
Abstract
A sand-casting technique for trans-tibial sockets was applied to 28 amputees, and the prosthetic fit observed through transparent check sockets. The results were better than historical reports of fittings with plaster of Paris casting by qualified prosthetists. The fit was consistently and evenly larger than the stump, but total contact could be achieved by applying three (two to five) stump socks. This would normally be considered on the high side of a good fit.
Introduction
Sand-casting technology was tested because it represents a possible improvement in consistency of prosthetic fit of trans-tibial (TT) amputation stumps and reduces the influence of technical skill in relation to plaster of Paris casting. Historical data from series of TT amputees fitted by the teachers and their associates at the schools educating orthopaedic technologists (ISPO Category-II) have shown good fits in only 20 – 53% of prostheses provided (Jensen et al. 2005; Jensen and Heim 2000; Jensen and Raab 2002). For visualization of the prosthetic fit, transparent sockets were applied (Reger et al. 1976).
Patients and methods
Thirty-five younger amputees were selected from amputees with well-known user records. Additionally, there were three primary fittings. In July 2003, prostheses with polypropylene draped sockets were manufactured for this group utilizing a supracondylar suspension brim (IPOS). Sand-casting according to the Center for International Rehabilitation (CIR), Chicago, USA was applied (Wu et al. 2003) First, the stump was dressed with two terry compression socks, and relief added over pressure sensitive areas (Figure 1a). A nylon sock was applied, and over that a thin plastic bag. A supracondylar brim (IPOS) was added (Figure 1b) and kept in place with tape (Figure 1c). The stump was inserted into a container with fluidized silica sand and a vacuum applied (Figure 2a). A thin plastic bag was pulled over the container to seal it, and the stump removed from within the thin plastic bag, leaving the brim as part of the walls of the negative cast (Figure 2b).
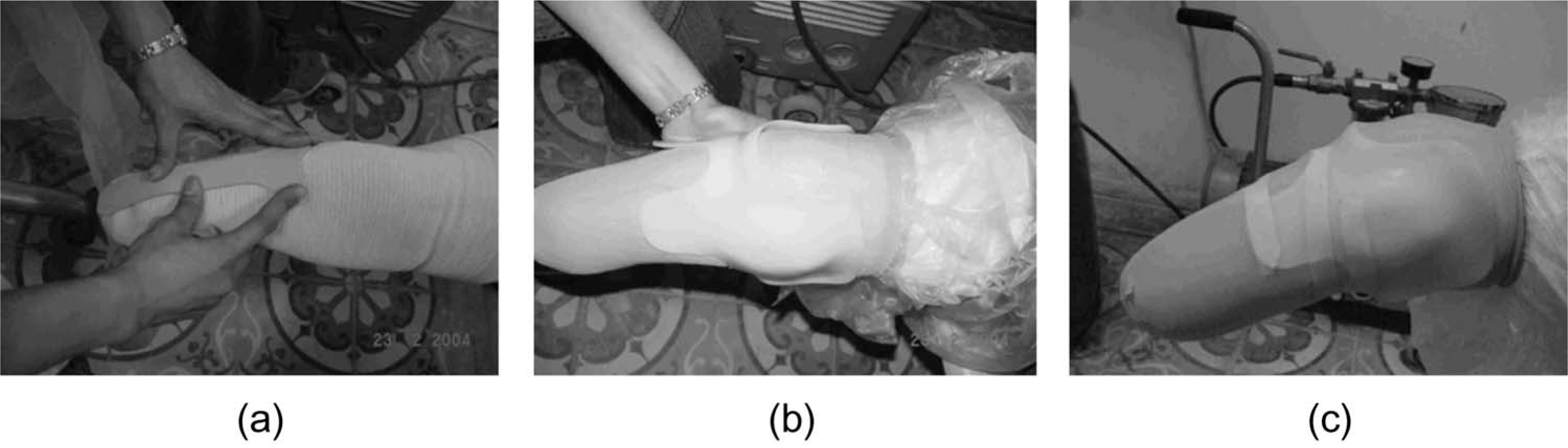
(a) Stump dressed with socks with reliefs added over pressure sensitive areas. (b) Nylon sock and thin plastic bag applied; supracondylar brim added. (c) Supracondylar brim kept in place with tape.
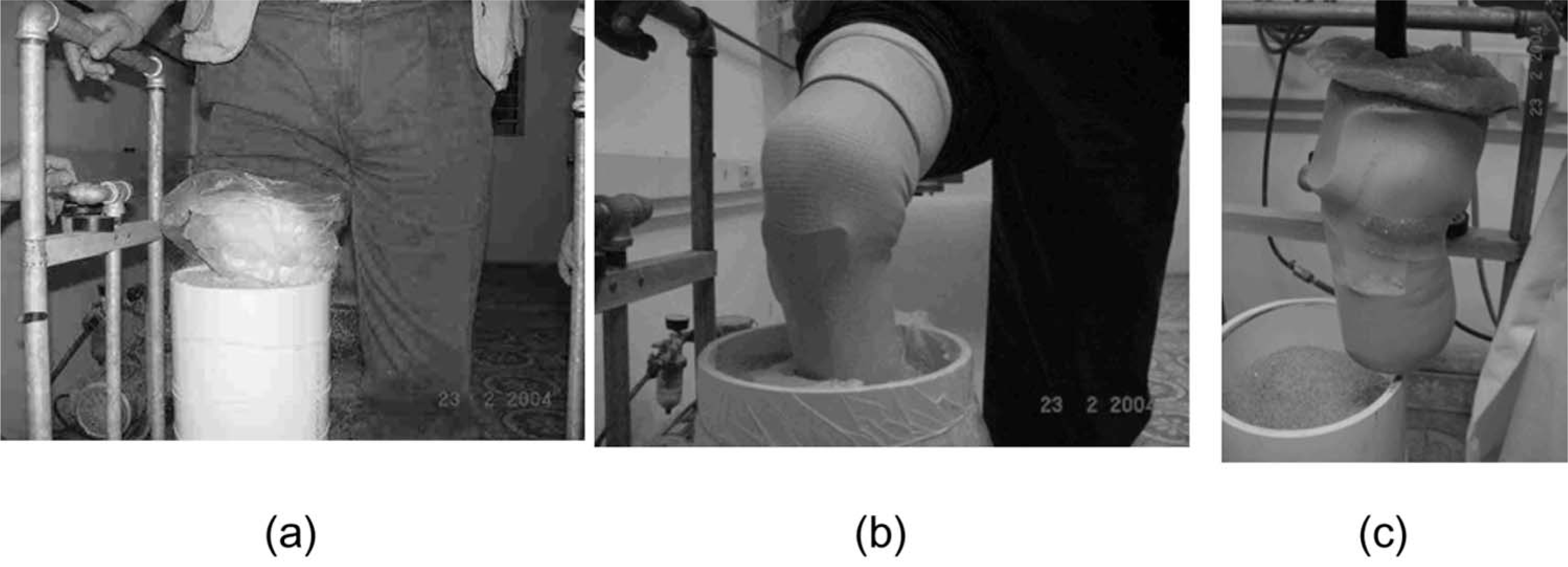
(a) Stump inserted into container with fluidized silica sand and vacuum applied. (b) Thin plastic back pulled over container to seal it and stump removed from within the bag leaving the brim as part of the walls of the negative cast. (c) Vacuum released and positive model with adhered brim removed.
A suction mandrel was placed in the negative mould, which was filled up with silica sand, sealed with the plastic bag, and a vacuum applied. The vacuum was released from the main container and the positive model with the adhered brim removed (Figure 2c). The brim and nylon sock were removed and the positive model rectified by gentle pounding (Figure 3). The positive model was vacuum-draped with a thermoplastic polypropylene sheet after having added a small plastozote disc to the end of the stump to prevent grounding in the socket. A modular/tubular endoskeletal system was provided, together with a polyurethane foam SACH foot. The patients were told to come back for control and follow-up at regular intervals. This obligation was fulfilled by 80% (28/35) on two occasions, after 7 and 11 months.

Brim and nylon sock removed and positive model rectified by gentle pounding.
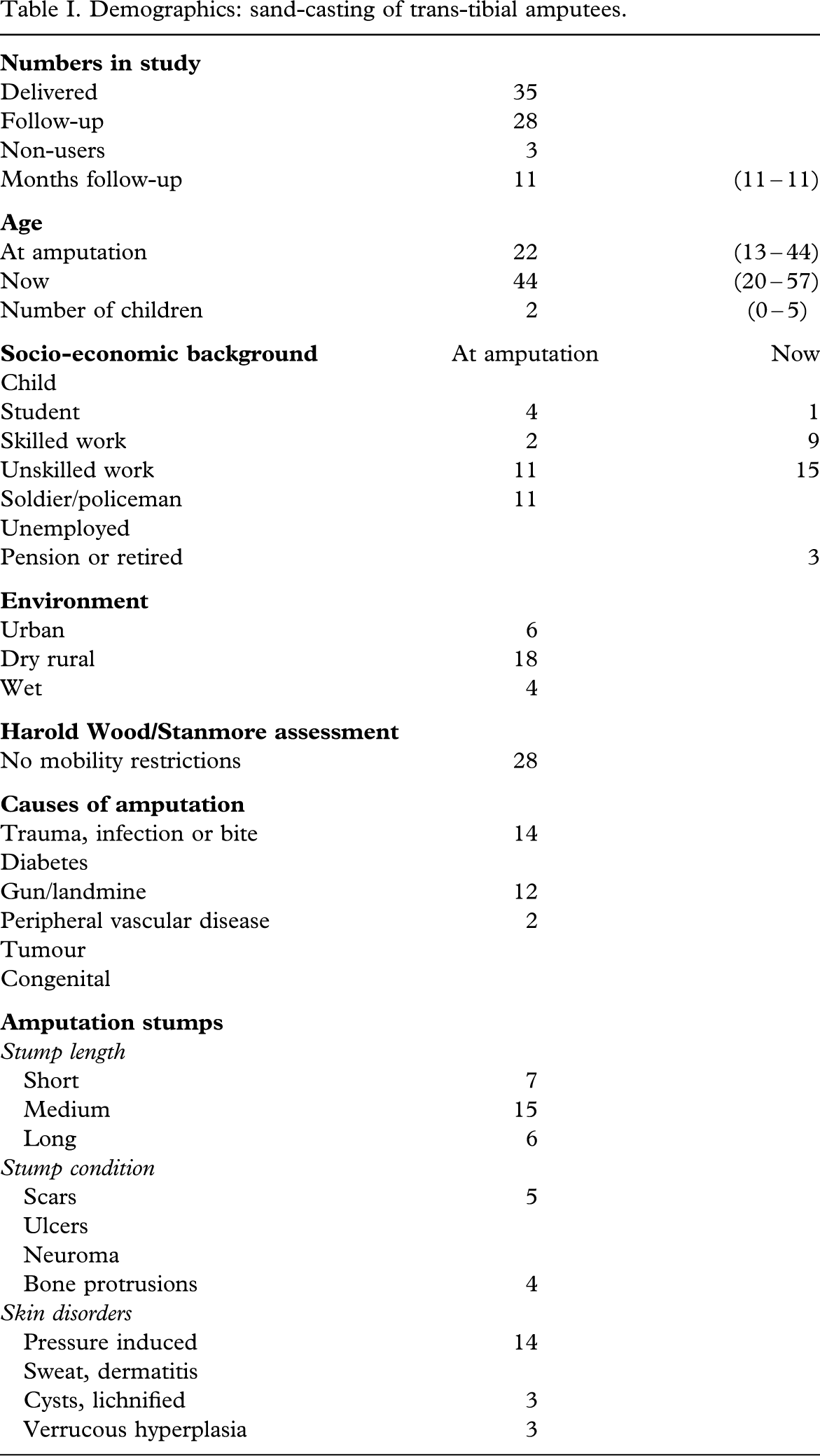
The demographics of this series (Table I) are equivalent to other patient series used for testing of prosthetic technology in the South East Asia region, which means amputees mainly as a result of trauma, living in families with a couple of children and mostly working. They have no restrictions in mobility, being community ambulators (Davies and Datta 2003). The amputation stumps were in generally good conditions for fitting, with only minor scar formations or bone protrusions and few skin disorders.
Demographics: Sand-casting of trans-tibial amputees.
At the follow-up, the amputees were interviewed by a team consisting of the prosthetist providing the prosthesis and acting as an interpreter to a Danish orthopaedic surgeon and a Dutch prosthetist. The stump was examined as well as the prosthesis. Further, a transparent socket was made by the sand-casting technique (trial socket) at the first follow-up in January 2004 together with a transparent socket by plastic draping on a positive plaster of Paris cast of the prosthetic socket provided at first (check socket).
At both follow-up visits, socket mapping was performed after dressing the amputation stump with two (one to four) compression socks, a thin plastic bag, and nylon socks. The check socket and the trial socket, respectively, were sequentially mounted in a casting jig, and a sufficient amount of methylene blue solution filled into the socket, after which the amputee introduced the stump into the socket applying full weight bearing. The methylene blue fluid filtered up along the stump until it was stopped by the total contact between socket and stump. This borderline was drawn up on the transparent socket with a blue or red filter pen, respectively, on the two occasions. The illustration (Figure 4) shows a typical pattern with the blue and the red line overlapping each other.

Normal design with overlapping weight-bearing areas (check socket right, trial socket left).
The weight-bearing areas of the socket were assessed by the orthopaedic surgeon comparing longitudinally between the two mappings and between the check socket and the trial socket. Total contact was encountered in all cases, meaning that the weight-bearing areas could be graded as expected, larger, or smaller.
For statistical analyses, Student's t-test (unpaired, two-tailed, two-sample, unequal variance) was applied.
Results
Patient compliance
The patient compliance (Table II) was high, with 89% (25/28) being users of the prosthesis under investigation; 82% (23/28) describing themselves as intensive users. The median time of wear was 15 (3 – 18) h/day, and 79% (22/28) could walk for more than 1 km, wearing shoes or sandals.
Patient compliance and prosthetic fitting with sand-cast sockets.
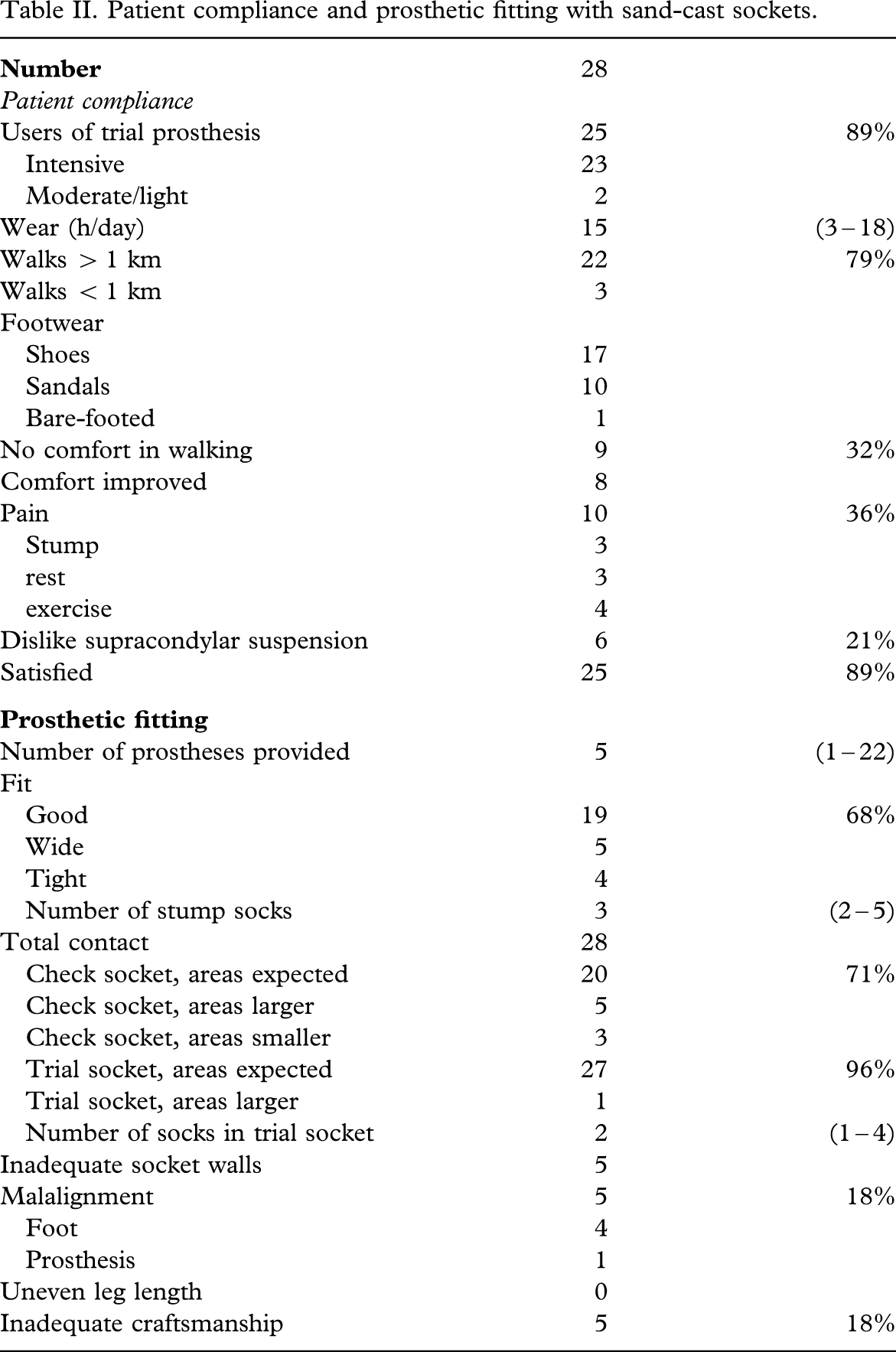
No comfort in walking was recorded in 32% (9/28) of patients, and pain was recorded in 36% (10/28). Although 21% (6/28) disliked the supracondylar suspension, 89% (25/28) declared satisfaction with the prosthesis. In this respect, it should be borne in mind that five (one to 22) prostheses had been provided previously, only three being first-time users.
System-related failures
System-related failures (Table III) were encountered in 21% (6/28). This was not different to two series with plaster of Paris casting (Jensen and Heim 2000; Jensen and Raab 2002), but significantly better (P < 0.000002) than that reported with HDPE-Jaipur technology (Jensen et al. 2004).
System related failures with trans-tibial sockets.
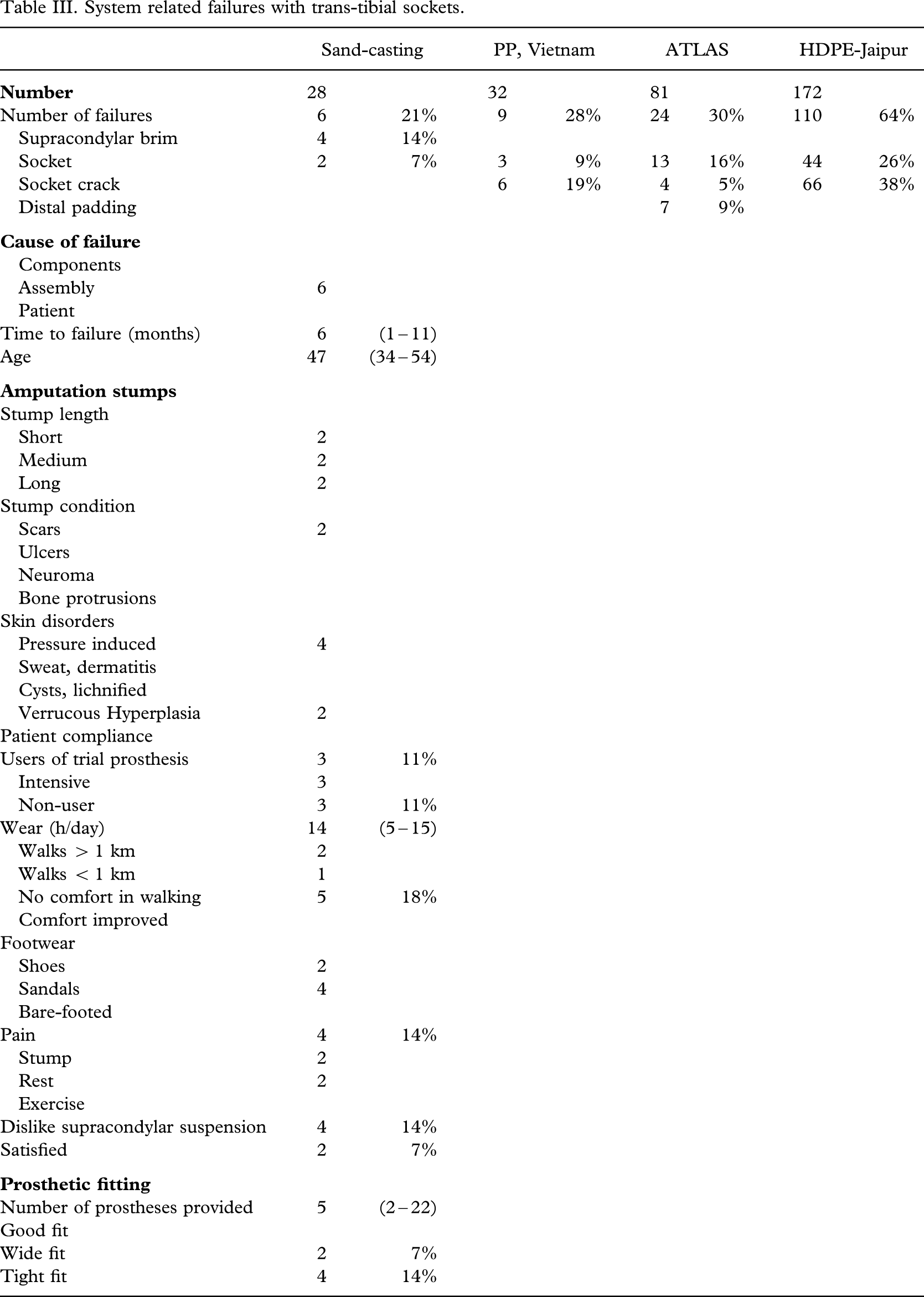
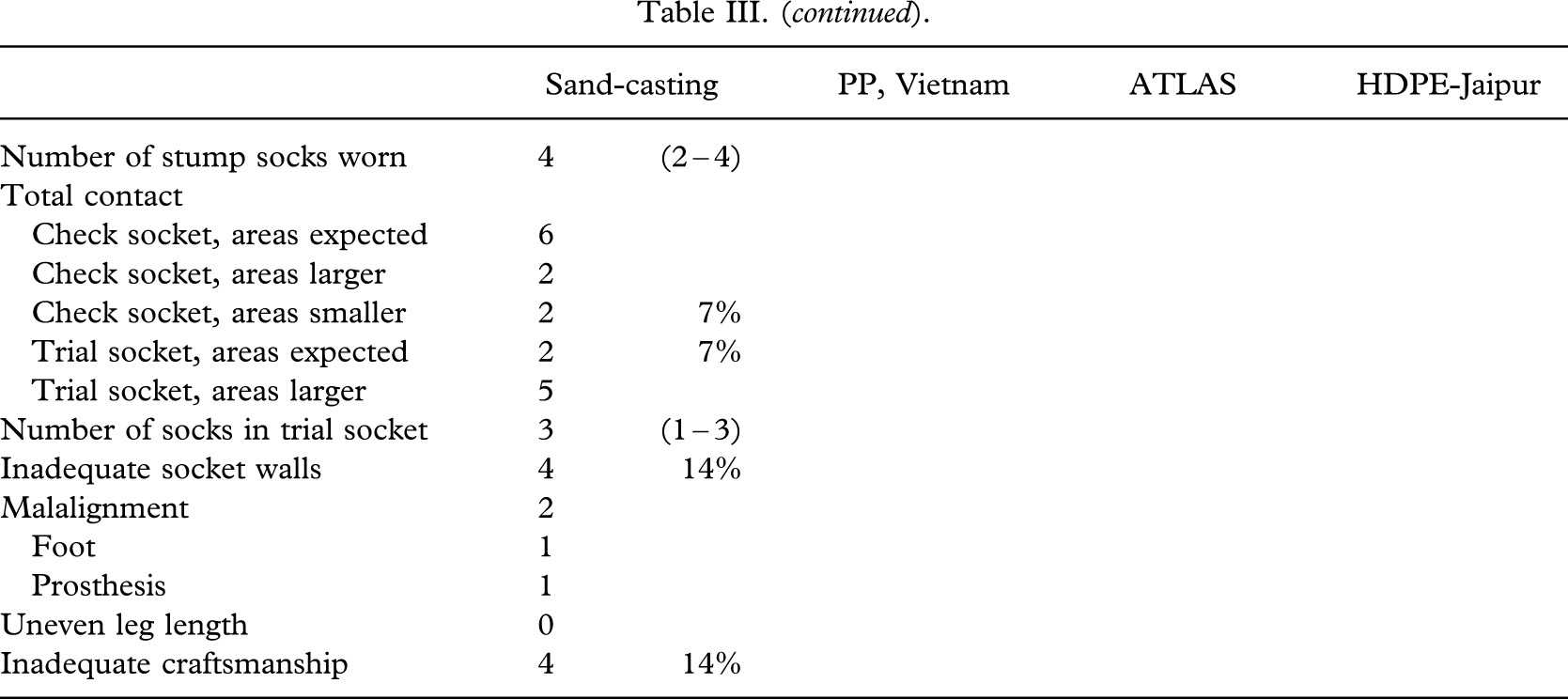
In four cases (14%), the supracondylar suspension was the cause of failure, as they all had pain and discomfort in walking, and three were non-users. An overly tight fit, inadequacy of socket walls, and insufficient craftsmanship were found in all these cases.
Total failure of the sand-casting technique was encountered in two cases (7%), where the socket was far too wide, requiring four socks for use. However, both individuals used the prosthesis for the whole day and could walk more than 1 km. The socket mapping showed in both cases the usual pattern with contact between socket and stump apart from the very distal end. Nevertheless, the second mapping showed larger contact areas, indicating sinking. There were no differences to be seen between check socket and trial socket. For the short stump, an explanation could be found in one sock less being used at the mapping procedure, whereas no explanation can be offered for the long stump (Figure 5).

Failed socket (too wide with the result that the weight-bearing area was 2 cm2 too large and the stump sunk in the socket; check socket right, trial socket left).
Non-system failures, no failures (table IV)
Non-system related failure or no complaints.
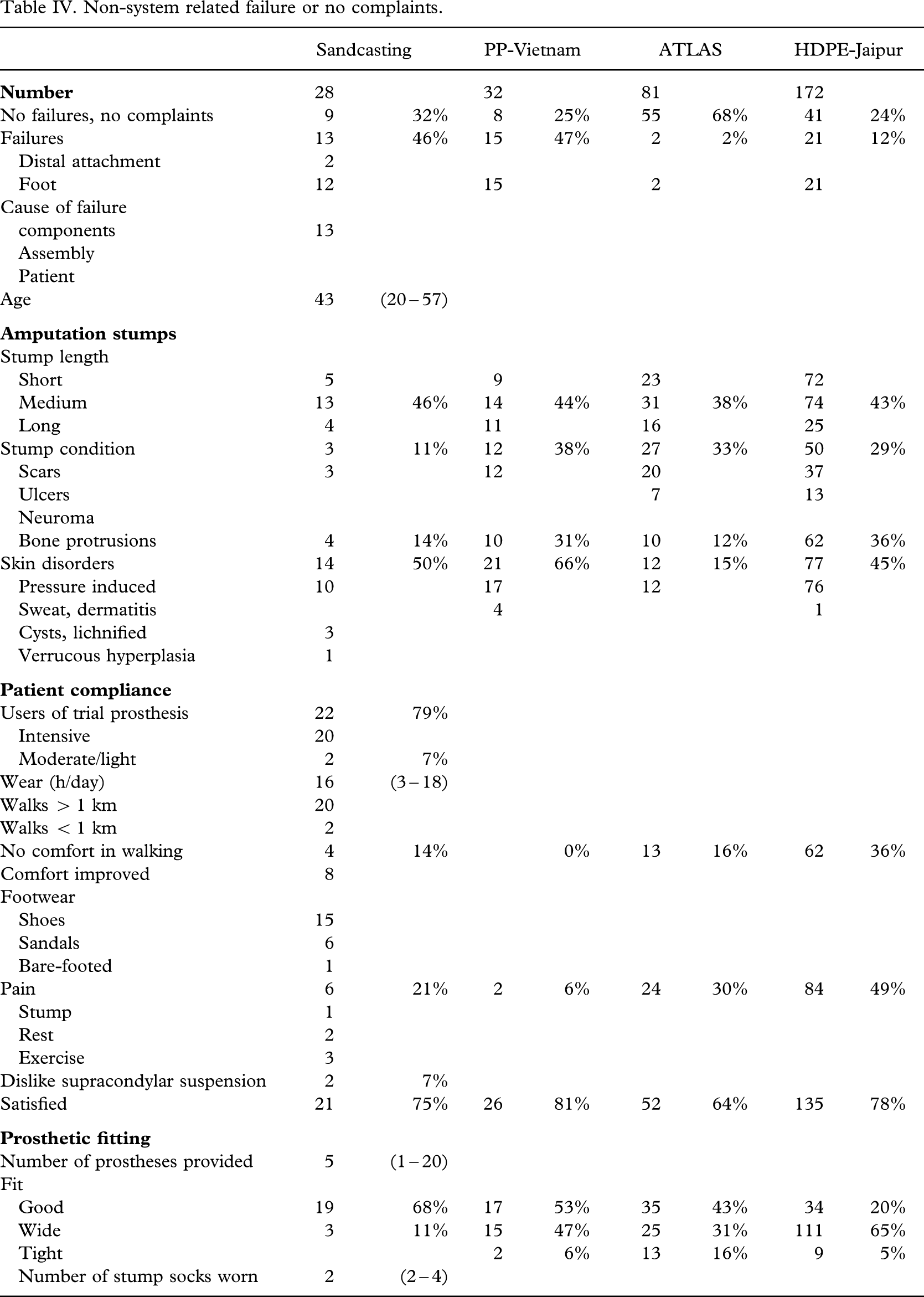
Among the 79% (22/28) of patients without socket failure, breakdown of the distal alignment adaptors, or in particular the polyurethane foam foot, was encountered in 46% (13/28), but this is an issue independent of the sand-casting technique. Clinically, the patient series did not differ much from the historical series.
The interviews revealed that the whole group used the prosthesis and mostly intensively, 16 (3 – 18) h/day, walking more than 1 km, apart from two subjects who had pain and disliked the supracondylar suspension. The others were happy with the suspension and satisfied with the prosthesis. They used a median of three (two to five) socks. Some 75% (21/28) were satisfied with the prosthesis.
Clinically, a fit that was too wide was observed in 11% (3/18). One did not like the supracondylar suspension because of pain and only used the prosthesis occasionally. The two others had no limitations in use, although one had pain, but both were satisfied. They used three and five socks, respectively. The socket mapping was not within the expected pattern.
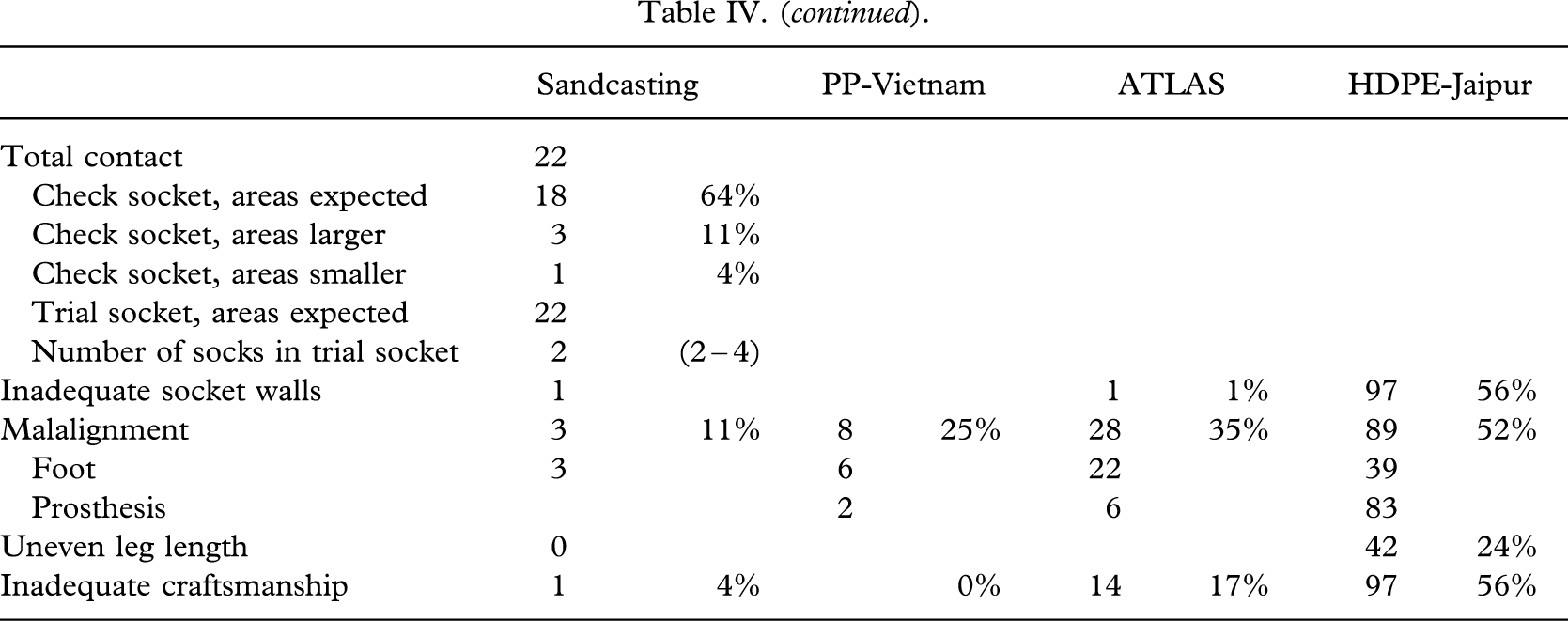
The remaining 19 patients, or 68%, had a good socket fit, and the craftsmanship was found to be satisfactory, with only one inadequate socket wall, and three feet in dorsiflexion.
The socket mapping was as expected in 15/19 (79%) of cases, but three showed larger contact areas at the second mapping indicating sinking. In one case, the sinking amounted to about 20 mm, but as seen from the clinical photograph (Figure 6), the stump was somewhat swollen at the time of manufacturing the prosthetic socket. In the two other cases, no explanation can be offered. As can seen from the tables, there was a high degree of consistency of fit, as reflected by all areas, but one being as expected with the trial socket made at the follow-up and the imprint of the original socket (check socket).

(a) Weight-bearing area increases (check socket left, trial socket right). The short trans-tibial stump was swollen on its first prosthetic fitting.
A few laboratory experiments were carried out in an attempt to cast some light on technical pitfalls. First, PTB-casts were made of four patients according to the CIR technique. A traditional plaster of Paris mould was made, and then the socket was draped on the rectified plaster model. There were no changes in the patterns of socket mapping between these two techniques to that experienced in the test series (Figure 7). Second, a glass wine bottle was sand-cast and dressed in the same fashion as the amputation stumps. It was found that the radius increased between 1.7 and 3.5 mm, which is close to the thickness of the dressing. There was no effect of adding the supracondylar brim.
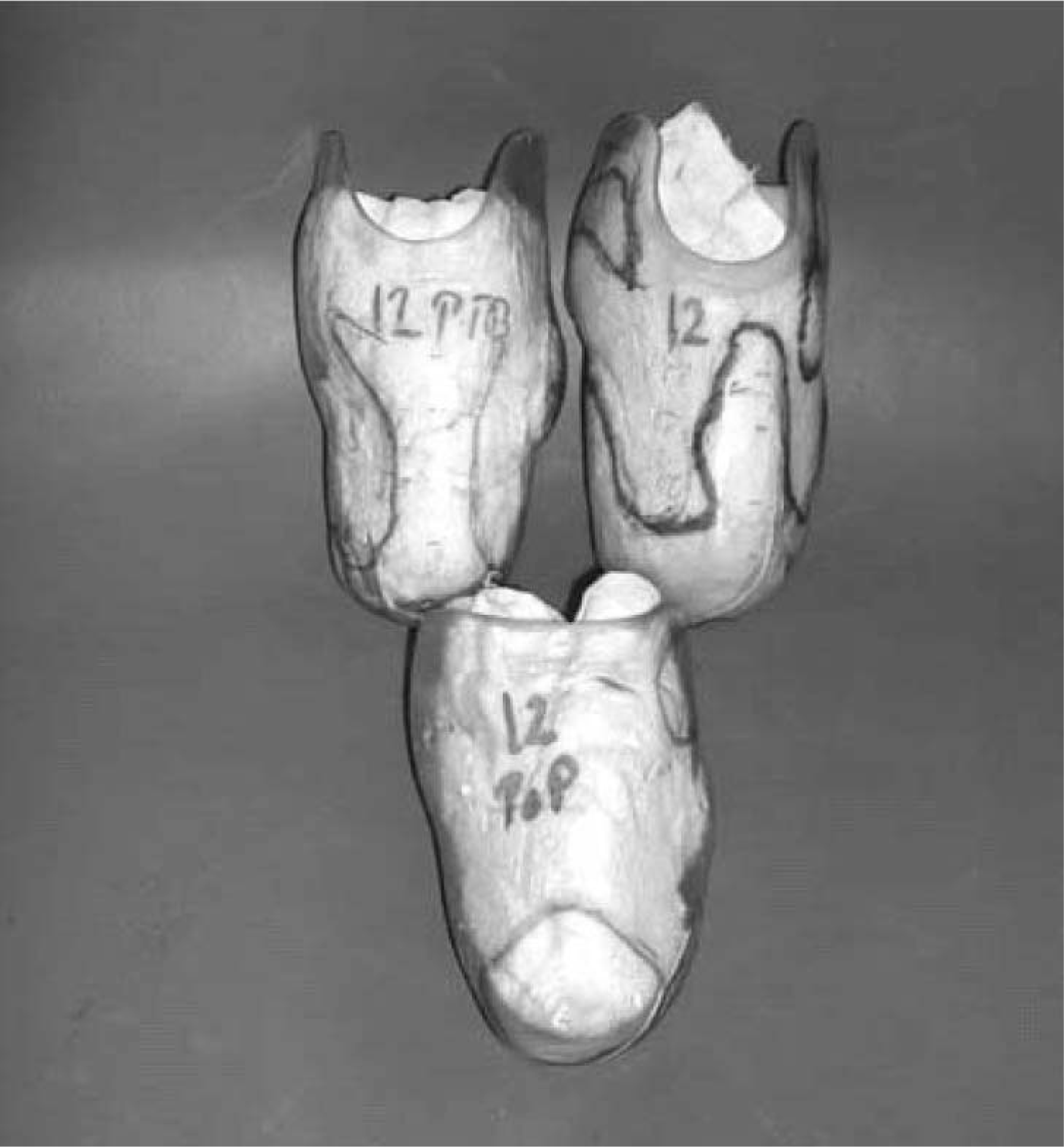
Stump mapping: (top left) PTB socket—sand-cast. (Top right) Trial socket—sand-cast. (Bottom) Plaster of Paris cast without reliefs (check socket). The weight-bearing areas are virtually identical on all three sockets.
Discussion
The results of this patient series using a supracondylar brim and sand-casting technique for trans-tibial prosthetic socket production with regard to fit mostly conformed with data published by Jensen et al. (2005) from a benchmark study, and matched or surpassed data from a number of historical studies conducted by ISPO on trans-tibial prosthetic technology (Jensen and Heim 2000; Jensen and Raab 2002; Jensen et al. 2004, 2005).
The results using the sand-casting method matched those recorded in historical series in respect of failure with conventional plaster of Paris casting carried out by qualified prosthetists (Jensen and Heim 2000; Jensen and Raab 2002), and far exceeded those obtained with artisans using plaster casting and draping with HDPE-Jaipur drain-pipe technology.
The sand-casting technique using the brim still needs the attention of a trained and educated prosthetist with good knowledge about biomechanics and tissue interfacing. Some smaller rectifications have to be made to the positive model before draping. Still, it was not possible to obtain an optimal fit in all cases, and there was a requirement of no less than two thick terry stump socks in most cases to ensure an acceptable fit in use. The clinical relevance of the laboratory findings is that a socket evenly larger than the stump will result from the application of sand-casting. This relates to the dressing of the stump but can be compensated for with the stump socks. The authors did not encounter any stumps with only a proximal fit. However, the requirement of three (two to five) socks would normally be considered on the high side for a good fit.
In conclusion, it was found that the sand-casting technique offers an interesting alternative to plaster of Paris casting, but cannot eliminate the involvement of a professional prosthetist. It might contribute to a more consistent good fit, if correctly used, and does make it possible to manufacture a finished prosthetic socket in less than 1 h. However, it does depend on the vacuum machine and other electrically powered machinery working without power cuts throughout the entire working period. The use of a power generator should be considered.
Footnotes
Acknowledgements
The study was sponsored by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO, and do not necessarily reflect the views of the USAID.