
Abstract
The primary objective was to test the hypothesis that walking with a shock-absorbing pylon (SAP) decreases the peak magnitude and frequency content of the heel-strike-initiated shock wave transmitted to the stump. The secondary hypotheses were that walking with a SAP decreases the heel-strike transient force between the ground and the foot and increases function as measured by walking velocity and subjective assessments. Seven people with unilateral trans-tibial amputations walked at self-selected speeds without and with a SAP. As the primary outcome measure, accelerometers were used mounted proximally and distally along the prosthetic pylon to measure the transmitted shock wave. Secondary measures included ground reaction forces from a force plate, a ten-minute walking test to determine walking speed and a questionnaire to evaluate gait function and subjective preference. The SAP provided no significant shock absorption as indicated by either the mean peak proximal accelerations of 3.19 g and 2.82 g (p = 0.28) without and with the SAP respectively or the mean difference between the peak proximal and distal accelerometers, 0.16 g and 0.19 g (p = 0.58). No significant change in the frequency content was found. Variances were high. There were no significant differences noted in the secondary measures. Although this study failed to identify any statistically significant effects due to the SAP, the magnitude and variance of the data will permit an accurate estimation of the appropriate sample size for future studies required to determine the efficacy of SAPs.
Keywords
Introduction
Shock-absorbing pylons (SAPs) are intended to provide people with lower-limb amputations with shock-absorption during walking, running and other high impact activities. Gard and Konz (2003) speculated that the reason people with lower-limb amputations walk slowly is to reduce impact forces. During gait, heel-strike transient forces are generated as the heel makes initial contact with the ground. The result of this is that a shock wave (also referred to as a transient acceleration) is transmitted along the skeletal system (Whittle 1999). It has been suggested that the magnitude and rate of loading of the lower limb is linked to degenerative joint diseases (Collins and Whittle 1989). With amputation of the foot and part of the tibia, components of the natural shock absorbers of the lower limb are lost.
The impact of heel-strike transient forces on the body during gait and the effect of interventions have been quantified through the use of force plates and accelerometers attached to the body (van Jaarsveld et al. 1990; van Leeuwen et al. 1990; Shorten and Winslow 1992; Lafortune et al. 1996; Voloshin 2000; Derrick et al. 2002; Gillespie and Dickey 2003; Folman et al. 2004). The heel-strike transient force, as measured by a force plate, can be visually identified as a short duration spike superimposed on the upslope of the vertical ground reaction force (GRF) shortly after impact (Whittle 1999). The magnitude and rate of loading of such heel-strike transient forces have been shown to decrease (10 – 35%) when walking with shock-absorbing materials between the foot and ground (Lafortune and Hennig 1992; Gillespie and Dickey 2003; Folman et al. 2004). Reductions in heel-strike transient shock waves along the prosthetic pylon (7 – 40%), as measured by mounted accelerometers, were seen with different prosthetic feet and with wearing sneakers in individuals with trans-tibial amputations (van Jaarsveld et al. 1990; van Leeuwen et al. 1990). An increase in the magnitude of the power spectrum density (PSD) was seen between frequencies of 6 and 30 Hz when comparing SACH feet to Multiflex feet (van Leeuwen et al. 1990).
Few studies have quantitatively studied the effect of SAPs on gait. People with trans-tibial amputations were found to have a significant decrease in energy expended as measured by oxygen consumption (5 – 9%) with the addition of a SAP during treadmill walking at speeds above normal (Buckley et al. 2002). Few kinematic and kinetic differences were seen with people with trans-tibial amputations with or without a SAP. A reduction in the magnitude of the heel-strike transient force, as measured by a force plate, was the most consistent change but not significant across all subjects and walking speeds, with the addition of the SAP (Gard and Konz 2003). No study to date has directly measured the transmission of heel-strike transient shock waves along the prosthesis to determine if, with the addition of the SAP, the magnitude of shock is diminished.
The primary objective was to test the hypothesis that walking with a shock-absorbing pylon (SAP) decreases the peak magnitude and frequency content of the heel-strike transient shock wave transmitted to the stump. The secondary hypotheses were that walking with a SAP decreases the heel-strike transient force between the ground and the foot and increases function as measured by walking velocity and subjective assessments.
Methods
Participants
A sample of convenience, 7 participants (6 males, 1 female) with an age range from 16 – 38 years old (median 33 years) was studied. A statistical power analysis to estimate sample size required to obtain statistically significant differences was not possible because data magnitude and variability were not known. All subjects were people with trans-tibial amputations and had experience using their prostheses for 2 – 29 years (median 15 years). One subject had a congenital amputation, 5 subjects had traumatic amputations, and 1 subject had an amputation due to cancer. All subjects were able to ambulate independently in the community with 5 of the participants functioning at a US Medicare Functional Classification Level (MFCL) of K3 and 2 of the participants functioning at a K4. The MFCL is a 5-level classification system which is used to describe a lower-limb amputee's level of ambulatory function from no ability or potential to ambulate to having ambulation ability or potential that exceeds basic skills, K0 to K4 respectively (HCFA Common Procedure Coding System 2001).
Study design
Cross-over, within-subject comparisons were used. Two conditions were measured, with and without a SAP, the latter referred to as the pylon-only condition (pylon). The two measurement sessions occurred within one day of each other. Because this was a pilot study, the condition order was not randomized and was selected based on convenience, pylon before SAP for all subjects but one. There was no attempt to blind the tester to condition.
Ethical issues
The Research Ethics Board of the Queen Elizabeth II Health Sciences Centre approved the study. Participants provided their informed consents.
Recruitment and screening
Participants were either inpatients or outpatients of the Queen Elizabeth II Health Sciences Centre Amputee Service based at the Nova Scotia Rehabilitation Centre Site. Participants met the inclusion criteria of having had a unilateral transtibial amputation, being able to walk comfortably for a minimum of 10 min without aids or assistive devices, and having a physician's permission to participate. Participants were excluded if the SAP could not be adapted to fit their current prosthesis configurations or if their weights exceeded the recommended maximum for the SAP.
Prosthetic considerations
The prosthesis of each participant was modified so that the straight pylon portion of the prosthesis could be removed and replaced with a pylon that contained a shock-absorbing device, the Seattle AirStance (Seattle Systems, Poulsbo, WA, USA). The Seattle AirStance utilizes pressurized air to provide longitudinal shock absorption for people with a mass up to 136 kg. Although this specific model is no longer manufactured, it is representative of a class of similar devices. The SAP was adjusted based on body weight and recommendations of the manufacturer. The addition of the shock absorber did not alter the alignment of the prosthesis. The subjects wore their usual footwear, which remained constant between conditions. The type of prosthetic foot and suspension system differed among the subjects, but this was not considered to be a problem for the within-subject comparisons planned.
Heel-strike transient shock wave
Two small, low mass uniaxial piezoresistive accelerometers (Endevco Model 7265A, Range 0 – 100 g, mounted resonant frequency 2700 Hz) were used to record the accelerations of the heel-strike transient shock waves along the prosthetic pylons. The accelerometers were each mounted on an aluminium device, which enabled the accelerometers to be attached to the bottom of the pylon and below the SAP (if present) and to the proximal prosthetic socket while allowing the measurement axis of the accelerometer to be visually aligned parallel to the long axis of the pylon. Calibration of the accelerometer was performed prior to testing by turning the prosthesis over, providing a measurement range of 2 g. Signals from the accelerometer were conditioned prior to sampling using an Endevco piezoresistive preamplifier (Model 106). A Kistler force plate (Type 9281B) positioned along the walkway was used to obtain the GRF. Subjects were allowed to warm-up and determine a comfortable walking speed as they walked a 20 m distance prior to testing. During testing, each subject completed five trials for each condition.
The two accelerometer signals and three components of the GRF measured by the force plate were simultaneously sampled at 1000 Hz for 10 sec. A high sampling rate was chosen to ensure the higher frequency components of the heel strike transient force were recorded (Voloshin et al. 1985).
A single stance phase of gait was extracted from the accelerometer data recorded for each trial. Heel-strike was identified as the point when the vertical GRF first exceeded a threshold of 10 N. Toe-off was identified as the point after heel-strike when the GRF first decreased below a threshold of 10 N. To ensure the data extracted for analysis contained the heel-strike transient force, the data window extracted contained information 75 ms prior to heel-strike and 75 ms after toe-off.
The vertical GRF was analyzed and the initial peak force (IPF) and force loading rate (FLR) were calculated for the heel-strike transient force of each trial. IPF was calculated as the first peak vertical ground reaction force (GRF) occurring after heel-strike as illustrated in Figure 1. FLR was calculated using a method similar to that used by Lafortune and Hennig (1992) incorporating the following formula:
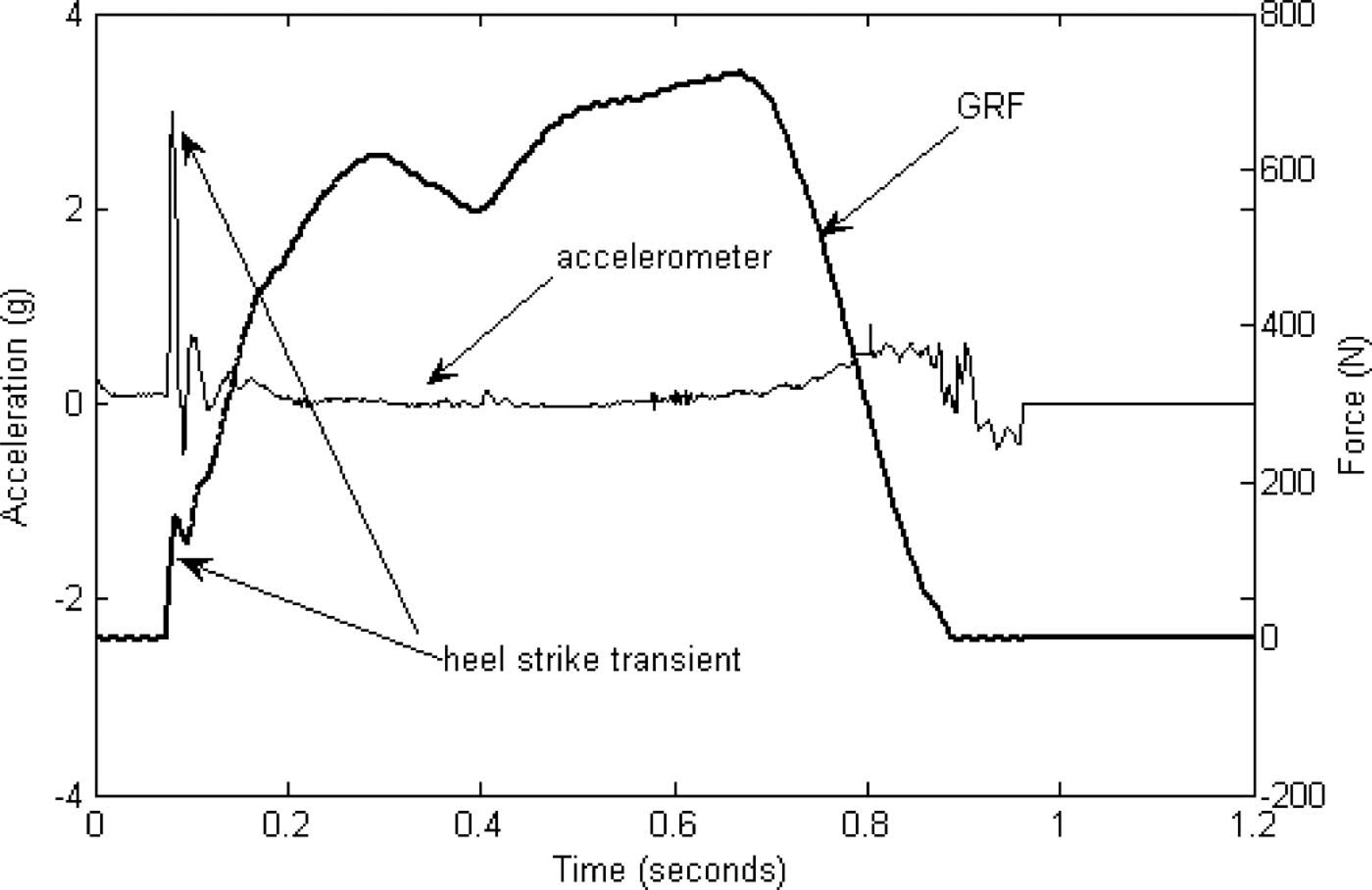
Typical distal accelerometer recording and vertical ground reaction force (GRF) for one stride of gait.
Because the piezoresistive accelerometers respond to the steady state effects of gravity, the accelerometer data was corrected for the effects of gravity to obtain representative dynamic accelerations. It was assumed that the lower leg was near vertical during the stance phase. The mean offset due to gravity was calculated at the start of each trial during quiet standing, as has been done in other studies (Ledoux and Hillstrom 2001; Wakeling et al. 2003). Peak amplitudes were extracted from the first 50% of the stance phase as only heel-strike information was of interest, and peak values were averaged across trials. The difference between the readings of the distal and proximal accelerometer was calculated and averaged across trials as a measure indicative of the amount of the heel-strike transient shock wave attenuated by the SAP or along the length of the pylon.
The accelerometry data were also analyzed to determine the frequency content of the transient shock wave. Because the piezoresistive accelerometers respond to the effects of gravity, there was a linear trend offset present in the data that had to be removed prior to calculating the PSD. The mean value and any linear trends during the entire stance contact phase were removed to avoid bias in the resultant PSD. The PSD was calculated for the accelerometer data, for the entire stance phase, using a 500 point discrete Fourier transform (DFT) providing a resolution of 2 Hz. Each accelerometer dataset was padded with zeros to obtain the appropriate data length of 500 points. The PSD was adjusted to account for differences in the amount of zero padding and length of the original acceleration data set using a method similar to Shorten and Winslow (1992). The mean (MNF) and median (MDF) frequency of the PSD were found for each trial using a method similar to a previous study (Voloshin et al. 1998). The MNF and MDF are commonly used parameters in electromyography signal processing, and were chosen since they reflect the typical frequency of the transient shock wave (Ritter et al. 2005). Although only the heel-strike transient was of interest, the entire stance phase of gait was analyzed for the frequency content. This was done to allow comparison with previous studies (Shorten and Winslow 1992; Voloshin et al. 1998). It was assumed that most of the movements during stance and toe-off would be of low frequency as compared to the impact of heel-strike and that any changes in the high frequency content would be due to impact-related changes and subsequently reflected in the MNF and MDF values.
Subjects' results were averaged for five trials and for each condition. All data processing was done using conventional DFT and statistical routines in Matlab (The Mathworks Inc.) version 6.5.1. In order to compare the SAP to pylon condition 2-sided paired t-tests (α level as 0.05) were used. Comparisons were similarly made between the SAP and pylon condition for the peak proximal accelerometer magnitudes, the difference between the proximal and distal peak accelerometer magnitudes, and the MNF and MDF of the proximal accelerometer. Comparisons were also made for the force plate measures of the IPF and FLR.
Gait function
The distance walked in 10 min was recorded along a 50 m length hall for each condition, allowing calculation of mean walking speed, as a representative functional measure. In order to compare the walking speeds in the SAP and pylon conditions 2-sided paired t-tests (α level as 0.05) were used.
Subjective perceptions
Each subject completed a questionnaire in which the prosthetic conditions were evaluated through the use of visual-analogue scales (VASs). Questions asked related to the pressure felt on the stump during gait, the weight of the prosthesis, shortening of the prosthesis during weight transfer and the spring or energy return provided by the prosthesis. Questionnaire group means were calculated for each question and reported descriptively.
Results
A typical accelerometer recording for one stride of gait is illustrated in Figure 1. Peak acceleration values obtained ranged from 2 – 5 g. A representative PSD (average ± 1 standard deviation) for the pylon and SAP conditions are illustrated for a representative subject in Figure 2. The peak power occurred between 2 and 12 Hz. A resonance phenomenon was noted between 10 and 60 Hz in all subjects. In Figure 2, this was seen in the pylon-only condition with a resonance phenomenon around 5, 13 and 40 Hz, and with the SAP distally with a resonance phenomenon around 5, 10 and 20 Hz. Group average results of the heel-strike transient shock wave, as measured by the accelerometers, are summarized in Table I. Both mean and median results are tabulated since the data could not be assumed to have a normal distribution due to the small sample size. There was no significant difference between the SAP and pylon conditions with respect to the mean proximal accelerometer signal magnitude, with mean values of 2.82 g and 3.19 g respectively (p = 0.28). No significant difference was found between the mean distal and proximal peak accelerations for the SAP and pylon condition, with mean differences of 0.19 g and 0.06 g respectively (p = 0.58). There were no significant differences in the mean and median frequency of the proximal accelerometer signals. The mean frequencies of the proximal accelerometer signals were 18.34 Hz and 15.61 Hz for the SAP and pylon conditions respectively (p = 0.31). The median frequency of the proximal accelerometer signals were 19.31 Hz and 20.63 Hz for the SAP and pylon conditions respectively (p = 0.57).
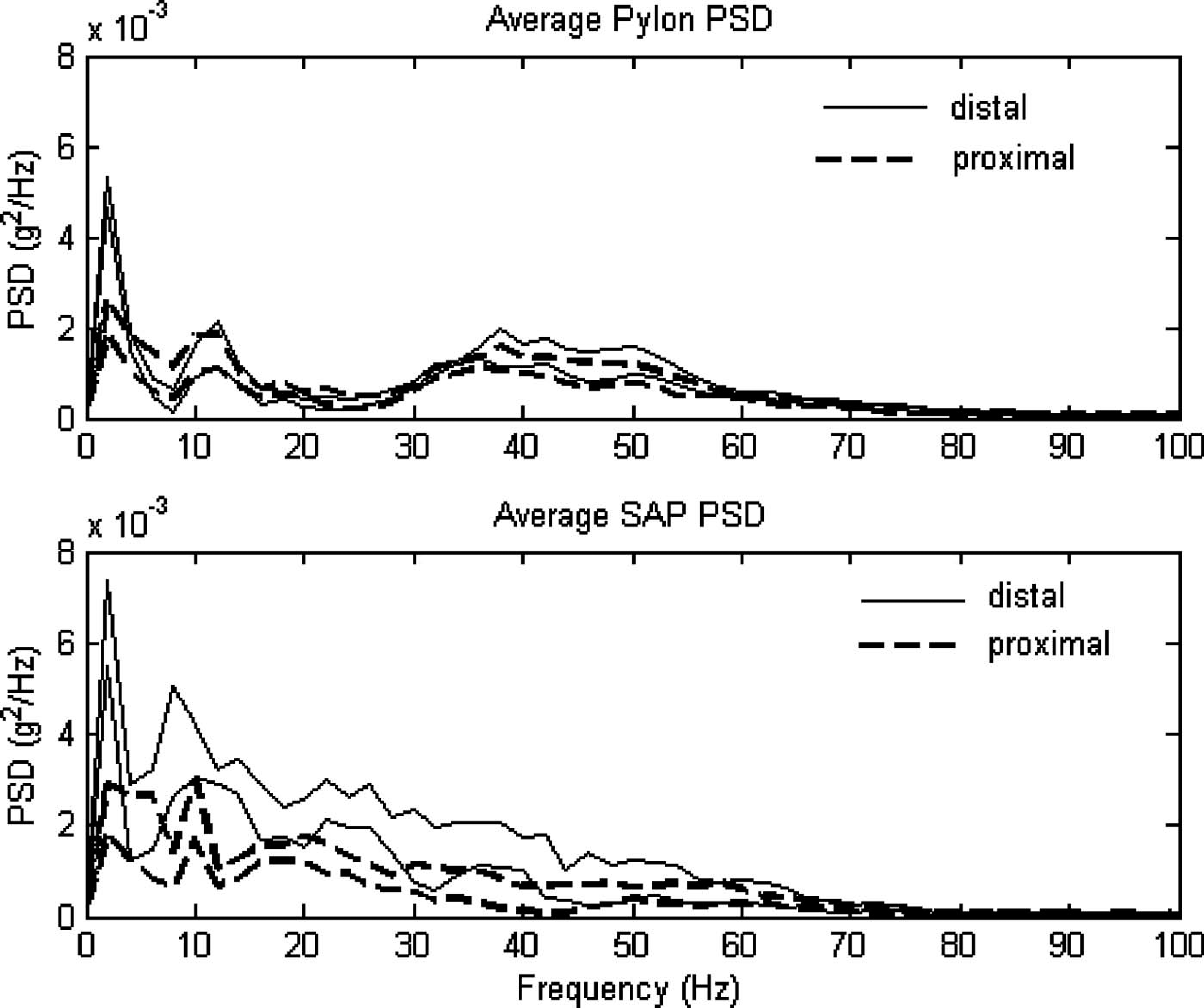
A representative power spectrum density (PSD) (average ± 1 SD) of the distal accelerometer (solid) and proximal accelerometer (dashed) with and without the SAP (SAP and Pylon, respectively).
Accelerometer measurement results.
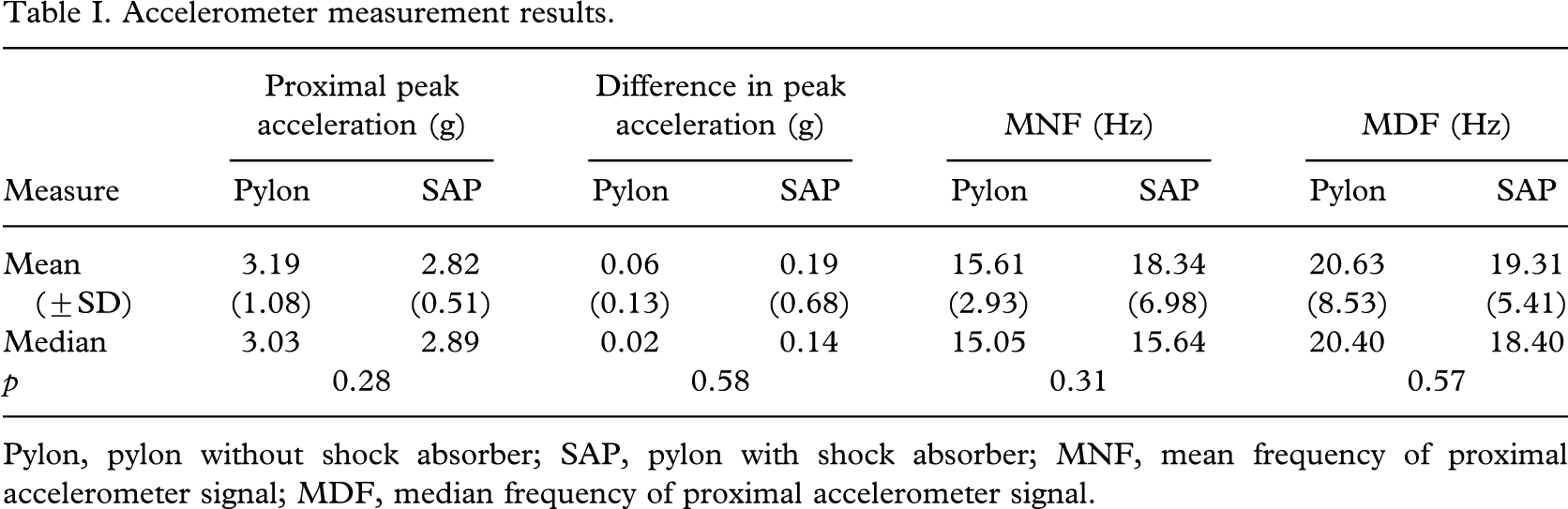
Pylon, pylon without shock absorber; SAP, pylon with shock absorber; MNF, mean frequency of proximal accelerometer signal; MDF, median frequency of proximal accelerometer signal.
The group average results of the force plate analysis, and 10-minute walking test are summarized in Table II. Not all subjects or all trials had a heel-strike transient superimposed on the vertical GRF. Because of this, the number of trials averaged per condition and subject ranged from one to five. There were no significant differences between the SAP and pylon conditions for the force plate data. Mean IPF of 0.14 BW and 0.13 BW were obtained for the SAP and pylon conditions respectively (p = 0.74).
Force plate and walking speed and distance results.
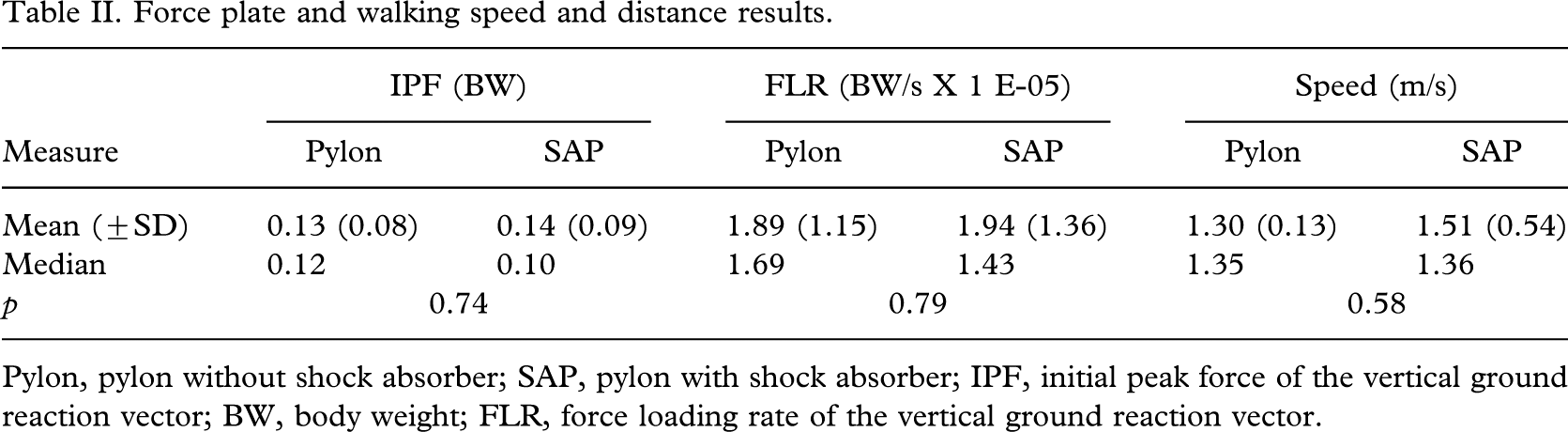
Pylon, pylon without shock absorber; SAP, pylon with shock absorber; IPF, initial peak force of the vertical ground reaction vector; BW, body weight; FLR, force loading rate of the vertical ground reaction vector.
The mean FLRs for the SAP and pylon conditions were 1.94 × 10−5 BW/s and 1.89 × 10−5 BW/s respectively (p = 0.79). The mean 10-min walking speeds were 1.51 m/s and 1.30 m/s for the SAP and pylon conditions respectively (p = 0.58). Questionnaire results were close between the SAP and pylon conditions with a slight decrease in pressure on the stump, increase in shortening during stance and increase of weight with the SAP. Questionnaire results are summarized in Table III.
Questionnaire results.
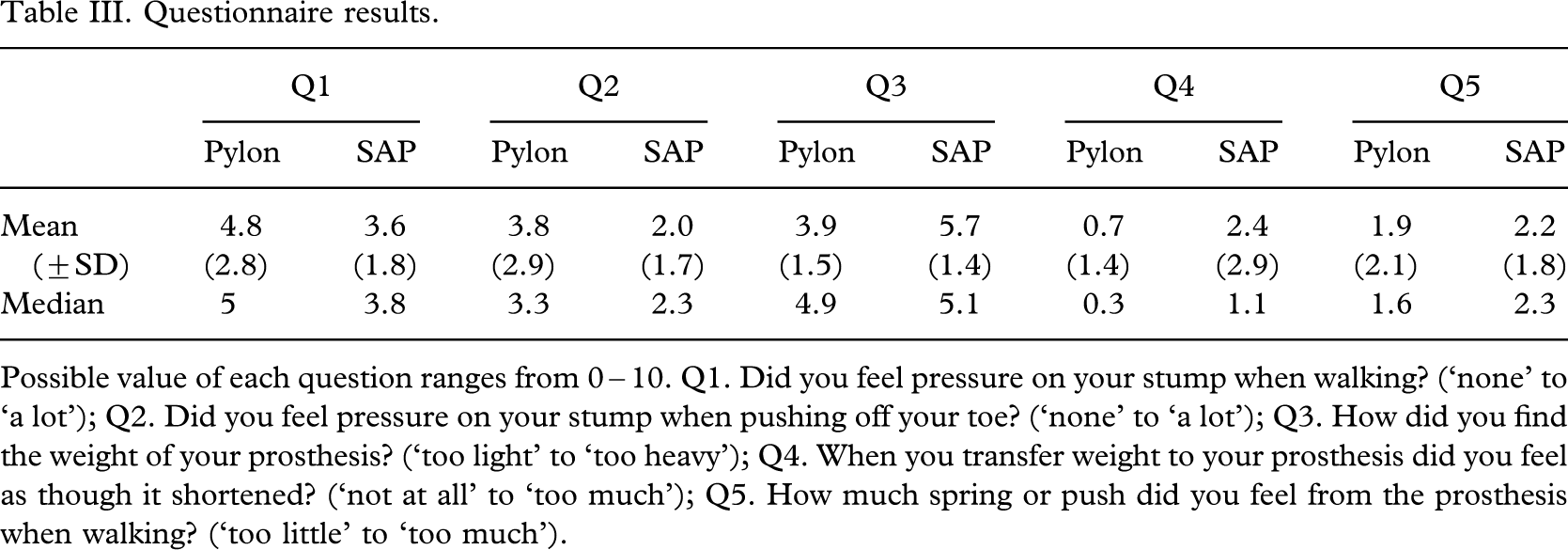
Possible value of each question ranges from 0 – 10. Q1. Did you feel pressure on your stump when walking? (‘none’ to ‘a lot’); Q2. Did you feel pressure on your stump when pushing off your toe? (‘none’ to ‘a lot’); Q3. How did you find the weight of your prosthesis? (‘too light’ to ‘too heavy’); Q4. When you transfer weight to your prosthesis did you feel as though it shortened? (‘not at all’ to ‘too much’); Q5. How much spring or push did you feel from the prosthesis when walking? (‘too little’ to ‘too much’).
Discussion
The primary objective was to test the hypothesis that walking with a shock-absorbing pylon (SAP) decreased the peak magnitude and mean and median frequency of the heel-strike transient shock wave transmitted to the stump. To do so, the transmission of the heel-strike transient shock wave along the prosthetic pylon was quantified through the use of accelerometers. Peak acceleration values obtained were similar to other studies (van Jaarsveld et al. 1990; van Leeuwen et al. 1990). The small number of subjects studied and the variability in the acceleration measurements obtained resulted in a study with limited statistical power and subsequently no statistically significant differences were found between the SAP and pylon peak acceleration conditions.
The frequency analysis used provided little additional insight. A resonance phenomenon in the PSDs was found similar to that obtained in previous research. Van Leeuwen et al. (1990) found a resonance phenomenon at approximately 30 – 40 Hz with the SACH foot and a series of resonance peaks with the Multiflex foot below 50 Hz. Van Leeuwen et al. (1990) found it difficult to isolate the heel-strike transient PSD information from the resonance of the prosthetic components. PSD peaks below 10 Hz would be reflective of the low frequency motion of the lower limb during the stance phase, and heel-strike would be reflected in the second PSD peak ranging from 10 – 30 Hz for running and walking (Johnson 1986; Whittle 1999; Wakeling et al. 2003).
Regarding the hypothesis that the SAP would reduce mean and median frequency of the heel-strike transient shock wave transmitted to the stump, this was not found when comparing the MNF and MDF. These may not have been the most appropriate measures to use due to the resonance frequencies present in the PSD, which differed across subjects, and this may have skewed the results. As more knowledge is gained on the impact of different frequencies of force on the skeletal system, a more systematic analysis approach should be used to determine the true benefits (if any) of the SAP and implications of the resonance frequency of the SAP and other prosthetic components on the skeletal system.
The secondary hypotheses were that walking with a SAP decreases the heel-strike transient force between the ground and the foot and increases function as measured by walking velocity and subjective assessments. No significant differences were noted for these measures. It was somewhat surprising to find that the heel-strike transient force superimposed on the vertical GRF was not always consistently present. This may be reflective of the gait variability of the population studied and the interactions of their footwear and prosthetic feet. The lack of consistency in this measure seems to indicate it would not be useful for future studies. Because the population studied had a high level of function, the difference in walking speed was difficult to detect. A more appropriate measure of function may be to measure the amount of physical activity or energy expenditure of participants and duration of prosthesis wear times over a longer time period, such as a week, with and without the SAP.
This study had some limitations. The acceleration magnitude has been shown to be dependent on walking speed and future studies should account for this (Voloshin 2000). Although the location of the accelerometers provided knowledge about whether the SAP provided an enhanced level of shock absorption, further insight would have been gained by studying the transmission of the heel-strike transient to the skeletal system through accelerometer measures at the sacrum or head. Problems have been noted in using Fourier analysis because it is not appropriate for non-stationary signals such as the heel-strike transient shock wave and errors can be produced (Gillespie and Dickey 2003). This method was used because Fourier transforms are so commonly used in other studies investigating the transmission of heel-strike transient forces. Finally, the study was a pilot study. In order to determine the effectiveness of SAPs to a prosthesis-user population, a larger study population, with randomized device order is required.
Future studies should include measurement of the transmission of the heel-strike transient shock wave to the skeletal system. Analysis of accelerometer measures will provide further understanding on the impact of the SAP, and its interaction with other components in terms of frequency and magnitude of shock attenuated or gained. The measurement of the heel-strike transient force with the force plate did not provide any useful information and it is recommended that this measure should not be used in future studies. Subjective perceptions should be included to determine if there is a device preference and the reason for any preference through open-ended questions or validated questionnaires. It is also recommended that the benefits to the overall function of people with amputations should be documented through studies of community-level activity over longer durations of time.
Conclusions
Although this pilot study had some limitations, this study was a first attempt to document the direct effect of SAPs on the transmission of the heel-strike transient shock wave along the pylon through the use of pylon-mounted accelerometers. Although, at best, a slight trend of a decreased peak proximal acceleration was found with addition of the SAP, it was not significant and indicates there may be little benefit of SAPs for level walking. Future studies are required to evaluate whether SAPs truly provide any additional benefit to people with transtibial amputations for everyday and high-level activities. The authors suggest that focus should be placed on the measurement of shock absorption by the SAP and the effect on the skeletal system through the use of prosthetic and body-mounted accelerometers, subjective perceptions, and activity measurement in the community.
Footnotes
Acknowledgements
This research work was supported by the Capital District Health Authority. The authors would like to acknowledge and thank the subjects, and staff at the Nova Scotia Rehabilitation Centre for their participation.