
Abstract
Background:
Previous literature has suggested that age, level of amputation, residual limb length, comorbidities, mental disorders, and cause of amputation can affect the ability to successfully ambulate with prosthesis.
Objectives:
The objective of this study was to analyze the predictors that affect the rehabilitation outcome of war-related transtibial amputees and the relationship of these factors with ambulation ability after prosthetic fitting.
Study design:
Retrospective observational study.
Methods:
We reviewed the records of 69 war-related transtibial amputees. The rehabilitation outcome was analyzed according to the grade of rehabilitation summarized in three grades. Multiple logistic regression analysis was used to determine the odds of achieving the first rehabilitation grade.
Results:
The majority of patients with transtibial amputations achieved the first grade of rehabilitation (59.4%). The factors that significantly influenced the achievement of the first grade of rehabilitation were age and absence of posttraumatic stress disorder. For every 1-year increase in patient age, the odds of achieving first grade of rehabilitation decreased by a factor of 0.9. Patients without posttraumatic stress disorder had 12.9 greater odds of achieving the first rehabilitation grade compared to patients with posttraumatic stress disorder.
Conclusion:
Achievement of the first grade of rehabilitation among war-related transtibial amputees is dependent on patient age and the absence of posttraumatic stress disorder.
Clinical relevance
Understanding the factors that may affect the rehabilitation outcome of war-related amputees could lead to a more specific organization of the rehabilitation, especially in a country that has recently been involved in war. This is the first study to focus on determinants of prosthetic rehabilitation in these patients.
Introduction
Transtibial amputation is the most common type of major amputation seen during war and peace. 1 Due to an increase in the number of armed conflicts in recent times, the number of amputations has increased as well. 2 War-related lower-limb amputations are usually a consequence of injuries from mine fields.2–4 Previous literature has suggested that age, level of amputation, residual limb length, comorbidities, mental disorders, and cause of amputation can affect the ability to successfully ambulate with prosthesis. 1,5–23
Increasing age seems to be a prognostic factor for a low functional level of the lower-limb amputee as well as transtibial amputees.5–9 Nevertheless, it is still not clear whether the determinant is age itself or whether increasing comorbidities and diminished physical condition with age are more important determinants that influence functional outcome.10–12
The length of the residual limb may also influence the functional outcome.13,14 No consensus in the literature currently exists with respect to tibia length, which provides better functional activities. A range of measurements have been provided for tibia length, including “one hand’s breadth,” 24 20 cm, 25 9–11 cm distal from the knee joint line as ideal for the ischemic patient, 26 and 4–7 in. 27 In general, residual limb with a tibia length of 15 cm, measured from the tibial plateau, provides better functional activities in patients. 16
Among individuals with traumatic physical impairments, extensive burns, spinal disorders, amputations, and heart failure were found to be risk factors for posttraumatic stress disorder (PTSD). 18 In addition, data suggest that an amputation resulting from accidental injury may lead to a higher prevalence of PTSD, in part because of the emotional stress surrounding the accident 19
The relative risk of PTSDs among individuals with six types of traumatic physical impairments, including spinal disorders, extensive burns, amputation, heart failure, major chest trauma, and cardiac arrest, were previously analyzed, and four of the six impairments were found to be risk factors for PTSD (extensive burns, spinal disorders, amputations, and heart failure). 18 In addition, data suggest that amputation resulting from accidental injury may lead to a higher prevalence of PTSD, in part because of the emotional stress surrounding the accident 19
In addition, comorbidities such as heart disease (coronary arteries disease), hypertension, cerebrovascular diseases, 7 pulmonary disease, peripheral artery disease, degenerative joint disease, blindness, 10 and diabetes mellitus type I 28 determine the success of rehabilitation.9,12 However, these comorbidities were not always identified in previous studies.8,11
In addition to transtibial traumatic amputation, the presence of other major injuries significantly influences a patients’ quality of life involving productivity at their job, family, and society in general. 1
After the 1998–1999 war in Kosovo, a training program was developed for the first time for patients with lower-limb amputations. The humanitarian organization Handicap International organized prosthetic rehabilitation immediately after the war as well as the manufacture of prosthetics. They were initially in charge of the program, and at the same time provided training to physiotherapists for prosthetic rehabilitation of amputees as well as prosthetists for the manufacture of more functional and comfortable prostheses.
We hypothesized that age, PTSD diagnosis, and comorbidity would have an impact on the rehabilitation outcome. Thus, the aim of this study was to analyze the influence of factors that affect rehabilitation outcome of war-related transtibial amputees and to identify the relationship of these factors with the ambulation ability of patients with prosthesis.
Methods
This was an observational retrospective study.
Subject population
The rehabilitation outcome was studied in 69 transtibial amputees who had received firearm injuries during the war or as a consequence of the war (mine explosion). The patients were managed at the Ortho-Prosthetic Center rehabilitation unit in University Clinical Center of Kosovo between 1 July 1999 and 30 June 2001. Information about the rehabilitation outcome was obtained from hospital records. Patients included in the study were between 9 and 88 years of age (mean ± standard deviation (SD): 34.8 ± 16.6 years).
Outcome measurements
Assessment of rehabilitation outcome was made on a 3-point scale adapted from the form provided by Handicap International and summarized as follows:
Grade I. Ambulating with prosthesis, completely independent from orthotics.
Grade II. Ambulating with prosthesis, independent indoors, but requiring one walking stick or crutch for outdoor mobility.
Grade III. Ambulating with prosthesis and one walking stick or crutch indoors, but requiring two crutches for outdoor mobility.
Other measurements
The following parameters were also recorded: age, residual limb length, PTSD, associated injuries on other extremities, comorbidities, and duration of rehabilitation. The residual limb length was measured from the medial tibia plateau to the fleshy end of the residual limb (actual residual limb length). 29
PTSD was evaluated and confirmed by a psychiatry expert. The associated injuries on other extremities presented as soft tissue injuries, injuries with mild muscular defect, long bone fractures, and amputations of one or more fingers. Comorbidities presented as cardiopulmonary disease, diabetes mellitus, and eye injuries. The other causes of injuries were from bombs, grenades, and bullets.
Rehabilitation procedure
Immediately after the war, all patients were included in an intensive training program, which consisted of three phases: postoperative, preprosthetic, and prosthetic phase. Since the majority of patients included in the study had their amputation performed during the war (in improvised field hospitals), not all of them could go through the postoperative phase, because at that time there was no training program for amputees. The patients who did undergo an amputation after the war (as a consequence of a land mine explosion) were subject to postoperative and preprosthetic phases that included the following: respiratory exercises, edema control, bandaging of the residual limb, range of motion exercises to maintain mobility of the remaining joints, isometric exercises for strengthening of the glutei and thigh musculature, static/dynamic balance exercises in the sitting position and in the erect position, exercise for general endurance, exercise for the bed-walking aids transfer, and walking exercises with appropriate walking aids.
In the prosthetic phase of the training program, the amputee rehabilitation was focused on fitting and walking exercise with the preliminary prosthesis: the donning of the temporary prosthesis, exercises on parallel bars (static balance on both legs and body weight bearing over the prosthesis and the sound leg, which was verified and controlled with two weight tiers), making a step with the prosthesis, and exercises for the same length and width between steps.
The same exercises were subsequently more advanced with the prosthesis and appropriate orthotics. Older patients were fitted with walking frames or axillary crutches, and younger patients were fitted with axillary or forearm crutches. This was followed by walking with the prosthesis and an appropriate walking aid, first over the flat floor, and then over a floor with obstacles, climbing up and down stairs, walking on slopes and uneven ground (indoors as well as the outdoors in the garden of our center), and falling and standing up from the ground. Finally, patients exercised walking with a single crutch and then without any crutches (in cases that had the ability to do so). The time needed to walk with two and then with a single crutch as well as the time to walk with no crutch was measured for each patient. There were also daily exercises of coordination and balance with the prosthesis. Physical therapy was adapted to each individual patient, but was always within the framework of the described standard procedure.
Statistical analysis
Statistical analysis was performed by using statistical package SPSS-Sigma Stat 2.03 version software (IBM, Inc., NY). The results were compared using a one-way analysis of variance (ANOVA) test, Student’s t-test, and Chi-square test. Multiple logistic regression analysis was used to determine the odds of achieving the first rehabilitation grade, and results were expressed as odds ratio (OR) with 95% confidence interval (CI). Statistical significance was considered if the value of the factor alpha was ≤.05.
Results
Table 1 lists the characteristics of the patients with war-related transtibial amputations treated at the XOrtho-Prosthetic Center rehabilitation unit in University Clinical Center of Kosovo. All of the transtibial amputations were unilateral. The distribution of patients by left versus right transtibial amputation was comparable (43.5% vs 56.5%, respectively; p = 0.3). The majority of patients achieved the first grade of rehabilitation (59.4%), but only 13% of the patients achieved the third grade of rehabilitation.
Characteristics of the patients with war-related transtibial amputations treated at the Ortho-Prosthetic Center (OPC) of the University Clinical Center of Kosovo.
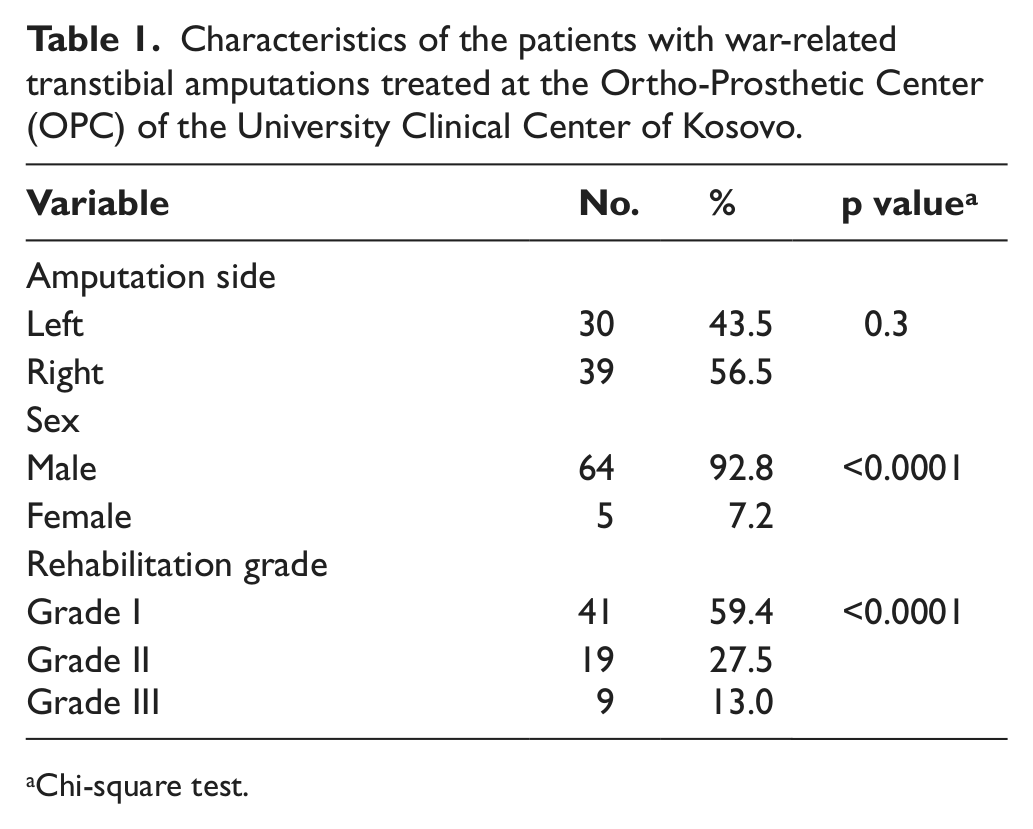
Chi-square test.
The majority of the cases fell within the 20–39 years age group (43.5%). The majority of the patients who achieved the first and second grades of rehabilitation fell within the 20–39 years age group (46.3% and 47.4%, respectively), and the majority of patients achieving the third grade of rehabilitation (33.3%) were within the 60+ years age group (Table 2). The average age of the patients who achieved the first grade of rehabilitation was lower than that for patients who had achieved the second and the third grades of rehabilitation (30.17 ± 13.15 years vs 41.21 ± 14.54 years and 42.67 ± 26.72 years, respectively; Table 2). In addition, 43 patients had associated injuries on other extremities, while 20 patients had comorbidities.
Structure of war-related transtibial amputees by age group, PTSD, injuries in other extremities, and comorbidity according to rehabilitation grade.
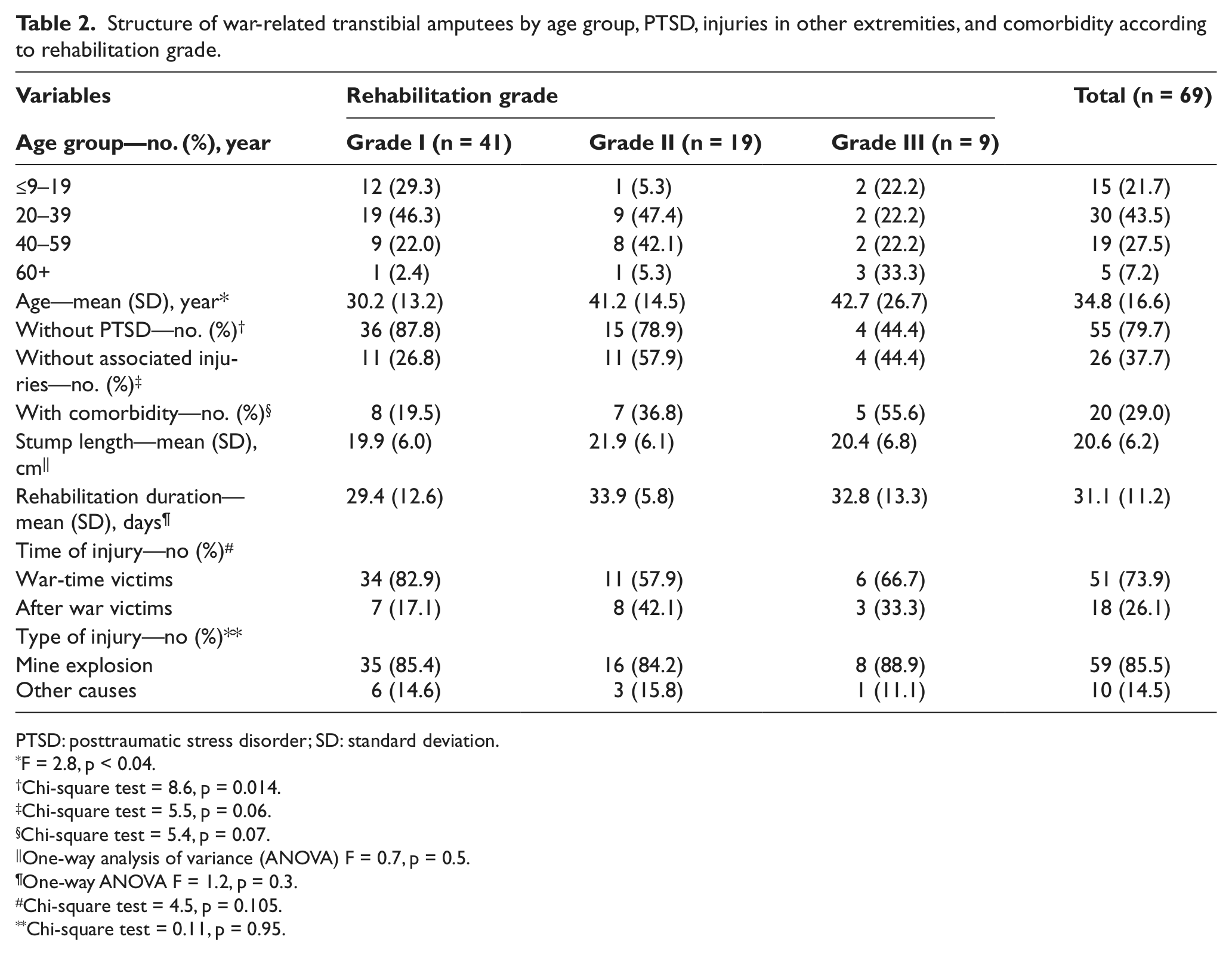
PTSD: posttraumatic stress disorder; SD: standard deviation.
F = 2.8, p < 0.04.
Chi-square test = 8.6, p = 0.014.
Chi-square test = 5.5, p = 0.06.
Chi-square test = 5.4, p = 0.07.
One-way analysis of variance (ANOVA) F = 0.7, p = 0.5.
One-way ANOVA F = 1.2, p = 0.3.
Chi-square test = 4.5, p = 0.105.
Chi-square test = 0.11, p = 0.95.
The patients who achieved the first grade of rehabilitation were significantly younger than those achieving the second and third grades of rehabilitation (ANOVA F = 2.8, p < 0.04) (Table 2). More patients without a PTSD diagnosis achieved the first grade of rehabilitation compared to those with a PTSD diagnosis (χ2 = 8.6, p = 0.014). There was no difference in the number of patients without associated injuries or with a comorbidity based on the rehabilitation grade (χ2 = 5.5, p = 0.06 and χ2 = 5.4, p = 0.07, respectively).
The mean stump length and mean rehabilitation duration in relation to the rehabilitation grade was comparable (ANOVA F = 0.7, p = 0.5 and F = 1.2, p = 0.3, respectively).
There was also no difference in the number of patients injured during or after the war as well as mine explosion versus other causes of injury according to the rehabilitation grade (χ2 = 4.5, p = 0.1 and χ2 = 0.11, p = 0.95, respectively) (Tables 2 and 3). The mean rehabilitation duration with regard to the time of injury (war-time vs after war) was also comparable (t-test = 0.13, p = 0.9; Table 3).
Rehabilitation outcome according to the time of injury of war-related transtibial amputees.
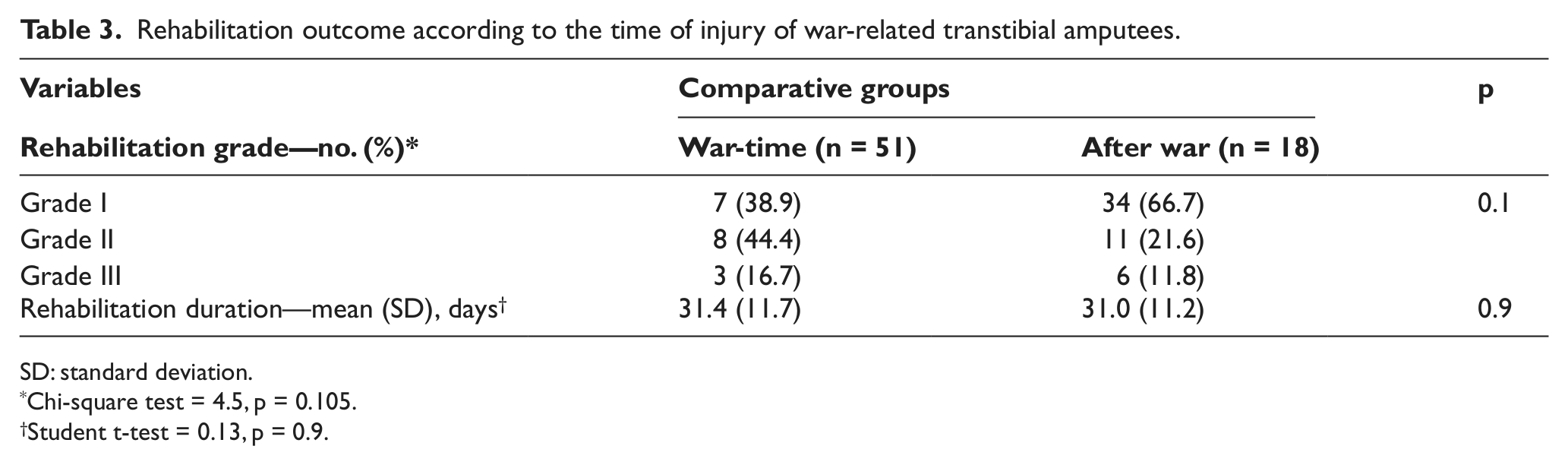
SD: standard deviation.
Chi-square test = 4.5, p = 0.105.
Student t-test = 0.13, p = 0.9.
The factors that significantly influenced achievement of the first grade of rehabilitation were age and the absence of PTSD. For every 1-year increase in patient age, the odds of achieving the first grade of rehabilitation decreased by a factor of 0.9 (or by approximately −10%) (OR (95% CI): 0.9 (0.9, 1.0), p = 0.002). Patients without PTSD had 12.9 greater odds of achieving the first rehabilitation grade compared to patients with PTSD (OR (95% CI): 12.9 (2.2, 76.7), p = 0.005) (Table 4).
Multiple logistic regression analysis—influence of factors for achieving the first grade of rehabilitation.
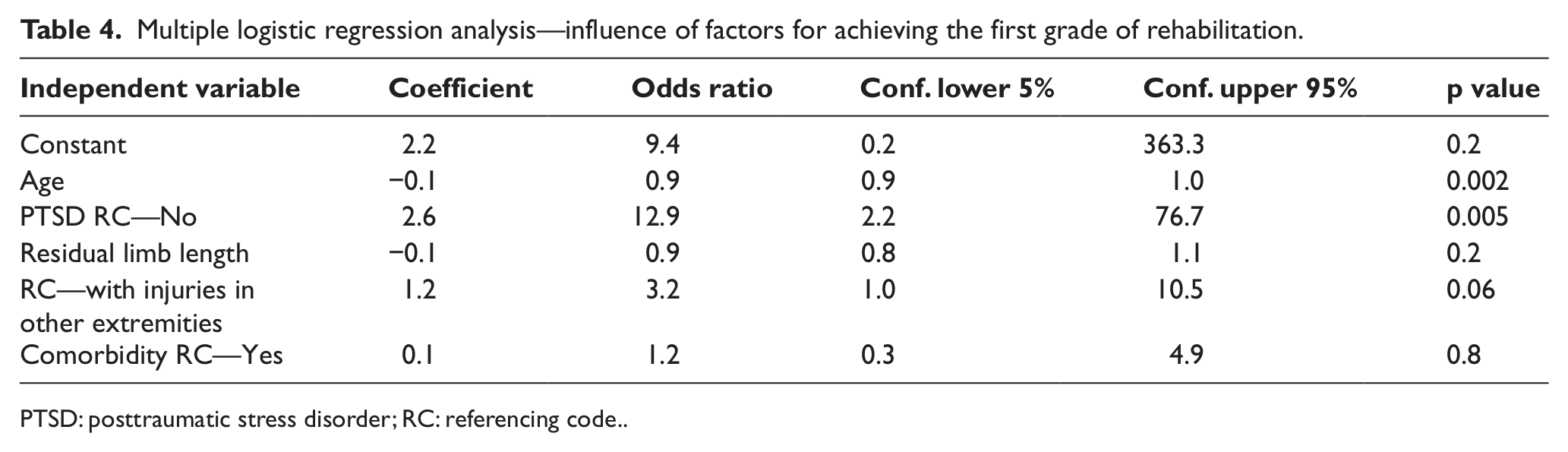
PTSD: posttraumatic stress disorder; RC: referencing code.
Discussion
In order to plan rehabilitation for patients with war-related below-knee amputation, it is critically important to identify the factors that have an impact on the rehabilitation outcome. It is also important to learn more about these prognostic determinants and their relationship to functional outcome.5,7,8,10–12,15,30–42 We found that age and a PTSD diagnosis had the greatest impact on rehabilitation outcome, but comorbidities did not. This result could be due to the small number of cases with comorbidity.
In our study, all patients were ambulatory with their prosthesis. Of the 69 follow-up patients, 41 (59.4%) could ambulate with their prosthesis indoors and outdoors without any assistive device. Previous studies have also found similar high percentages of prosthesis usage for mobility (ambulation). Of the below-knee amputees reported by Pohjolainen et al., 35 85% (67/79) had useful ambulation, at least indoors, while 5% (4/79) were nonambulators with their prosthesis. The main symptom that restricted walking was ischemic leg pain.
Narang 34 also found that 54% of below-knee amputees younger than 30 years of age and 10% of below-knee amputees above 30 years of age did not need assistive devices. In that study, the first grade of rehabilitation was achieved in 70% of below-knee amputees, 36% of above-knee amputees, and 30% of bilateral amputees. 34
The mean age of our amputees was 34.8 years, which is a relatively young age and related to the cause of amputation (trauma and injuries from firearms). This finding was in accordance with the mean age of patients in previous studies where trauma led to amputations.4,34,39,40,43 In this study, we found that patient age and PTSD were independent variables with greater influence in rehabilitation outcome. Other studies 5–9,34,37,39,40 have also indicated that patient age is an important risk factor for functional outcome in lower-limb amputees. However, one study 10 concluded that regardless of age, patients with more medical problems were poor ambulators.
The length of the stump as the determinant of rehabilitation outcome has been studied by many authors,13,14,44,45 particularly in amputations that occur as a consequence of vascular insufficiency. In our study, the stump length had no significant impact on the achievement of first grade of rehabilitation. Thus, several factors may contribute to the rehabilitation outcome in amputees.
Pohjolainen and Alaranta 7 found a significant relationship between the length of the stump and walking distance in a group of transtibial amputees. However, they did not precisely describe their measurements of stump length and did not explain this relationship in detail. Another study 44 assessed the relationship between tibia length and functional mobility 1 year after transtibial amputation caused by vascular insufficiency. In that study, it was found that a tibia length of 12–15 cm distal from the knee joint line was related to a better outcome than a tibia length shorter than 12 cm. However, the authors could not reach a conclusion regarding stumps with a tibia length longer than 15 cm due to a lack of patients. 44 Subbarao and Bajoria 45 concluded that relatively short stumps (e.g. 8–10 cm long), which are likely to heal quicker and are associated with less risk of reamputation than long stumps, may be an advantage in ischemic patients. In addition, patients with a longer stump length were found to require less energy on average based on computer dynography and electrocardiogram (ECG) analyses. 42 Thus, an ordinary stump length (approximately 15 cm of tibial length) can provide a better functional level, resulting in better control of prosthetic devices. 46
Approximately 20% of our cases were diagnosed with PTSD. During and after the war in Kosovo, some physicians of general practice and psychiatrists were trained to diagnose and treat PTSD (supported by humanitarian organizations such as Medicine Sans Frontiers (MSF) and Cooperative for Assistance and Relief Everywhere (CARE)). These psychiatrists worked as consultants at Ortho-Prosthetic Center or as an abbreviation OPC, and patients of this study were under their supervision only during the prosthetic phase of rehabilitation. PTSD clearly had a substantial impact on patients, as amputees without PTSD had 12.9 times greater odds of achieving the first grade of rehabilitation. Similar findings were also observed in other studies. Indeed, psychological factors and coping strategies have been found to be associated with poor outcomes after amputation.47–49
For many patients, the outcome of rehabilitation following amputation is markedly dependent on the presence of comorbidities. However, we did not find any significant influence of comorbidity on the rehabilitation grade. Pernot et al. 9 reported that lower-limb amputees with a comorbidity were less likely to reestablish normal living. Johnson et al. 10 reported that cardiac disease and diabetes mellitus influenced postamputation mobility scores by lowering them individually or together. Moreover, other studies8,11 found that the presence of diabetes mellitus had no effect with regard to functional outcome.
A small number of studies have analyzed the influence of injuries on other extremities in rehabilitation outcome. Most of these studies analyzed the rehabilitation outcomes in vascular insufficient amputations. In this study, we found that 62.3% of patients had injuries in other segments, but these injuries did not have a significant influence on rehabilitation outcome. It is difficult to explain this finding; it may be due to the high percentage (45.34%) of soft tissue injuries among our patients.
Some consideration should be given to the limitations of the study. While we were able to capture data from the Ortho-Prosthetic Center or you can use as OPC rehabilitation admissions in a retrospective approach, we wanted to present the achievements of rehabilitation outcome immediately after the war. Our goal was also to gain an understanding of variables that contribute to the failure or success in prosthetic ambulation. The fact that many independent variables were not significant may reflect the preselection process of enrolling only below-knee amputees, who are patients thought to have a high probability of success. In order to measure the overall effects of each variable, we would have to study all individuals with amputation regardless of the perceived rehabilitation potential. The use of prosthesis for transfers is also important for amputees, but this was not examined because the focus was on prosthetic ambulation. A review of the literature also revealed a great discrepancy with respect to the criteria used to determine functional outcome within the amputee population, and therefore, it was very difficult to compare our results with the results of other studies, since the assessment of the functional achievements of lower-limb amputees and below-knee amputees differs from one study to another. Thus, we are unable to directly relate our results with other studies because of different study designs and statistical analyses that were used.
Conclusion
Our findings show that achievement of a first grade of rehabilitation among war-related below-knee amputees is dependent on patient age and the absence of PTSD. The findings of this study attest to the fact that adjustment to amputation is complex and long term, highlighting the importance of encompassing the psychological component of injury across the continuum of prosthetic rehabilitation. In addition, the development of standardized criteria to determine functional outcomes would allow for better comparisons to be made between various programs in various geographical locations.
Footnotes
Acknowledgements
The author would like to express his gratitude to Prof. dr. Cen Bytyqi, MD PhD, EPOS member, Reconstructive Department, Orthopedic Clinic Prishtina, University Clinical Center of Kosovo, for his professional review and technical support of this research article.
Declaration of conflicting interests
The author reports no conflicts of interest. The authors alone is responsible for the content.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.