
Abstract
The Canadian prosthesis is indicated for the more proximal levels of amputation of the lower limb (very short trans-femoral, hip disarticulation and hemipelvectomy cases); it is frequently rejected by many patients for different reasons (awkwardness, intolerance of the socket, excessive energy expenditure to ambulate among others). The objective was to analyse the use or rejection of Canadian prostheses (n = 23) after an 8-year follow-up study (range: 2 – 16 years). The sample consisted of 52% men and 48% women, and the average age at the time of amputation was 52.26 ± 19.71 SD years (range: 1 – 74 years). The most frequent aetiology was malignant tumour (56.5%). Eight of the subjects continued to use the prosthesis through the entire study (34.7%). Gender, age, and aetiology were not significant determinants of use. The daily use was 12.5 h per day. The rejection of the Canadian prosthesis was after 20 months of use (range: 2 – 48 months), and the main reasons were death (all tumour causes), intolerance to the socket, or difficulty in ambulation. In conclusion, many years after their discharge from rehabilitation services, more than one-third of the sample (34.7%) were wearers of the Canadian prosthesis.
Introduction
The Canadian prosthesis was designed in 1954 by Colin McLaurin in Toronto, Canada and later developed by James Foort at the University of Berkeley, USA.
This design has been indicated for the hemipelvectomy, hip disarticulation, and the very short trans-femoral amputation. The socket or pelvic-basket is carefully moulded with a broad integral belt gripping the pelvis. A mechanical hip articulation is placed anterior and distal to the anatomic hip joint. The prosthetic knee is set posterior to the weight line in a position of considerable stability (Murphy 1960) (Figure 1).

Canadian prosthesis (modular system).
In the field of rehabilitation medicine, several scales have been developed to describe the function gained with lower-limb prostheses, but there is still no universally agreed upon method to measure the functional capacity of which amputees are capable (Legro et al. 1998; Rommers et al. 2001).
On the other hand, an aspect gaining interest among health care professionals in relation to lower-limb amputations is what happens with the prosthetic use after discharge from the rehabilitation service (Gauthier-Cagnon et al. 1999).
The authors' objective was to analyse the use or rejection of the Canadian prostheses prescribed in their prosthetics unit during the last 16 years.
Patients and method
The sample was obtained from the amputees treated in the Prosthetics Unit of the Central Hospital of Asturias from January 1987 to December 2002. This regional unit treats the amputated population of the Community of Asturias (1,100,000 inhabitants) coordinating the rehabilitation treatment, and the prosthetic fitting and training of the newly amputated.
During the 16 years of the study, 1433 lower limb prostheses were fitted (excluding those for the foot) 23 of which were Canadian prostheses (1.6%).
The following variables were studied: gender, age, aetiology, level of amputation, mean delay between the amputation and prosthetic fitting, independence in donning and doffing the prosthesis, household or community mobility, and acceptance or rejection of the prosthesis.
All of the patients were evaluated at least 1 year after treatment and discharge from the rehabilitation unit.
The variables were introduced in the SPSS 8.0 database program. A descriptive study of all the variables was performed to compare the prosthesis use with non-use. For the comparison of the qualitative variables, the Mann – Whitney test was used for non-parametric variables. The analysis of the variance for the comparison of means considered the values P < 0.05 as significant.
Results
The follow-up study was for 8 years (range: 2 – 16 years). In the sample, 12 (52%) patients were men, and 11 (48%) were women; the mean age at the time of amputation was 52.26 ± 19.71 SD years (range 1 – 74 years).
The distribution according to the level of amputation was: hemipelvectomy two cases (8.7%), hip disarticulation 20 cases (87%), and short trans-femoral one case (4.3%).
Regarding aetiology, 13 (56.5%) were tumour, five (21.7%) infection, four (17.4%) trauma, and one (4.3%) congenital malformation (phocomelia).
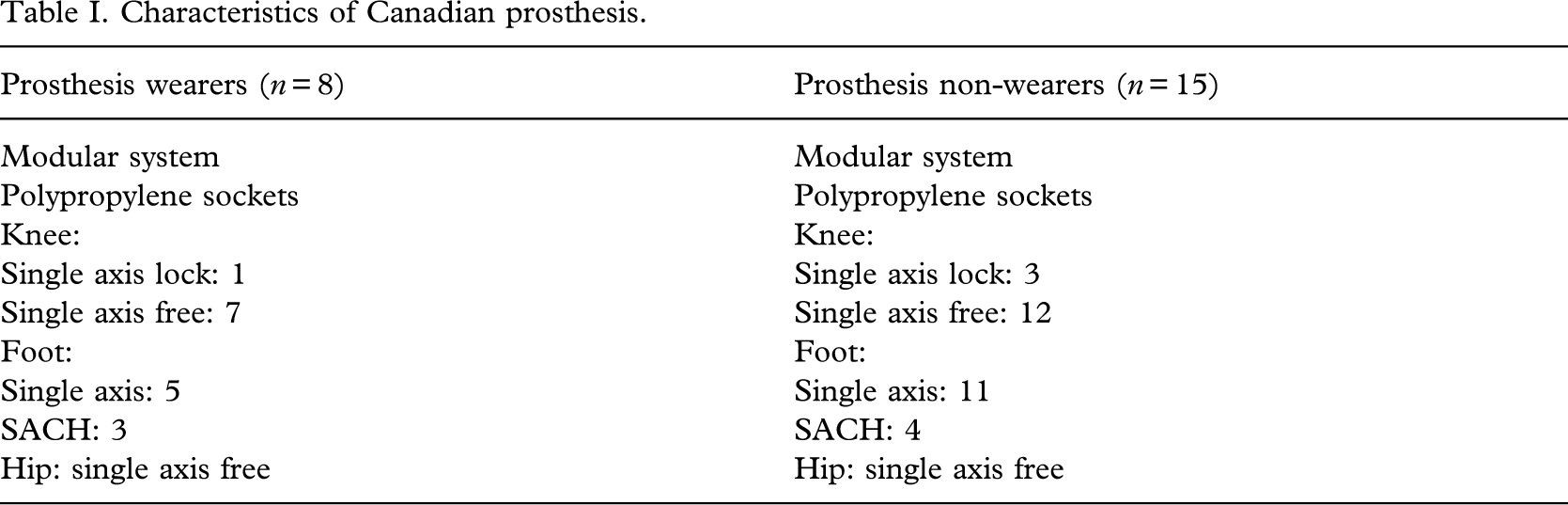
The Canadian prosthesis was fitted at 16.5 ± 9.45 SD weeks (range, 4 – 36 weeks) from amputation. The delay in the fitting was due to infection of the stump or a previous treatment (chemotherapy). All patients left the unit to go home and were independent to don and doff the prosthesis. Likewise, all were community ambulators. The characteristics of the prosthesis are detailed inTable I.
Characteristics of canadian prosthesis.
At the time of the study, eight patients (34.7%) wore the prosthesis, and the daily use was 12.5 h (range 7 – 15 h). According to the amputation age, those who used the prosthesis were younger than those who rejected it: a mean age of 42.25 ± 26.56 SD years (range 1 – 63 years) of the wearers in contrast to the mean age of 57.60 ± 13.03 SD years (range 28 – 74 years) of the non-wearers. This difference is not statistically significant.
Gender did not significantly influence the use or rejection of the Canadian prosthesis. The relationship between the aetiology and the prosthetic use is reflected inTable II and does not show any significant differences.
Use of canadian prosthesis according to aetiology of amputation.

Of the remaining 15 non-users, nine patients (60%) had died (all of tumoural causes) and six had abandoned the prosthesis approximately 20 months after their fitting (range 2 – 48 months). In all cases, the cause of rejection was attributed to the difficulty of ambulation, intolerance to the socket, or excessive weight of the prosthesis.
Discussion
It is a very well-known fact that different factors such as age, gender, aetiology, level of amputation, or general health conditions play an important role in determining prosthetic use (Gauthier-Cagnon et al. 1998; Grieve and Lankhorst 1996; Leung et al. 1996).
For some authors, the Canadian prosthesis has few indications for the elderly (McAnelly et al. 1998; Menager et al. 1996). In this aspect, our results are similar because those patients who accepted the prostheses were younger than those who rejected them.
The aetiology of amputation is also a decisive element in evaluating the results. Tumour was the main cause (56%) in the study. Amputees with vascular disease experience more difficulty in ambulation with the prosthesis. In a previous paper about ischaemic patients, only 10% of subjects were Canadian prostheses wearers (Malone and Goldstone 1986). In another comparative study among 24 tumoural hip-disarticulation and 37 ischaemic cases, the tumour patients were more likely to accept the prosthesis (Denes and Till 1997). It remains unclear as to why there was a greater use among tumour patients, but the authors agree with Ferrapie et al. (2003), who affirm that the neoplasic amputees find some benefit with the prosthesis and are able to use it and to walk. Courneya et al. (2000) estimate that exercise would increase the motivation of the patients with cancer, combating psychological aspects such as depression, anxiety, preoccupation with body image, or low self-esteem. It would also improve cardiorespiratory, muscular, and immunological systems.
The Canadian prosthesis requires the participation of the muscles of the lumbar region that in many cases can explain the pain in the lumbar spine. Besides the difficulty in obtaining a good fit and suspension with this prosthetic system, there are unpredictable movements in the oscillation during the stance phase that causes wearers to complain frequently of discomfort (Zaffer et al. 1999). This poor socket tolerance represents a clear disadvantage that can explain the rejection of the prosthesis (Malone and Goldstone 1986; Starc 2001).
Waters et al. (1976) have demonstrated that the energy expenditure for ambulation with a prosthesis increases as the amputation level is more proximal. Walking with a Canadian prosthesis can increase energy costs by 80 – 250%, another reason that would justify the abandonment of the prosthesis (Nowroozi et al. 1983; Starc 2001).
In the programme of training with the prosthesis, the patients carry out walking activities. As patients progress, the difficulty is modified. At the beginning, these activities are basic, e.g. standing, transferring, ascending and descending stairs, etc., and in the end, they incorporate more complex activities. When this training is concluded, the patient is discharged from the rehabilitation service, and the functional results are measured. It is unsure if the results remain the same when the patient returns home (Gauthier-Cagnon et al. 1999).
Nevertheless, the definition of the term ‘prosthetic use’ is not sufficiently described because different options exist when other aspects are contemplated such as independence to don and doff the prosthesis, hours of use per day or week, household or community mobility, traversing obstacles, walking with adverse climatic factors, or the use of canes or other assistive devices. Keeping in mind this variability in the definition of ‘prosthetic use’ in different published studies (which are always for trans-tibial and trans-femoral amputees), they give a prosthetic use between 36 and 89% (Gauthier-Cagnon et al. 1998; Grieve and Lankhorst 1996; Jones et al. 1993; Leung et al. 1996; Nielsen 1991).
This percentage was smaller, between 22.1 and 38.6%, in a follow-up study of 5 years from the discharge among trans-femoral amputees and with hip-disarticulation cases (De Luccia et al. 1992). For Davies and Datta (2003), after 1 year of follow-up, 29% of the trans-femoral patients maintained community mobility.
In contrast with many articles about trans-femoral and trans-tibial amputees, there are few publications about long-term follow-up of Canadian prosthesis wearers. Menager et al. (1996), in a study of 118 cases with Canadian prosthesis, did not mention the percentage of wearers who continued use over time. Denes and Till (1997) reported a user rate of 43% (from a total of 61 patients), while Unruh et al. (1990) did not find any patient able to use the prosthesis among 38 cases with hip disarticulation. Finally, after 1 year of adaptation of the prosthesis, the mobility decreased if the level of amputation was more proximal, and amputation age was higher (Davies and Datta 2003).
In conclusion, many years after their discharge from rehabilitation service, more than a third of the sample (34.7%) were wearers of the Canadian prosthesis.