
Abstract
Purpose:
Gait and posture disorder severely impedes the quality of life of affected patients with lumbar spinal canal stenosis (LSCS). Despite the major health concern, there is a paucity of literature about the relationships among spatiotemporal gait parameters and spinal sagittal parameters. This is a cross sectional study performed in a single tertiary referral center to determine the relationships among spatiotemporal gait parameters and spinal sagittal parameters in patients with LSCS.
Methods:
A total of 164 consecutive patients with LSCS, 87 men and 77 women with mean age of 70.7 years, were enrolled. Spatiotemporal gait parameters were studied using a gait analysis system. Spinal sagittal parameters were studied including sagittal vertical axis (SVA), thoracic kyphosis (TK), lumbar lordosis (LL), sacral slope (SS), pelvic inclination (PI), and pelvic tilt (PT) both in the neutral and stepped positions.
Results:
SVA was significantly larger in the stepped position than in the neutral position (neutral position, 72.5 mm; stepped position, 96.8 mm; p = 0.003). Parameters regarding the pelvis exhibited significant differences, which could represent pelvic anteversion in the stepped position. By stepwise multiple regression analysis, the prediction models, containing SVA (neutral) and PT (stepped) for double supporting phase, exhibited statistical significance, and accounted for approximately 50% of the variance.
Conclusions:
The present study provides statistically established evidence of correlation among spatiotemporal gait parameters and spinal sagittal parameters. Differences between sagittal parameters in neutral and stepped position may stand for the postural control during gait cycle, and increased SVA in neutral position and increased PT in stepped position may correlate with prolonged double supporting phase.
Introduction
Lumbar spinal canal stenosis (LSCS) is a commonly recognized condition with narrowing of the spinal, which often occurs in middle ages and due to degenerative changes. 1 Neurogenic intermittent claudication, which is usually getting worse during standing and walking, is one of the most common symptoms of LSCS, and may deteriorate the ability of walking. 2 Previous reports showed enhanced spinal epidural pressure which was revealed to be related to walking and standing posture from objective measurements using instrumented devices of micro-tip catheter. 3 In addition, postural control impairment in walking is considered as a major risk factor for falls in the elderly 4 ; therefore, early recognition and quantification of gait and posture impairment is important in elderly patients.
For the past few decades, there have been significant advances in the understanding of spinal alignment in light of the development of spinal deformity analysis. Particularly, spinal sagittal contour has been studied in various models that have demonstrated the correlations among spinal sagittal alignment and health-related quality of life scores according to patient-reported outcomes in the setting of spinal pathology. 4,5
For knowledge regarding health concerns of an aging population, gait and posture may be the key factors for predicting the impediment of health-related quality of life in the future, since there might be apparent relationship between walking posture and symptoms such as intermittent claudication. Gait and spinal parameters, however, have been analyzed separately. There is a paucity of evidence about the relationships among gait and spinal parameters. The aim of the present study was to examine the relationships among spatiotemporal gait parameters and spinal sagittal parameters in elderly patients with LSCS. Health-related quality of life score, the Oswestry Disability Index and clinical assessment using Japanese Orthopaedic Association score for low back pain were also examined.
Materials and methods
Basic patient data
This is a cross sectional study performed in a single tertiary institution. After obtaining institutional review board approval, a retrospective analysis of spatiotemporal gait parameters and radiographic profile was performed for preoperative patients with LSCS who were planed surgical treatment. In a retrospective analysis of 164 consecutive patients, 87 men and 77 women with mean age of 70.7 years were included in this study. The patients with scoliosis as determined by a Cobb angle >10°, patients with osteoarthritis of lower extremity, patients with cervical spondylotic myelopathy, and other patients with gait disorder such as neuro-mascular disease or motor neuron disease were excluded from analysis. The mean value of height and body weight were 158.4 ± 9.6 cm and 58.3 ± 10.1 kg, respectively. All patients were cauda equina type of LSCS, who showed intermittent claudication with the findings of redundant nerve on magnetic resonance imaging, and the patients who have abnormal value of ankle brachial pressure index were excluded. The mean value of the duration of symptom which was defined as the period from the onset of the symptom to the period we evaluated them was 12.5 months. All patients were the candidates for surgery where they evaluated before surgery and underwent surgery after that. LSCS was diagnosed by board-certified spine surgeon after experiment of X-ray, computed tomography, and magnetic resonance imaging.
Clinical assessment
All patients received gait analysis using a gait analysis system with sheet type foot pressure sensor to record the motion of the foot markers as the subject walked along the walkway (Walkway MW-1000, Anima Co., Tokyo, Japan) (Figure 1) and (1) step length, (2) step width, (3) foot angle, (4) gait cycle, (5) stance phase, (6) swing phase, (7) double supporting phase, and (8) gait speed were calculated (Figure 2). Lateral standing radiographs were obtained by using vertical film with a constant distance between the subject and the radiographic source with a radio-opaque calibration tool and standardized protocol with the patients standing in a neutral position and in a stepped position. We defined stepped position moving load to front leg as telophase of double supporting phase in gait. The following spinal parameters were assessed: (1) C7-S1 sagittal vertical axis (SVA), which was measured as the distance between the C7 plumb line and S1 supero-posterior corner, (2) thoracic kyphosis angle (TK), which was measured as the angulation of intersection between lines parallel to the T4 superior endplate and the T12 inferior endplate, (3) lumbar lordosis (LL), which was measured as the angulation of intersection between lines parallel to the superior endplate of T12 and the sacrum, (4) sacral slope (SS), which was measured as the angulation of intersection between lines parallel to the superior endplates of the sacrum and the horizontal plane, (5) pelvic tilt (PT), which was measured as the angulation of intersection between lines parallel to a line connecting the midpoint of the superior endplate of the sacrum to the center of the hip axis and the vertical plane, and (6) pelvic incidence (PI), which was measured as the angulation of intersection between lines parallel to a line connecting the midpoint of the superior endplate of the sacrum to the center of the hip axis and a perpendicular line to the superior endplate of the sacrum. 6 –8 The accuracy of the methods, including intra-rater and inter-rater agreements were analyzed in detail in a previous paper. 8 Clinical assessment and health-related quality of life score were evaluated using the Japanese Orthopaedic Association score of low back pain (JOA score) and Oswestry Disability Index score (ODI score). Clinical disability was estimated as 14.8 ± 3.4 by JOA score, and 47.2 ± 12.8 by ODI score.

Gait analysis system with sheet type foot pressure sensor on the walkway.

Representative of gait parameters: (1) step length, (2) step width, and (3) gait angle.
Statistical analysis
Statistical analyses were performed using commercially available software (JMP version 11.0, SAS Institute, Inc. Cary, North Carolina, USA). Descriptive statistics including mean values and standard deviations were calculated for each parameter. After determining that the data followed a parametric distribution using the Shapiro-Wilk normality test (where p > 0.05 suggests that the data are from a normal distribution), Pearson product-moment correlation coefficients were calculated for all combinations of spatiotemporal gait parameters and radiographic measurements. The level of significance was set at p < 0.05. Multiple regression analysis was then used to determine spinal sagittal parameters which were most closely related to spatiotemporal gait parameters.
Results
Spatiotemporal gait parameters
Mean values and standard deviations of spatiotemporal parameters were estimated as follows: step length, 46.2 ± 10.1 cm; step width, 9.6 ± 3.7 cm; foot angle, 14.0 ± 6.9°; gait cycle, 1.2 ± 0.2 s; stance phase, 0.8 ± 0.01 s; swing phase, 0.4 ± 0.01 s; double supporting phase, 0.2 ± 0.04 s; gait speed, 76.9 ± 25.4 cm/s. Correlations among spatiotemporal gait parameters and health-related quality of life score are summarized in Table 1. Double supporting phase and ODI score exhibited significant positive correlation (r = 0.45, p < 0.01).
Correlations among spatiotemporal gait parameters and health-related quality of life scores.

JOA: Japanese Orthopaedic Association; ODI: Oswestry Disability Index.
* Significant correlation at p < 0.05.
Radiographic measurements
Radiographic measures in the two position are summarized in Table 2. SVA represented a positive imbalance of the sagittal plane, where SVA exhibited >50 mm. SVA was significantly larger in the stepped position than in the neutral position (neutral position, 72.5 mm; stepped position, 96.8 mm; p < 0.01). TK, LL, and PI were not statistically different between the two postures. In contrast to these parameters, parameters regarding the pelvis exhibited significant differences, which could represent pelvic anteversion in the stepped position. To determine the reliability of the pertaining method used to measure SVA in stepped position, calculation of intra-class correlation coefficients (ICC) and evaluation of 95% confidence interval (CI) according to the procedure as described by Bland and Altman was performed. 9 The agreement resulted in an ICC of 0.95 (95% CI 0.89–0.98; p < 0.001) as inter-rater reliability and an ICC of 0.87 (95% CI 0.74–0.94; p < 0.001) as intra-rater reliability, of good consensus.
Mean (SD) values of spinal sagittal parameters in neutral and stepped positions.

C7-S1 SVA: C7-S1 sagittal vertical axis; TK: thoracic kyphosis angle; LL: lumbar lordosis angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Correlations among sagittal parameters and health-related quality of life scores are summarized in Table 3. SVA and LL were significantly correlated with ODI score (ODI vs. SVA neutral: r = 0.43, p < 0.01; ODI vs. SVA stepped: r = 0.46, p < 0.01; ODI vs. LL neutral: r = −0.40, p < 0.01), and pelvic parameters in the stepped position were significantly correlated with JOA score (JOA vs. SS stepped: r = −0.42, p < 0.01; JOA vs. PT stepped: r = 0.43, p < 0.01).
Correlations among spinal sagittal parameters and health-related quality of life scores.

JOA: Japanese Orthopaedic Association; ODI: Oswestry Disability Index; C7-S1 SVA: C7-S1 sagittal vertical axis; TK: thoracic kyphosis angle; LL: lumbar lordosis angle; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
* Significant correlation at p < 0.05.
Statistical analysis
Among spatiotemporal gait parameters, double supporting phase, which exhibited significant correlations with ODI, were performed further statistical analysis using stepwise multiple regression model to determine the relationship with radiographic measurements. Correlations among spatiotemporal parameters and radiographic measurements are summarized in Table 4. Combinations of step width and PT stepped, foot angle and PT stepped, gait cycle and SVA neutral, and double support phase and SVA neutral were statistically significant.
Correlations among spatiotemporal gait parameters and spinal sagittal parameters.
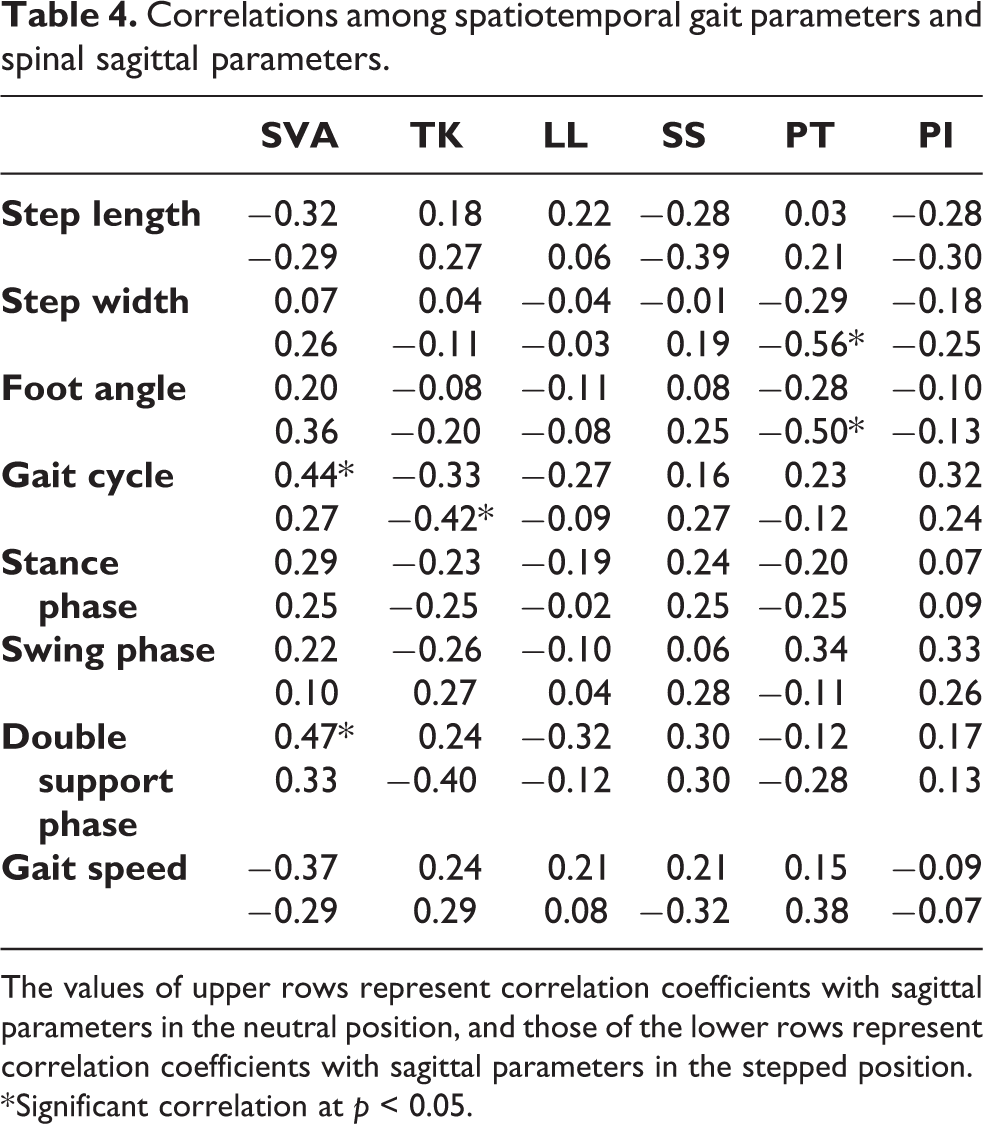
The values of upper rows represent correlation coefficients with sagittal parameters in the neutral position, and those of the lower rows represent correlation coefficients with sagittal parameters in the stepped position.
* Significant correlation at p < 0.05.
All radiographic measures, which exhibited significant correlations with clinical disability or double supporting phase, were used in a stepwise multiple regression analysis to predict double supporting phase. The prediction model for double support phase contained two predictors of SVA neutral and PT stepped, and accounted for approximately 50% of the variance (R 2 = 0.49, adjusted R 2 = 0.45, p < 0.001) as follows: y = 0.07 + 0.01 SVA (neutral) + 0.01 PT (stepped).
Discussion
We observed significant correlations among clinical disability with spatiotemporal gait parameters (ODI vs. double supporting phase: r = 0.45, p < 0.01) and with spinal sagittal parameters (JOA vs. SS stepped: r = −0.42, p < 0.01; JOA vs. PT stepped: r = 0.43, p < 0.01; ODI vs. SVA neutral: r = 0.43, p < 0.01; ODI vs. SVA stepped: r = 0.46, p < 0.01; ODI vs. LL neutral: r = −0.40, p < 0.01) in the current study. Stepwise multiple regression analysis indicated sagittal spinal parameters in the neutral and stepped postures as the predictors of the spatiotemporal gait parameter. To the best of our knowledge, analysis of morphologic parameters and gait parameters using the stepwise method in LSCS has not been reported before. The results provide guidance as to which radiographic analysis not only in the neutral position but also in a forced position like stepping might be important in assessing the clinical outcomes of LSCS. These findings might also shed some light on the spinal sagittal alignment in neutral and forced postures in evaluating and planning for treatment intervention for patients with LSCS: enlarged SVA in the neutral position and retroverted PT in the stepped position should be corrected to establish better gait cycle.
In light of the results in this research, spatiotemporal gait parameters such as gait speed and cadence estimated from the gait cycle are almost equal in value to that in a previous report, 10 and relatively low in value compared with healthy elderly subjects. 11 From the viewpoint of correlations with quality of life scores, only double supporting phase and ODI score exhibited significant positive correlation (r = 0.45, p < 0.01) among spatiotemporal gait parameters. Referential correlations among gait parameters and ODI score seem more apparent in previous results. 12 The previous paper reported that ODI was strongly correlated with step length and gait velocity in LSCS. 12 These differences could possibly arise from disparities in the patient profiles, whereas our LSCS cohort were all preoperative patients who were planed surgical treatment and was estimated to have relatively severe ODI score compared to the referential value. Moreover, evaluation methods for spatiotemporal gait parameters are varied among papers. 13 –15 There is usually a trade-off relationship between the accuracy of a gait measurement and pertinence to clinical use. For instance, three-dimensional motion analysis systems provide precise and valuable information, but are sometimes costly, technical difficult to use, and labor intensive, and therefore not ready for application to clinical settings. 13 For such limitations, the recently introduced walkway systems, used in this study, have been designed to measure spatiotemporal gait parameters with accuracy comparable to sophisticated motion analysis systems, but are carried out in an automated fashion.
Increasing interest in sagittal plane analysis has led to a better understanding of the importance of spinal sagittal alignment. 4,5 General understanding about gait and posture in patients with cauda equine type of LSCS may be known as setting their posture flexed which relief their symptom and increase step length and hip extension angle. 16 However, multiple studies have demonstrated that trunk flexion with sagittal imbalance is the strongest driver of pain and disability. 17,18 Our results, which show significant correlations among sagittal parameters and health-related quality of life scores, are supported by these reports. Similarly, sagittal balance, which could affect the center of mass of the trunk, is believed to play a crucial role in the control of gait and posture. 19 However, only a few studies have documented the relationships among spinopelvic parameters and the spatiotemporal gait parameters. Arima et al. reported the relationship between gait disorder and spinal imbalance in an adult spinal deformity cohort similar to our results in patients with LSCS. 20 In this study, JOA score, which contains grading about activities of daily living including walking ability, exhibited correlation with PT, which is considered related to walking ability as well as pelvic conversion. 21 Multiple studies have also demonstrated that sagittal imbalance is the strongest driver of pain and disability. Our results, which show significant correlations among sagittal parameters and clinical disability, are supported by these reports.
In this study, sagittal parameters were tested in neutral and forced position, which we believed to reflect the postural control in gait cycle. Difference of SVA seems to represent the postural control of center of mass of trunk, and differences of SS and PT may typify the control of pelvic conversion. The prediction models, containing SVA in neutral position and PT in stepped position for double supporting phase, which was considered related to the clinical disability as well as gait ability for the results of correlation with ODI score, exhibited statistical significance, and accounted for approximately 50% of the variance. In brief, double supporting phase may tend to be prolonged in the case which has greater SVA in neutral position and retroverted PT in stepped position, which is ordinarily anteverted in stepped posture: these parameters exhibited the significant correlation with the clinical disability. For this result, gait parameters representing gait ability could be affected by spinal contour in neutral and forced position to some degree, which seems simple explanation to the gait improvement after corrective surgery for spinal deformity. 21,22 Moreover, spinal surgery has been reported to reposition the pelvic retroversion compensated for the preoperative malalignment into anteversion, 22 which may be circuitous explanation to the gait improvement by surgical intervention. It also seems interesting that stepped PT was significant associated with JOA scores but not with the ODI scores in the univariate analysis. Stepped PT has positive correlation with JOA score that might be translated the patients who could deeply tilt pelvic backward marked better JOA score. Tilting pelvis adequately at each phase of gait cycle may be essential in achieving better ADL function. This issue remains unsolved because the relationship among ODI, gait cycle, and sagittal parameters was in focus in this research where relationship between JOA score and gait cycle was not significant. However, stepped PT was selected as two most significant predictors of double supporting phase with neutral SVA. Pelvic conversion is considered as compensatory mechanism for the thoracolumbar kyphosis. 10 In this concept, most of the cases should exhibit the increased PT, standing for the pelvic retroversion, and PT may exhibit the strong correlation with double supporting phase by the same token of SVA. However, in fact, there is another type of malalignment of PT. In the case of segmental instability due to spondylolisthesis, pelvic compensation for thoracolumbar kyphosis may be impaired, and PT may be wrongly normalized. 23 These discrepancies have been reported by several study. 24 That normal PT is considered as a confounding factor which make the relationship between PT and double supporting phase obscure. These contradictions around dynamic and static analysis make us forecast several confounding factors and this issue may be some key to increase our pathological understanding and functional regaining after treatment.
One strength of the current study is the inclusion of a conspecific population of consecutive patients with LSCS. Limitations to this study must also be acknowledged. First, the sample is small and has some skewed characteristics arising from inclusion and exclusion criteria. Further studies are needed from a larger sample size of patients, including the heterogeneous population. Second, since dynamics of lower extremities is an important mechanism to maintain balance during walking, 3 the lack of parameters regarding the lower extremities due to study design might be a limitation of this study. Probably these mechanisms were expressed in our results as having a robust effect on the stride-related parameters. Future study requires full length analysis including lower extremities. Third, postoperative performance of the gait analysis was not evaluated. It may be an important issue whether the surgery improve the gait performance of the patients with PSCS, or not. Despite these limitations, we could consider this study to have some importance toward understanding the biomechanics of LSCS.
Conclusion
The present study provides statistically established evidence of correlation among spatiotemporal gait parameters and spinal sagittal parameters. Differences between sagittal parameters in neutral and stepped position may stand for the postural control during gait cycle, and increased SVA in neutral position and increased PT in stepped position may correlate with prolonged double supporting phase.
Footnotes
Acknowledgment
The authors are indebted to the medical editors from the Department of International Medical Communications of Tokyo Medical University for editing and reviewing the initial English manuscript.
Author contributions
Kazuma Murata is responsible for the manuscript preparation. Kenji Endo, Takato Aihara, Hidekazu Suzuki, Yuji Matsuoka, Hirosuke Nishimura, Taichiro Takamatsu, and Kengo Yamamoto participated in the review of manuscript and data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Review Committee statement
This study was approved by the Ethics Review Committee of Tokyo Medical University Hospital. Informed consent was obtained by an opt-out manner.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.