
Abstract
Background: Good suspension lessens the pistoning (vertical displacement) of the residual limb inside the prosthetic socket. Several methods are used for measuring the pistoning.
Study Design: Clinical trial.
Objectives: To introduce and evaluate a new simple method for measuring the pistoning between the soft liner and socket in transtibial prostheses.
Methods: Five transtibial prostheses with Iceross silicone liner and shuttle lock were made for the subjects. The pistoning was measured between the liner and socket by a photographic method in single limb support on the prosthetic limb (full weight bearing), non-weight bearing and under three static axial loading conditions (30, 60 and 90 N).
Results: This new method enabled us to measure the pistoning between the liner and prosthetic socket. The reproducibility of measurements in different trials of one session and between two sessions by two observers was shown to be high. The average of displacement between the liner and socket was about 9 mm in non-weight bearing compared with full weight bearing. Furthermore, as we expected, the average of pistoning increased consistently by adding the loads.
Conclusions: This new method provides for easy and inexpensive determination of pistoning between the liner and socket by every prosthetist in clinical settings.
Clinical relevance
A new method is demonstrated for evaluating the pistoning between the liner and socket in transtibial prosthesis. This provides a faster and easier way of clinical pistoning measurement. It can be implemented in any prosthetic centre by every prosthetist.
Background
The lower limb prosthesis’s efficiency is mainly guaranteed by its optimal suspension in order to secure the socket to the amputee’s stump. Suspension and fitting have main roles in the patient’s comfort and prosthetic function.1-6 According to the amputees, the most important factor in every prosthesis is the fit of their prosthesis and suspension.7-9 Pistoning or vertical movement 10 of the residual limb inside the prosthetic socket is said to be one of the major indications of successful or unsuccessful suspension in lower limb prosthesis. 11 Also, prosthetic fitting had been shown to be correlated with pistoning.11-14 Thus, measuring the pistoning would be helpful in determining the optimal prosthetic fit and suspension.13,15 Ideally, each prosthetist should be able to measure the pistoning in order to enhance the suspension and prosthetic fit. Several methods have been used to measure pistoning movement in different levels. The movement can be either between the hard socket and the liner, between the liner and the skin, or the skin and the bone. 14 Radiological methods include roentgenology,16-18 cineradiography,11,19,20 and roentgen stereophotogrammetric analysis. 18 Ultrasonic methods or transducers have also been used to record the pistoning or displacement inside the socket.21-23 However, these methods require complicated devices and settings 24 and it is not possible for every rehabilitation clinic to provide such costly imaging systems. Even if the amputee is referred to an imaging centre, there might still be a risk of repeated exposure to the X-ray.14,25 Therefore, these studies have been mostly limited to the laboratory and could not be used clinically.
The objective of this study was to introduce and assess a new method for measuring the pistoning within the socket, designed and developed in-house at Össur (Reykjavik, Iceland) for the first time.
Methods
Subjects
Five male unilateral transtibial amputees (average age 45 ± 7.3), with the mobility grade K3 (based on the American Academy of Orthotists and Prosthetists) participated in this study (Table 1). Ethical approval was granted from the University of Malaya Medical Centre (UMMC) Ethics Committee. Five transtibial prostheses with silicon liner and shuttle lock were made by one prosthetist to avoid variability due to manufacture, fitting and alignment factors. The subjects were required to complete five static trials for five different static conditions to simulate the gait, including single limb support on the prosthetic limb (full weight bearing), off-loading the prosthetic limb (non-weight bearing), and three different axial loading. Loads of 30, 60 and 90 N were added to the prosthetic foot. Average value was used for the analysis
Subject characteristics.
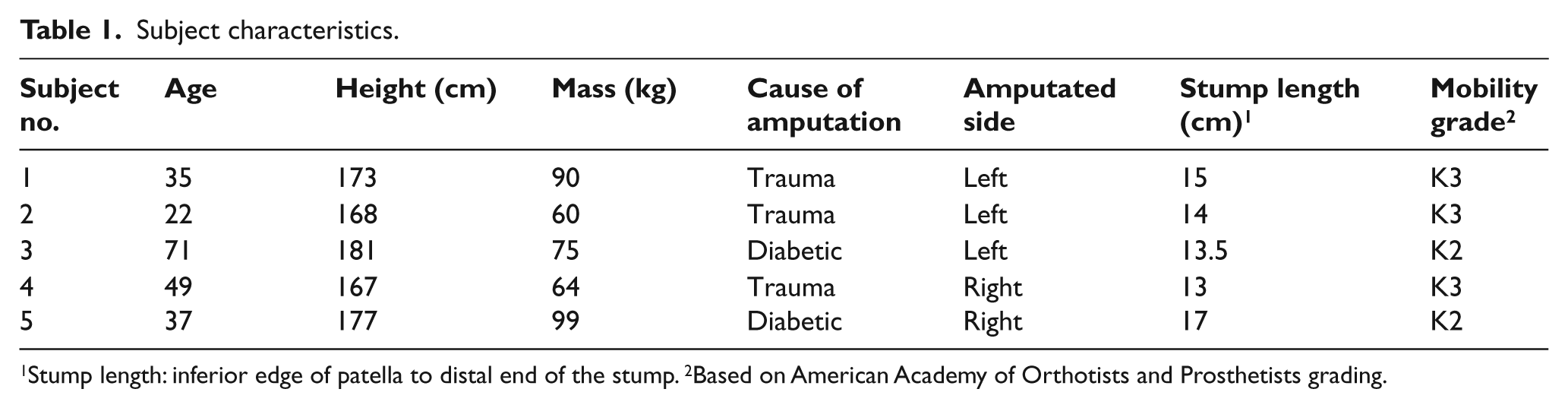
Stump length: inferior edge of patella to distal end of the stump. 2Based on American Academy of Orthotists and Prosthetists grading.
Technique for measuring the pistoning
To identify the pistoning movement inside the prosthetic socket with this new method we used the following equipments:
30, 60 and 90 N loads;
a high-resolution camera (Sony A, alpha, DSLR-A200K, 3,872 x 2,592 dpi);
two reference rulers (with known length of 100 mm) attached to the lateral side of the limb and the socket (Figure 1) as a reference to measure the real displacement on the photos;
markers on the following positions (Figure 2): greater trochanter (A), proximal lateral end of the liner (B), proximal lateral end of the socket (C), distal end of the socket (D).
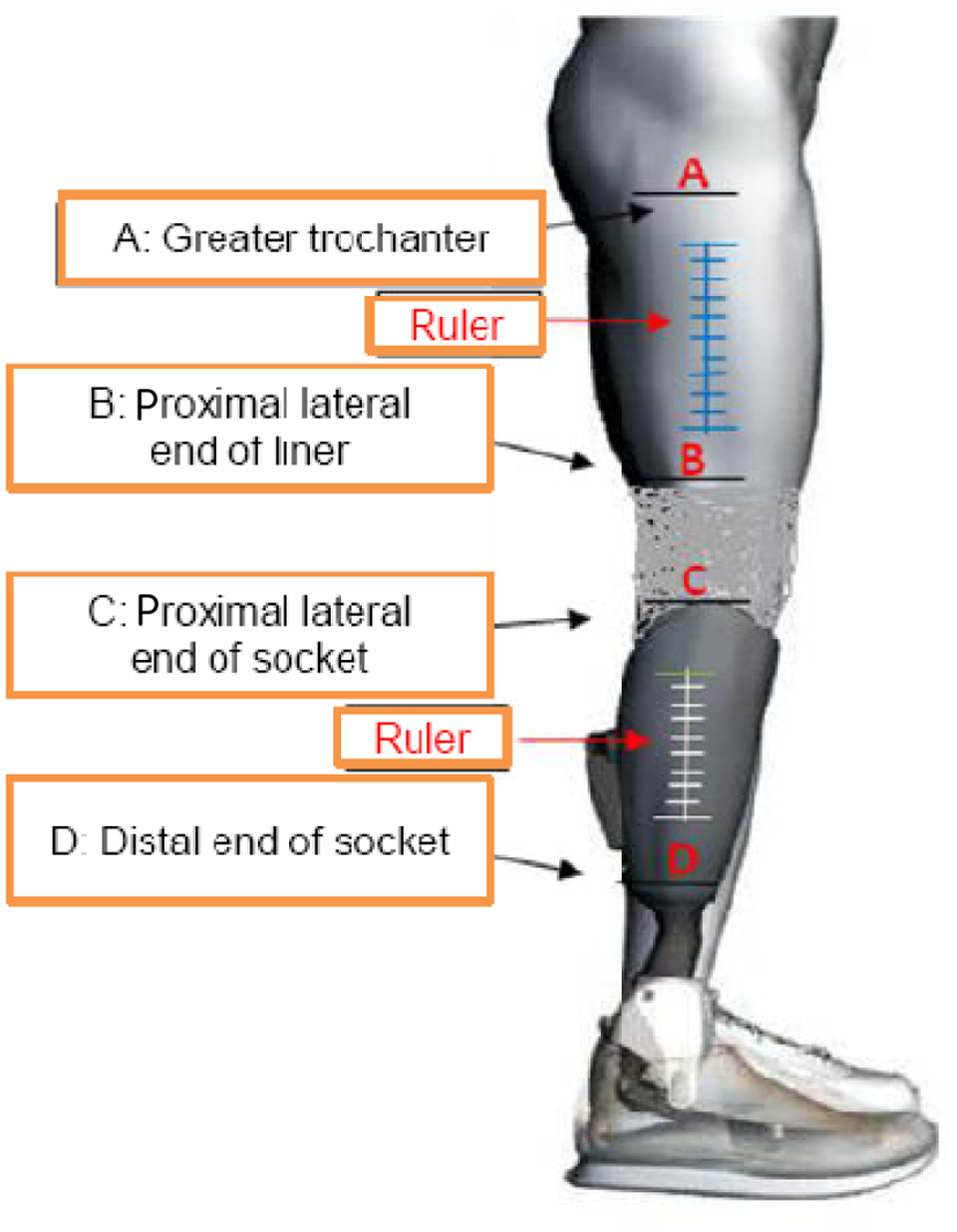
Position of markers and rulers.

(A) Full weight bearing, (B) non-weight bearing, (C) applying a load.
The ruler attached to the limb (thigh) was used as a measuring reference for the markers A and B, and the other ruler was used as measurement reference for the markers C and D.
In each of the five conditions below, we took a photo from a fixed distance using a photo stand. The photos were taken so that the markers and the reference rulers could be seen clearly, and were not at an angle from the stand:
Amputee standing full weight bearing on prosthetic limb. This was considered the baseline position which all other were compared with (Figure 2).
Amputee standing with no weight on the prosthesis and straight leg (e.g. on the stairs with the sound leg on the step and the prosthesis freely suspended).
Applying a 30-N load along the longitudinal axis of the prosthesis.
Applying a 60-N load along the longitudinal axis of the prosthesis.
Applying a 90-N load along the longitudinal axis of the prosthesis.
We examined the accuracy of the method. Six markers were attached to a solid object. The distance between each two markers was measured by a digital caliper. A photo was taken from the object, with a reference ruler placed next to it. One of the researchers was asked to calculate the distances on the photo, while he was not aware of the distance values. In comparison, a measurement error of 0.1 mm was found.
It is possible to measure the pistoning between the socket and liner with only two markers (B and C, or A and C). However, to check the accuracy of the method, two extra markers were attached to the socket as a solid object. Therefore, since the markers on the solid object do not have any displacement, it was possible to check the accuracy of the displacements between other markers. These additional markers are assumed to enable every prosthetist to check the accuracy of their calculations.
Calculating pistoning movements
The measurement value when the amputee applied full body weight on the prosthesis was used as a baseline (AB standing, AC standing, AD standing, BD standing). Then the other four conditions were compared with the baseline value to identify any pistoning movement. The ΔAD displacement was calculated as follows:
ΔAD (90N) = AD 90 N – AD standing;
ΔAD (60N) = AD 60 N – AD standing;
ΔAD (30N) = AD 30 N – AD standing;
ΔAD (no weight) = AD no weight – AD standing.
The calculations of the previous step were repeated for AB, AC and BD. We compared the displacement for the three distances (AC, AD and BD) and found the mean. Ideally, the displacement should have been the same for the three distances AC, AD and AB + BD. Deviations represented errors of measurement.
The reproducibility of measurements was evaluated by intraobserver intrasession, intraobserver intersession and interobserver intersession variability. Two observers performed the experiments in two sessions with a one-week interval. The data analysis was performed by SPSS 18.0.
Results
The intraclass correlation coefficient (ICC) of intraobserver intrasession, intraobserver intersession and interobserver intersession was 0.90, 0.84 and 076 respectively. The averages of displacement between the markers in different static conditions are shown in Figure 3. Results showed that ΔAC and ΔAD were the same in different static positions and ΔAB + ΔBD = ΔAD. In this study we observed that the most displacement was between changing the position from full weight bearing on the prosthetic limb to non-weight bearing (10 ± 9.2 mm). Adding 30 N to the prosthesis increased the pistoning by about 4 ± 2.6 mm. After changing the position from a 30-N to a 60-N load, the pistoning increased 2 ± 0.8 mm. Finally, when we added a 90-N load to the prosthetic limb we found a 2 ± 1.4 mm displacement compared to when the 60-N load was used. There was only a 1-mm displacement between the markers A and B (skin and liner) after the subjects changed their position from full weight bearing to non-weight bearing. This amount was increased to 2 mm for the 60- and 90-N loads.
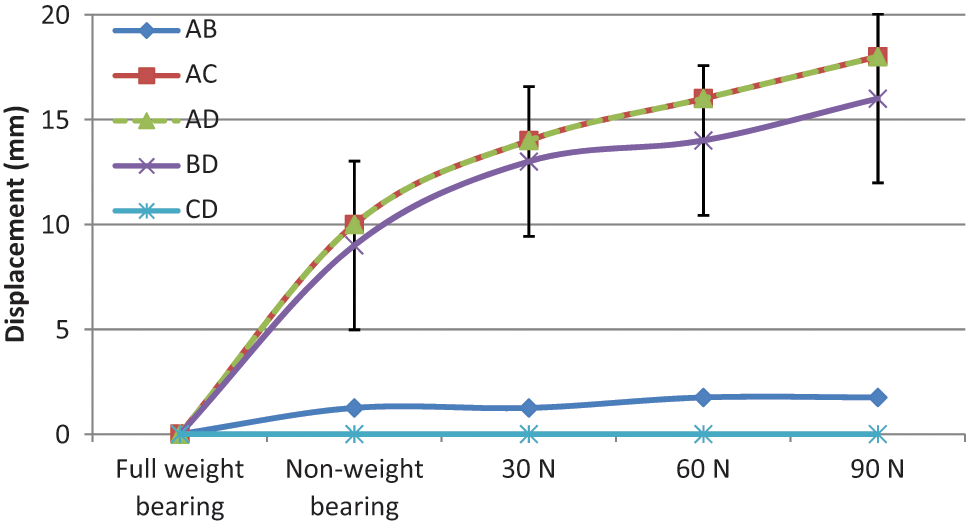
The averages of displacement between the markers in different static conditions.
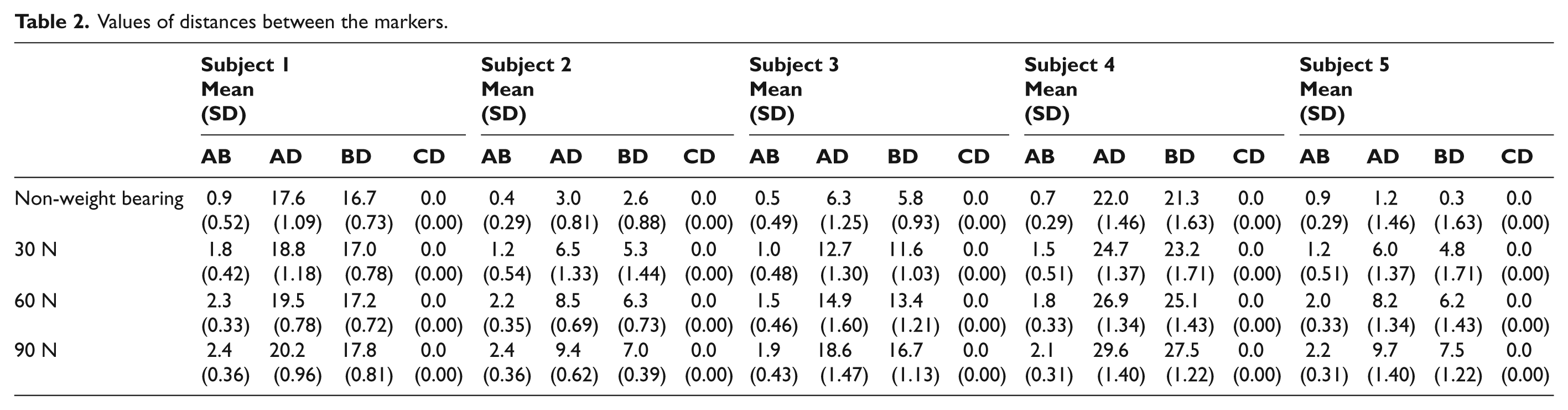
As we expected, the distance between the markers C and D was constant during the experiment, and no displacement happened between these two (ΔCD = 0). The distances between the markers for the five subjects are represented in Table 2.
Values of distances between the markers.
Discussion
Lack of pistoning is considered an important indicator of the successful functioning of the prosthetic suspension system. 11 In this study, the new method for measuring the pistoning between the soft liner and socket in transtibial prostheses, designed and developed in-house at Össur (Reykjavik, Iceland), was evaluated. The repeatability of the measurements by this new method was shown to be quite high. Nevertheless, this preliminary result needs to be investigated on a larger sample.
This amount of pistoning between full weight bearing and non-weight bearing positions seemed unreal to the authors. We found out that between these two positions the knee angle did not remain the same. The muscles’ reaction caused the knee to bend slightly which resulted in a sudden change in the pistoning. In contrast, while adding the loads (non-weight bearing position until 90 N), the pistoning increased constantly (8 ± 1.4 mm). It was interpreted as less change in the knee angle.
The amounts of vertical movement (pistoning) for our subjects support the findings of some previous studies.13,17,19,20 Based on our literature review, most of the researchers measured the displacement between the bone and the socket or the soft tissue by using different techniques in static position2,11,15-18,26,27 or during the gait.14,19-22,25 Some tried to mimic the gait by adding certain loads to the prosthesis.13,20 However, no research was found to measure the displacement between the Iceross Dermo® liner (thickness: 3mm) and the socket in transtibial or transfemoral prosthesis. In 2006, a non-contact sensor was used in a study to check pistoning between the stump and socket during the gait in a supracondylar socket with Pelite liner. However, the authors could not measure the pistoning between the silicon liner and the socket using this sensor. 14 The above-mentioned methods are complicated for measuring the pistoning between the liner and the socket and they are impossible to be performed in rehabilitation clinics by every prosthetist. Utilizing the camera brings the possibility of easy and fast determination of pistoning between the liner and socket and it can be a safe method if X-ray exposure is a concern.14,25,28
This technique can also be used for measuring the pistoning in transfemoral prostheses. In our study, we could not examine the real pistoning during the gait (dynamic), but we tried to mimic the gait by using different loads.13,20 Moreover, to optimize this method the knee angle should be controlled to obtain more accurate results.
Conclusion
We introduced a new method for evaluating the pistoning between the prosthetic liner and socket in transtibial amputees. The vertical movement can be measured by this simple technique by every prosthetist in any clinical setting. We hope it can help to enhance the quality of gait and patient’s satisfaction in lower limb amputees. Future research is also recommended for different liners and with a larger sample size to verify this preliminary result.
Footnotes
Acknowledgements
The authors would like to thank Mr. Stefán Karl Sævarsson and Mr. Scott Eliott for their help and encouragement.
Funding
This study was supported by Malaysia UM/MOHE/HIR Project No. D000014-16001 and Össur (Reykjavik, Iceland)
Conflict of interest
The authors have no conflict of interest.