as diaphragm deflection transducers and plunger piston-type gauges, (2) piezoresistive sensors, (3) capacitive sensors, and (4) optical sensors such as fibre Bragg grating (FBG) sensors and optoelectric sensors.129,132 Early interface stress measurements were limited to a few specific areas of the residual limb; were unable to simultaneously measure shear and normal stresses; imposed difficulty with calibration, accuracy and hysteresis; and were mostly limited to pressure measurement during static conditions. Moreover, holes in the socket wall or liners were required to accommodate the pressure sensors. There have also been problems with sensor movement, crosstalk between sensors and interference with the residual limb and socket interaction.127,131
To address some of the above-mentioned challenges, a few approaches have been explored. For example, a backpropagation artificial neural network (ANN) has been suggested.134 –136 ANN requires examples of data to be trained so that it can predict the full-field interfacial pressure from strain data collected from the exterior surface of the socket. However, there are limitations due to the lack of a standard method for selecting the most efficient ANN parameters, lengthy and expensive ANN training, and the need for ANN retraining after each socket modification. Another suggested approach is using AM of elastomeric material to manufacture flexible sensor frames to conform to the shape of the socket for measurement of shear and normal stresses at the socket–residual limb interface. 137 The sensor demonstrated pressure and shear signal linearities comparable to those of commercially available sensors. 137 Furthermore, FBG sensors have been used.138 –140 These sensors are flexible, reliable, with high sensitivity and minimum hysteresis and enable simultaneous measurement of different variables such as force, pressure, shear, temperature, and humidity, which makes them a potential choice for use in smart and active sockets.
Residual limb displacement within a socket
The stiffness of the user–prosthesis coupling is defined by the socket geometry, flow property of the liner material, the soft tissue compliance, the coefficient of friction between liner and residual limb, and the suspension system. Suitable socket shape, and choice of liner and suspension system can help minimise slippage or undesired displacement between the residual limb and socket; movements that contribute to soft tissue breakdown. To evaluate the efficacy of the suspension system and appropriateness of socket fit, previous studies have used radiography, US, CT, photographic methods, and motion analysis systems to measure socket–bone, socket–liner, and liner–soft tissue displacements in static, simulated loading, and dynamic conditions.133,141 Vertical displacement, that is, pistoning, is the most frequently measured displacement mainly to evaluate the efficacy of suspension systems (see section ‘Clinical effectiveness research’ and review by Eshraghi et al. 141 ).
Assessment of the residual limb bone and soft tissue displacement in relation to the liner or the socket can help us understand residual limb–socket mechanics and evaluate different socket designs. In the late 1990s, using CT, Commean et al. 142 measured residual limb skin slippage and tibia movement inside a socket under different loading conditions to assess socket fit. Recently, optical two-dimensional (2D) motion sensor arrays have been used to measure residual limb displacement inside the socket in vertical, anterior–posterior and transverse rotational directions relative to gait cycles.143,144 A combination of magnetic and optical motion capture systems was also used to assess socket–residual limb pistoning during gait. 145 An inductive sensor was used for measurement of distal residual limb displacement in VASS and suction sockets. 51 Using motion capture systems and markers placed on a pin liner within a transparent socket, rotational displacement, pistoning, and regional liner deformation were measured. 146 Using whole-body inverse kinematic, inverse dynamics, and motion detection data, residual limb–socket load, and displacement were estimated. 147 Low-profile inductive sensors were laminated inside the socket wall, and using a liner with a ferromagnetic flexible target and a portable controller, the distances between the liner and socket were measured at various locations to give insight into liner–socket displacement. 148 As noted previously, data derived from microprocessor-controlled VASS may be used to quantify and monitor socket fit. 52 Future studies could explore the effects of different socket designs, liner materials, and tissue compliance on multi-directional socket displacement and local soft tissue movement relative to the gait cycle, and prosthetic alignment, and components, for a better understanding, and management of, socket–residual limb interactions. 143
Smart monitoring system
Current clinical practice, although based on years of empirical evidence, relies largely on practitioners’ expertise and clinical judgement, and users’ subjective feedback and comments for assessment, treatment prescription, and follow-up evaluation. Monitoring and sensing technologies have the potential to complement current clinical practice approaches by improving therapeutic, diagnostic and prognostic outcomes.149,150
Instrumented socket inserts incorporating sensors (e.g. proximity, force and inductive), wires, and circuitry have been employed to collect field data on socket–residual limb variables. 151 A wireless system with flexible support for up to 32 force sensors, an analogue front-end reader and a low-power microprocessor controller was also designed to be capable of continuous measurement of interfacial load for up to 8 h. 152 As noted earlier, 3D printing with elastomeric material was used to manufacture flexible sensor frames for pressure and shear measurement. 137 An inductive proximity sensor 153 and bioimpedance 154 have also been used for monitoring residual limb volume changes and activity in the community.
In a stakeholder event, participants expressed a preference for a lightweight monitoring system for short-term use that would enable measurement of in-socket temperature and pressure. 155 A potential monitoring system has to be of a minimal disturbance to the user and may initially be considered for a certain group of users, for example, people with vascular disease and older adults.
Automated data-driven socket design
In the 1980s, computer-aided design (CAD), computer-aided manufacturing (CAM) and FEA were introduced to the field of prosthetics. 156 Improvements in pressure measurement techniques, advances in the understanding of soft tissue stress and strain behaviour, and the advent of reliable computers and manufacturing technologies provided the field with opportunities to better understand the biomechanics of the socket–residual limb interface and to explore approaches for automated data-driven manufacturing of prostheses.
Several attempts were made to design a patient-specific, data-driven socket in a research environment.157 –162 Goh et al. 157 developed a CAD/FEA program and used a commercial CAD surface scanner to create a 3D model. The internal bone geometry was determined using an anthropometric method. The researchers then validated the finite element (FE) model against experimentally-measured data showing fast and accurate analysis. Lee and Zhang also used quantitative pressure and pain data, and MRI images of a residual limb as input data for FEA to fabricate a socket. 158 Another group manufactured a variable impedance socket using AM technology based on an MRI image of the residual limb. 159 The shape of the socket geometry in relation to the bone was defined based on inverse correlation of tissue thickness over the tibia. In later works, the same group of researchers quantified mechanical properties of the residual limb soft tissue using a computer-controlled multi-indentation device.160 –162 Then, using an inverse FEA, the 3D model of a socket was designed, evaluated, and used for AM.
Despite the promising results of the above-mentioned endeavours, several technological challenges must be addressed before FEA can be introduced in to clinics (see next section). Current clinical CAD/CAM systems use a surface scanning device to create a digital 3D model of the residual limb, CAD software to modify the 3D model into a desired socket shape, and CAM to fabricate the modified CAD model. This conceptually replicates the conventional socket design in a digitised form; the design process is still iterative and subjective based on the prosthetist’s experience.66,130,163 Nevertheless, the CAD system offers the possibility for storage of a digital 3D model of the residual limb for future evaluation of prosthetic management in an environmentally-friendly manner as it reduces material waste.
Finite Element Analysis
Many research groups have reviewed decades of research findings on prosthetic socket FEA.39,131,163 –166 Early FEA studies were mostly method development.131,163,166 An extensive recent review of the topic highlights FEA findings and development in (1) modelling preloading from socket donning and friction/slip, (2) modelling of residual limb soft tissue internal mechanics, for example, viscoelasticity/hyperelasticity, deep tissue injury and thermal analysis, (3) identification of residual limb tissue characteristics, for example, creep, stress relaxation and pain tolerance threshold, (4) proposals for incorporating FEA into socket fit and assessment, and (5) analysis of osseointegrated prostheses. 164
Further research is needed to enable commercial CAD/CAM with computational modelling of the optimal socket design based on quantitative data. To be feasible, the accuracy and validity of FEA in the prediction and evaluation of socket fit must be confirmed. FE predictions depend on reliable data about geometry, material and soft tissue properties, and loading and boundary conditions.
A reliable, safe and accessible method is needed for quantification of residual limb geometry. Current imaging methods of internal and external structure quantification are either unsafe or inaccessible and costly (see section ‘Residual limb geometry quantification’ for summary of imagine methods). A potential approach could employ methods proposed by Goh et al., 157 as described earlier. To enhance accuracy, FEA also needs to model soft tissue hyper-viscoelasticity, anisotropy, and inhomogeneity, taking into account tissue pressure pain/comfort thresholds. Furthermore, accuracy is influenced by additional factors such as socket–residual limb mechanics, socket-induced soft tissue preloading, load types, static and dynamic gait conditions, bone–soft tissue kinematics, heat and perspiration inside the socket, prosthetic alignment and components, residual limb volume fluctuation, tissue adaptation, muscle contraction, age and health conditions, and liner/socket material properties. Considering the current state of science and technology, it seems impossible to include all the above factors in a model. However, exponential advances in computing technology may make it possible in the future.
Achieving a high level of accuracy raises another issue that is concerned with lengthy solver time, costs, and requirement for specialised expertise to use FEA software. FEA solutions could be developed including as many of the above factors in the design process to validate a fast and user-friendly simpler model. As an example, using a statistical shape model, a surrogate model was developed capable of real-time prediction of residual limb shape and socket design. 167
Another approach for quantitative automated socket design could be based on artificial intelligence and knowledge-based system approaches. A rectification map was created as a socket fabrication template in CAD/CAM. 168 Also, the design experience of several prosthetists was employed to develop an algorithm to build a quantitative compensation model for socket design based on tissue characteristics of the residual limbs. 169 A research group proposed automatic rectification based on empirical rules. 170 The method established a correlation between the local rectification quantitative data and qualitative scores of soft tissue tonicity, activity levels, and subject weight. Then, performance was assessed by FEA and a socket was manufactured using AM. For such an algorithm to be successful, a large amount of data is required to train the system.
Tissue response to load
Quantification of, and understanding the relationship between, soft tissue behaviour under different loading conditions, its mechanical properties, and load-induced pain/comfort threshold, could improve quantitative socket design and evaluation using FE and virtual prototyping.
There are a few hypotheses, with varying levels of evidence, about tissue response to excessive load, including (1) arterial blockage resulting in local ischaemia and anoxia, (2) toxic substances build-up in the tissues as a result of a disturbance in the lymphatic system, (3) reperfusion injuries and reactive hyperaemia, and (4) cellular necrosis as a result of mechanical insults. 171 There is an inverse relationship between the magnitude of the load and loading durations that results in tissue breakdown. 172 Shear force accounts for 40% of pressure ulcers, 173 and addition of shear to pressure increases the susceptibility of tissue to breakdown. 174 Cyclic loading and unloading results in more skin breakdown than constant loading alone, most likely due to cumulative reperfusion and reactive hyperaemia. 171 However, if a load is applied within a certain magnitude and duration window, tissue adaptation may happen. 105
Soft tissue exhibits anisotropic, inhomogeneous, and non-linear viscoelasticity properties that change by anatomical location, muscle contraction, tissue composition, ageing, and pathological conditions.64,171,175 Indentation measurement, US, MRI, CT, and computational modelling (e.g. reverse FEA) have all been used for quantification of soft tissue properties. 64 Indentation has been the most commonly used technique for in vivo measurement of mechanical properties of the soft tissue.64,176 However, there are concerns with the validity of indentation measurement including the effect of indentor misalignment, muscle contraction, indentation rate, and being limited to measurement over a few anatomical locations. To address the limitation of previous methodologies, a multi-indentor device, comprised of 14 indentors with a known angle-of-attack and position and force controller, has been developed. 162 The device circumferentially surrounds the residual limb to form an actuator ring to characterise soft tissue hyper-viscoelasticity.
Load-induced pain varies between anatomical location, and from person to person.105,171 Generally, the method for measuring load-induced pain involves measuring minimum pressure causing discomfort or pain (pressure threshold) and maximum tolerable pressure. 177 Animal experiments suggest a sigmoid-type pressure duration tolerance curve exists, for example, muscle damage occurs after a short exposure to pressure >32 kPa whereas < 5 kPa pressure can be tolerated for a long time. 171 To understand the behaviour of residual limb tissue, studies of pressure and shear force tolerance curves for different tissue types and anatomical location are needed. 171
Radcliffe qualitatively defined tolerant and sensitive areas of a residual limb as a design principle for the PTB socket. 12 Studies have shown that the magnitude of pressure at the popliteal area correlates with patients’ discomfort level178,179 and pressure-induced pain is lower in the popliteal area than over the patellar tendon. 88 Use of a PTB socket can result in degeneration, neovascularity, and morphological changes in the patellar tendon. 180 The load-tolerance levels of the distal ends of residual limbs have also been reported in previous studies.181,182 In an HS, high peak pressures in the anterior proximal region, and longer durations of submaximal loading in the lateral proximal region and the anterior and medial distal regions, were factors related to discomfort. 183
Understating cumulative tissue damage that results from loading and subsequent oxidative reperfusion and inflammation, and the relationships between load–unloading cycles, the tissue healing process, and tolerance threshold from persons with amputation are needed.171,184 Capitalizing on advances in powerful computing technologies, full-field FEA, including all the previously described important factors, is needed to evaluate correlation and predictability of certain measurements taken in a clinical environment to assess whether this technology can be used for socket design and evaluation.
Additive Manufacturing
AM has the potential to bring about a paradigm shift in socket and prosthesis design and manufacturing. This technology enables the creation of complex geometric sockets, using less material, in a shorter time, while eliminating the need for an intermediate plaster mould, and hand laminating and finishing procedures. In a limited clinical evaluation, AM demonstrated the capability of fabricating well-fitting lower limb prosthetic sockets with adequate strength, mostly using Nylon 11 and 12 in selective laser sintering, and polypropylene in fused deposition modelling.185,186 Sockets could be made to have: compliant features in order to lower average or peak pressure over bony prominences or pressure-sensitive areas of the residual limb;187,188 wall hardness with an inverse relationship to tissue compliance, that is, less compliant tissue resting against a softer wall material and vice versa, 159 and inflatable/deflatable elements 189 or printed inserts 190 to accommodate volume fluctuations of the residual limb.
Multi-material AM technology could make it possible to fabricate the socket and or prosthesis in materials of varying stiffness. 191 AM could offer opportunities for manufacturing customised elastomeric liners109 –111 and printing electrodes and sensors for smart and active monitoring and measurement of interface mechanics.192,193 However, further work is needed to integrate AM with current CAD systems that may be potentially compatible with FEA. The high initial cost of AM equipment and material, slow printing speed, and material strength are challenges that may be addressed using central fabrication AM facilities, metal, fibre-reinforced, or multi-material AM, and cloud-based systems.186,194,195
Osseointegration
OI is a direct attachment of a prosthesis to the skeletal structure via an intramedullary implant. 196 During the last 30 years, OI has become a clinically-viable procedure. 197 Potential candidates are individuals who have complications with, and are unable to use, their prosthetic socket. Generally, the implant anchoring systems involve a threaded connection, a press–fit interface, or contain interosseous pins. 198
A great deal of literature reporting benefits and complications of OI in observational studies exists, and as a result, several reviews have been conducted recently.9,10,199 –204 Studies indicate that OI may improve walking ability, stability, functional capacity, and quality of life in individuals with amputation who cannot tolerate their prosthetic socket.9,199,201 –203 A few studies reported complaints of pain, usually associated with weight-bearing, and some users raised concerns with the relatively long post-surgical rehabilitation time. 9 Phantom limb pain may not improve when using an OI prosthesis 9 and the effect of OI on emotional state is not clear. 201 Compared to prostheses with a socket, OI may be cost-effective based on conservative estimates. 201
The common complication of OI is a minor infection at the skin–implant interface that can be treated with antibiotics.9,199 Although serious, adverse events such as periprosthetic or overall fractures, implant loosening, osteomyelitis, revision surgery, or implant removal are rare, they pose a serious clinical concern.9,10,199 Three long-term follow-up studies (5, >9, and 15 years) indicate that, although improvement in patient-reported outcomes has been reported since OI was first introduced, there are still concerns with tissue infection205,206 and the mechanical properties of the implant,206,207 possibly related to higher activity. 207 In addition, loss of bone density is associated with implant removal. 208
One should note that a substantial proportion of evidence regarding OI comes from observational studies with overlapping study samples.199 –201 OI is prescribed to people experiencing problems with their prosthetic socket and those who do not have vascular disease. However, there is a lack of evidence as to the effectiveness of different implant anchoring systems, both in terms of clinical outcome and from a biomechanical perspective, for example, degree of OI or infection prevention. Future development could be directed towards improvement of the surgical protocol and shortening the rehabilitation period; improving implant designs to enhance bone ingrowth and reduce loosening; increasing the implant safety mechanism; infection control and prevention strategies; and improving mechanical properties of the implant for intense activities.
More recently, a distal weight-bearing implant has been developed, consisting of a femoral stem placed inside the femoral intramedullary canal and a spacer that is connected to the stem using a screw/plug.209,210 The implant is located beneath the distal soft tissue of the residual limb, enabling distal weight-bearing and an improvement in distance and speed of walking.209,210 An FEA and laboratory simulation of a similar conceptual implant with a distal fluid-filled elastomer bladder showed an increase in distal weight-bearing and decrease in pressure and shear forces at the proximal regions of the residual limb. 211 More evaluation and longer-term studies are needed regarding benefits, and possible complications, before wider exploitation of these concepts are possible.
In 2013, the standard OPRA (Osseointegrated Prostheses for the Rehabilitation of Amputees) implant was upgraded to eOPRA (enhanced Osseointegrated Prostheses for the Rehabilitation of Amputees) and included implanted electrodes to provide biological signals for bidirectional communication between an upper limb prosthesis and the user’s neuromuscular system. 212 Later, the system was further developed to include a controller capable of decoding motor intent and providing sensory feedback. 213 Also, an agonist–antagonist myoneural interface (AMI) has been proposed to enable voluntary control and proprioceptive feedback in lower limb OI prostheses. 214 The AMI consisted of two subdermal grafts linking agonist–antagonist muscles to imitate dynamic interaction found within an intact limb. Further research is needed to explore OI facilitation of neuromuscular integration for enhanced prosthetic control, proprioception and sensory feedback.214 –218
Conclusions
Nearly 50 years ago, in the first issue of Prosthetics and Orthotics International, Dr Fishman stated that the study of physics, materials sciences and mechanics is necessary for the design of prostheses and orthoses, and that a qualified practitioner requires knowledge of biology, anatomy, kinesiology, pathology, biomechanics, and pathomechanics when fitting a device to a human being. 1 In the intervening years, clinical practice, and research proved that Dr Fishman was correct. However, more recently, new fields of study such as engineering, computer modelling, artificial intelligence, AM, and electronics have begun to play an important role in enhancing our understanding and fabrication of prosthetic sockets. In the near future, sensing, monitoring, and actuator technologies may facilitate socket fit, control of volume and heat, and residual limb health. Prosthetic sockets that incorporate sensing, monitoring, and actuator technologies will likely be manufactured through a fully automated, person-specific and data-driven process using powerful computer modelling, reliable quantification of residual limb geometry and mechanical properties, artificial intelligence and simulation techniques, and AM; the combination of which will bring a paradigm shift in the user–prosthesis interface resulting in intelligent sockets. Through improvement in mechanical features of OI implants, advancements in infection control and prevention strategies, and the potential for neuromuscular integration, OI will likely become appealing to more people with amputation. Regardless, it is unlikely that one method (OI or sockets) will significantly overtake the other, given the heterogeneous needs and preferences of lower limb prosthesis users.