
Abstract
The physiological cost of walking is greater in bilateral amputees (BA) than in both unilateral amputee and non-pathological gait. The aim of this study was to describe the physiological costs and other standard gait characteristics in a sample population of BA, walking at self-selected (comfortable) speeds. Amputees had bilateral trans-tibial, bilateral trans-femoral or trans-tibial/trans-femoral amputations as a result of trauma or congenital defects. All amputees wore their own prosthetic limbs which were either full-length prostheses or short non-articulating pylon prostheses (SNAPPs). The results were compared with a base line data set collected from a non-pathological control group. It was anticipated that amputees with high-level amputations would walk at the slowest speeds, have the highest physiological costs and lowest perception of walking ability. However, varying walking speeds resulted in varying exercise intensities, exercise heart rates and perceptions of walking that could not be directly related to amputation levels. It is therefore concluded that bilateral amputee gait is complex, varied and not easily categorized.
Introduction
During steady state, non-pathological walking, the selection of an optimum speed (normally between 1.1 m/s and 1.4 m/s) and use of specific gait determinants serves to maintain gait efficiency (Saunders et al. 1953; Perry 1992). Limb pathologies such as lower-limb amputation can result in a decrease in walking speed, which is known to reduce gait efficiency (Detrembleur et al. 2005). Abnormal movement patterns associated with amputee gait are also likely to decrease the mechanical efficiency of walking because body segment movements become disjointed and typically awkward. This in turn affects the smoothness of the pendular-like movement of the centre-of-mass (CoM); additional mechanical work is needed to move the CoM and energy recovery during each step is significantly lower when compared to non-pathological walkers (Gitter et al. 1995; Tesio et al. 1998; Detrembleur et al. 2005).
Bilateral lower limb amputees (BA) find walking increasingly more difficult as the level of amputations increase (Waters et al. 1976). It is thus not surprising that research has found bilateral amputee gait to be less efficient when compared to unilateral amputee and inevitably non-pathological gait (Huang et al. 1979; Wainapel et al. 1985; Crouse et al. 1990; Hoffman et al. 1997; Wu et al. 2001; Perry 2004). However, much of what we know about BA gait is derived from case study (single patient) data (Wainapel et al. 1985; Crouse et al. 1990; Wu et al. 2001; Perry 2004). Whilst this information is important for rehabilitation of the individual, and comparison and performance studies between different types of limbs are important for prosthetic manufactures, information gained from a larger population will help researchers and clinicians to uncover relationships between form and function in BA gait which could help inform future clinical decision making.
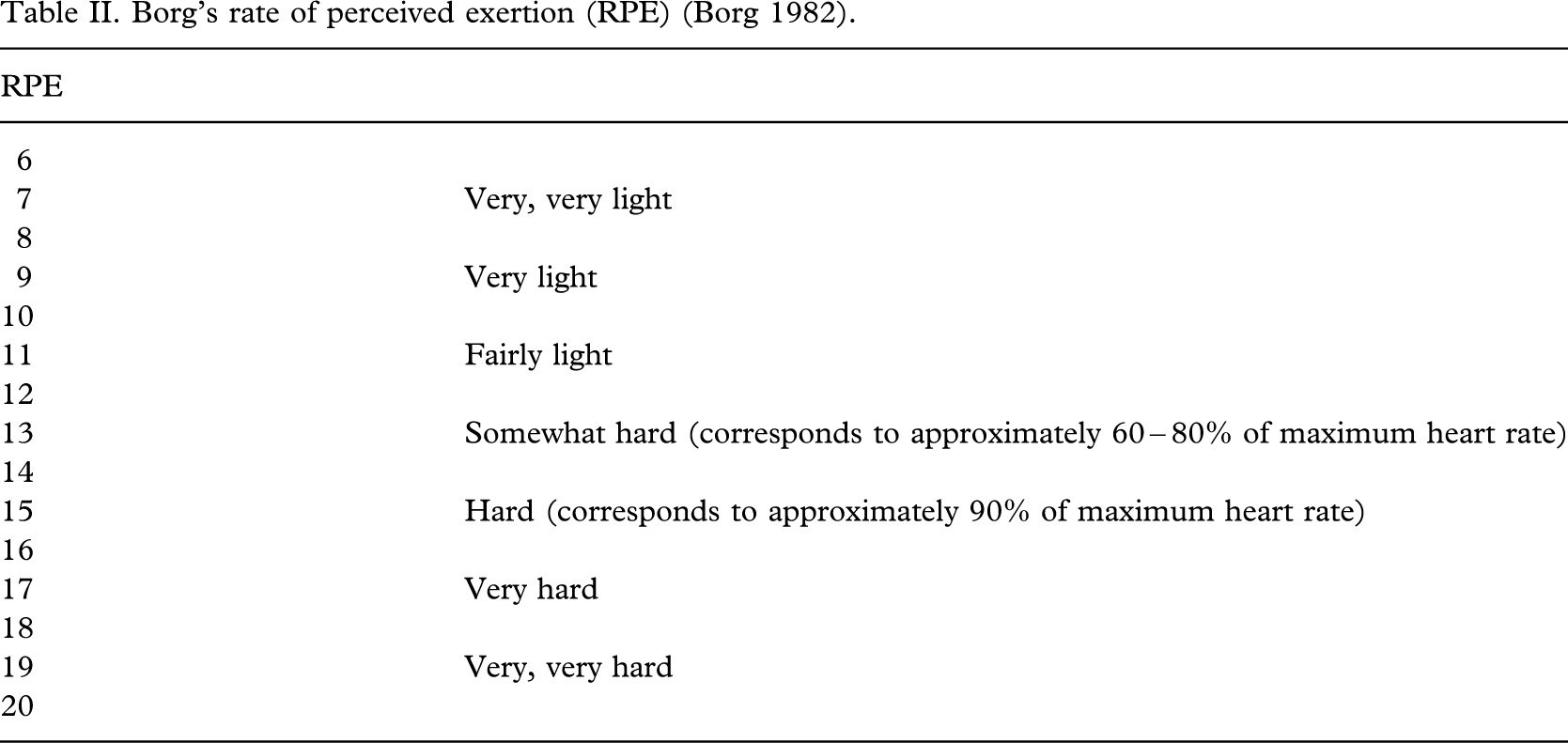
The aims of this study are: (i) To determine the physiological cost of walking, and (ii) to record basic stride characteristics in a sample population of BA with differing levels of amputation. It is hypothesized that of all lower-limb amputees, bilateral transfemoral amputees (TF/TF) will experience the greatest physiological costs during walking, simply because they have lost the greatest proportion of tissue and are likely to walk at the slowest speeds. The objectives are to quantitatively assess aspects of gait in each individual walking for a set duration (2, 4 or 6 min) at their self-selected walking speed whilst wearing the prostheses that they have been rehabilitated with. Each individual's perceived exertion levels (Borg 1982) during the walking test will be measured and a self-assessment questionnaire, adapted from Boonstra et al. (1996), investigating their perceived walking ability will also be completed.
Subjects and methods
Ten male individuals with bilateral amputations participated in this study. Apart from their amputations, each individual was to be healthy with no other relevant medical problems or disabilities. Eight BA were recruited from The Royal National Orthopaedic Limb-Fitting Centre (RNOH Stanmore, UK) and a further two were selected from the Preston Limb-Fitting Centre (Disablement Services Centre, Preston, UK). Two had transtibial/transtibial (TT/TT) amputations and wore full-length prostheses (FLPs), three had transfemoral/transtibial (TF/TT) amputations and wore FLPs, two had transfemoral/transfemoral (TF/TF) amputations and wore FLPs, one had bilateral knee disarticulations (KD/KD) and wore FLPs, one had TT/TF and wore short non-articulating pylon prostheses (SNAPPs) and one had TF/TF amputations and wore SNAPPs. Subject data including prosthetic type/design are summarized in Table I. The mean age of the amputees was 40.5 years (±11.9 years) with a range of 26 – 59 years. To enable comparison with able-bodied gait, a non-amputee (NA) control group matched for gender and age was also examined.
Subject data, amputation levels and type of prostheses.
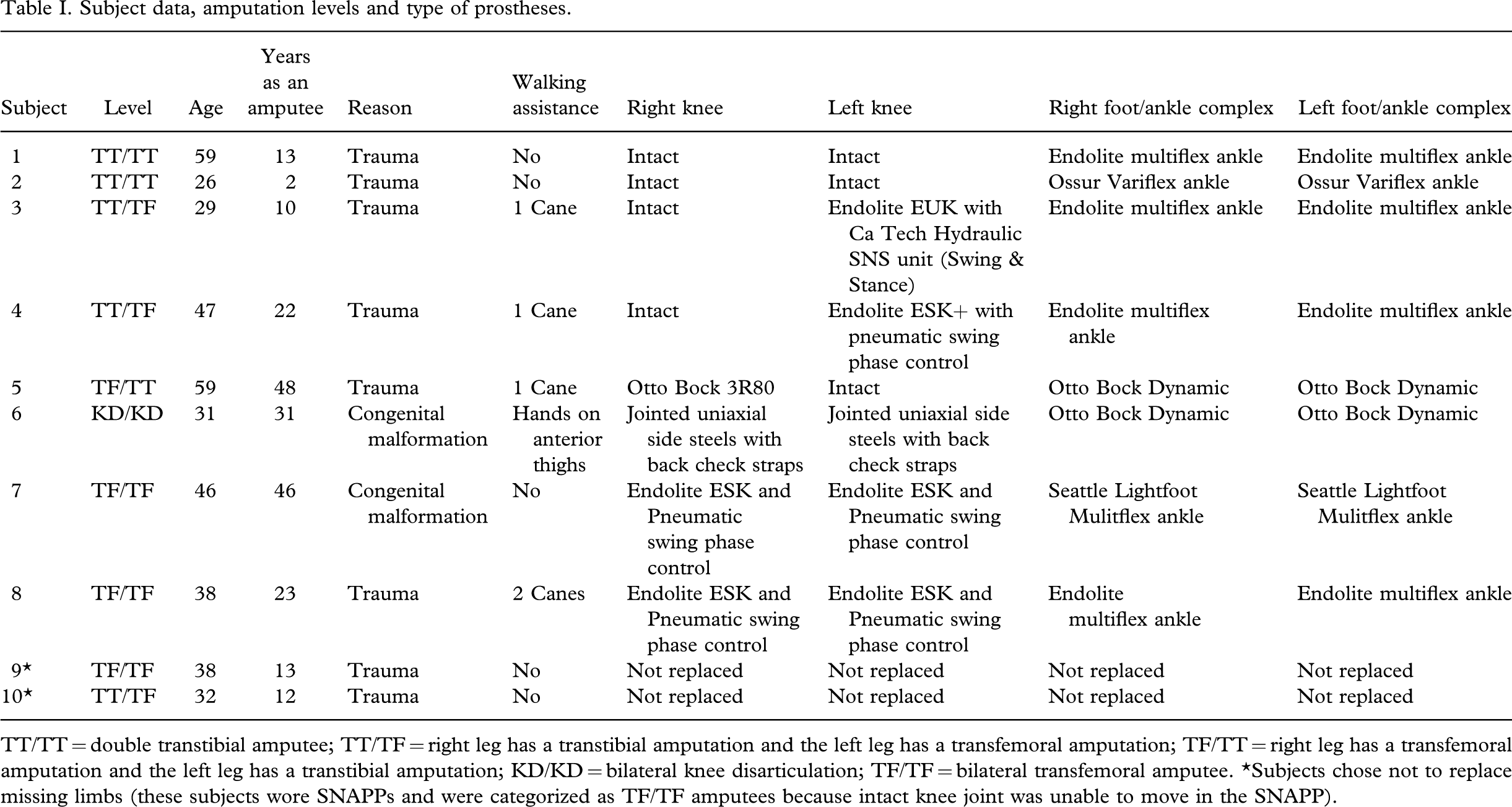
TT/TT = double transtibial amputee; TT/TF = right leg has a transtibial amputation and the left leg has a transfemoral amputation; TF/TT = right leg has a transfemoral amputation and the left leg has a transtibial amputation; KD/KD = bilateral knee disarticulation; TF/TF = bilateral transfemoral amputee. ∗Subjects chose not to replace missing limbs (these subjects wore SNAPPs and were categorized as TF/TF amputees because intact knee joint was unable to move in the SNAPP).
Experiments were undertaken in the morning and all subjects had a light breakfast (i.e., cereal/toast and a hot drink) several hours before testing. The subjects wore their own prostheses and walking stick use (if required) was permitted. The Ethics Committee at the Royal National Orthopaedic Hospital (Stanmore) and Brunel University granted ethical approval for the study. Subjects were required to attend a single testing session. Initially, subjects completed a questionnaire relating to their perceived walking ability at normal speeds. The questionnaire was based on multiple-choice questions (see the Appendix). Low scores (6 was the lowest) indicated that the amputee perceived their walking ability to be ‘excellent’ and high scores (28 was the highest) indicated that walking was ‘impossible’. Subjects were asked to walk for 6 min without stopping, but a 2- or 4-min option was also offered for those who were not confident in walking for 6 min non-stop. Only amputees 9S-TF/TF and 10S-TF/TF (wearing SNAPPs) chose to walk for 6 min, all remaining amputees selected the 2-min option. Subjects were instructed to walk at their normal walking speed. To avoid sharp turns, a 30 m circular level walkway was demarcated in the gait laboratory. Subjects were free to stop or abandon the test if needed. In order to directly compare data between the amputees, gait parameters were only recorded during the first 2 min of exercise (however long they chose to walk for): time to complete 30 m, exercise heart rate (with a Polar heart rate monitor), perceived level of exertion (Borg 1982) and number of steps taken over a 30 m stretch. Later, walking speed, cadence (number of steps per minute), step length (left initial contact to right initial contact), body mass index (BMI), exercise intensity and physiological cost index (PCI) were calculated. A detailed description of each parameter is provided below.
Basic gait parameters
The physiological cost index (PCI; Butler et al. 1984) is a reliable estimation of metabolic energy
expenditure (Bailey and Ratcliffe 1995). PCI was calculated as follows: 

Borg's rate of perceived exertion (RPE) (Borg 1982)
Results
The NA controls compared well with previously published data on non-pathological gait (Hamill and Knutzen 1992; Winter 2005) and their data were therefore used in a comparison with the bilateral amputee data. The NA controls generally had relatively fast walk speeds, long step lengths, low PCIs and EIs compared to BA. The NA also had the lowest RPE and PWA scores compared to BA wearing FLP. Physiological parameters and gait characteristics are provided in Table III; the subjects are ordered according to mean walking speed from top (fastest, 2TT/TT at 1.3 ms−1) to bottom (slowest, 8TF/TF at 0.68 ms−1). Subjects walking at the fastest mean speeds (e.g., NAs, and amputees 2TT/TT and 1TT/TT) had both a relatively long step length and a high cadence. Subjects walking at the slowest speeds (amputees 6TF/TF and 8TF/TF) had a relatively short step length and/or slow cadence. With the exception of amputees 1TT/TT and 4TT/TF, exercise heart rate was always greater (>80 bpm) than the mean of the NA. In amputees 6TF/TF and 8TF/TF slower walking speeds did not result in lower exercise heart rates.
Physiological parameters and stride characteristics during walking in BA and NA controls
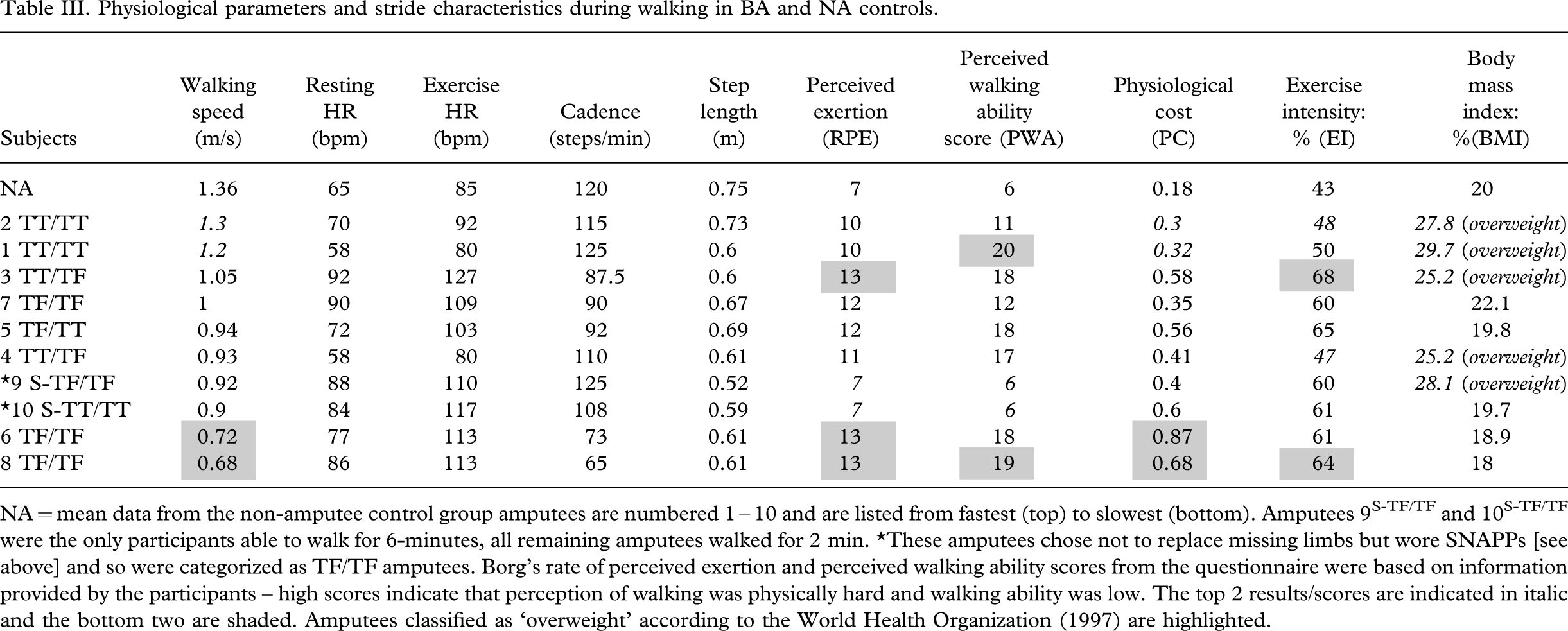
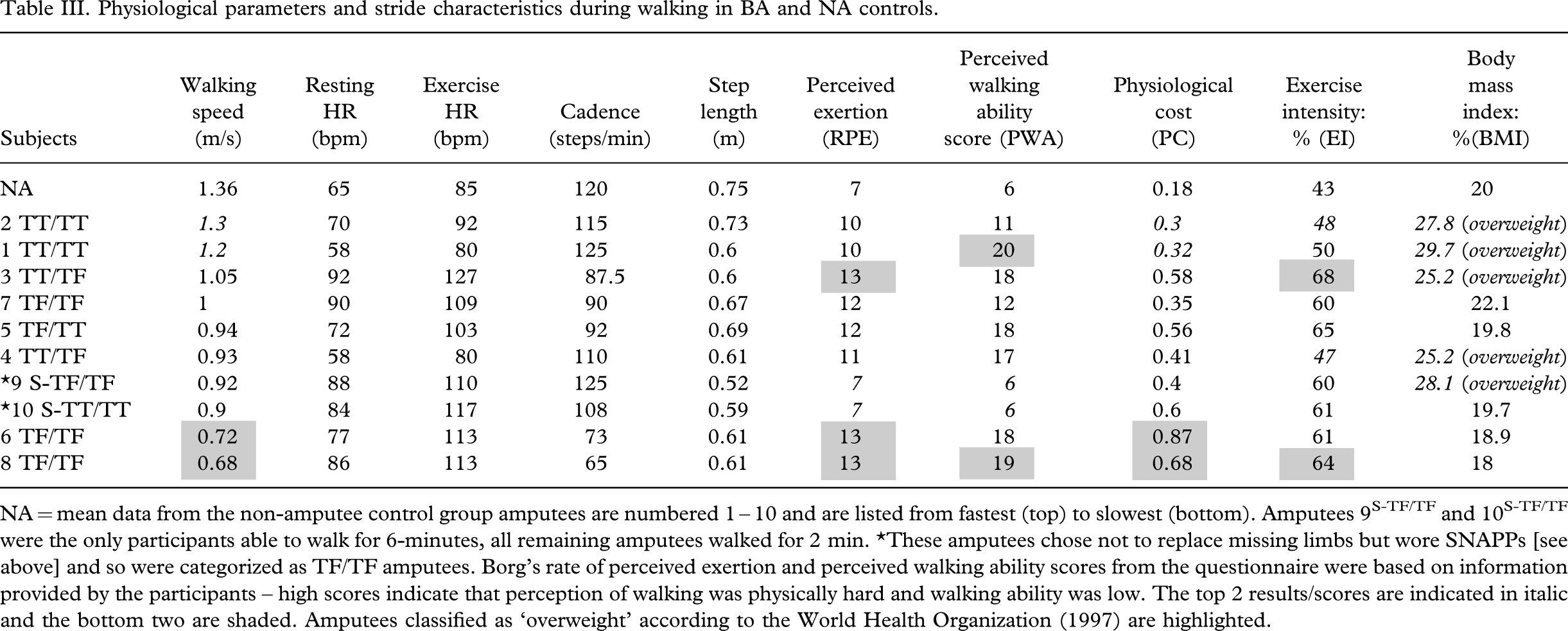
For all BA, the physiological costs (PCI) of walking and exercise intensity (EI) were greater than those calculated for the NA controls (Table III). Yet, there was no definite pattern between the amputees and we did not necessarily observe the greatest PCI and EI in the amputees with bilateral TF amputations (Table III). Amputees 6TF/TF, 8TF/TF, 3TT/TF and 5TT/TF had poor perceptions of their walking ability and reported the test to be ‘somewhat hard’ on the Borg scale of perceived exertion, which were matched with high values of PCI and/or EI (Table III). This relationship between walking perception and physiological cost was also observed in amputees 2TT/TT and 7TF/TF. Others (amputees 1TT/TT and 4TF/TF) had lower levels of EI and PCI with high RPE or poor PWA scores, whereas amputees 9S-TF/TF and 10S-TF/TF (who walked with SNAPPs) had higher physiological costs, yet perceived walking ‘very, very light’.
Discussion
This study provides novel data on the diversity in step characteristics, physiological costs and perception of walking in people with differing levels of bilateral amputations when compared with walking in a NA control group. All BA studied here had undergone prosthetic rehabilitation and were considered by their limb fitters to be successful walkers. The data revealed that in a (relatively small) group of BA, walking speeds, exercise intensities, exercise heart rates and perceptions of walking ability/performance were highly variable and not necessarily linked to levels of amputation (i.e., TT/TT, TT/TF and TF/TF).
Walking speed
Amputees were instructed to walk at a self-selected walking speed, which was in all cases, as expected, slower than the mean speed of the NA control group (see Table III). It was hypothesized that walking speed would decrease as the level of amputations increased. This hypothesis was only partially accepted as although amputees 2TT/TT and 1TT/TT had the lowest levels of amputations and walked at the fastest speeds, the remaining amputees all walked at a range of speeds (from 1.05 and 1.00 m/s in amputees 3TT/TF and 7TF/TF to 0.68 m/s in amputee 8TF/TF), which could not be related to level of amputations or type of prostheses worn (i.e., type of FLPs or SNAPPs, Table III). Similar to non-pathological gait (Sutherland 1997; and data collected from the authors' NA control group), in this study's BA, walking speed was linked to both cadence and step length. Amputees with the fastest walking speeds used either a long step length and/or a fast cadence. BA may therefore select walking speeds for reasons other than or in addition to the level of their amputations such as walking situation and cardiovascular fitness levels.
Physiological cost and exercise intensity
In previous work, both bilateral and unilateral amputees were found to reduce their chosen walking speed so that their physiological energy costs are comparable with able-bodied individuals (Huang et al. 1979; Gonzalez and Corcoran 1994). The present study did not observe this relationship (Table III). Of the BA tested, the authors expected those with bilateral TT amputations to have the fastest gaits with lower levels of physiological cost, because they have fewer joints and musculature missing compared to those with TF amputations. With the exception of amputee 2TT/TT, this relationship was not observed in our study: Although all EI and PCI scores were greater (up to 5-fold) in BA when compared to NA, the data were varied between amputees and differences could not easily be related to either level of amputations or type of prosthetic design (Table III). There are several possible reasons for this. Firstly, it is generally assumed that a symmetric gait is energetically most efficient (Waters and Mulroy 1999; Mattes et al. 2000). In this study, disjointed gait patterns were common, which could be a cause of high PCI and EI. Assistive gait may also have increased energy expenditure in amputees 3TT/TF, 6TF/TF and 8TF/TF (Christensen 2002; Chen et al. 2004). Furthermore, increased body weight caused by a sedentary lifestyle can affect the respiratory, cardiovascular, muscular and metabolic systems (Waters and Mulroy 1999). Overweight/obese walkers will experience elevated rates of oxygen consumption which can be greater than those recorded in fast walking in normal adults (i.e., decrease the individual's maximal aerobic capacity – VO2 max (Saltin et al. 1968; Bassey et al. 1971; Mattsson et al. 1997). The amputees studied here reported a decrease in physiological activity since undergoing amputations, and half of the group (1TT/TT, 2TT/TT, 3TT/TF, 4TT/TF and 9S-TF/TF) are medically classed as ‘overweight’ (World Health Organization 1997) (see Table III). Stewart and Jain (1992) found that cardiovascular disease (associated with obesity) is a major cause of premature death among amputees. To help reduce this risk, a loss of just 20% body weight has shown to reduce the rate of oxygen consumption during walking by approximately 30% (Foster et al. 1995). Improved locomotion function could improve cardiovascular health in BA and could by extension help reduce the risk of premature death caused by obesity.
Walking perception
Perceived exertion is related to the physical sensations (e.g., increased heart rate, increased respiration or breathing rate, increased sweating, and muscle fatigue) experienced during walking. Although this is a subjective measure, a person's exertion rating has been shown to provide a fairly good estimate of the actual heart rate and level of exercise intensity during physical activity (i.e., RPE level 13 corresponds to approximately 60% of maximum EI) (Borg 1998). The authors also observed this relationship in 6 of the 10 BA (2TT/TT, 3TT/TF, 5TF/TT, 6TF/TF, 7TF/TF and 8TF/TF). However, amputees 1TF/TT and 4TF/TF had high RPE with low PC/EI, and amputees 9S-TF/TF and 10S-TF/TF had high PC/EI with low RPE. This would suggest that psychological factors (walking confidence, self belief, motivation etc.) could be very important in gait performance. The bilateral amputees studied here found walking challenging; eight of the ten subjects chose the shortest duration (2 min) walk test and five were clinically overweight. Thus it is perhaps not surprising that a high proportion of BA eventually abandon their limbs in favour of a wheelchair, become increasingly less active and are less likely to lead independent lifestyles. The link between psychology and physical performance needs further investigation if one is to tackle problem gait in amputees.
The amputees wearing SNAPPs (9S-TF/TF and 10S-TF/TF) were the most confident walkers with the highest levels of PWA and the lowest RPE (similar to the NA results see Table III). This could be because SNAPPs do not replace the missing distal limb and thus the amputee has a lower centre of gravity and is likely to feel more stable than the FLP- wearing amputees. Both SNAPPs amputees were also ex-army soldiers and were extremely active and highly motivated pre-amputation and might have been more able and determined (both physically and psychologically) to withstand the added physiological costs of walking post amputation. In previous studies, (Wainapel et al. 1985; Crouse et al. 1990; Wu et al. 2001; Perry 2004) the physiological energy cost, metabolic energy expenditure and heart rate during walking was found to be lower in amputees when they wore SNAPPs compared to FLPs. The authors were unable to compare gait in amputees walking in different prosthetic designs (i.e., FLPs versus SNAPPs) because changes in prosthetic design are often accompanied by changes in limb/stump morphology so that other/old prostheses no longer fit. In fact, a SNAPP-wearing amputee was excluded from this study at its inception as he lost a significant amount of weight after their adoption and could not wear the limbs until they had been re-fitted. The results obtained in this study and those reported elsewhere in case studies (Wainapel et al. 1985; Crouse et al. 1990; Wu et al. 2001; Gitter et al. 2002) suggest that SNAPPs can offer practical benefits for those BA experiencing difficulty in ambulating with FLPs or those permanently confined to a wheelchair. Further research is needed to quantify the mechanical, physiological and energetic advantages and disadvantages of this design.
Amputees 2TT/TT and 7TF/TF perceived their walking ability to be ‘good’ and were the most confident of the amputees walking in FLPs. In the case of amputee 7TF/TF this is likely because his legs were amputated at birth. Amputee 2TT/TT was a confident walker, had one of the lowest exercise heart rates, walked the fastest and had the lowest physiological costs in spite of having the most recent amputations (2 yrs). This was likely due to his age (26 yrs) and his reported high activity levels. Low physiological costs can be linked to the fact that he was the only amputee to wear energy-storing prosthetic feet (Ossur Variflex™ foot). The construction of Variflex™ feet provides dynamic function and allows energy to be stored through compression during heel contact and early stance with subsequent energy release during late stance and push-off. Such designs aim to mimic the missing ankle-foot complex and associated muscle-tendon function. They have previously been shown to lower physiological costs of gait, and our results would support this (Nielsen et al. 1988). Psychological factors may have played an additional role here. Klute and colleagues (2002) showed that energy-storing/releasing feet lessen the magnitude of stress going through the residue limbs and improved comfort during walking. Hence, feeling comfortable when walking lowers EI levels and reduces exercise HR (see also Huang et al. 1979; Garvin et al. 2001).
The present study's results highlight the diversity in locomotor performance within this sample population. Some BA cope very well with the added physiological demands of prosthetic walking, whilst others find this task somewhat difficult (for some it was almost unmanageable). Further research examining the functionality of the different FLPs currently available to NHS patients would help us to identify markers of successful rehabilitation and also could help uncover the reasons behind prosthetic limb abandonment.
In conclusion, BA (regardless of level of amputations and type of prosthetic design) did not reduce their walking speed to the extent that physiological costs matched those of the NA control group as has previously been reported. BA with similar levels of amputations, reasons for amputations and prosthetic design had varying physiological costs, step characteristics and differing levels of perceived walking ability. So much so, that the authors felt that it would have been inappropriate to group and compare these amputees solely on their level of amputations and type of prosthetic design (SNAPPs or FLPs). However a relationship was found between walking perception and physiological cost in over half of the group (i.e., high RPE and poor PWA matched high PCI and EI). Yet, in the rest of the group amputees had either low RPE or good PWA with high PCI and EI, and visa versa.
Amputees wearing SNAPPs had the lowest levels of perceived exertion and better perceptions of walking ability when compared to BA with the same levels of amputations walking in FLPs. SNAPPs could potentially help non-mobile amputees increase activity levels and hence aid weight loss. Further research investigating the physiological and psychological factors (and their interplay) affecting walking performance is needed in order to gain a better understanding of the problems encountered in BA gait.
Footnotes
Appendix
Questionnaire: Walking Ability Rating (adapted from Boonstra et al. 1996).
Trial with SNAPPs Trial with FLP
The right limb is TF TT
The left limb is TF TT
Questions for normal walking
I am able to walk without a rest: 5. Less than 50 m 4. Between 50 and 500 m 3. Between 500 and 2,000 m 2. Between 2,000 and 5,000 m 1. More than 5,000 m Never Only when walking a long distance or on uneven ground Usually Always I never walk outside 5. Less than 5 mins 4. Between 5 and 15 mins 3. Between 15 and 30 mins 2. Between 30 and 60 mins 1. Longer than 60 mins Never Sometimes Usually Always Never Sometimes Usually Always Never Only while walking a long distance on uneven ground Usually Always I never walk outside
I have to be careful not to fall when walking outside:
I an able to walk without a rest:
I use a walking cane or crutch or support myself on pieces of furniture or some
other support while walking inside:
I use a walking cane or crutch or some other support or I walk supported by
someone else while walking outside:
I have to be careful not to stub the foot of the prosthesis on uneven ground:
Score for normal walking: 6 means has excellent ability to ambulate, 28 means does
not have the ability to ambulate