
Abstract
Background:
Although the incidence of major pediatric lower limb loss secondary to either congenital deficiencies or acquired amputations is relatively low, the prevalence of lower limb loss among children in the United States (US) remains unknown.
Objectives:
To estimate the prevalence of major lower limb loss, and the associated prosthetic services use and costs among commercially-insured children in the US.
Study design:
Observational, retrospective, longitudinal cohort study.
Methods:
The IBM MarketScan® Commercial Database was used to identify children (<18 years) with major lower limb loss in the US between 2009 and 2015. Descriptive statistics were used to characterize pediatric cases according to sociodemographic and limb loss characteristics. Multivariate models assessed factors associated with annual prosthetic visits, prosthetic-related costs, and overall medical costs.
Results:
Of the 36.5 million children in the MarketScan database, 14,038 had a major lower limb loss, yielding a prevalence estimate of 38.5 cases per 100,000 commercially insured children in the US during the 7-year study period. Congenital deficiencies accounted for 84% of cases, followed by 13.5% from trauma. Only 10.1% had at least one prosthesis-related visit during any 12-month period following their cohort entry. Among those, the mean annual prosthetic-related costs ranged from $50 to $29,112 with a median annual cost of $2778 (interquartile range = $4567). Annual coinsurance and copays for prosthetic services accounted for nearly half of the overall annual out-of-pocket outlays with medical care for these children.
Conclusion:
Pediatric lower limb loss results in lifelong prosthetic needs. This study informs insurers and policy-makers regarding the prevalence of these patients and the medical costs for their care.
Background
Childhood limb loss often leads to significant physical, emotional, and financial stress to the child and their family. A study of pediatric amputation cases presenting to United States (US) hosptial emergency departments found that the average age for traumatic amputations was 6.2 years. 1 Congenital causes of limb loss, estimated to occur two times more often than trauma-related amputations, suggest that a number of children are living through the early stages of their development with limb loss. 2 Despite their impact, little is known about the national prevalence, outcomes, and cost of caring for children with major lower limb loss in the US.
Prosthetic devices provide an opportunity to optimize functional independence and improve psychological well-being of persons with congenital deficiencies or acquired loss of the lower limbs. Existing studies report varying compliance with prosthetic use in children fitted with these devices. Boonstra et al. 3 reported that 89% of children who underwent an amputation were successfully fitted with a prosthesis and, among those, the majority reported wearing the prosthesis for most of the day. Similarly, in a study of 258 experienced pediatric lower limb prosthesis users, Vannah et al. 4 reported that 88% of children used their devices for more than 9 h/day, although one in five reported experiencing moderate or worse pain and serious issues with tissue breakdown due to use of the device. In contrast, Le and Scott-Wyard 2 and Griffet 5 noted that prosthesis rejection rates were substantially higher among children than adults. The authors attributed the high rejection rate to the challenges posed to the prosthetic team by the unpredictable growth of children and the more varied limb anomalies and configurations that characterize pediatric limb loss patients. In addition to clinical reasons, economic considerations may influence prosthesis use. Despite the known benefits and potential for full restoration of functioning, such devices can be prohibitively costly for many families with estimated cost per single pediatric lower limb amputation ranging from $73,000 to $116,000 from time of injury to 18 years of age. 6 The purpose of this study was to estimate the prevalence of pediatric major lower limb loss among commercially insured children in the US, and to provide estimates of the prosthetic and overall medical care costs associated with their care.
Methods
Study design
A retrospective, longitudinal analysis of IBM MarketScan® Commercial Database 7 was used to identify children (<18 years) with major lower limb loss in the US from 2009 to 2015. MarketScan is a national database comprised of de-identified patient records built from billing and claims data from large, self-insured employers and US commercial firms. Claims data are available for employees, early retirees (who are not Medicare eligible), and their dependents.
All patients under the age of 18 identified as having major lower limb loss in any given calendar year between 2009 and 2015 were included in the analysis. The cohorts of children with lower limb loss were identified based on their first amputation or prosthesis-related claim during the 7-year study period. Prevalence of pediatric lower limb loss was estimated based on total unique children with billing/claims information between 2009 and 2015. In order to calculate annual healthcare utilization, subjects were also required to have continuous enrollment in a MarketScan submitting employer claims during the 12-month follow-up period.
Demographic information as well as level and etiology of amputation were ascertained based on the child’s cohort entry year, that is, the calendar year in which we first observed an amputation-related or prosthetic-related claim for each given child in the cohort. The number of prosthetic-related visits and prosthetic-related costs were determined for the subset of children with lower limb loss who were enrolled at least 12 months from the date of their first limb loss–related claim.
Study population and variables
Identifying the study cohort
Diagnosis and procedure codes were used to identify our study cohorts. Cohort identification as well as classification of limb loss according to etiology and level were based on: (1) International Statistical Classification of Diseases and Related Health Problems – Ninth Edition, Clinical Modification (ICD-9 CM) diagnosis codes, (2) ICD-9 CM procedure codes, (3) Current Procedural Terminology (CPT) procedure codes, (4) Healthcare Common Procedure Coding System (HCPCS) codes identifying visits associated with lower limb prosthetic use and fitting, and (5) HCPCS codes for prosthesis-related components (Table 1). We focused on ICD-9 CM codes as the study period is fully contained within the period preceding implementation of International Statistical Classification of Diseases and Related Health Problems, Tenth Edition codes (i.e. prior to 1 October 2015).
Diagnostic and procedure codes used to identify children with limb loss, etiology, and level.
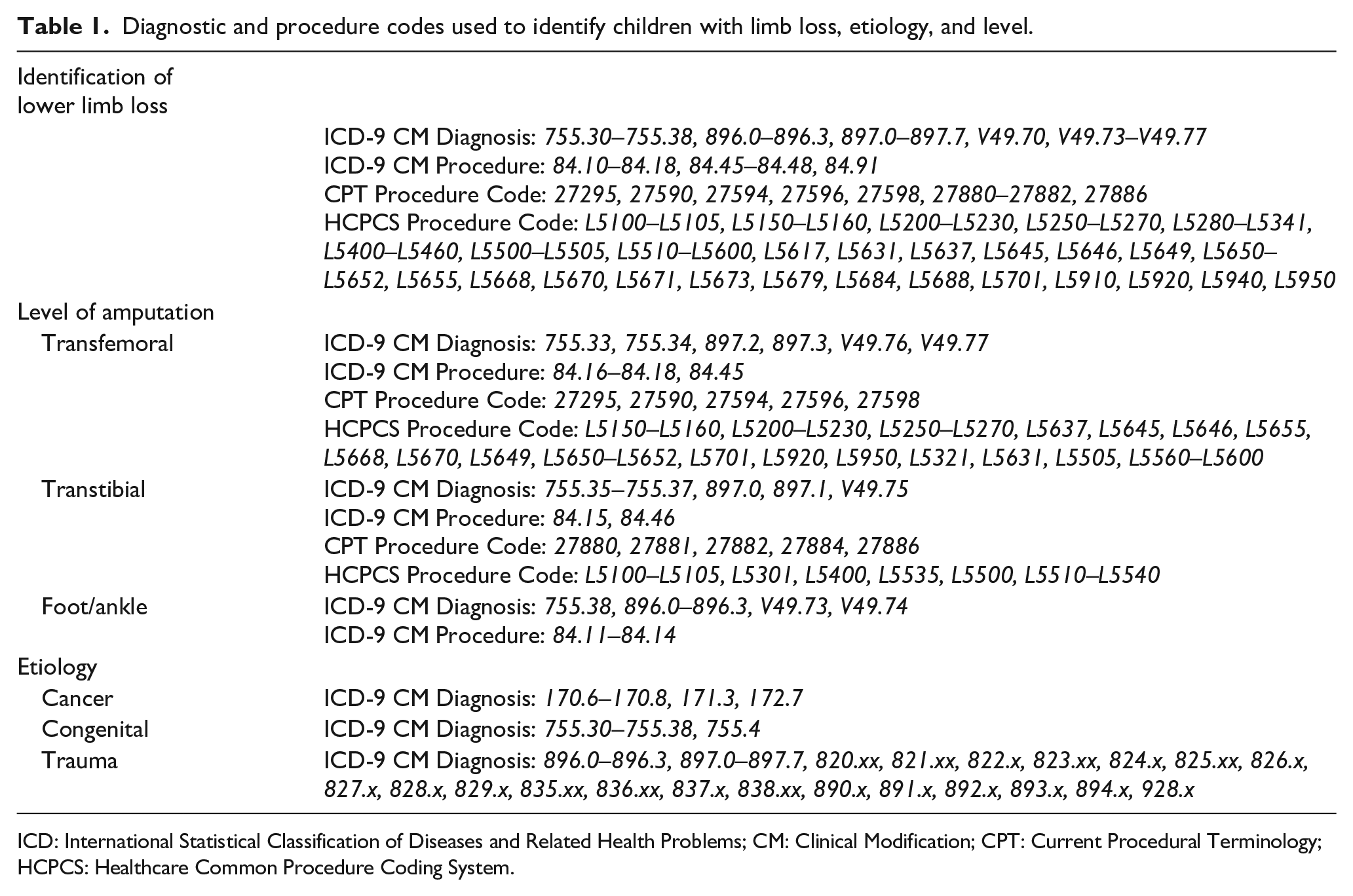
ICD: International Statistical Classification of Diseases and Related Health Problems; CM: Clinical Modification; CPT: Current Procedural Terminology; HCPCS: Healthcare Common Procedure Coding System.
Determining the etiology and level of limb loss
An algorithm was developed to classify children with major lower limb loss according to etiology based on mutually exclusive categories—trauma-related, congenital deficiency, or cancer-related. For the small number of children with billing data indicating more than one etiology code, we imposed a hierarchical classification whereby the final etiology was coded as (1) trauma (if there was at least one medical visit with trauma-related limb loss during the first year when the child entered the cohort), followed by (2) congenital deficiencies (if there were no visits with a trauma-related limb loss code in the year the child entered into the cohort), and (3) cancer-related deficiencies. Etiologies that did not easily fall into one of the above categories were classified as “Other” and reviewed in-depth for reclassification. Level of lower limb amputation was classified in mutually exclusive categories as foot/ankle (at or below the ankle), transtibial (above the ankle but below the knee), and transfemoral (at or above the knee, including hips). Diagnostic and procedure codes used to classify children’s limb loss according to etiology and level are listed in Table 1.
Estimating costs
L-codes listed above, under inclusion criteria (4) and (5), were used to identify prosthesis-related visits and associated costs based on total gross payments to providers (i.e. the amount eligible for payment to the provider after applying pricing guidelines such as fee schedules and discounts, and before applying deductibles, copayments, and coordination of benefits pricing reductions). We used a similar approach to calculate overall medical care costs for children in the sample, which is comprised of all gross payments for services provided either in an inpatient or outpatient setting, including hospital and physician payments associated with physical medicine and rehabilitation services. Overall medical care costs accounted for all healthcare utilization for children over a 12-month period, including prosthetic-related costs. Finally, we calculated the amount of gross covered payments applied toward the deductible at every visit as well as the amount of coinsurance applied toward the stop loss and/or amount of copayment, separately for prosthesis-related visits and overall healthcare utilization. These amounts were calculated over a 12-month period for every child, and averaged over the relevant sample.
Data analysis
Our key study outcomes were (1) prevalence of children with major lower limb loss in the US; (2) rate of prosthetic-related visit during each 12-month period in which a child was observed in the study; (3) the annual cost of prosthesis-related visits among those children with at least one visit within a 12-month period; and (4) the annual cost of overall medical care of children with lower limb loss.
In all analyses, the unit of observation was the child/study year. A generalized linear model was applied to the logarithmic transformation of the cost measures while a logistic specification was used to model the binary outcome of any prosthesis-related visit during each 12-month period since study entry. All analyses were adjusted for patients’ age (in categories), gender, insurance plan type (classified as Basic Major Medical/Comprehensive (BMM); Preferred Provider Organization (PPO); Point-of-Service/Exclusive Provider Organization (POS/EPO); Health Maintenance Organization (HMO)/PPO with capitation; High Deductible Health Plan/Consumer-Driven Health Plan (HDHP/CDHP); limb loss etiology (trauma-related, cancer-related, congenital deficiency)), amputation level (transfemoral, transtibial, foot/ankle, or lower limb not specified if congenital deficiency without amputation), and census division of residence (Figure 1). These multivariable regressions also included indicators for years in the panel (i.e. number of 12-month periods since first billing code identifying limb loss, ranging from one to six) and were adjusted for clustering (i.e. children contributing multiple years of data during the study period) via the generalized estimating equations (GEEs) method. 8

The United States (US) 48 contiguous states’ census divisions.
All analyses were performed using STATA 15.0 software package (Stata Corp, College Station, TX, USA).
Results
Prevalence and sample characteristics
A total of 36,439,701 children were enrolled in a plan included in the MarketScan database from 2009 to 2015. Of those, 14,038 unique children were identified as undergoing a major lower limb amputation or receiving prosthetic care for a major lower limb amputation. This yielded a point prevalence estimate of 38.5 cases per 100,000 commercially insured children in the US during the 7-year study period.
Slightly more than half (50.7%) of the children were male and the majority were covered by a PPO (62.3%). Nearly 40% were aged 10–14 years at the time of the first limb loss claim. Consistent with the distribution of firms contributing data to MarketScan, nearly one-third of children with major limb loss resided in the South (including South Atlantic, East South Central, West South Central, 31.3%) (Table 2).
Characteristics of commercially insured children with major lower limb loss.
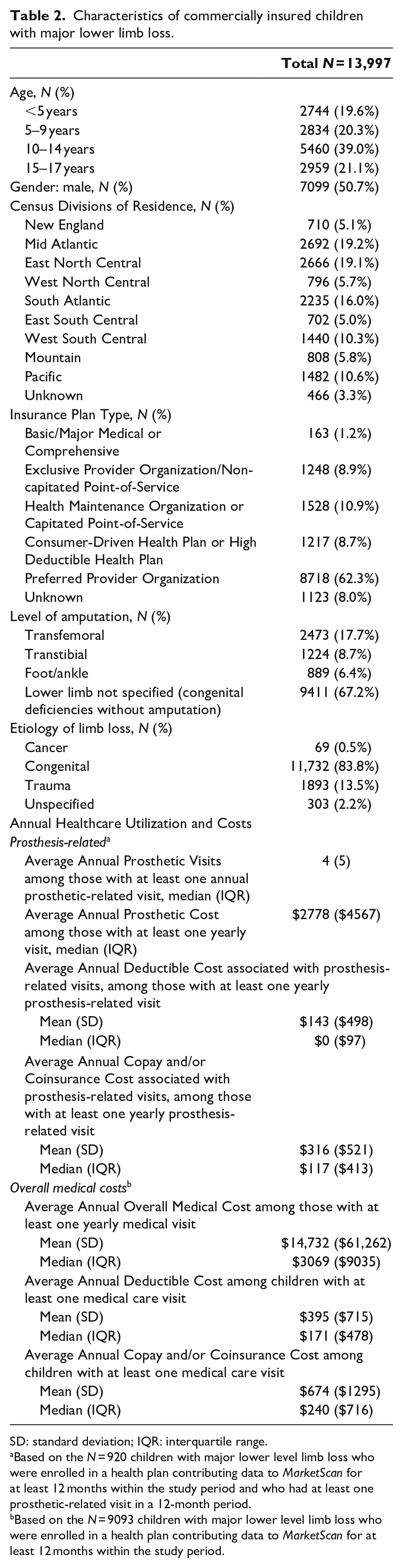
SD: standard deviation; IQR: interquartile range.
Based on the N = 920 children with major lower level limb loss who were enrolled in a health plan contributing data to MarketScan for at least 12 months within the study period and who had at least one prosthetic-related visit in a 12-month period.
Based on the N = 9093 children with major lower level limb loss who were enrolled in a health plan contributing data to MarketScan for at least 12 months within the study period.
Congenital deficiencies accounted for 83.8% of all major pediatric lower limb cases, followed by 13.5% from trauma and 0.5% from cancer. Among those with amputation level specified (i.e. children undergoing an amputation procedure during the study period), amputations at the transfemoral level were the most common (Table 2).
Prosthesis-related visits and associated costs
Sixty-five percent of the children identified as having a major lower limb loss (N = 9093) were enrolled for at least 12 months within the study period and were included in the annual estimations of healthcare and prosthetic utilization and associated costs. Of those, only 10.1% (N = 920) had at least one prosthesis-related visit during any 12-month period following their cohort entry. Among those with at least one visit, the median average annual number of prosthetic-related visits was 4 (interquartile range, IQR = 5 annual visits).
Average annual prosthetic-related costs, measured as the gross payments to providers prior to collection of copays, coinsurance, or other reductions due to coordination of benefits ranged from $50 to $29,112; among those with at least one prosthetic-related visit in any 12-month period following cohort study entry, the median cost was $2778 (IQR = $4567). In the initial year after being identified as having a limb loss, these costs were slightly higher than in subsequent years, with an average annual cost ranging from $100 to $78,043 and a median of $3997 (IQR = $6313). The mean annual out-of-pocket expenses for prosthetic-related visits were $459 (standard deviation (SD) = $957) comprised of $143 (SD = $498) toward the families’ deductible payments and $316 (SD = $521) in annual coinsurance/copays.
Overall medical costs
The annual overall inpatient and outpatient medical care cost (including prosthesis-related costs) among the 9093 children with major lower limb loss with at least one medical visit within a 12-month period ranged from $1080 to about $3,388,000 with a median of $3069 (IQR = $9035) (Table 2). These costs were substantially skewed by healthcare utilization of children with cancer-related amputations. On average, out-of-pocket expenses totaled $1069 (SD = $2002), of which $674 (SD = $1295) were accounted for by coinsurance/copays. In aggregate terms, the annual prosthesis and medical care costs for children with lower limb loss totaled $206.8 million in 2015 US dollars.
Multivariate results
The first column in Table 3 shows factors associated with observing children with major lower limb loss having at least one annual prosthetic-related visit over the study period. Estimates indicate that, other factors being constant, boys were more likely to have a prosthetic-related visit than girls (odds ratio (OR) = 1.17, p < 0.05). Relative to those covered by a PPO, children covered by an HMO with capitated or partially capitated POS plan (OR = 0.77, p < 0.05) or by CDHP/HDHP (OR = 0.57, p < 0.05) were less likely to have an annual prosthetic-related visit during the study period. Similarly, relative to children with trauma-related amputations, those whose etiology of limb loss was cancer (OR = 0.07, p < 0.05) or congenital (OR = 0.39, p < 0.05) were less likely to have such a visit as were those with amputations at the transtibial (OR = 0.04, p < 0.05) or foot/ankle (OR = 0.004, p < 0.05) level (relative to those with transfemoral-level amputations).
Multivariate results: factors associated with having at least one annual prosthetic visit, annual prosthetic-related costs, and annual overall medical care costs among commercially insured children.
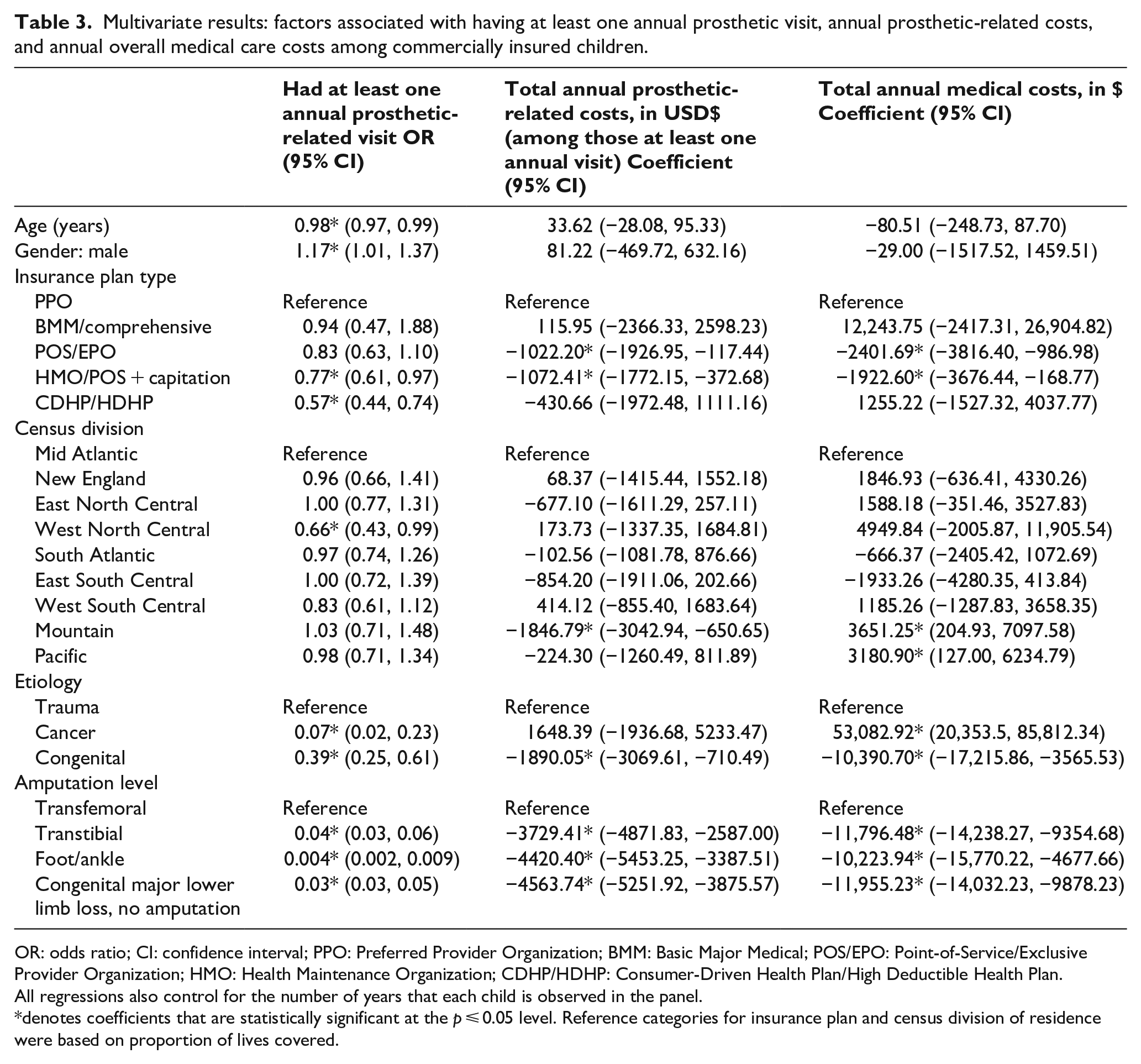
OR: odds ratio; CI: confidence interval; PPO: Preferred Provider Organization; BMM: Basic Major Medical; POS/EPO: Point-of-Service/Exclusive Provider Organization; HMO: Health Maintenance Organization; CDHP/HDHP: Consumer-Driven Health Plan/High Deductible Health Plan.
All regressions also control for the number of years that each child is observed in the panel.
denotes coefficients that are statistically significant at the p ⩽ 0.05 level. Reference categories for insurance plan and census division of residence were based on proportion of lives covered.
In the second column of Table 3, we present coefficient estimates from the multivariate analysis of total annual prosthetic-related costs. Here again, children covered by EPOs with non-capitated POS (mean −$1022, p < 0.05) and HMOs with capitated or partially capitated POS (mean −$1072, p < 0.05) incurred lower annual prosthesis-related costs than their counterparts covered by a PPO plan. Having a lower limb loss secondary to congenital causes (mean −$1890, p < 0.05, relative to those with trauma-related amputations) and having a transtibial amputation (mean −$3729, p < 0.05) or at the foot/ankle level (mean −$4420, p < 0.05) relative to those with transfemoral amputations were significantly associated with lower annual prosthetic-related costs.
Children with lower limb loss associated with cancer incurred substantially higher annual medical care costs (mean +$53,083, p < 0.05) than those with trauma-related amputations. As with prosthetic-related costs, insurance coverage by plans from EPOs with non-capitated POS or HMOs with capitated or partially capitated POS insurance plan, residence in the mountain or pacific regions, and having a transtibial amputation (relative to those with amputation at the transfemoral level) were significantly associated with lower annual overall medical costs (Table 3).
Discussion
To our knowledge, this is the first study to provide an estimate of the prevalence of major pediatric lower limb loss using nationwide US data. Our results indicate that congenital deficiency was the most common etiology of lower limb loss among the population of 13,997 commercially insured children, followed by trauma-related and then cancer-related amputations. 9 Only about 10% of children with major limb loss had at least one visit to their prosthetist during any 12-month period while in the study; among those, copayments/coinsurance costs totaled an average of $316 accounting for nearly half of the families’ annual overall medical care coinsurance outlays for that child.
Our estimate of 38.5 per 100,000 children with major lower limb loss based on commercial claims data is likely a lower boundary of the real prevalence as publicly insured children account for a disproportionate number of pediatric patients. In 2008, Ziegler-Graham et al. 10 estimated a prevalence of 25,000 persons under 18 years of age with limb loss using incidence rates, with 22,000 of these persons with limb loss attributed to trauma. In addition to including children with congenital limb loss, a group that was excluded from Ziegler-Graham’s prevalence estimation, we restricted our estimates to children with major lower limb loss, which may account for the some of the difference between our prevalence estimates and those reported in that study.10,11
Prosthetic devices provide many benefits for those with major lower limb loss—enhanced physical function, emotional health, and positive body image. A proper fitting and comfortable prosthesis facilitates optimal childhood and adolescent growth and development and the achievement of maximal ambulatory function and independence. Despite their benefits, only 10% of children in our study had a prosthesis-related visit over a 12-month period, suggesting that there are likely barriers to access.
MarketScan is comprised of encounter-level data. This means that any clinical contact between a provider and patient will be reflected in the administrative data regardless of payment. Even for bundled services, subsequent follow-up visits will be recorded in the database. Therefore, visits for prosthetic adjustments, or socket modifications, even if included in the capitated or bundled original payments, will result in a recorded encounter in the MarketScan database.
Our finding of only 10% of children with limb loss using prosthetic services during a 12-month period implies some degree of reduced access to these services. Our multivariate analyses, in fact, showed that families with high deductible insurance plans were significantly less likely to have a prosthetic visit for their children (Table 3), suggesting some financial barriers to accessing prosthetic services. This finding may reflect a strategy by families to “stretch out” prosthetic care to minimize out-of-pocket copays and coinsurance payments.
The low use of outpatient prosthetic services is concerning, particularly among children and adolescents experiencing periods of rapid limb and body growth, which might necessitate more frequent prosthetic visits to optimize socket fit and alignment. For those who did have at least one prosthetic-related visit during each 12-month period since cohort entry, the annual prosthesis-related costs varied widely, ranging from $50 to nearly $30,000 annually. On average, annual coinsurance and copays for prosthetic services, which varied substantially by health plans, accounted for nearly half ($316/$674) of the overall annual out-of-pocket outlays with medical care for these children. Although relatively lower over time, prosthetic-related outlays remain a financial burden to families (and insurers) due to ongoing adjustments and replacement of these devices as children grow. These findings should prove useful to health policy-makers, the prosthetics industry, and national medical societies in their efforts to improve access to affordable prosthetic devices for these children by advocating for full coverage for prosthetic care by insurance carriers—with no out-of-pocket expenses for families.
The median annual prosthetic cost in this study was $2778 (IQR = $4567)—about double that reported in a study by Weir and colleagues in 2010 that used membership data maintained by the Amputee Coalition of America. 12 Although part of the difference is likely due to inflationary pressures on healthcare costs and medical equipment between study years, our higher costs may also reflect the different demographic composition of the samples. To that point, the MarketScan data, which served as the basis for this study, are comprised entirely of children who are dependents of commercially insured parents or guardians, while over a quarter of the families in Weir et al.’s cohort had incomes below the Federal Poverty Level and, therefore, were likely insured by a federal or state public program.
Several factors may have contributed to the relatively low utilization of prosthetic services in our study population; among others, the timing at which the child was introduced to their first prosthetic device; limited access to affordable devices; the potentially limited selection of appropriate, often costly, components to the prosthesis to ensure its comfort and function; and restrictions on the number, frequency, and timing of devices covered by the family’s insurance plan. In addition, the number of visits and associated costs were reported over a 12-month period. As prosthetic devices in children are covered at 24-month intervals, a longer observation period may have captured more prosthetic-related visits. However, by studying 12-month intervals, we were able to best capture children who may have had changes to their insurance plan or coverage during the study period. It is also plausible that children may have been fitted but rejected their prostheses prior to contributing data to MarketScan; as evidence suggests that secondary complications tend to be frequent in this population.3,4,13 Unfortunately, our insurance-based data set does not contain information that might shed light into these factors.
Three important limitations of the study merit comment. Although appropriate to estimate prevalence of limb loss among a large sample of commercially insured children, our study based on the MarketScan database precluded us from estimating incidence of the disease and, consequently, from documenting patterns of prosthetic service use from the initial surgery. In addition, although the MarketScan data set includes a wide range of health insurance plan types, our findings are not generalizable to children covered by public insurance, such as states’ Children’s Health Insurance Programs or those who are dependents of commercially insured persons employed by firms not contributing data to MarketScan. Finally, although the MarketScan commercial claims database, with its de-identified information on more than 250 million patients across all US states, afforded us a unique opportunity to examine the healthcare utilization and costs among commercially insured children with major lower limb loss, the database cannot be considered nationally representative as it reflects the experience of employees (and dependents) of large, self-insured employers and managed care organizations contributing data during the study period and is unable to account for variability in access to prosthetic resources. Our findings regarding healthcare utilization and cost, however, are likely more accurate than those relying on surveys, as they are not subject to recall and other biases associated with estimates derived from small, opportunistic samples drawn from prosthetists’ or advocacy societies’ records.3,4,14–17
Conclusion
Comfortable and functional pediatric prosthetic devices can provide independence and promote a child’s physical and emotional well-being. Children and adolescents require more frequent prosthetic changes to accommodate normal musculoskeletal growth and development. Our findings suggest that access to and use of such prosthetic care may be limited for many families and their children with limb loss. Using commercial claims data that are national in scope, our study documents the prevalence of major pediatric lower limb loss in the US, thereby providing an estimate of the number of children who require prosthetic services.
Footnotes
Acknowledgements
MarketScan data were provided by the Medical College of Wisconsin under an institutional data agreement with IBM.
Author Contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.