
Abstract
This study compares a standard soft dressing (SSD) with a removable rigid dressing (RRD) in a randomized, controlled trial using 50 dysvascular trans-tibial amputees. Both dressing types were applied immediately post-operatively and were only removed for wound dressing changes. Half the subjects were allocated prospectively by ballot to either the RRD group or the SSD group. There was a strong trend indicating that primary wound healing of the stump occurred almost 2 weeks earlier in subjects using the RRD (RRD = 51.2 days ± 19.4; SSD = 64.7 days ± 29.5; P = 0.07; RRD: n = 17; SSD: n = 14.) There were no significant differences between the other parameters measured which included time to prosthetic fitting, length of hospital stay, incidence of stump breakdown, and time taken for stump volume to stabilize. The incidence of stump damage due to falls was also recorded, the results indicating that RRDs may protect the new stump from trauma.
Introduction
The traditional post-operative stump dressing used at Ballarat Health Services (BHS) consisted of a gauze and wool dressing, held in place with crêpe bandages. These standard soft dressings (SSDs) are adequate but allow the stump to develop considerable post-operative oedema, making the fitting of prosthesis more difficult. Prosthetic fitting may be delayed, and there are often several prosthetic sockets made as the oedema reduces. These dressings also fail to protect the new stump from accidental bumps or trauma.
An alternative to the SSD for trans-tibial amputees is the Removal Rigid Dressing (RRD), which began as the post-operative rigid dressing in the 1970s. The early rigid dressings encompassed the stump and knee, preventing knee motion and knee contractures and were non-removable, preventing inspection of the suture line. These rigid dressings produced shorter rehabilitation hospital stays (Baker et al. 1977). Due to cases of infection and re-amputation, non-removable rigid dressings fell out of favour (Cohen et al. 1974). Their use appears to be hampered by the concern of surgeons and rehabilitation teams about the difficulty of wound inspection, which could delay early detection of wound breakdown or infection (Hughes et al. 1998). Smith et al. (2003) critically reviewed the use of post-operative dressings for trans-tibial amputees. They suggested opinion was divided over the most effective dressing technique because either existing studies were only descriptive or, where controls existed, very few claims had been conclusively proven.
To address problems caused by the non-removal of early rigid dressings, Wu and Krick (1987) described a Removable Rigid Dressing (RRD) made from plaster bandage, which could be easily removed for wound inspection. The authors claimed, but did not demonstrate, that the benefits of the RRD included: soft tissue immobilization and prevention of oedema, which facilitate wound healing; elimination of skin breakdown commonly seen in poorly applied elastic bandaging; protection of the stump from trauma in the event of a fall; provision of early training in stump sock and socket donning which may facilitate independent prosthesis use. A lightweight, easily applied fibreglass casting sock was used in a new version of the RRD (Atkinson et al. 1996).
Some empirical support for RRDs exists. Removable rigid plaster casts reduce stump volume (Mueller 1982), promote more rapid healing and are associated with a shorter duration of hospitalization (Vigier et al. 1999) when compared with gauze dressings or elastic compression bandages. RRDs may reduce the time to fitting of a prosthesis (Hughes et al. 1998; Woodburn et al. 2004), but this has not been demonstrated conclusively. When compared with thigh-length rigid dressings, RRDs may have the disadvantage of allowing knee contractures to develop, and suggestions have been made to prevent such contractures (Hughes et al. 1998). Although faster wound healing, less oedema, shorter hospitalization and quicker prosthesis provision imply improved prosthetic treatment, no investigation of the effect of RRD on an already rapid rehabilitation service was found.
This study sought to compare a standard soft dressing with a fibreglass, removable rigid dressing in a randomized, controlled trial using 50 dysvascular trans-tibial amputees. The setting was a hospital at which both acute and rehabilitation services were provided. The centre has a practice of early prosthetic casting and fitting. It was expected that the RRD would prevent oedema from developing, and it was hypothesized that, when compared with the SSD, the RRD would be associated with less time to primary wound healing; reduced time to prosthetic fitting; reduced total inpatient stay duration; and a lower incidence of post-surgical trauma to the stump; and that stump volume would stabilize earlier, as indicated by a need for fewer prosthetic sockets in the first 6 months following amputation. The effect of containment was being investigated, not the effect of active compression, so no silicone sleeve, elastic bandaging, or shrinkers were used in the RRD group until after healing occurred.
Method
Subjects
Fifty (50) consecutive trans-tibial amputees from the vascular units of both the public hospital acute site (BHS) and the local private hospital (St John of God), who consented to participate, were included in the study. The amputees were randomly allocated by ballot into two groups, with 26 in the RRD group and 24 in the SSD group. There were no significant differences between the two groups of amputees in terms of age, sex, side amputated, or incidence of diabetes (Table I).
Details of the two groups of amputees (RRD and SSD subjects after initial exclusions)a.
RRD: removable rigid dressing; SSD: standard soft dressing.
Exclusions
A number of exclusions were applied, which resulted in not all subjects being included in all categories of analysis. The number of subjects included in each category of results is shown in each instance and is listed inTable II. Complications were divided according to whether or not they were related to stump healing. These included revision to trans-femoral level and surgical debridement, but not delayed healing where no intervention occurred. Medical complications included organ failure or illness not directly related to residual wound healing.
Number of patients excluded from each analysis and reasons for exclusiona.
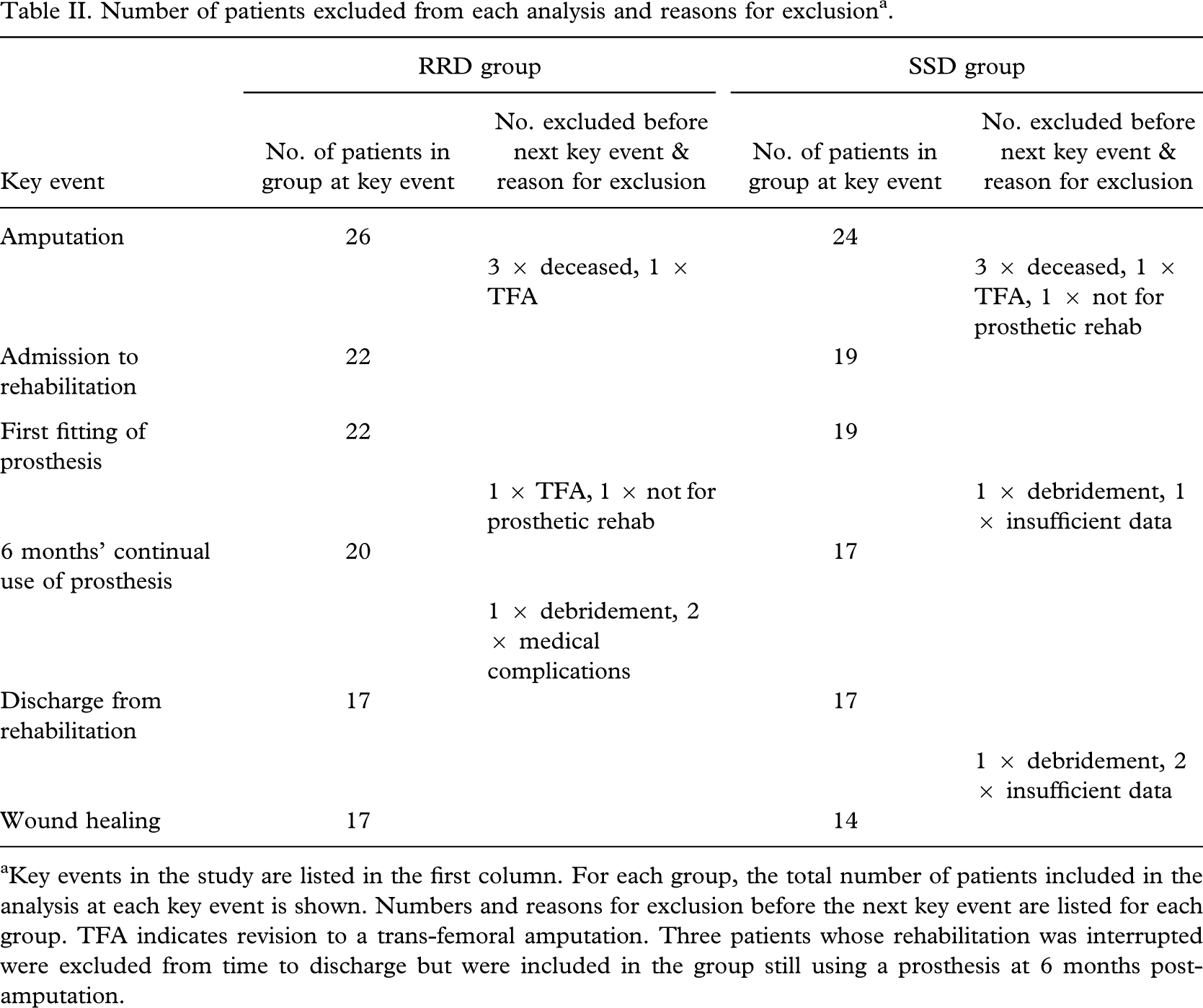
Key events in the study are listed in the first column. For each group, the total number of patients included in the analysis at each key event is shown. Numbers and reasons for exclusion before the next key event are listed for each group. TFA indicates revision to a trans-femoral amputation. Three patients whose rehabilitation was interrupted were excluded from time to discharge but were included in the group still using a prosthesis at 6 months post-amputation.
To indicate the volume control of the two dressing types, the number of sockets required over a 6 month period was measured. All the amputees discharged from the rehabilitation ward using a prosthesis were included. The two in the RRD group who had their rehabilitation interrupted by medical complications were included in this measure, as was one who underwent a wound debridement.
Materials and protocol
The SSD cohort continued to use the standard soft stump dressing post-operatively, having it applied in theatre according to the usual surgical practice. This consisted of gauze, a wool pad, and a crêpe bandage. The other group had the removable rigid dressing applied in theatre or in the recovery room within 20 min of wound closure by the treating prosthetist and assistant. The RRD was fabricated over a thin non-adherent dressing (‘Tegaderm’) and a ‘coolmax®’ terry-toweling sock (Law Comfort, Melbourne, Australia). The method of application is described by Atkinson et al. (1996) and similar to Wu and Krick (1987), except that a fibreglass and resin sock (Seattle Shapemate®) was used in place of plaster. The surgical finishing details were standardized across both groups. All amputations were done using a long posterior flap, closed with a continuous suture, ‘steristrips’, with a drain exiting proximally.
The amputees wore their SSDs or RRDs 23.5 h a day; the dressings were removed only for wound dressing or inspection and were not left off the stump for longer than 15 min per episode until casting for prosthetic fitting. The decision to cast for a prosthesis was made by the rehabilitation team. The prostheses were thermoplastic sockets made over a modified cast and a ‘Pelite’ liner, set up on lightweight endoskeletal components. Since initial prosthetic fitting usually occurred before complete stump healing, the SSDs and RRDs were replaced at this time with a thin, well-adhered dressing. When not wearing their prosthesis, the RRD group continued to wear their rigid dressing, with increasing sock thickness as necessary to accommodate reducing stump volume, while the SSD group was bandaged with blue-line elastic bandage. Once healing occurred, subjects stopped using their respective dressings. The nursing staff performed an assessment and documentation of date of wound healing. An education programme was implemented across the acute and rehabilitation sites of the hospitals to teach all staff involved about the study protocols.
Data collected
Data collected included:
client demographics
dates of key events
amputation
admission and discharge from both acute and rehabilitation settings
prosthetic fitting
wound healing
any incidents that affected wound healing (e.g. falls, infection)
concomitant disorders
medications
dressings
the number of prosthetic sockets provided in the 6 months from the date of amputation.
Simple calculations were performed to give the following time durations (in days) for each subject:
from amputation to admission to rehabilitation (amp-adm)
from amputation to first prosthetic fitting (amp-fit)
from amputation to discharge from rehabilitation (amp-d/c); this was also referred to as total inpatient stay, but the number of days in the acute setting prior to amputation was not included in the calculations because this time was unrelated to the dressing type used
from amputation to date of healing (amp-heal); healing was as defined as ‘complete, pink epithelial bridging of the suture line’ (Hallam and Jull 1988).
Data analysis
Data were averaged for all subjects in each group. Independent t-tests were used to test for differences between the two groups for each variable. Significance was determined at the P < 0.05 level, and one-tailed tests were used when directed hypotheses existed.
Results
Wound healing
There was a strong trend suggesting that primary wound healing of the stump occurred almost 2 weeks earlier in those subjects using the RRD. Mean days to healing in the RRD group were 51.2 days ± 19.4, compared with 64.7 days ± 29.5 in the SSD group; P = 0.07 (RRD: n = 17; SSD: n = 14) (Figure 1).
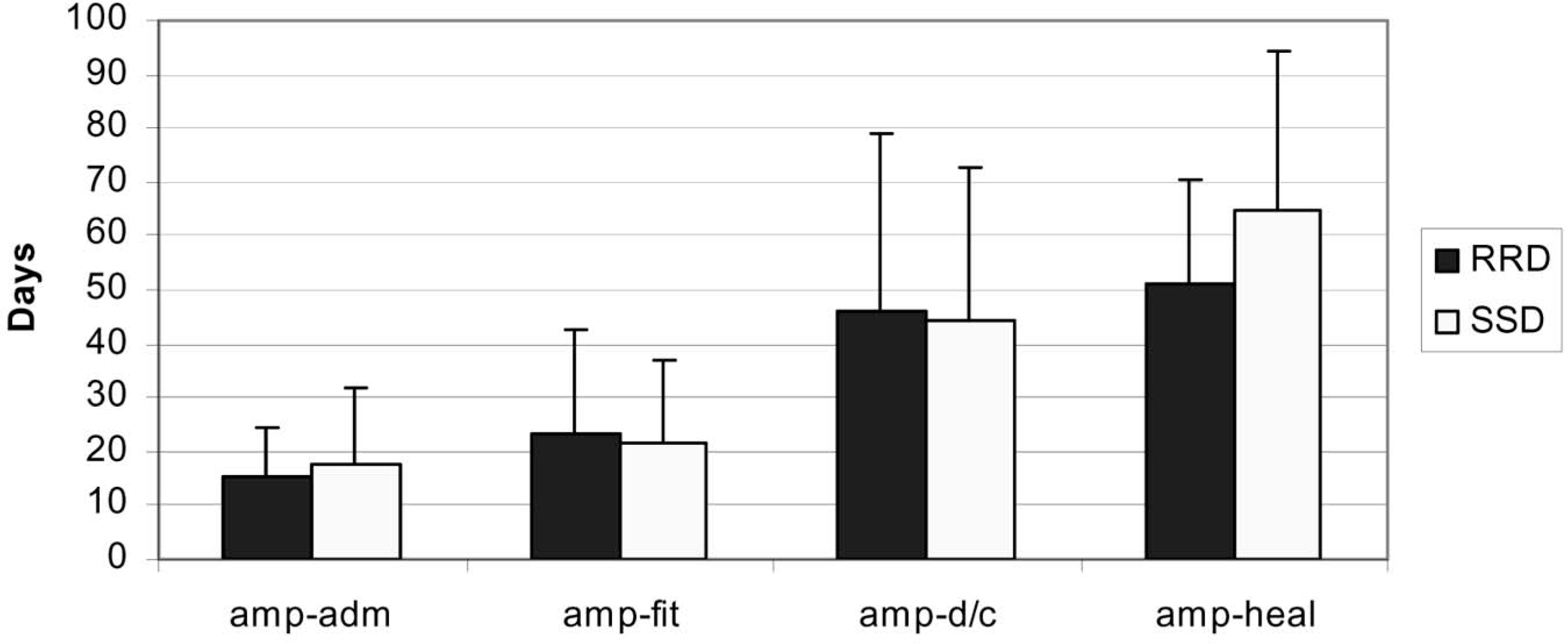
Summary of results showing the mean number of days between amputation and admission to rehabilitation (amp-adm); between amputation and prosthetic fitting (amp-fit); between amputation and discharge from inpatient rehabilitation (amp-d/c); and between amputation and the date of stump healing (amp-heal). Removable Rigid Dressing (RRD) cohort is compared with the Standard Soft Dressing (SSD) group. Error bars indicate the standard deviation; ≈ indicates a trend towards a significant difference (P = 0.07).
Time to prosthetic fitting
The RRD group was fitted 23.3 days ± 19.5 post-amputation, while the SSD subjects were fitted at 22.6 days ± 15.7; P = 0.45 (RRD: n = 22; SSD: n = 19) (Figure 1).
Inpatient length of stay
The mean number of days in the acute setting after amputation was 15.5 days ± 9.2 for the RRD subjects and 17.4 days ± 14.3 in the SSD group; P = 0.61 (RRD: n = 22; SSD: n = 19). The mean number of days between amputation and discharge from rehabilitation (considered to be the total length of stay) also showed no significant difference between the two groups: RRD = 46.1 days ± 32.7; SSD = 44.6 days ± 28.0; P = 0.38 (RRD: n = 17; SSD: n = 17) (Figure 1).
Discussion
Faster wound healing
There was a strong trend supporting the first hypothesis that there would be less time to primary wound healing in the RRD group. The RRD group healed on average 13.5 days quicker than the SSD group. This supports the findings of Vigier et al. (1999), who had a faster rate of healing in their RRD/silicone group (71.2 days compared with the control group's 96.8 days). Healing times at BHS were 20 – 30 days less than in Vigier et al.'s (1999) paper. However, in the Vigier study, RRDs also included the variable of a silicone sleeve, were only worn for a maximum of 5 h/day, and were not applied immediately after surgery. Any of these differences may account for the overall slower healing rate of the Vigier subjects.
Wu et al. (1979) reported an even larger reduction in healing time in a RRD group compared with SSD (46.2 days and 109.5 days, respectively). However, their definition of wound healing was taken to be the date that the first prosthesis was requested, which may not accurately reflect the date of healing.
A larger sample group would have been necessary to achieve statistical significance at (P ≤ 0.05) with regard to wound healing in the present study. Because of the apparent success of the RRD, it was deemed unethical to persuade surgeons and other staff that it was appropriate to continue to withhold the RRD from half of the new amputee population. BHS now fits RRDs to all new trans-tibial amputees.
Time to prosthetic casting and fitting
Casting generally occurred at approximately 20 days for both groups, much sooner than the 42 days (SSD) and 36 days (RRD) findings of Woodburn et al. (2004). The time to prosthetic fitting was similar in both groups. Hughes et al. (1998) reported more rapid fitting after introducing a RRD programme. However, they started with much longer time frames and reduced their average time to fitting from 101 days to 46 days.
Although this study did not demonstrate a reduction in time to fit, the centre has had an early fitting policy in place for many years, with amputees being fitted (usually prior to primary wound healing) at around day 21 post-surgery. It may be impossible to further reduce the time to prosthetic fitting due to post-operative stump pain. A floor effect may exist in regard to early fitting and weight bearing in a prosthesis.
Reduction in inpatient stay
There was no significant difference between the groups in time from amputation to rehabilitation admission; time from amputation to prosthetic fitting; or total inpatient length of stay. This contradicts the findings of other authors who have demonstrated a reduction in inpatient stay with the use of RRDs (Hughes et al. 1998; Vigier et al. 1999), and with thigh-length rigid dressings when compared with soft dressings (Baker et al. 1977). However, the shorter hospital stays achieved with rigid dressings (both removable and non-removable) by these researchers are much longer than that of both groups in the present study. It is possible that the inpatient stays reported in this study are approaching the lower limit. The annual mean length of stay for amputees in rehabilitation at BHS has varied between 19 and 30 days over the last 12 years.
Decreased stump breakdown
The qualitative data on the stump damage incurred as a result of falls indicate that the RRD may have a protective function when compared with SSDs. No stump damage was reported in those four subjects in the RRD group who fell in the acute setting. However, in the SSD group, three of the six subjects who fell required stump revision surgery, with two subjects being revised to become trans-femoral amputees. Although authors have claimed that a protective effect is likely (Woodburn et al. 2004; Wu and Krick 1987), there is no statistically significant evidence to support the assumption that rigid dressings protect new amputation stumps from injury. However, the retrospective descriptive study by Hughes et al. (1998) demonstrated a 22% reduction in injury to trans-tibial stumps (down to a zero incidence) after the introduction of an RRD programme.
Earlier stump volume stabilization
The number of prosthetic sockets was measured as a clinical indicator of volume control, and no differences between the groups were found (P = 0.26; RRD: n = 20; SSD: n = 17). Amputees in the RRD group required an average of 1.33 sockets, while those in the SSD group required 1.47 sockets. Although the difference in the number of sockets was not significant, it is possible that further investigation with a larger sample would produce a statistically significant result. Alternatively, direct measurements of stump volume could be taken by filling sockets with water as described by Graf and Freijah (2003) and Johansson and Öberg (1998).
Other benefits
There have been other unintentional benefits from this research project. The communication between staff working with amputees at the acute and rehabilitation sites, as well as those at the private hospital, has developed significantly. There have been regular meetings of the amputee team and the vascular surgeons, resulting in standardization of post-operative dressings and procedures, and the possibility of development of a ‘care pathway’ across the two sites.
The amputee team is now always forewarned about each new amputee. The surgeon, theatre staff, or nursing staff informs the prosthetist of an impending trans-tibial amputation so that the prosthetist can be present at the close of the surgical wound, ready to apply the dressing. The physiotherapist treating amputees at the acute site reported that she was much more confident to exercise new amputees with the stump more protected. Nursing staff report a decreased amount of time spent dressing and re-bandaging stump wounds.
Conclusion
There was a strong trend towards faster wound healing in the RRD group. Those with RRDs healed almost 2 weeks faster than those fitted with SSDs. There were no statistically significant differences between the two groups in the other parameters measured. Qualitative effects were noticed, which may indicate areas for further investigation. Those with RRDs may be less likely to damage their stumps in the event of a fall and more likely to avoid subsequent surgical revision or debridement. Overall, RRDs are likely to be beneficial to the rehabilitation of new trans-tibial amputees. Further research is indicated to confirm these results with a larger sample.
Footnotes
Acknowledgements
The authors would like to thank Ms Margaret Hodge, President of ISPO Australia and Lecturer at Latrobe University (Melbourne, Australia) for her assistance with data analysis.