
Abstract
A high degree of gait symmetry is characteristic of healthy gait. The aim of this study is to examine the symmetry of various gait parameters in subjects with unilateral trans-tibial amputation over a range of acceptable anteroposterior translational and tilt alignments, and further to examine if a consistent alignment of highest symmetry can be found. Acceptable alignments were determined by bench, static and dynamic testing on level and non-level surfaces. A total of 15 kinetic and kinematic parameters were then measured in the seven subjects participating in this study. Results indicate that some parameters show consistently higher symmetries, particularly the vertical ground reaction force parameters and the stance duration, step length and time to full knee flexion during the swing phase. Symmetries in other parameters such as knee flexion at loading response, acceleration impulse, and peak anteroposterior propulsive force seem to have little relevance in determining whether the gait pattern for that prosthetic alignment is acceptable or not. While analysis of the symmetry of more relevant gait parameters may assist the prosthetist in consistently and objectively identifying a most symmetrical alignment within the acceptable range, further clinical study is required before any conclusions can be drawn regarding evaluation of symmetry as a tool in defining any optimum alignment.
Introduction
Alignment of a lower limb prosthesis is the three-dimensional orientation of the socket with respect to the prosthetic foot, and is an important factor in optimizing the gait of subjects with amputation. A misaligned prosthesis affects the gait pattern (Hannah et al. 1984; Sanders et al. 1993; Pinzur et al. 1995; Rossi et al. 1995), and may result in problems such as abrasion and irritation at the interface of the socket and the stump.
The alignment of trans-tibial prostheses is generally defined in terms of six parameters: anteroposterior (AP) translation (or shift) of the socket relative to the foot; AP tilt (or rotation); mediolateral (ML) translation of the socket relative to the foot; ML tilt (or rotation); length of the prosthesis and the toe-out angle (Berme et al. 1978; Zahedi et al. 1986). The AP and ML tilt and translation of the socket relative to the foot are illustrated in Figure 1. Although the prosthetic alignment can be measured using a conventional plumb-line, this approach suffers from low accuracy and poor repeatability. Berme et al. (1978) developed a socket axis locator, which allowed the six alignment parameters of the prosthetic socket to be measured with good repeatability, and Sin et al. (1999) described a simple jig allowing accurate and reliable measurements of the alignment of the prosthetic foot relative to the socket.
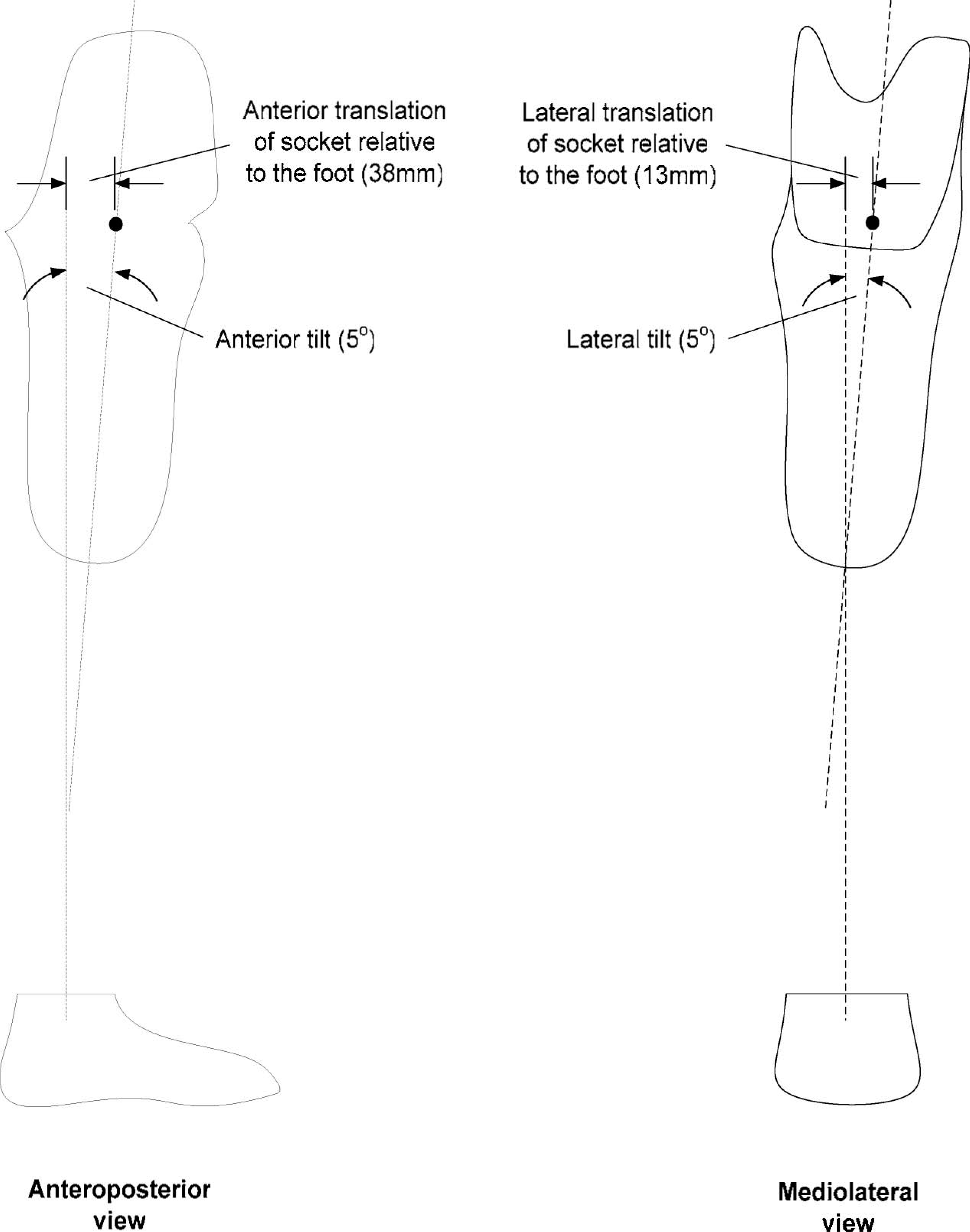
Prosthetic alignment parameters in the anteroposterior and mediolateral directions. The initial bench alignments are stated in parentheses.
In current clinical practice, the prescribed alignment is determined by bench, static and dynamic alignment procedures, and is that assessed by a prosthetist to be free from any observable gait abnormality, with due regard to the subjects' comments regarding any discomfort, instability or poor performance. However, the results of these subjective assessments vary both with the experience of the prosthetist and the tolerance of the subject, producing a range of acceptable alignments (Zahedi et al. 1986), rather than a truly optimal alignment. Within this range of acceptable alignments there is still conjecture on whether a truly optimal alignment exists that will be unique for a given patient, prosthesis and level of activity. Sin et al. (2001) showed that non-level walking during dynamic alignment reduces the number of acceptable alignments found in level walking and Zahedi et al (1986) concluded from the non-uniform distribution of data from 283 alignment trials with 10 trans-tibial and 10 trans-femoral prostheses that a true optimum alignment of the prosthesis does exist. If a unique optimum alignment does exist, then the problem is the objective and consistent determination of which of the acceptable alignments is optimal.
Dynamic alignment of the prosthesis relies on the observational and analytical skills of the prosthetist. Without instrumentation, skilled prosthetists can achieve an alignment acceptable for the individual needs of their patients. Dynamic alignment allows fine-tuning of the prosthetic alignment, where the prosthetist can observe the relative differences between the prosthetic and contralateral limbs. The contralateral limb serves as a dynamic benchmark for the function of the prosthetic limb for a given individual, and experience will allow the prosthetist to take into account subtle asymmetries in the gait. A generally symmetric gait pattern is indicative of healthy gait, and is one of the aims of gait rehabilitation following lower limb amputation (Baker and Hewison 1990; Isakov et al. 1996). Gait symmetry has the biomechanical advantage of decreased excursion of the centre of mass during each gait cycle, and therefore provides for more energy efficient ambulation (Skinner and Effeney 1985). However, Winter and Sienko (1988) pointed out that the prosthetic and contralateral limbs constitute two distinct biomechanical systems, and the gait pattern on the prosthetic side is therefore not a truly symmetric image of the sound limb (Bagley and Skinner 1991; Isakov et al. 2000). Considerations of symmetry or asymmetry are further complicated by the fact that the degree of symmetry exhibited also depends on which gait parameter is being considered. Isakov et al. (1997) found a distinctly asymmetric double support time (ratio: 0.74), while Hirokawa (1989) found that the step length and stance duration to have symmetry ratios of 0.98 and 0.96, respectively. Dingwell et al. (1996) found improvements in gait symmetry in subjects with unilateral trans-tibial amputation following feedback training, but indicated that the asymmetries of different variables were not necessarily related. As a result, it was suggested that more work was required to identify the gait variables for which attaining a more symmetrical gait pattern is most beneficial.
The aim of this study is therefore to quantify the asymmetries of various gait parameters in subjects with unilateral trans-tibial amputation, one facet of what the prosthetist observes and interprets when dynamically aligning a prosthesis. The asymmetries were examined over a range of acceptable antero-posterior translational and tilt alignments, to establish if any of these parameters show consistently higher symmetry than others, and also to establish if a consistently least asymmetric alignment can be found amongst the determined range of acceptable alignments.
Methodology
Subjects and prostheses
Seven volunteers aged from 26 – 58 years (Table I) were recruited for this study under the selection criteria of: (i) unilateral trans-tibial amputation; (ii) a prosthetic history of unassisted pain-free gait of two years or longer; (iii) no observed gross gait deviation or asymmetry, and; (iv) a high or very high Day's activity level (Day 1981). Ethical approval and subjects' written informed consent were obtained prior to their participation in this study.
Anthropometric and prosthetic history data of the subjects taking part in this study.
All subjects were using patellar-tendon-bearing (PTB) socket prostheses fitted with a solid ankle cushion heel (SACH) foot at the time of recruitment, but as some of these prostheses were exoskeletal and of fixed alignment, a new endoskeletal prosthesis with supracondylar PTB socket was therefore provided for each subject for the purposes of this study. To minimize the variances of fit and comfort among the sockets, the casting and rectification procedures were performed by a single prosthetist. Two sliding socket adapters were assembled into the prosthesis to extend the range of alignment change in addition to the conventionally used pyramid socket adapter, and a suitable SACH foot was prescribed for each subject. The experimental prostheses were then fitted to individual subjects following the conventional static and dynamic alignment procedures. Appropriate adjustments of the trim-line and the fit of the socket and soft liner were made where necessary to ensure the comfort and the snug fit of the socket. The height and the toe out angle of the prostheses were set to be symmetrical to the sound side, and the initial alignment of the prosthesis was set according to Radcliffe and Foort (1961), such that the socket anterior and mediolateral tilts were both 5°, and the socket was set 38 mm ahead of and 13 mm lateral to the centre line of the shank of the tube adapter (Figure 1). Subjects were asked to wear the same footwear that they were accustomed to throughout the experiment.
Range of acceptable alignments
The prosthetic alignment was quantified by a special alignment jig (Figure 2) designed by Sin et al. (1999). This consists of a socket axis locator described by Berme et al. (1978) and alignment table with an adjustable socket mount for prescribing prosthetic alignment during the assembly of the prosthesis. The Cartesian co-ordinate system and the unique axis adopted were exactly the same as that defined by Berme et al. (1978). Only the effects of different AP alignments were considered in this study. The AP socket translation relative to the foot was varied in 5 mm increments, and the AP tilt in 1° increments, with ML alignments kept at 5° tilt and 12.5 mm lateral translation of the socket relative to the foot (Figure 1). The alignment jig has a resolution of 1 mm and 1° (the marked intervals), and showed good intra- and inter-tester reliabilities (Sin et al. 1999).
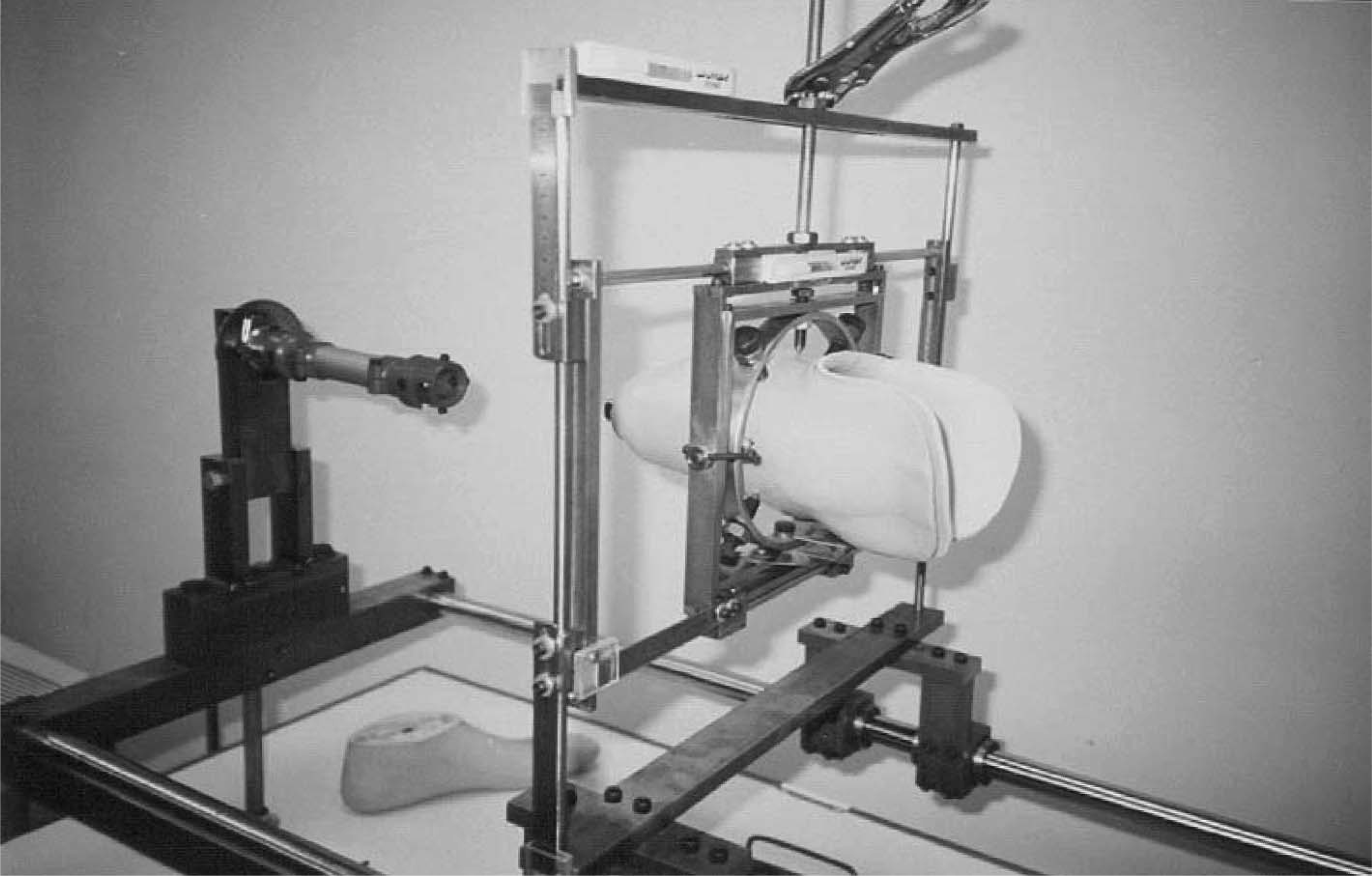
Purpose-built frame for setting prosthetic alignments.
As non-level walking is more demanding than level walking, and it has been shown that the acceptable alignment range for non-level walking is a smaller subset of that for level walking (Sin et al. 2001), both level and non-level walking trials were used to define the acceptable alignment range. The non-level walking trials consisted of a 15-step flight of stairs (135 mm riser and 245 mm depth), and a 4-m long ramp with slope of 1 in 10. The alignment was deemed as acceptable if the subject reported it to be comfortable, and no gait deviation could be observed by two prosthetists. Alignments were then changed and the evaluation process was repeated until the boundary of the acceptable alignment range was defined (Sin et al. 2001). The acceptable alignments were defined by varying the translation and tilt independently and randomly in 1° increments to establish the four boundary points of maximum and minimum tilt at 0 mm translation, and also in 5 mm increments to determine the maximum and minimum translation of the socket relative to the foot at 0° tilt. The alignments were also randomly varied with equal incremental increases in tilt and translation (e.g., ±1° and ±5 mm; ±2° and ±10 mm, etc.) to record the boundary points along these four directions. As a result, the boundary of acceptable alignments was found along eight directions from the origin defined by shift in translation or tilt alone, or equal shift in both values.
Data acquisition
Once the range of acceptable alignments had been determined, as above, gait analysis was performed for each alignment within that range along the eight directions from the origin defined by shift in translation or tilt alone, or equal shift in both values at intervals of 5 mm and 1°, as outlined. Gait analysis was performed using two force platforms (Advanced Mechanical Technologies, Inc., USA) and a motion analysis system (VICON 370, Oxford Metrics, UK) to determine a total of 15 gait parameters (Table II), which are commonly measured in clinical gait analysis using standard equipment.
Listing of the measured gait parameters, and their abbreviations and units.
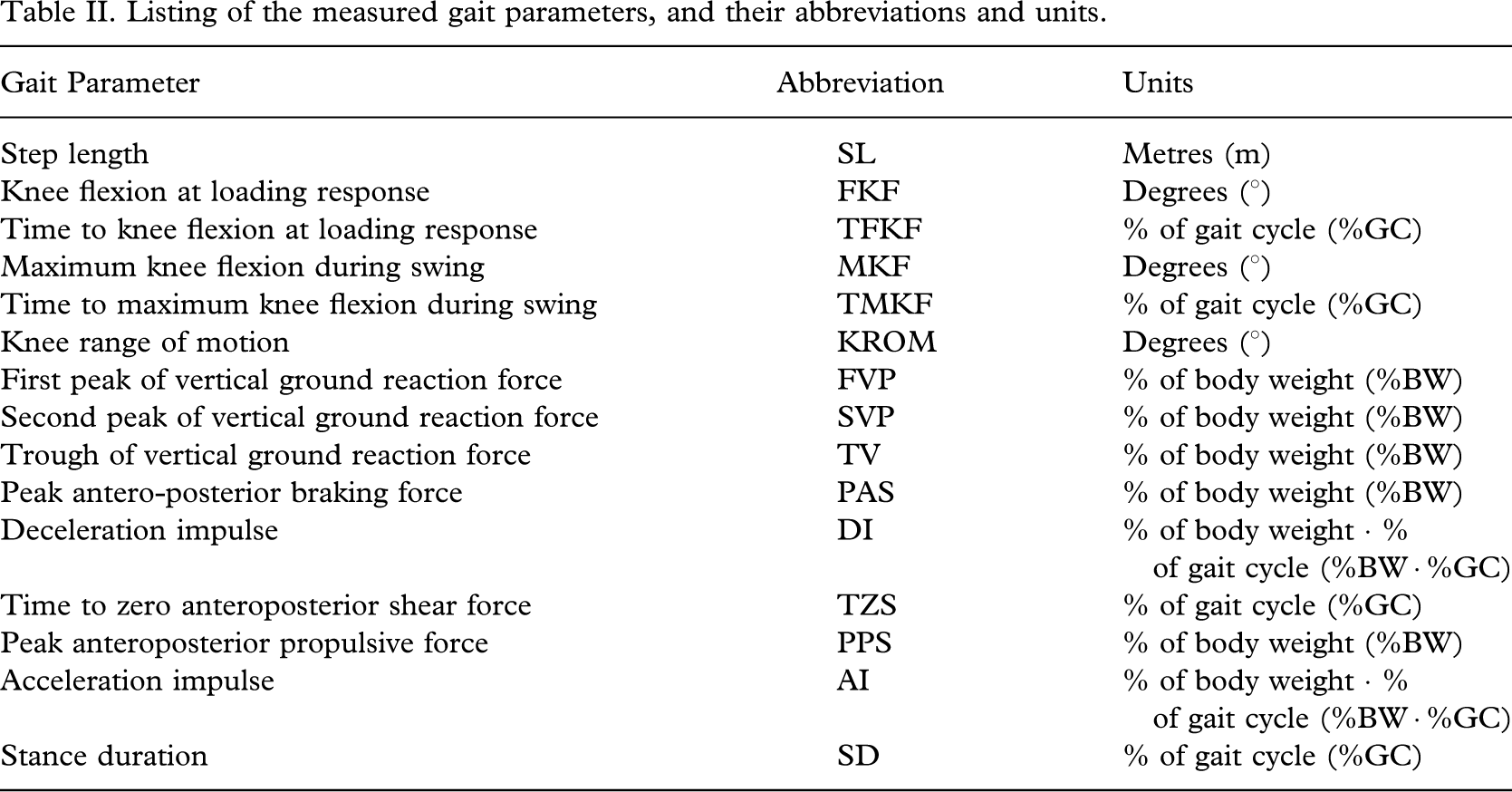
All of the temporal-distance and force platform parameters were recorded simultaneously at sampling rates of 60 Hz and 240 Hz, respectively. Reflective markers were placed at the left and right greater trochanter, lateral epicondyle, and lateral malleolus, or equivalent positions on the prosthesis. Skin markings were used to ensure reproducible placement of the markers. Calibration of the motion analysis system showed the linear accuracy to be 2 mm. Subjects were allowed to walk freely for at least 5 min with their own shoes to re-ascertain that the prosthetic alignment was acceptable and become accustomed to the alignment, and the 15 parameters (Figures 3 and 4) were measured for each acceptable alignment in each subject, varied in random order.
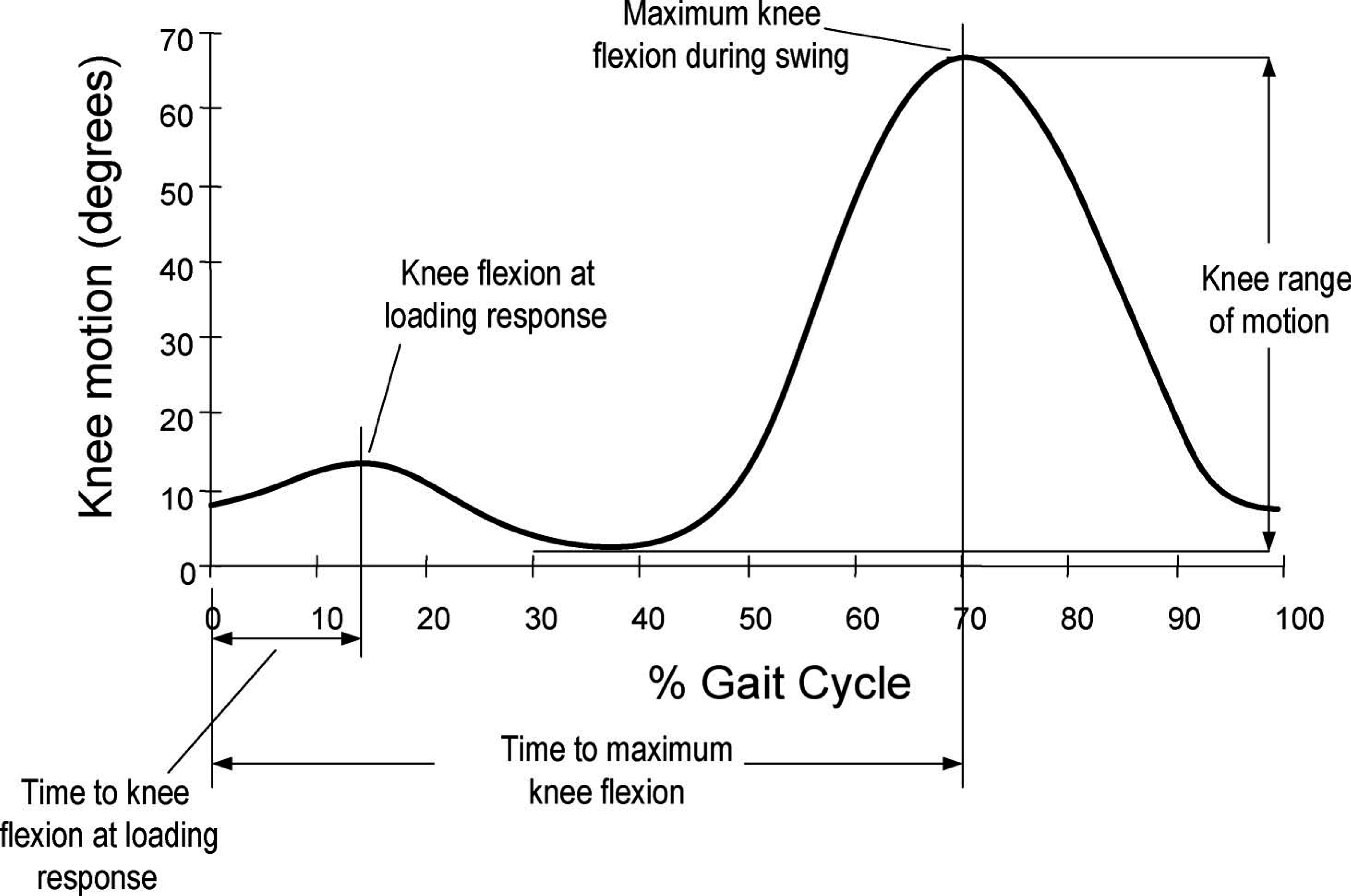
Graphic representation of the kinematic gait parameters recorded for each subject. The step length is not illustrated, but was also measured.
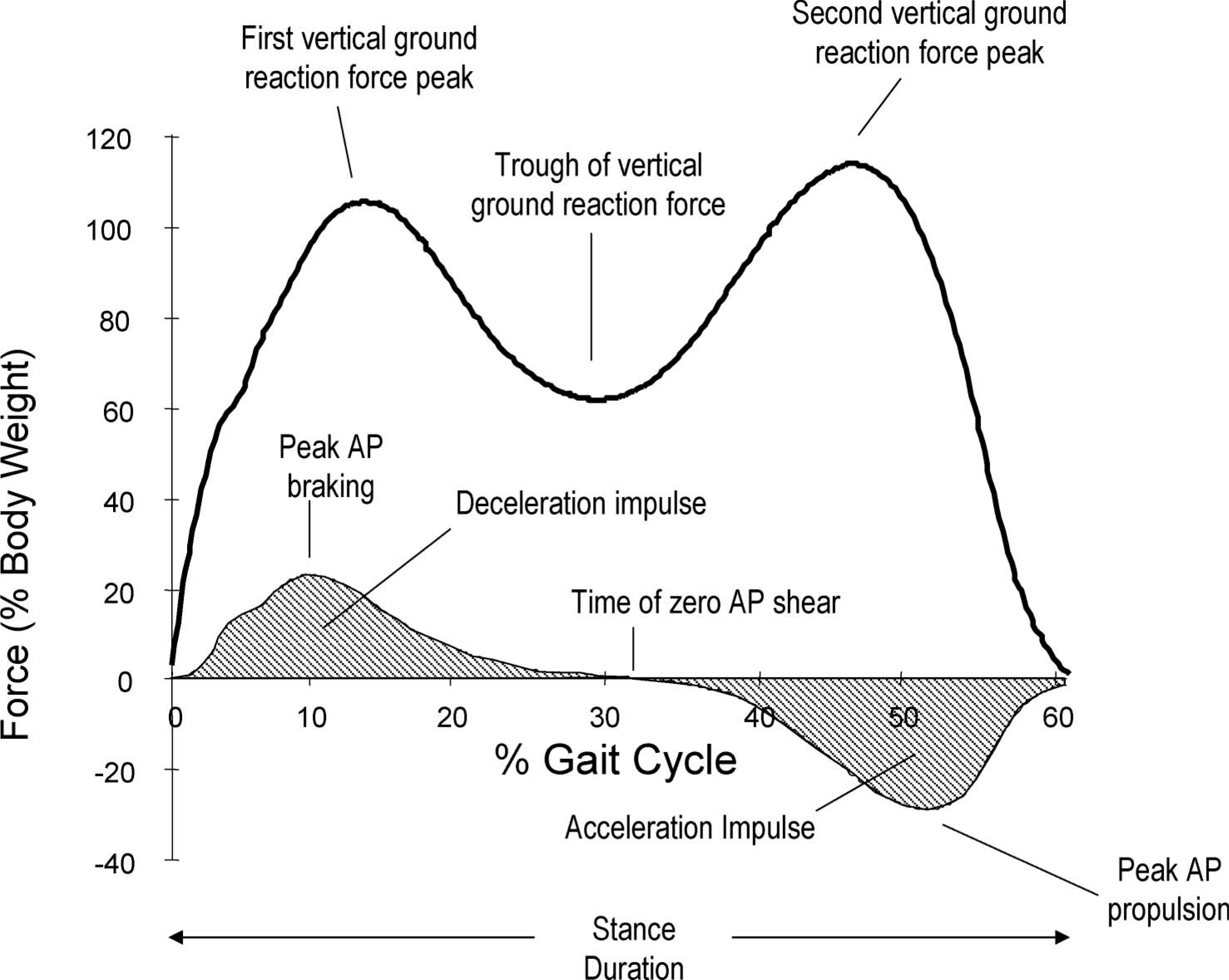
Graphic illustration of the dynamic gait parameters measured for each subject. The acceleration and deceleration impulses are the shaded areas under the shear force curve. A complete list of parameters with abbreviations and units is given in Table II.
The subjects were asked to walk along a 10-m walkway at a self-determined speed, which was also recorded. Gait patterns of five gait cycles trials were recorded for each alignment setting, and averaged. All kinetic data were normalized by the subjects' individual body weight. The subjects were then allowed to rest for approximately 20 min while the alignment of the prosthesis was changed, and the above process was repeated until data had been recorded for all of the acceptable alignments for that subject. In order to avoid fatiguing the subjects, gait analysis was typically conducted over 2 – 3 separate days, depending on the number of acceptable alignments.
Calculation of symmetry indices
All of the 15 gait parameters recorded were compared to the same values obtained from the sound limb, and an index was calculated for each parameter by dividing the absolute difference between the two values by their mean, as described by Herzog et al. (1989). For reference, the authors have termed this the absolute asymmetry index (AAI) as the value of this index always positive, and the larger the value the greater the asymmetry (perfect symmetry is equivalent to a value of 0). The mean value of this index averaged across all seven subjects was used to rank the 15 parameters in order of symmetry, both for all of the acceptable alignments, and also for the single most symmetric alignment in each subject. This single most symmetric alignment for a particular subject was found by determining which of the acceptable alignments showed the lowest mean AAI value over all 15 parameters.
Once the ranking of parameters for the most symmetric alignments had been established, the consistency of this single most symmetric alignment was examined by removing the lowest ranking parameter, and recalculating the most symmetric alignment on the basis of the remaining 14 parameters. These remaining 14 parameters were then ranked again on the basis of the new most symmetric alignments, and the process repeated continuously until only one parameter remained. This sequential removal of the most asymmetric parameters allows the effect of the number of parameters considered on the determination of the most symmetric alignment to be examined.
Results
Acceptable alignments
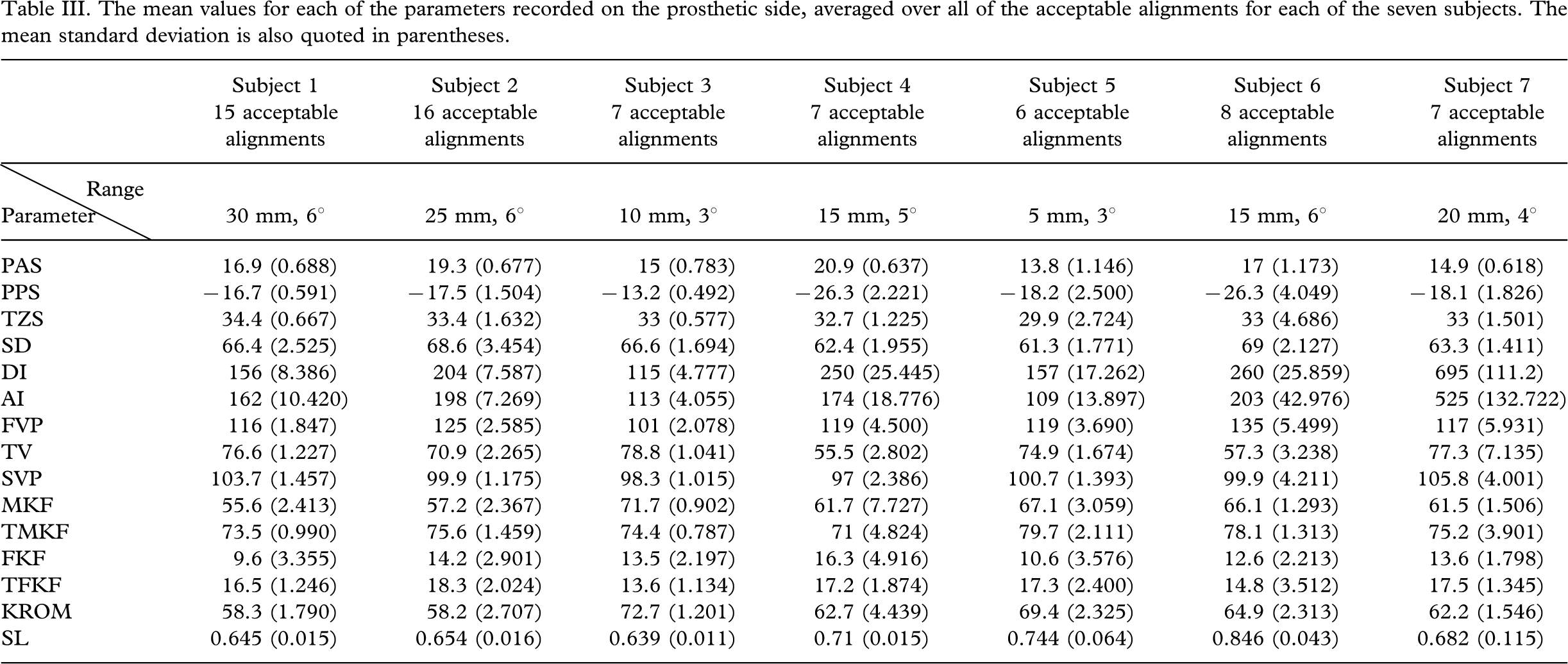
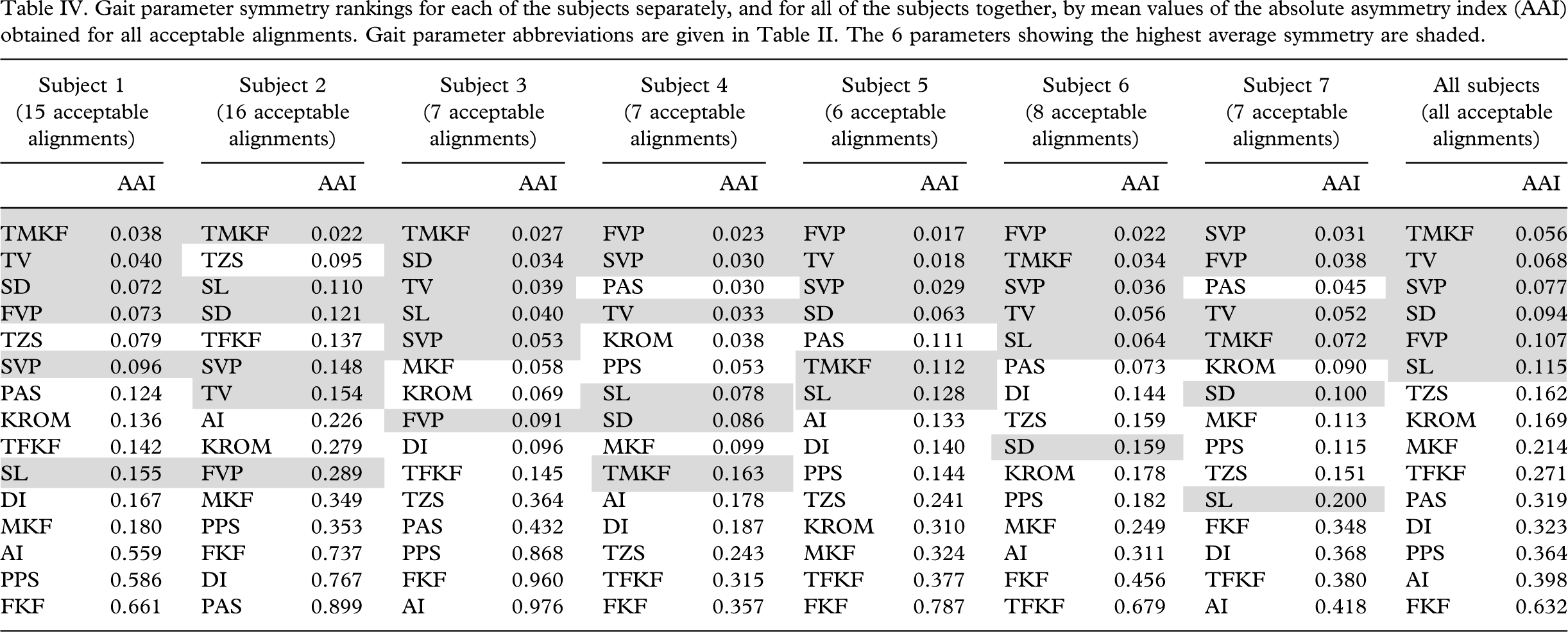
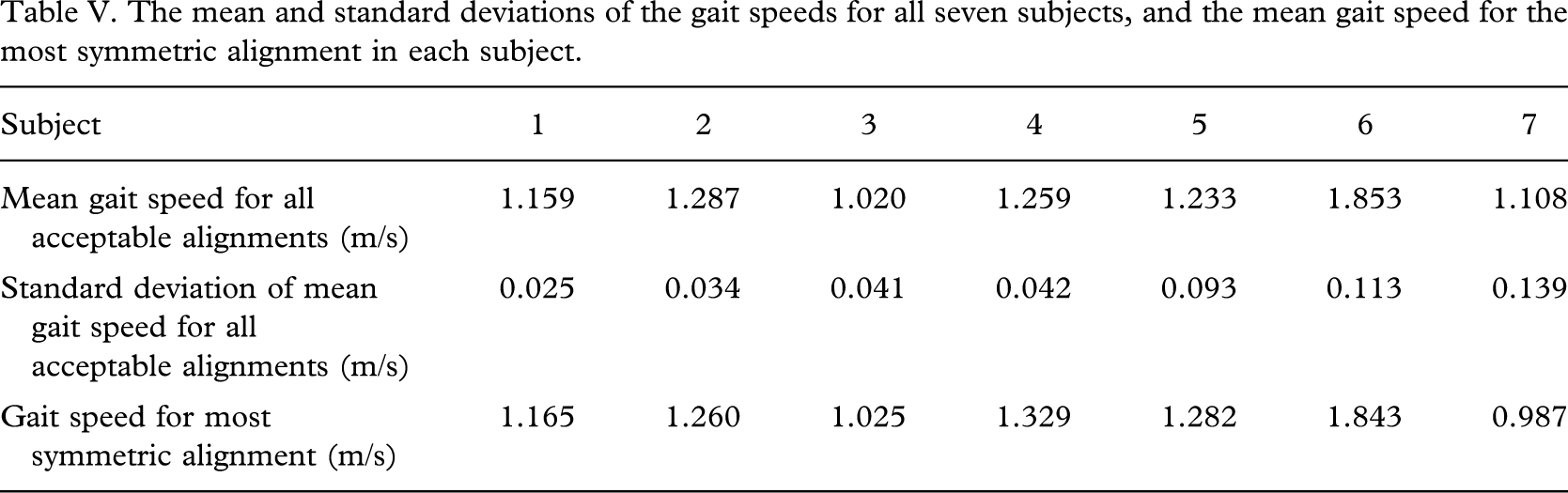
The number of acceptable alignments found ranged from six alignments (subject 5) to 16 alignments (subject 2), as shown in Table III, which shows the mean values of each of the 15 parameters averaged over all of the acceptable alignments, as well as the mean standard deviation. The range of acceptable alignments (in mm and degrees) for each subject is also shown in Table III. The mean AAI determined over all of the acceptable alignments for each of the 15 gait parameters in each of the seven subjects separately are shown in Table IV, listed in order of highest symmetry, with the lowest AAI values at the head of the columns. The mean AAI averaged over all acceptable alignments was also determined as a mean over all seven subjects (Table IV), and showed highest symmetries for the vertical ground reaction force parameters (the first and second peaks of the ground reaction force, FVP and SVP respectively, and the trough values between them, TV) and the kinematic parameters of stance duration (SD), step length (SL) and time to maximum knee flexion during swing (TMKF). It can also be seen from the results presented in Table IV that at least three, and on average four of these six parameters (FVP, SVP, TV, TMKF, SD and SL) were in the top six most symmetric parameters of each subject. Only slight variations in gait speed were seen across the acceptable alignments (Table V).
The mean values for each of the parameters recorded on the prosthetic side, averaged over all of the acceptable alignments for each of the seven subjects. The mean standard deviation is also quoted in parentheses.
Gait parameter symmetry rankings for each of the subjects separately, and for all of the subjects together, by mean values of the absolute asymmetry index (AAI) obtained for all acceptable alignments. Gait parameter abbreviations are given in Table II. The 6 parameters showing the highest average symmetry are shaded.
The mean and standard deviations of the gait speeds for all seven subjects, and the mean gait speed for the most symmetric alignment in each subject.
Most symmetric alignment
The most symmetric alignment was determined as the alignment that showed the lowest mean AAI value over all 15 parameters for a particular subject. No obvious similarities were seen in the locations of most symmetric alignments between subjects. The parameters were also ranked in order of symmetry using the single most symmetric alignment for each subject, instead of all acceptable alignments, as described in the methodology. The resulting order of removal of parameters is shown in Table VI, along with the ranking results for all acceptable alignments for comparison. It can be seen that the general ranking of the parameters when only the most symmetric alignment is considered is roughly similar to that for all acceptable alignments, although the step length (SL) is rated higher in the most symmetrical alignment, while the time to maximum knee flexion (TMKF) is rated lower.
Comparison of parameter ranking by symmetry for all alignments (AAI) and for the single most symmetric alignment (AAI). Details of the ranking schemes are given in the text.
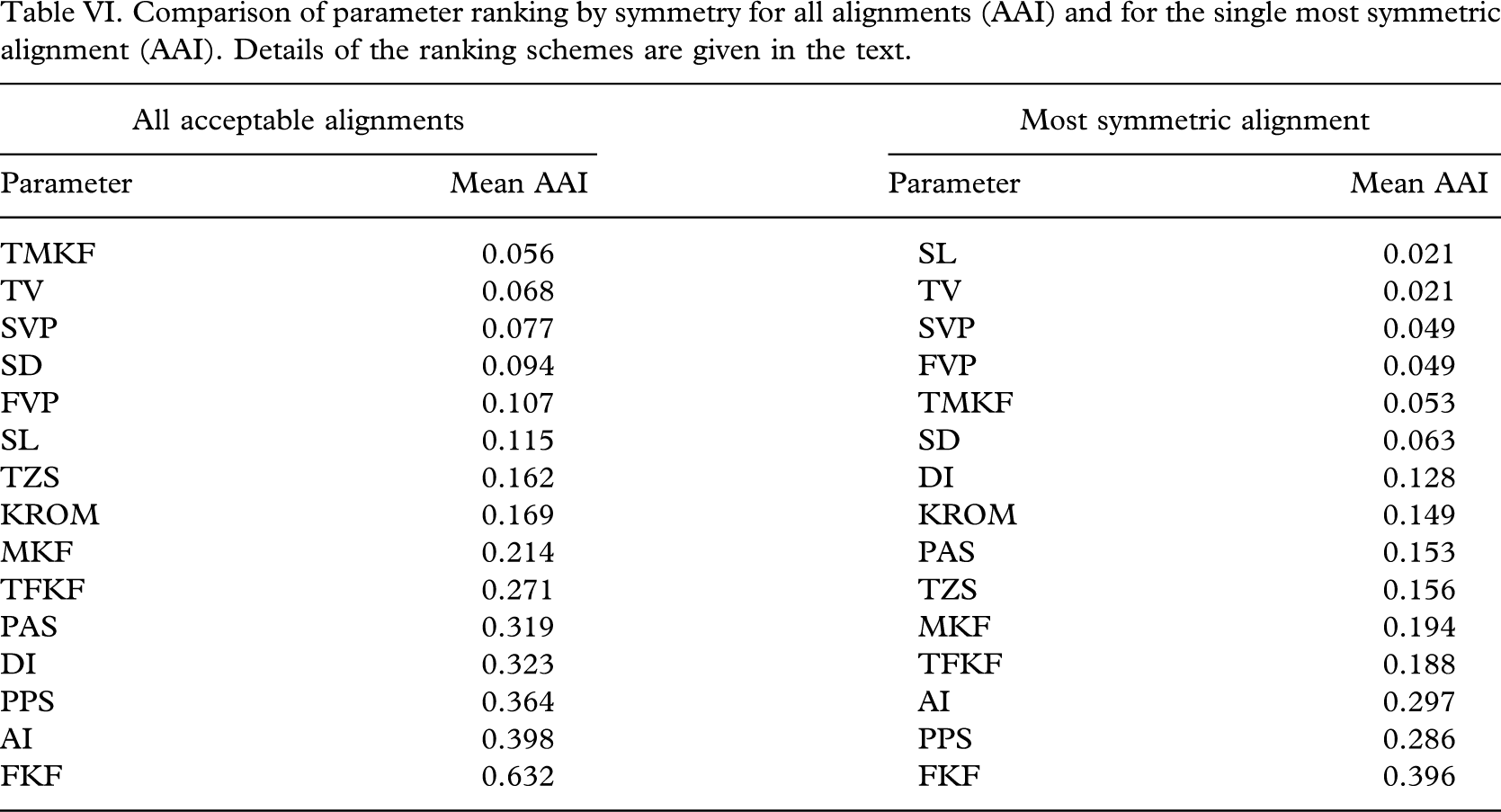
The six most symmetric parameters (FVP, SVP, TV, TMKF, SD and SL) were consistent irrespective of whether the most symmetric alignment or all acceptable alignments were considered. The gait speed at the most symmetric alignment was generally similar to the mean gait speed over all of the acceptable alignments (Table V).
The sequential removal of parameters of lowest symmetry involved the recalculation of the most symmetric alignment, and allowed the effect of selective parameter removal on the determination of the most symmetric alignment to be observed. In general, the alignment determined to be most symmetric was not constant, but depended somewhat on the number of parameters. This was observed when only a few parameters were considered, and the removal of one parameter has a large effect on the calculated mean AAI values, causing the determined most symmetric alignment to vary. As the total number of parameters increases, then the addition or removal of another parameter has proportionally less effect on the overall mean AAI value, and this was observed as the most symmetric alignment tended to vary when less than 3 or so parameters were considered, but typically remained constant when more parameters were considered. This is illustrated by the fact that in 6 of the 7 subjects, the alignment indicated to be most symmetric by the 6 most symmetric parameters (FVP, SVP, TV, TMKF, SD and SL) was consistent until at least 12 parameters were included. In subjects 1 and 7, the alignment indicated to be most symmetric by the 6 most symmetric parameters proved to be the most symmetric alignment for all 15 parameters, and in subjects 2, 4 and 5, the alignment indicated to be most symmetric by the 6 most symmetric parameters was the most symmetric for all parameters except the least symmetric (knee flexion at loading response, FKF). The exception was subject 6, which showed slightly more fluctuation in most symmetric alignment with the number of parameters considered. Apart from the most symmetric alignment indicated by the six most symmetric parameters, two other alignments were also found to be most symmetric, depending on the number of parameters considered.
Discussion
The authors have chosen 15 kinetic and kinematic gait parameters for analysis in this study, on the grounds that these are commonly used gait parameters that do not require any equipment other than that found in a standard gait laboratory. Gait symmetry has been quantified using an asymmetry index (AAI) between the sound and prosthetic limbs, similar to that of Herzog et al. (1989). Strictly speaking, the mean asymmetry for a single parameter in a particular subject is more appropriately defined by a non-rectified version of this index (where the index is negative if the parameter is less than that on the sound side, and positive if it is greater) similar to that used by Dingwell et al. (1996), which reduces the effect of experimental and recording errors causing the index to fluctuate about zero for different alignments. However, values calculated for this index were found to be very similar to the AAI, and had no effect on the ordering of parameters, and therefore AAI was used throughout for simplicity.
The results presented show some of the parameters recorded to have low symmetry values, the lowest being the knee flexion at loading response (FKF), which had a mean AAI of 0.632 (Table IV). Nonetheless, some of the parameters are consistently symmetric between the prosthetic and sound sides. Step length (SL) and stance duration (SD) were both found to be highly symmetric between the prosthetic and contralateral sides, with values similar to those found by Hirokawa (1989). Other parameters shown to exhibit consistently high symmetries were the vertical ground reaction forces (FVP, SVP, TV), related to the force at the socket-stump interface, and the time to maximum knee flexion (TMKF). Overall, while the altered biomechanics of the prosthetic side mean that the gait is not symmetrical to the sound side in all respects, some parameters clearly appear to be consistently symmetrical between the sound and prosthetic sides. The ranking of gait parameters by symmetry was similar regardless of the subject (Table IV) or whether all acceptable alignments or the most symmetric alignment alone was considered (Table VI).
It therefore appears that some useful information on acceptable alignments can be gained from examination of the symmetry of gait in subjects with unilateral trans-tibial amputation, as asymmetry in the vertical ground reaction forces (first peak, trough and second peak values), the stance duration and the time to maximum knee flexion during the swing phase would tend to indicate an alignment that may not be acceptable. There are several possible reasons why some of the parameters show very low symmetries while others are highly symmetric. Even in normal gait some parameters are likely to be more asymmetric than others, and as the ground reaction forces are generally dominated by body weight, they are therefore more likely to show less variation and generally higher symmetries. It is almost impossible to walk without producing a ground reaction force on one side, but relatively simple to walk without any knee flexion or extension on the same side. Asymmetry in a particular parameter may be because of several reasons:
Simply the fact that this parameter is not relevant to healthy prosthetic gait;
That the parameter is relevant to healthy prosthetic gait, but the asymmetry is a reflection of the biomechanical difference between the prosthetic and contralateral sides; or,
That symmetry in this parameter is relevant to healthy gait, but can only be achieved at the expense of a certain level of symmetry in another parameter.
The judgments and compromises that the experienced prosthetist necessarily makes in dynamic alignment are likely to reflect the reasons behind the different symmetries of observable gait parameters.
In short, while symmetry of gait parameters can be used to determine the most symmetric alignment, it is difficult to establish which of the measured parameters are of most use in indicating this alignment. A highly asymmetric parameter may be equally indicative of (or sensitive to) the most symmetric alignment as a relatively symmetric parameter. Nonetheless, the alignments indicated to be most symmetric by using the six most symmetric parameters (SL, SD, TMKF, FVP, TV, and SVP) were generally and consistently found to be the most symmetric over most of the parameters considered, as shown by systematic removal of the lowest ranking parameters. While considering only a few parameters is bound to result in some fluctuation in the most symmetric alignment, all subjects showed some changes in the alignment determined to be most symmetrical as different numbers of parameters are considered, indicating that there is no single alignment that will give highest symmetry values in all parameters.
However, if the changes in parameter symmetry were simply due to random variation in walking rather than the changes in the alignment, then the most symmetric alignment would be expected to vary randomly with the number of parameters considered. This was not found to be the case, and while the alignment indicated to be most symmetric by SL, SD, TMKF, FVP, TV, and SVP is not the most symmetric for all parameters in all cases, they do indicate an alignment which is fairly consistently found to be the most symmetric with increasing number of parameters considered.
This study is limited in that only alignment changes in AP tilt and AP translation of the socket relative to the foot were considered and data were recorded for 5 mm and 1° incremental changes in AP translation or tilt, respectively, or equal incremental changes in both AP translation and tilt, due to experimental time constraints. Therefore, not all of the acceptable alignments were examined, and any truly most symmetric alignment might not have been included within the defined acceptable range. However, the aim of the study was to examine the effect of changes within an acceptable alignment range on gait parameter symmetries, rather than to determine any truly most symmetric alignment. Experimental time constraints also meant that no data were obtained for deliberately misaligned prostheses, and this is a major limitation of the study, as there is no data as to how the symmetries of the parameters change once the alignment is set beyond the acceptable range.
Inclusion criteria and experimental time requirements also meant that only seven subjects were included in this study. However, the results obtained were generally consistent among subjects. Only a limited time was available to the subjects to become accustomed to the altered prosthetic alignment, and so the results of this study only represent the instantaneous responses. The effects of gradual adaptation to the new alignment could not be taken into account due to the experimental design. The ability of the musculoskeletal system to adapt to changes in prosthesis alignment may also mean that several acceptable alignments are equally ‘optimal’ and no unique optimum exists. Even if a unique optimum does exist, then it is still unclear whether or not this alignment can be defined in terms of gait symmetry. While no definite conclusions regarding the existence of a unique most symmetric alignment can be drawn from this study, the consistent ranking of gait parameter symmetries nevertheless indicates that further studies into the reasons behind this may give a clearer picture of the effect of gait alignment on symmetry, and in particular, which parameters are most relevant to and indicative of healthy gait. It is also recommended that a longitudinal study be carried out to determine if any clinical benefits are obtained using the alignment giving the highest overall symmetry for the six most symmetric gait parameters (FVP, TV, SVP, SD, SL and TMKF).
However, it should also be noted that if no benefit is found using this alignment, it may equally mean that the alignment giving optimum symmetry in these six parameters is not an adequate method of determining the optimum alignment, or simply that an optimum alignment does not exist. Issues surrounding optimum alignment are clearly far from straightforward, and even if a unique optimal alignment exists and can be defined in terms of gait symmetry, identifying parameters of sufficient relevance to the optimum alignment yet of adequate sensitivity may be a complex task. This study only examines the effects of changes in AP alignments, whereas a truly optimum alignment would have to be defined in terms not only of AP translation and tilt, but also ML translation and tilt, toe-out angle, and prosthesis length, further complicating the task.
Conclusions
Truly symmetric gait over all parameters is not found between prosthetic and sound limbs, presumably due to the distinct biomechanical systems between the two sides. Nevertheless, symmetry is maintained in some gait parameters. The reasons for the range of symmetries seen in gait parameters are not clear, and asymmetry in a particular parameter may not necessarily be indicative of an unacceptable alignment. However, consistently symmetric values for the vertical ground reaction forces (FVP, TV, SVP), stance duration (SD), step length (SL), and time to maximum flexion during the swing phase (TMKF) were found, and asymmetry in these parameters may assist the prosthetist in identifying unacceptable alignments. The alignment identified as most symmetric by analysis of these six parameters is reasonably consistent as further parameters are included in the analysis.
While the consideration of gait symmetry is of value to the prosthetist, further work is required to determine what levels of symmetry in which gait parameters may be more relevant to healthy prosthetic gait before any conclusions can be drawn regarding evaluation of symmetry as a tool in defining optimum (as opposed to acceptable) alignments.
Footnotes
Acknowledgements
This work was supported by a Central Research Grant of the Hong Kong Polytechnic University (Project no. G-V145).