
Abstract
The purpose of the study was to investigate which systematic effects of prosthetic misalignment could be observed with the use of the SYBAR system. The alignment of the prosthesis of five well-trained unilateral trans-tibial amputees was changed 158 in magnitude in varus, valgus, flexion, extension, endorotation, exorotation, dorsal flexion, and plantar flexion. Subjects walked over a distance of 8 m at a self-selected walking speed with the alignment of the prosthesis as it was at the start of the experiment (reference) and with each changed alignment. Two video cameras (frontal and sagittal) and a force plate of the SYBAR system (Noldus Information Technology, The Netherlands) were used to capture gait characteristics of the subjects. Temporal and spatial characteristics, the magnitude and timing of the ground reaction force (GRF), and the external joint moments were derived from these data. Despite the substantial perturbations to prosthetic alignment, only a few effects were observed in the temporal and spatial characteristics of gait, the magnitude and timing of the GRF, and the external joint moments. Only the pattern of the ground reaction force in the mediolateral direction and the joint moment around the ankle in the frontal plane during terminal stance showed a systematic effect when the alignment was set into varus and valgus or exorotation. It was concluded that using the SYBAR system in this study revealed little effect of perturbations in prosthetic alignment, for this group of patients, and for the selected parameters. It was questioned whether this is due to the relatively low resolution of the SYBAR system or the capacity of the well-trained subjects to compensate for the disturbance in alignment. It was suggested that the usability of the SYBAR system in clinical settings should be further explored.
Introduction
In the Netherlands, about 3300 lower-limb amputations are performed every year (Rommers 2000). Parts of the locomotor system are lost with the amputation. Because of that, function is partly lost. A prosthesis can compensate for these losses, depending on the properties and alignment of the prosthesis (Blumentritt et al. 2001; Culham et al. 1986). The alignment of the prosthesis is established by the relative positions of the different parts of the prosthesis (Isakov et al. 1994; Klute et al. 2001; Schmalz et al. 2002). From different studies examining trans-tibial amputees, it is known that the alignment influences different aspects of function. From Hannah et al. (1984); Huang et al. (2000); Isakov et al. (1994); and Schmalz et al. (2002), it is known that the energy expenditure rises with a misaligned prosthesis. Hannah et al. (1984) found that walking velocity and step frequency are negatively influenced by misalignment. In addition, the alignment influences the comfort of the prosthesis. A misaligned prosthesis can bring soreness and pain to the stump (Blumentritt et al. 2001; Klute et al. 2001; Summers et al. 1987). This affects the progress of the rehabilitation process. Thus, the alignment of the prosthesis must be as optimal as possible (Isakov et al. 1994). However, current prosthetic alignment is mainly based on the prosthetist's subjective judgement and the amputee's comments, with no clear guidelines for correct alignment (Blumentritt et al. 2001; Fridman et al. 2003; Isakov et al. 1994).
In line with the development of technology, new instrumentation has been developed that can be helpful in the alignment process of prostheses (Blumentritt et al. 2001; Zahedi et al. 1987). However, although the alignment of the prosthesis is most important during dynamic tasks like walking, most of these systems permit only static alignment. One of the systems that could be possibly used for dynamic alignment in clinical practice is the SYBAR system (Noldus Information Technology, The Netherlands) (Harlaar et al. 2000). This system for gait analysis consists of video cameras, a force plate, and an EMG recorder. It provides two-dimensional video images from which temporal and spatial gait characteristics can be deduced in each phase of the gait cycle. In addition, it provides data on the amplitude and direction of the ground reaction force (GRF) and a projection of the force vector on to the two-dimensional video images, which visualizes the net joint torques around the joints of the leg (Figure 1).

An example of the sagittal and frontal video image with the projection of the ground reaction force vector during terminal stance generated by the SYBAR-system.
The SYBAR system is a user-friendly setup which is designed to be used for gait analysis in a clinical setting and does not require laborious data analysis and interpretation in contrast to more advanced movement analysis systems.
From the literature, only a few studies are known that have investigated the effect of prosthetic alignment on the kinematics and kinetics of the gait pattern of trans-tibial amputees. Blumentritt et al. (2001) and Schmalz et al. (2002) analysed the effect of translating the foot in the sagittal and frontal plane, and foot plantar and dorsal flexion on walking velocity, stride length, and knee joint angle and moment. They found systematic effects of alignment in knee angular displacement and knee joint moments. Zahedi et al. (1987), in a study on repeatability of kinematic and kinetic gait data, showed that a difference in prosthetic alignment can result in a substantial change in net joint moments at the ankle. In spite of these studies, however, objective knowledge on the effect of prosthetic alignment on the gait pattern is scarce, and it covers only a part of all possible features that can be aligned. Moreover, these studies used advanced movement analysis systems and relatively complex inverse dynamics calculations to obtain their data. These techniques are not very accessible in clinical practice.
In the current study, the effect of several systematic misalignments of trans-tibial prostheses were analysed using the SYBAR system. The effect on several parameters that can be observed with the SYBAR system, i.e. spatio-temporal parameters, ground reaction force patterns, and net joint moments, was analysed. The purpose of this study was to investigate which systematic effects of prosthetic misalignment could be observed using the SYBAR system. Ultimately, these effects can be used in the future to identify and correct misaligned prosthesis in clinical practice.
Methods
Subjects
Five male trans-tibial amputees participated in the study. The criteria of inclusion were: able to walk with the prosthesis without any additional aid, wearing the prosthesis most of the day, following no rehabilitation treatment, and being satisfied with the current alignment of the prosthesis. The subject characteristics are listed in Table I.
Protocol
In this study, the SYBAR system (Noldus Information Technology, The Netherlands) was used to measure gait characteristics. From this system, two video cameras (frontal and sagittal) and a force plate were used. To synchronize the data of the force plate and cameras, an electronic pulse and a light signal were given simultaneously. Subjects walked over a distance of about 8 m at a self-selected walking speed under different conditions. Alignment of the prosthesis was different in each condition (Table II). As can be seen from Table II, the first and last condition involved walking with the reference alignment. The reference alignment was defined as the alignment of the prosthesis the subject had before entering the experiment and which had previously been optimized to the requirements of the prosthetist and patient. Changes in alignment were about 158 in magnitude in each orientation and were performed by an experienced prosthetist. After each change in alignment, subjects had several minutes time to get used to the new condition. At least three trials for each condition were collected. To prevent subjects consciously targeting the force plate, subjects were told not to pay attention to the force plate and walk as normally as possible.
Subject characteristics.
Variables
The following variables were measured for all conditions: the temporal and spatial characteristics of gait, the magnitude and timing of the GRF, and the external joint moments. These variables were chosen, based on the capabilities of the SYBAR system in a clinical setting.
Temporal and spatial characteristics of gait. The following temporal and spatial characteristics of gait were analysed from the video recordings (sample rate 25 Hz): length and duration of the stride, length and duration (normalized to duration of stride) of the step, duration of both double support phases (normalized to duration of stride), duration of the single support phase (normalized to duration of stride), step frequency, and walking velocity. Stride and step were defined according to Perry (1992). All variables were determined for the leg that stepped on to the force plate. For each condition, one representative trial for each subject was chosen to determine these variables. Generally, the chosen representative trial was the last trial for each condition, unless force tracings and remarks made during the experiment indicated that this could be an outlier with respect to the other trials of that condition. Duration could be determined directly from the SYBAR system. To be able to determine the length of the stride and step, a line with a known length was placed on the walkway at the height of the step. This line was used as a reference length to convert length on the monitor to real-world length.
Experimental conditions.
Intact leg stepped onto the force plate while using the reference prosthetic alignment
Ground reaction force. The GRF was captured at 100 Hz and analysed in three directions: mediolateral (Fx), anteroposterior (Fy), and upwards (Fz). For each walking condition, the following variables were determined (averaged over all trials of one condition for each subject): the magnitude and timing of the two Fx peaks, the magnitude and timing of the two Fy peaks, and the magnitude and timing of the two Fz peaks and the local minimum of Fz (Figure 2). Only with the reference alignment was the GRF of both prosthetic and intact leg measured; for all other alignments, only the GRF of the prosthetic leg was measured. Timing was normalized to stance time.
External joint moments. To investigate the external joint moment at the ankle, knee, and hip of the leg that stepped on the force plate, the distance between the centre of rotation of the joints and the ground reaction force vector was scored with the use of a self-designed ordinal scale (Figure 3). With this scale, the moment arm was scored −3 to + 3, according to the zone in which the GRF passed the joint. Thus, the true external moments were not calculated; merely the magnitude of the moment arm was analysed. This was done because the moment arms can be observed qualitatively from the SYBAR system, which displays the GRF-vector on the video images of the subject, while calculating real external moments would require digitizing of the video images and relatively complex calculations. For each walking condition, the same representative trial as that used for the temporal and spatial characteristics of gait was chosen for each subject to determine the joint moments in both frontal and sagittal plane for each phase of the gait cycle (Perry 1992).
Statistics
A comparison between the walking conditions was made for each variable with a non-parametric Friedman test. If a missing value was present, that value was set equal to the value of the reference alignment. A post hoc test was performed to detect the cause of possible significant difference (Siegel and Castellan 1988). The significance level was set at P < 0.05.
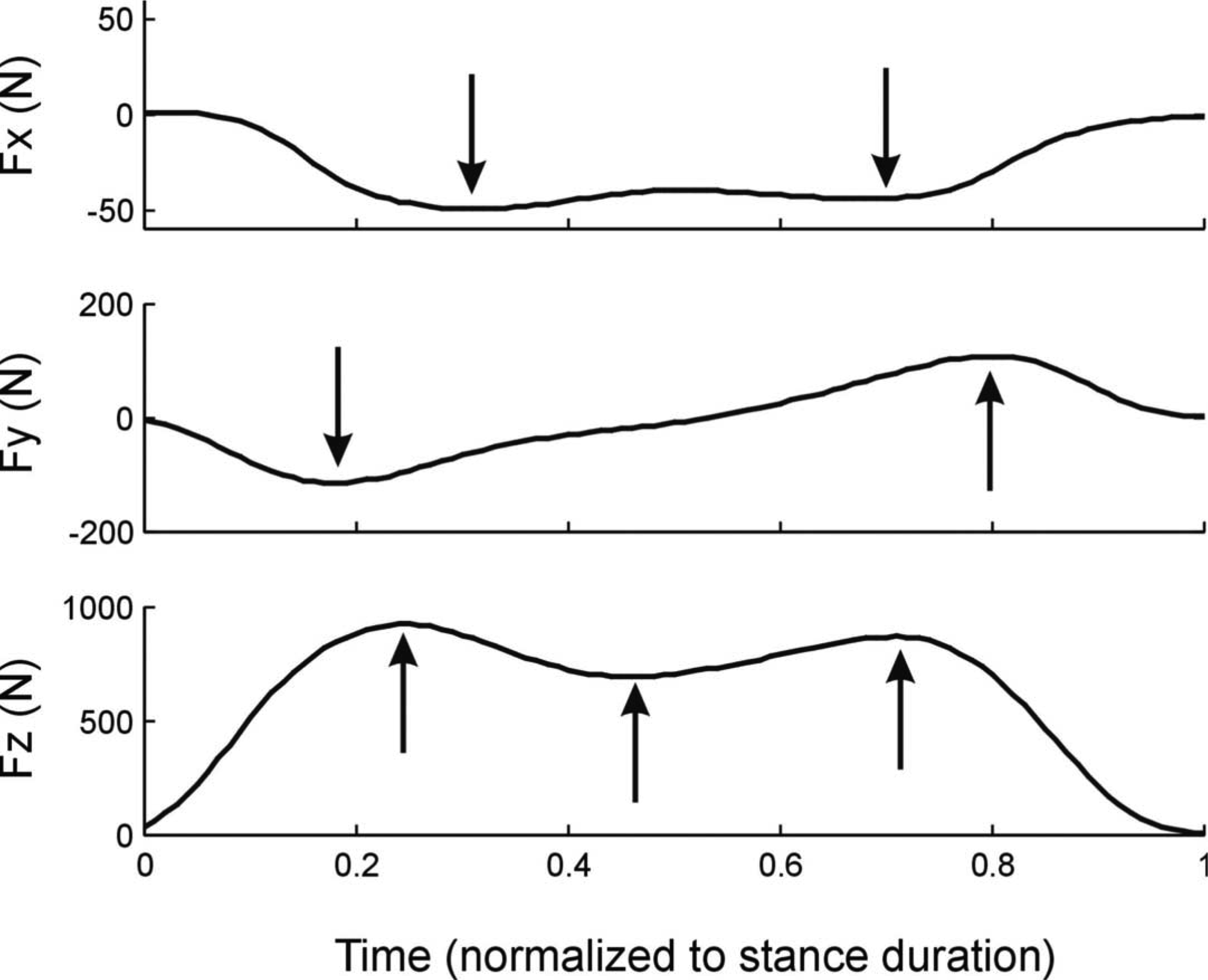
A typical example of the ground reaction force pattern in mediolateral (Fx), anteroposterior (Fy) and upward direction (Fz). Arrows indicate the quantified peaks for each signal.
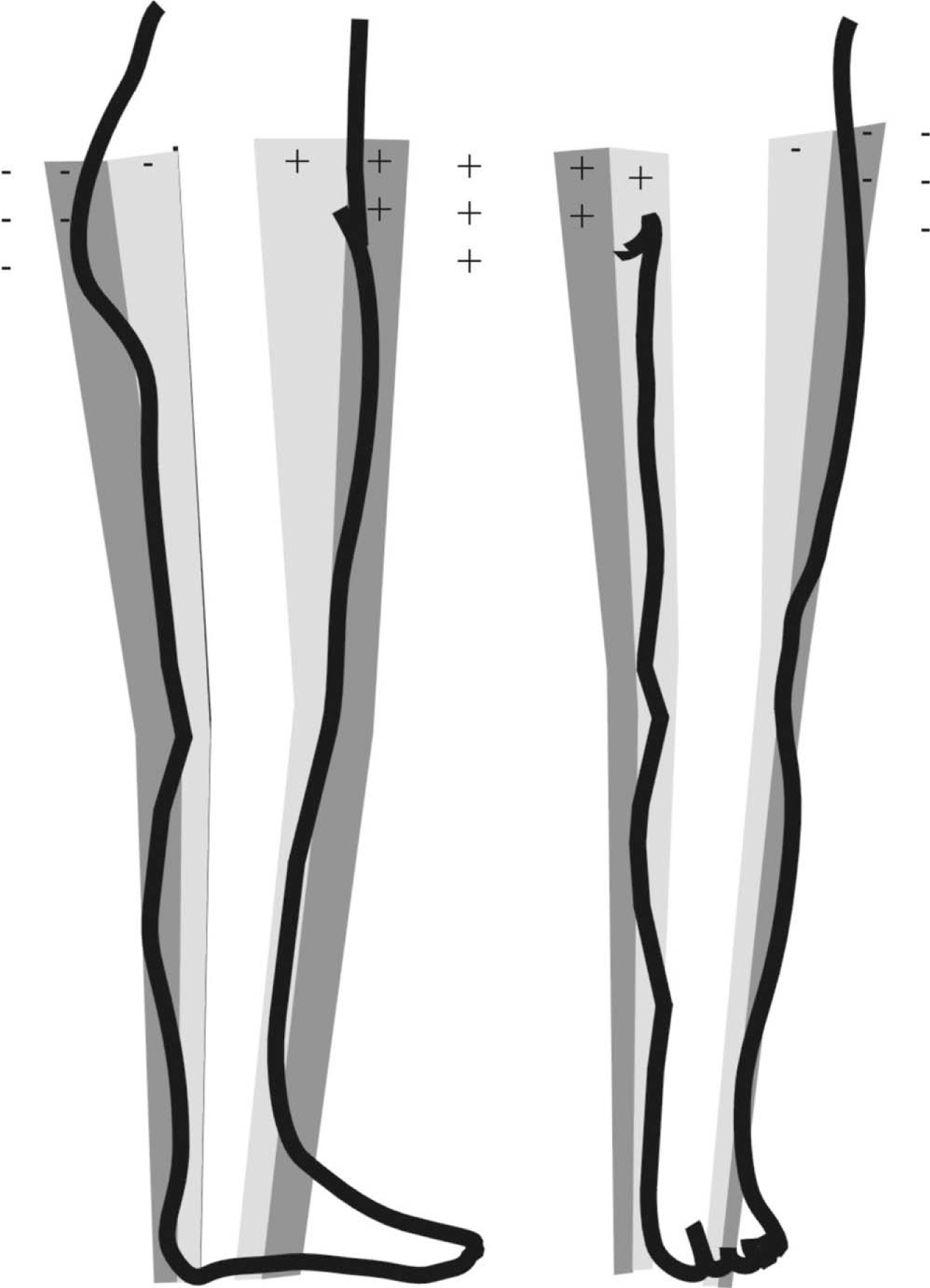
Ordinal score for the moment arms of the ground reaction force with respect to ankle, knee and hip joints in the sagittal and frontal plane. When the ground reaction force passes the joint in the white area inside the leg the moment arm is graded zero, in the light shaded area −1 (lateral or dorsal) or +1 (medial or ventral), in the dark shaded area 72 or +2 and outside the dark shaded area 73 or +3.
Results
Despite substantial changes in the alignment of the prosthesis, all subjects were able to walk without great difficulties. Remarkably, no statistically significant differences in walking speed were found between the conditions. All subjects completed all trials, but the alignment of some prostheses could not be changed in all directions. The alignment of the prosthesis of Subject 2 could not be changed to valgus and extension because it was already in the maximum position. The alignment of the prosthesis of Subject 5 could not be changed to dorsal and plantar flexion because of the characteristics of the foot. Between the initial and final reference trials, no significant differences were found. Therefore, these trials will be treated as one condition.
Temporal and spatial characteristics of gait
Results of the temporal and spatial characteristics of gait are shown in Table III. In general, the temporal and spatial characteristics remained constant, regardless of the alignment of the prosthesis. Only a small difference was found for the step duration between the intact condition and the condition in which the foot of the prostheses was aligned into dorsal flexion.
Magnitude and timing of the ground reaction force
The average GRF in the x, y and z directions for all conditions, normalized to stance duration, is shown in Figure 4. It can be seen that the ground reaction force was almost equal in all directions (Fx, Fy, or Fz) for all conditions, except for differences between the intact and prosthetic limb. This observation was confirmed by the results of the statistical test. For Fy and Fz, no statistically significant differences between the conditions were found, except for differences between the intact and prosthetic leg. However, some significant differences were found for Fx. These differences are shown in Figure 5 in more detail. In this figure, it can be seen that the shape of the curve is remarkably different for the different conditions. It can also be seen that the magnitude of medial force at the end of the stand phase is smaller when the prosthesis was aligned to varus (mean − 34.8N; SD 10.8N) and endorotation (mean − 31.4N; SD 13.5N) compared with valgus (mean − 54.7N; SD 20.1N) and exorotation (− 49.4N; SD 12.0N). The differences between endorotation on the one hand and exorotation and valgus on the other hand were statistically significant (P = 0.001).
Mean and standard deviation for the temporal and spatial characteristics of gait for all conditions.
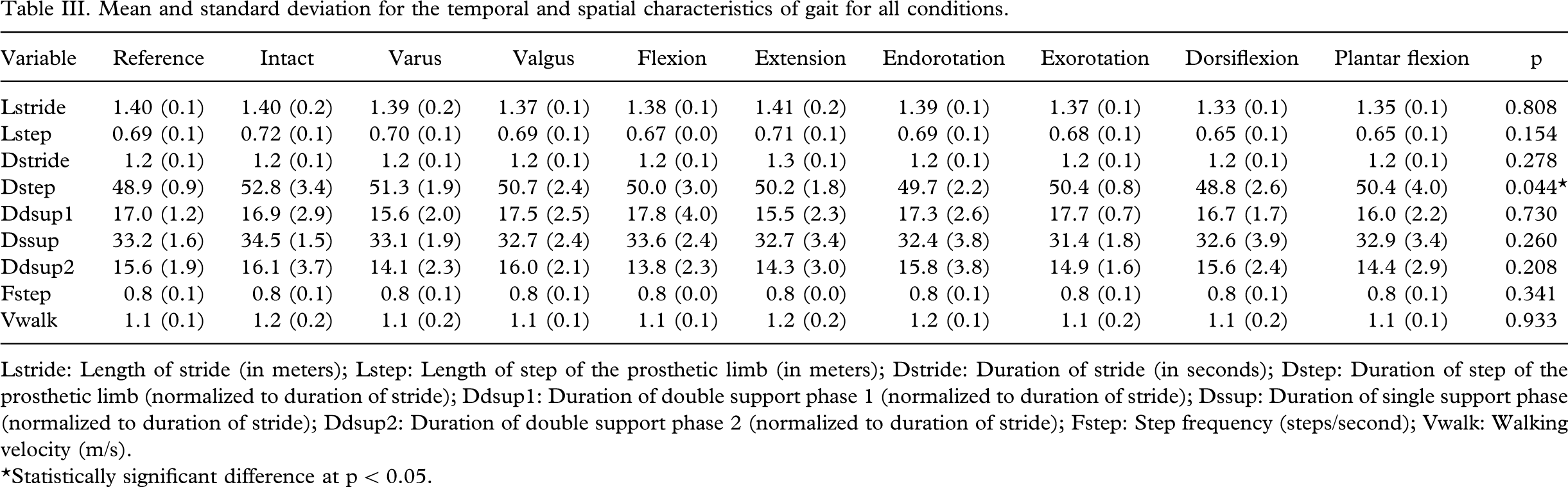
Lstride: Length of stride (in meters); Lstep: Length of step of the prosthetic limb (in meters); Dstride: Duration of stride (in seconds); Dstep: Duration of step of the prosthetic limb (normalized to duration of stride); Ddsupl: Duration of double support phase 1 (normalized to duration of stride); Dssup: Duration of single support phase (normalized to duration of stride); Ddsup2: Duration of double support phase 2 (normalized to duration of stride); Fstep: Step frequency (steps/second); Vwalk: Walking velocity (m/s).
Statistically significant difference at p < 0.05.
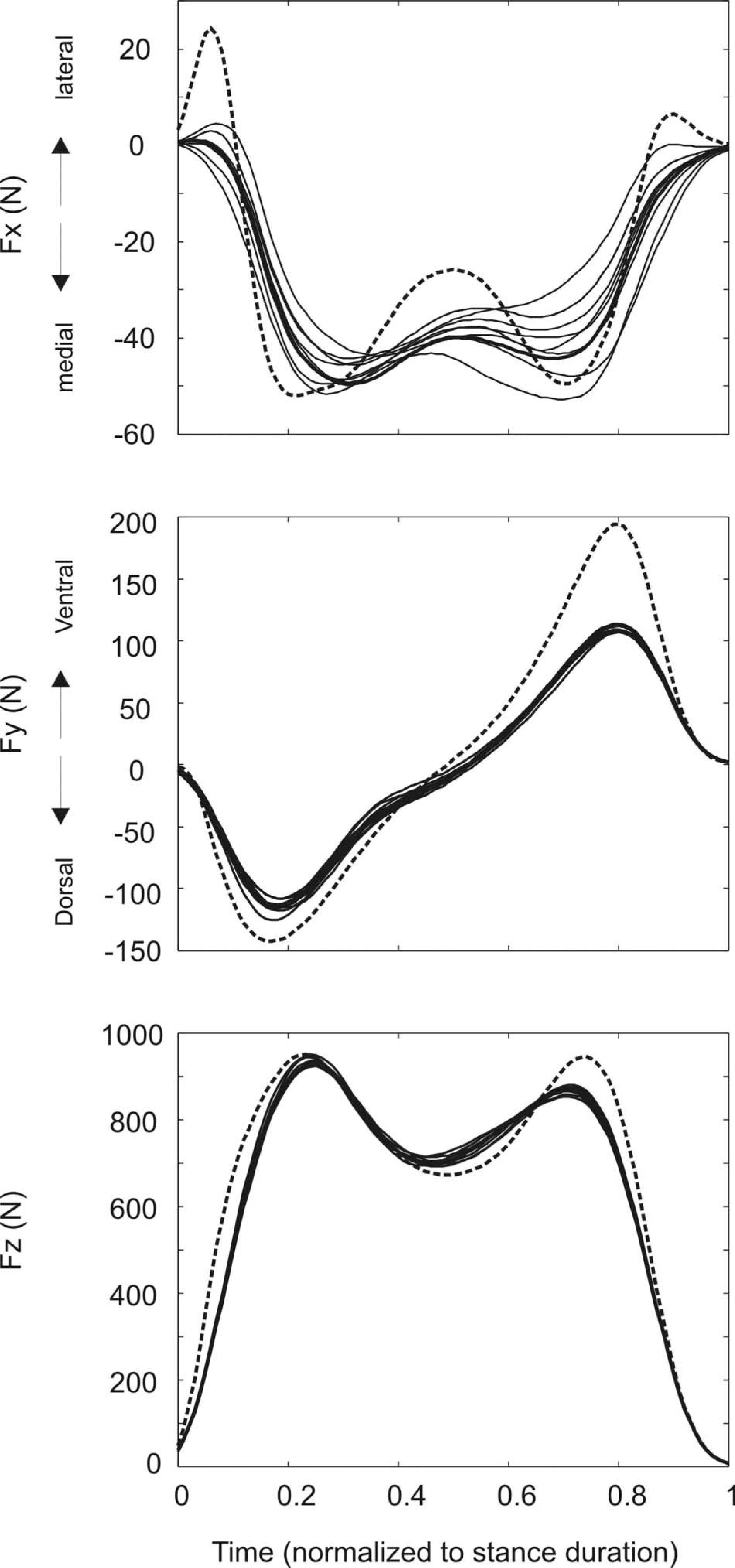
Average ground reaction force (Fx, Fy, Fz in N) for all conditions. The dashed line represents the ground reaction force for the intact leg, the thick solid line represents the reference alignment, the other alignments are represented by thin solid lines. Note that prosthetic alignment has little effect on the ground reaction force patterns and hence separate lines can be hardly distinguished, except for the Fx patterns which are shown in more detail in Figure 5.
External joint moments
As explained in the methods section, the external joint moments were scored by means of the moment arms of the GRF in the frontal and sagittal plane. In the sagittal plane, no significant differences were found. In the frontal plane, significant differences were found for the ankle during terminal stance (p = 0.006) and pre-swing (p = 0.001). During terminal stance, the vector of the GRF was directed more lateral to the ankle when the prosthesis was aligned into exorotation compared with all other walking conditions. Thus, in that condition, the external eversion moment was higher. During pre-swing, differences were found between endorotation (mean 0.6; SD 0.9) and exorotation (mean − 1.4; SD 0.5) and between varus (mean 0.4; SD 0.5) and exorotation. Again, in both cases, the vector of the GRF was directed more lateral to the ankle when the prosthesis was aligned into exorotation.
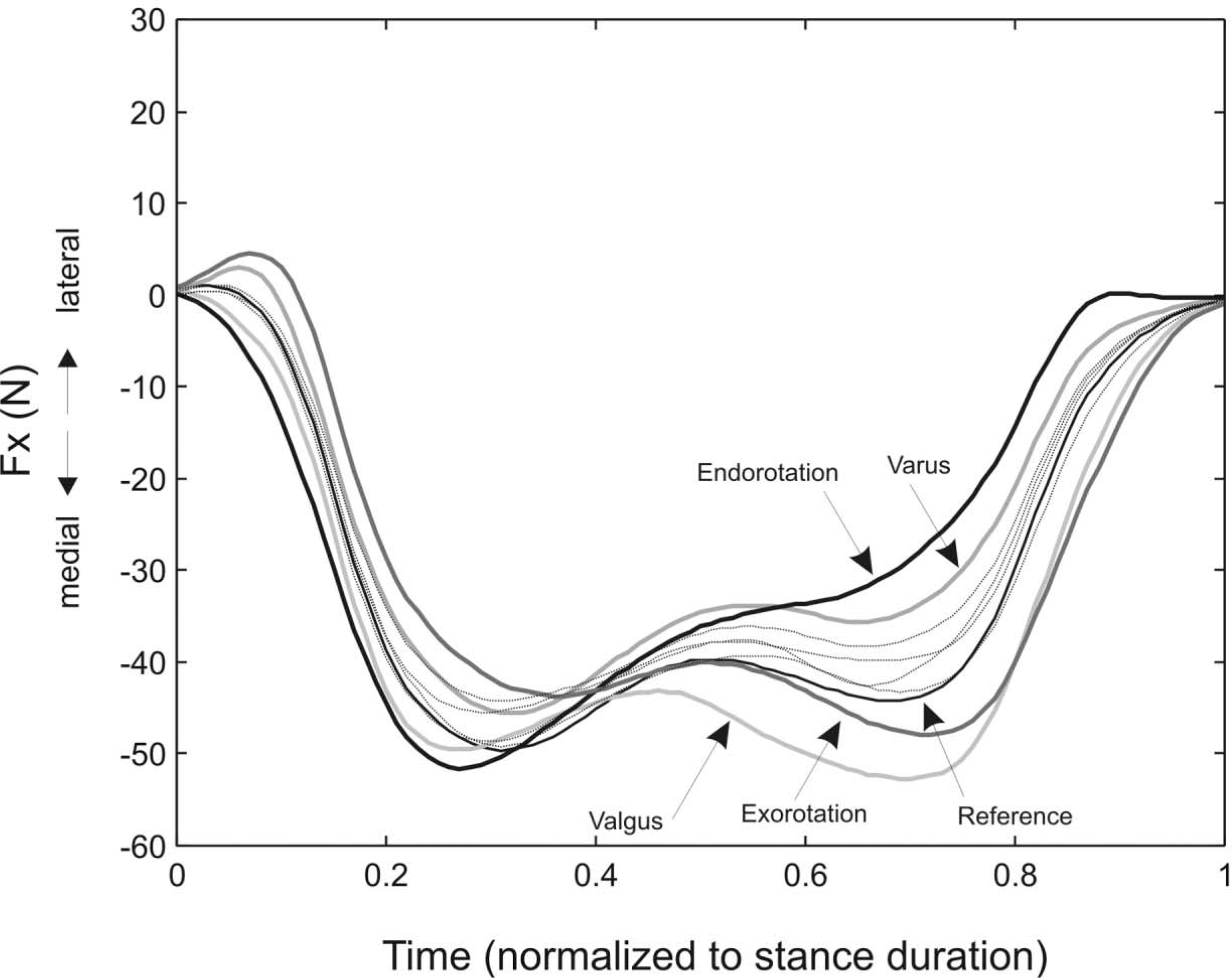
Average ground reaction force in mediolateral direction (Fx). The magnitude of the medial force at the end of the step is smaller with the prosthesis aligned into varus and endorotation compared to valgus and exorotation. The other conditions are displayed as thin solid lines in the background.
Discussion
In this study, the effect of the several systematic misalignments of trans-tibial prostheses was analysed using the SYBAR system. Despite the relatively large changes in prosthetic alignment, all subjects could walk well with the prosthesis. Remarkably, the walking velocity remained constant in all conditions. Consequently, the results of this study could not be influenced by changes in walking velocity. Subjects selected the same walking velocity, independent of the changes in alignment. This observation was supported by Fridman et al.'s (2003) study but contradicted by the results of Hannah et al.'s (1984) study. Possibly, these differences are caused by differences in the experimental population or design. In Hannah et al.'s (1984) study, five male subjects with trans-tibial amputation (minimum of 3 years post-operation) participated, one of whom had bilateral amputations and one of whom was blind; hence, this group could have experienced more problems with the misalignments. In the current study, also, no effects of alignment were found in the temporal and spatial characteristics of gait. This is according to the results of the study of Fridman et al. (2003) in which no significant differences in temporal and spatial characteristics were found between walking with the prosthesis in reference alignment and walking with the prosthetic foot externally rotated 188. In contrast, significant differences in step frequency were found again in Hannah et al.'s (1984) study when walking with a misaligned prosthesis.
The most remarkable result in the current study was the difference found for the mediolateral ground reaction force (Fx). When the prosthesis was aligned to endorotation, the magnitude of Fx at the end of the stand phase, was significantly smaller compared with valgus and exorotation. In Figure 5, it can be seen that the Fx of endorotation (and although not significant also varus) was at one side of the spectrum, and the Fx of valgus and exorotation was at the other side of the spectrum. This relationship between valgus and exorotation on the one hand and varus and endorotation on the other hand could be explained because in valgus and exorotation, the foot is positioned laterally, and in varus and endorotation, the foot is positioned medially. The pattern of Fx has not received much attention in the literature, which makes it difficult to interpret this effect. However, it might be hypothesized that when the ground reaction force is directed to the body's centre of mass during walking, a lateral foot placement requires a larger medial component in the ground reaction force (Inman et al. 1981) (Figure 6). Future studies have to be performed to investigate this effect.
Few significant differences for the external joint moments were found. Only in the frontal plane were significant differences found in the ankle during terminal stance and pre-swing. In both phases of the gait cycle, the GRF vector was directed more lateral to the ankle when the prosthesis was aligned into exorotation compared with the other conditions. This observation is connected to the differences in mediolateral ground reaction force patterns. When the foot is positioned laterally, the centre of pressure of the ground reaction force vector is also positioned more lateral to the ankle joint, and hence the moment arm increases (Figure 6). It needs to be stressed that the observed effect in the net joint moment around the ankle should not be interpreted as an increased external moment into valgus, since net joint moments were analysed in the absolute frontal plane of the subject and not in a local reference plane connected to the lower leg and foot. When the leg or foot rotates, both reference planes become unaligned, and hence the observed effect cannot be described as an increased moment into valgus.
In the current study, only a small number of structural effects of changes in the alignment as measured with the SYBAR system were found. The lack of effect in the spatio-temporal parameters was previously also observed by Fridman et al. (2003). Regarding the ground reaction force patterns, no other studies have been found in the literature. However, regarding the joint moments, clear effects have been observed (Blumentritt et al. 2001; Schmalz et al. 2002; Zahedi et al. 1987). It could be argued that the lack of results in the joint moments in the current study could be due to the low time and spatial resolution of the SYBAR system. In addition, the authors did not calculate true external joint moments, but estimated them on the basis of the magnitude and orientation of the moment arm of the GRF with respect to the joints with the help of a self-designed ordinal scale. However, Blumentritt et al. (2001) and Schmalz et al. (2002) observed differences in knee joint moments in the frontal and sagittal plane as much as 40 Nm after prosthetic misalignment similar to those performed in the current study. Given an unchanged amplitude of the ground reaction force, this could result in a change in moment arm of as much as 0.06 m. A difference of this magnitude should be large enough to be detected with the limited resolution of the SYBAR system and our ordinal scale. Hence, it remains the question whether the resolution of SYBAR and the used ordinal scale is too low to detect the occurring effects or whether no systematic effects occurred in the net joint moments around the hip and knee and ankle in the sagittal plane.
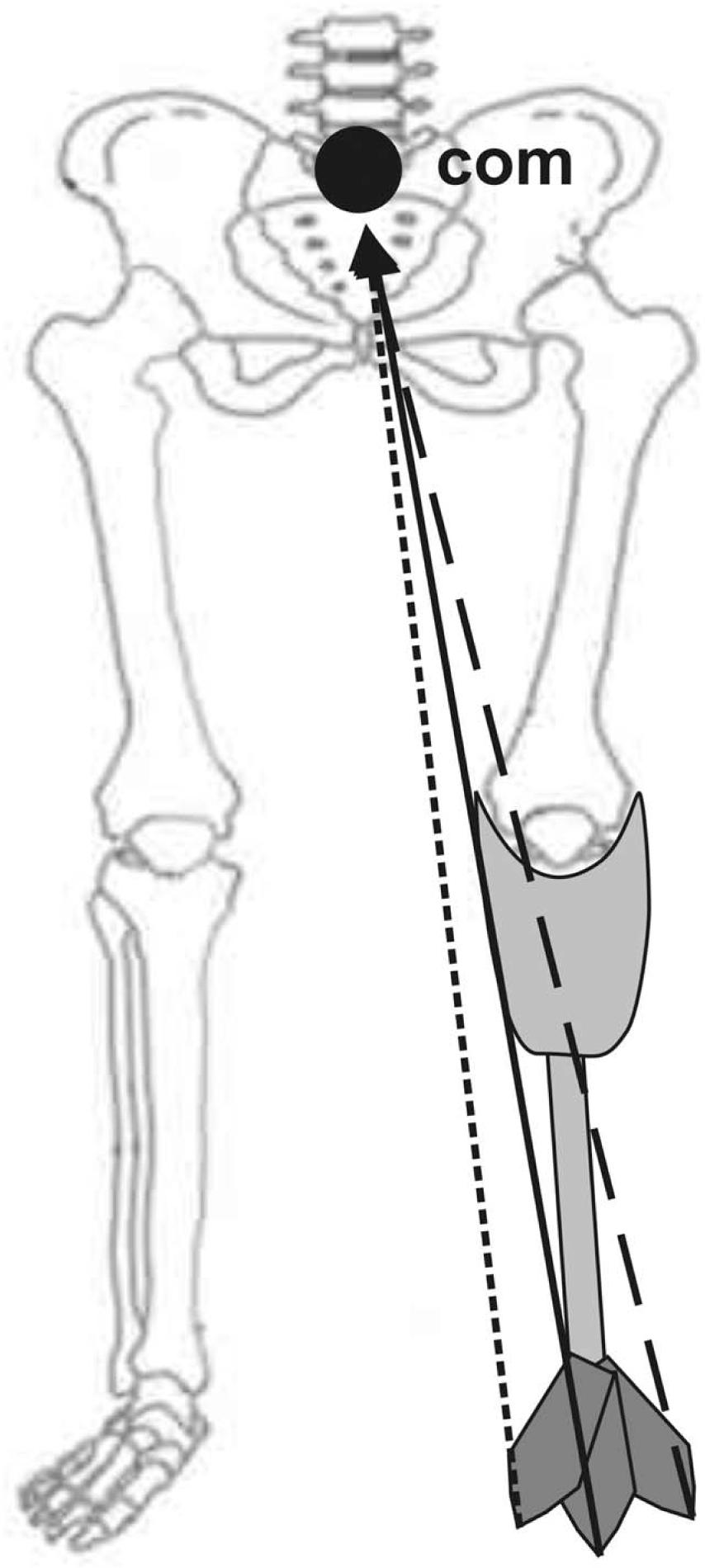
Schematic drawing of the orientation of the ground reaction force vector in the reference (solid), exorotation (dashed) and endorotation (dotted) condition in the frontal plane. When the foot is placed more laterally, through exorotation (or valgus) of the prosthesis, the medial component of the ground reaction force should increase in order to maintain the ground reaction force vector directed to the body's centre of mass (com) and keep the body in balance. For a medial foot placement, through endorotation (or varus), the opposite occurs. Consequently, the moment arm of the ground reaction force also changes around the ankle but not so much around knee or hip joint.
For the purpose of this study, however, it does not really matter whether this lack of results is due to a low resolution of the method or to the real absence of systematic effects. The purpose of this study was to investigate what systematic effects of prosthetic misalignment could be observed using the SYBAR system, and consequently whether and how this system could be used in the process of prosthetic alignment. Based on the results, only a few systematic effects could be observed using this method, and hence only a few possible guidelines for prosthetic alignment could be described for this group of patients. In the authors' opinion, however, this does not necessarily mean that the use of SYBAR for prosthetic alignment is limited. In this study, only subjects that were well trained in walking with a prosthesis participated. It is conceivable that these subjects developed subtle mechanisms of compensation over time that are difficult to trace. Perhaps in subjects who are less well trained, these subtle mechanisms of compensation are lacking. Therefore, the results could be different and more pronounced for subjects who are less well trained. In fact, these less well-trained subjects are the target group of the use of the SYBAR system during the alignment of prostheses. Furthermore, in this study, the kinematics or the EMG were not investigated. Both variables could provide more information on the effect of changes in alignment, and they should be explored in future research. Finally, the clinical use of gait analysis has more advantages than providing quantitative data. It allows for a systematic and off-line analysis of a large number of variables from a limited number of trials. This information can be analysed, stored and re-evaluated by a number of clinicians at any time. Hence, clinical use of gait analysis should not be discouraged in the future. In agreement with Rietman et al. (2002), the authors think instrumented gait analysis in a clinical setting is of interest but should be regarded critically.
Conclusion
The purpose was to investigate which systematic effects of prosthetic misalignment could be observed with the use of the SYBAR system. From this study, it becomes clear that structural effects of changes in the alignment of the prosthesis of five well-trained male lower-limb amputees were hardly found for the temporal and spatial characteristics of gait, the magnitude and timing of the GRF and the external joint moments using the SYBAR system. Systematic results were found only for the GRF in the mediolateral direction and joint moment around the ankle in the frontal plane. These seem to be parameters that could be used to identify misaligned prostheses. Because of the magnitude of the changes in the alignment and the results of earlier performed studies, more effects were expected. Therefore, the usability of the SYBAR system should be further explored for different groups of patients and for different parameters.
Acknowledgement
The authors gratefully acknowledge Cor Martijn of Livit Orthopaedics for his assistance in the alignment of the prostheses