
Abstract
Stump ulcers are common problems in amputees. Temporary discontinuation of prosthetic limb use is frequently employed to facilitate healing. Inevitably, this limits activity and may, for instance, prevent an amputee from going to work. A survey of clinical practice was carried out based on the premise that controlled continued prosthetic limb use in patients with stump ulcers will not adversely affect the ulcer nor prevent healing. The survey would also form a basis for developing future guidelines in the management of stump ulcers. All consecutive patients attending the Chapel Allerton Hospital prosthetic clinic between January 2003 and May 2004 with stump ulcers were recruited into the study. Primary outcome measures were changes in the surface area of the ulcers and in clinical photographs taken on 2 occasions 6 weeks apart. Some 102 patients with a mean age 60 years (range 18 – 88 years) were recruited. Eight patients who were established prosthetic limb users did not complete the study and were excluded from the analysis. Of the patients 52 were newly referred patients with delayed surgical wound healing while 42 were established prosthetic limb users for at least 1 year. Continued prosthetic limb was associated with a significant reduction in ulcer size (p < 0.05). Mean sizes of the ulcers at first and second observations were 3.30 cm2 (range 0.06 – 81) and 0.70 cm2 (range 0.00 – 13.00) respectively. The ulcers improved in 83 cases while two were unchanged. Deterioration was observed in nine cases. The current clinical practice is to allow most of the patients to commence or continue prosthetic limb wearing despite the presence of stump ulceration. This observational study found that, despite prosthetic use, 60 (64%) cases healed completely within the six-week study period and 23 (25%) ulcers reduced in size. The ulcers were unchanged in 2% of the cases. Deterioration was observed in nine (9%) cases. This survey suggests that the current practice of allowing patients to use their prostheses is safe. A clinical trial is now needed to establish whether this practice alters healing rate or has any other disadvantages for new or established amputees.
Introduction
Stump problems are very common, disrupt the day-to-day use of artificial limbs and hence interfere with the independence and lifestyle of amputees. Delayed prosthesis fitting is the main cause of increased costs of rehabilitation after amputation (Vigier et al. 1999). A recent point prevalence survey of patients registered at the Prosthetic and Amputee Rehabilitation Centre at Chapel Allerton Hospital (CAH) revealed that 43% of a random sample of amputees is troubled by stump problems at any one time (Wadwhani 2001). These problems include delayed wound healing, folliculitis, recurrent skin ulcerations and pressure damage.
These problems arise because the soft tissues of the stump are not adapted for load bearing (such as that of the palms and soles) but are subjected to compression and shear forces that may exceed body weight via the prosthetic socket interface. The instinctual response to development of stump skin problems is avoidance of weight bearing for a varying period until resolution.
The majority of amputees in the UK have peripheral vascular disease, diabetes associated with microvascular disease and sensory neuropathy or both (NASDAB 2004). Conditions of tissue oxygenation in distal lower limb amputation often make healing difficult (Vigier et al. 1999). Suggested general measures employed in dysvascular patients with wound healing problems include complete bed rest, optimization of diabetic control and good nutrition (Horne and Abramowicz 1982). However, the first of these may not be practical and can also cause economic hardship in many cases.
The presence of an open wound does not necessarily preclude weight bearing. Repeated wound assessment and modification of the treatment plan as needed are important and decisions should be based on the progression or deterioration of the particular wound (Berke 2004). Many lower limb amputations do not heal in a primary fashion and it is not uncommon for patients referred for prosthetic rehabilitation to have small areas of wound requiring secondary healing and a period of minor wound care (Berke 2004).
Furthermore established prosthetic limb users may develop ulcers in their stump as a consequence of pressure and shear forces. Relieving these forces by means of socket modification may enable the ulcers to heal while allowing continued prosthetic use. The use of silicone sleeves has been advocated as a strategy to minimise shear damage to vulnerable skin (e.g., grafted or tethered skin) and promote the healing of recurrent skin lesions along with reduction in peak pressures (Sonck et al. 1970).
The prevalence of chronic stump ulcers has been quoted to be up to 20% in some studies (Byung-Jin 2003). In addition, approximately 50% of the trans-tibial amputees have failure of primary wound healing which is defined as healing of the surgical incision by the 14th post-operative day. Subsequent breakdown after this period is defined as secondary wound breakdown (Horne and Abramowicz 1982).
The use of rigid plaster dressing in the early post-operative phase following amputation is well documented in allowing for mobilization, early prosthetic fitting and control of stump oedema (Sonck et al. 1970; Kraker et al. 1986; Maclean and Fick 1994). Drawbacks of this technique are the requirement for specialized training in application and removal of the casts and the risk of stump breakdown and infection occurring unnoticed under the cast (Smith et al. 2003). Semi-rigid dressings have been shown to be effective in promoting amputation limb wound healing and also assist in preparing the limb for prosthetic fitting (Wong and Edelstein 2000).
This survey is based on the premise that, though stump ulcers/tissue breakdown is common in amputation patients, continued prosthetic limb use combined with appropriate interventions to reduce shear and pressure stresses will not adversely affect healing. The authors describe a survey of continued prosthetic limb use in established limb users and fitting of prosthetic limb in newly referred patients with lower limb amputations with stump ulcers and delayed primary wound healing. Outcome measures were the surface area of the ulcers measured on two different occasions six weeks apart, supplemented with clinical grid photographs.
Methods
All lower limb amputation patients attending the prosthetic limb clinic based at CAH with stump tissue breakdown during the study period (January 2003 – May 2004) were recruited. Established limb users were defined as those patients with at least one year's prosthetic limb use experience.
An ulcer was defined as a break in stump skin of at least 0.25 cm in diameter.
The ulcers were mainly of category II variety defined as small open areas that can be managed, and ultimately heal with dressing strategies and wound care with no additional surgery required (Berke 2004).
Primary and secondary wound breakdown were as previously defined. Ulcers were assessed clinically using a wound tape measure along with grid photographs and their exact location noted diagrammatically in the study proforma on 2 separate visits 6 weeks apart. These data were used to estimate ulcer area. Any new areas of skin breakdown found at the second visit were noted, measured and photographed as above. Results from culture of wound swabs from specific ulcers and choice of dressing materials were recorded.
Advice on limb use for individual cases during the survey period was documented according to the following categories:
Temporary discontinuation of prosthetic limb use.
Continued prosthesis usage with cotton socks as skin interface material.
Continued prosthetic limb usage with silicon sleeve as interface material.
Socket adjustments were carried out as necessary. Casting and prosthetic fitting were carried out for new limb users.
At the second visit, established limb wearers were asked whether prosthetic limb usage during the preceding six weeks had been “less”, “more” or “as usual”. New prosthetic limb users were asked to describe their progress with prosthetic rehabilitation and mobility at therapy sessions and document any problems observed as a consequence of prosthetic limb use.
The results were analysed using the Statistical Package for Social Sciences (SPSS) Version 11.5 with descriptive statistics and Fischer's Exact Test (2 sided) for impact of limb usage and other factors on outcome measures.
Results
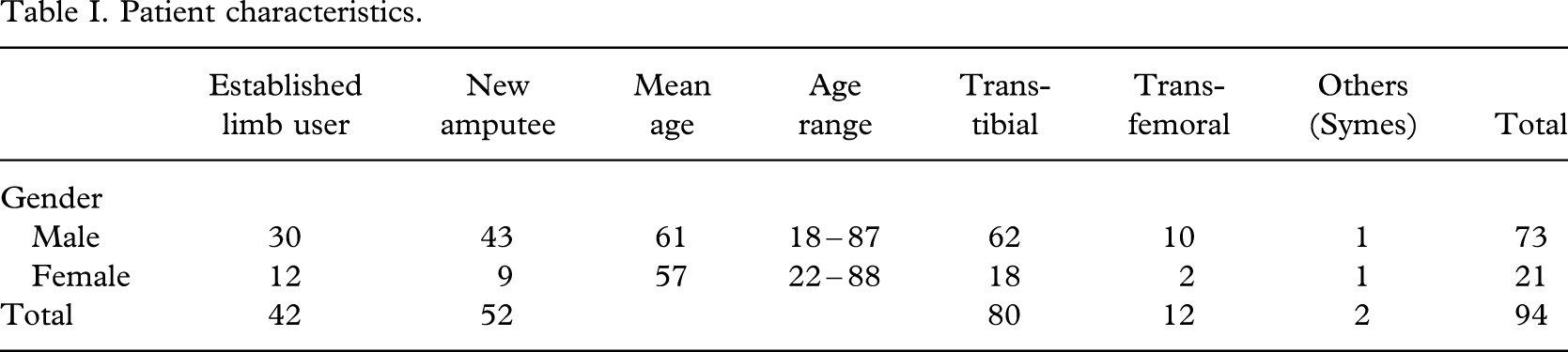
Between January 2003 and May 2004, 1888 patients attended CAH prosthetic limb fitting centre, of which 328 were new. During this time 52 new patients attended with unhealed stump wounds, and 50 established prosthesis users presented with stump ulcers. Both groups (102 patients) were monitored for this survey. As described earlier, the intention was to review ulcer/wound healing at six weeks after presentation. However, eight cases, all established prosthetic limb users were unavailable for assessment at six weeks (6 males and 2 females, 7 trans-tibial amputees and 1 at trans-femoral level) and were therefore excluded from analysis (Tables I and II).
Patient characteristics.
Diagnosis leading to amputation.
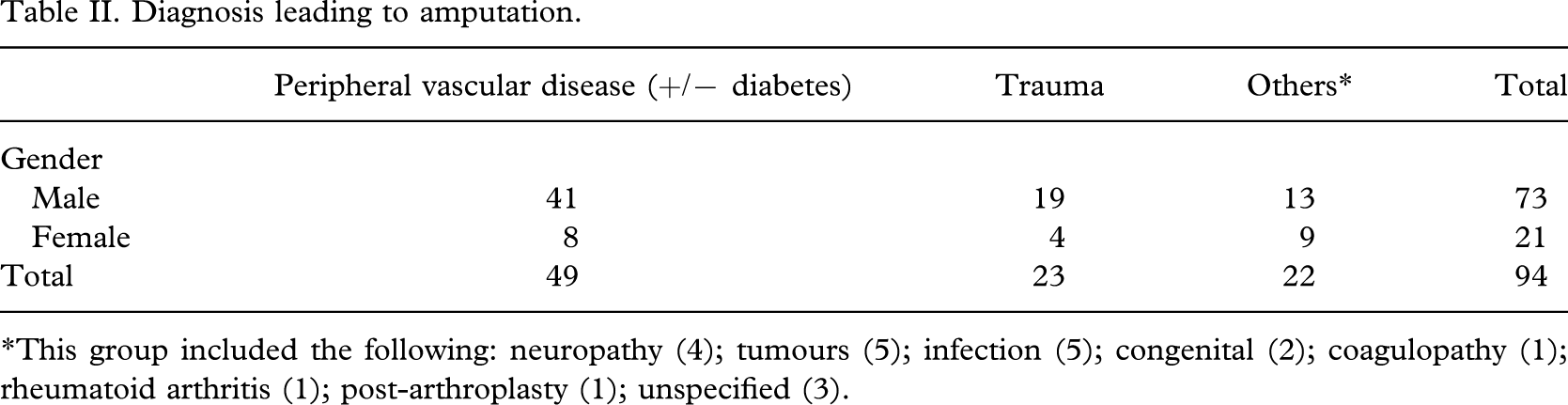
∗This group included the following: neuropathy (4); tumours (5); infection (5); congenital (2); coagulopathy (1); rheumatoid arthritis (1); post-arthroplasty (1); unspecified (3).
A further eight patients (5 males, 3 females) had multiple reviews on account of development of new stump ulcers which all healed within the study period although analysis was restricted to the first episode.
Some 39 patients had right-sided amputation, while 51 were on the left side; 4 of the patients had bilateral amputations.
Ulcer location and number
The ulcers lay in the surgical scar in 35 cases. Other common ulcer sites were the anterior stump surface (25 cases) and the distal surface (17 cases). Some 79 of the patients had a single ulcer while 15 had two or more ulcers on the stump.
Prosthetic limb use/ulcer healing
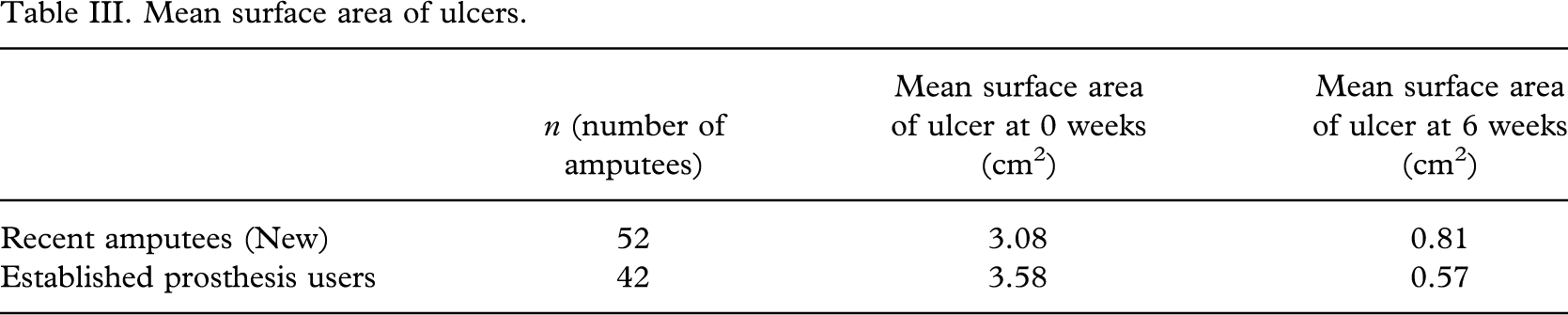
Five patients were advised to discontinue prosthetic limb use during the study period. Despite this advice, all five reported continued prosthetic limb use at their follow-up visits. Two of these had stump ulcers that deteriorated. Of those advised to continue prosthetic limb use, 35 wore their prosthesis with cotton socks as skin interface material, 24 used silicon sleeves and socket adjustments were carried out in 20 patients. Table III gives the mean surface areas of the ulcers at 0 weeks and 6 weeks for both new and established amputees and Table IV shows the progress of the patients during the study.
Mean surface area of ulcers
Progress of patients during the study.
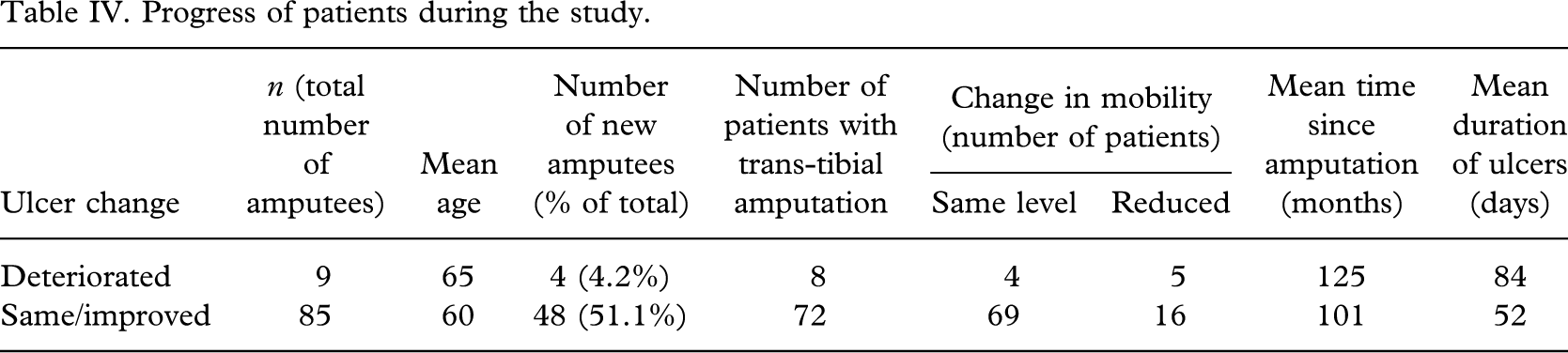
Overall 83 cases (88%) improved with continued weight bearing. In 60 of these, the ulcer healed completely within the six weeks study period, with reduction in ulcer size in 23 cases. The ulcer size remained unchanged in two cases (2%). Deterioration, defined by an increase in surface area of the ulcer was observed in nine cases (10%). Fifteen patients had multiple areas of skin damage on the stump with two ulcers per limb in 10 patients, three ulcers per limb in four patients and one patient had five ulcers.
Discussion
The state of the stump skin has a crucial influence on amputees' ability to use their prosthesis and the importance of early recognition and treatment of skin lesions cannot be over-emphasized (Levy 1995). Although allergic and irritant dermatitis are often seen, the most frequent causes of skin breakdown are mechanical factors, notably compression causing pressure ulcers and shear forces causes local irritation and breakdown (Lyon et al. 2000).
Varying management strategies are employed in treating these problems. Clinical practice employed in treating ulcers that encroach upon weight bearing areas usually includes a period of non-weight bearing to eliminate direct pressure effect on the tissues. The rationale for this is that by off-loading the weight bearing area, repetitive trauma associated with walking is prevented thereby promoting healing (Boulton et al. 2004). However, the situation in amputees is not strictly analogous. It is possible to adjust the artificial limb socket to redistribute loading away from damaged soft tissue in the stump and to incorporate strategies such as silicone intervening layers to absorb shear, where this has contributed to stump soft tissue damage. Furthermore, there is also some evidence in the literature that supports weight bearing and continued activity in certain situations to enhance wound healing (Wilson 1922; Zettl et al. 1969). These studies showed that in many circumstances, initiation (or continuation) of activity is helpful in controlling oedema and facilitating healing. The use of occlusive dressings along with continued weight bearing in the treatment of stump ulcers has also been described (Pinzur and Osterman 1990). The recently updated British Society of Rehabilitation Medicine (BSRM) Guidelines and Standards (2nd edition) for Amputee Rehabilitation provide advice on most aspects of management but were unable to offer clear guidance on this area due the dearth of evidence (BSRM 2003).
The authors' observational study indicates that continued prosthetic limb use combined with strategies to relieve direct pressure and shear forces did not adversely affect ulcer healing in the majority of established amputees presenting with such problems. Furthermore, it was possible to proceed with prosthetic rehabilitation apparently without adversely affecting wound healing in the majority of new amputees presenting with unhealed wounds. Overall, 83 cases of the present series improved using this management strategy with complete healing in 60 of these.
There were nine cases in which clinical deterioration in ulcer size was observed (Table IV). These patients were older with a mean age of 65 years compared to 60 years in those that improved. They also had a longer interval of time since amputation (Mean 125 months) as well as a longer duration of ulcer prior to presentation (Mean 84 days). Some of these patients also had compounding medical problems requiring varying additional intervention including femoro-popliteal bypass surgery for severe ischaemia in the stump as well as recurrent cellulitis.
The authors are uncertain whether their approach to ulcer management in those who continued to use their prostheses conferred any particular advantages. Healing was significantly better with a p value of 0.024 in those than mobilized at their usual level compared to those who were less mobile with their prosthesis. Other factors such as age, gender, diagnosis, number of ulcers, amputation level, antibiotic use and duration of ulcer prior to presentation did not have a significant relationship to ulcer healing (p>0.05). Primapore was used as the dressing material in 44 cases (47%). It has the added advantage of not being bulky with minimal effect on stump volume and shape thereby allowing for easy incorporation into the socket. However, this practice is not unusual (Pinzur and Osterman 1990).
The present study also included only a small sample of five (7%) patients who were advised to abstain from prosthetic limb use. Two of these had ulcers that deteriorated. A multi-centre study comparing varying approaches to management would help clarify all the above issues. Limitations of this survey are that ulcer depth was not measured precisely; instead comments were sometimes noted that certain ulcers were unchanged in area but reduced in depth.
Enquiring from patients if they used their prosthetic limb “less”, “more”, or “as usual” is a crude measure of prosthetic limb usage within the study period although it has been used in other studies on outcome measurement in amputees (Datta et al. 1996).
Nevertheless, if further work confirms that (with appropriate socket modifications, etc.) prosthesis use is safe despite the presence of stump ulcers or unhealed surgical wounds, this could have a major impact on independence, time lost from employment and other aspects of lifestyle in amputees. Although, the majority of amputees are over 65, about 45% are of working age (NASDAB 2004) and the majority of these are in full-time employment and are dependent on their artificial limb(s) to carry out their work (Schoppen et al. 2001).
It is recommend that further studies be done to determine the patient and ulcer features that characterize those with poor healing and more detailed investigations on how best to help this sub-group. It is important to delineate this group further as ulcer deterioration may lead to more widespread sepsis including osteomyelitis, necessitate a more proximal amputation, or even lead to septicaemia.
However, overall, the message seems to be that prosthesis use should not be stopped if a stump ulcer develops nor should a delay or failure of primary wound healing post-amputation surgery preclude prosthetic limb fitting and rehabilitation.