
Abstract
The provision and maintenance of prostheses in 100 trans-femoral amputees and 73 trans-tibial amputees were retrospectively analysed over a 10-year period. The aim of the study was to analyse the prosthetic episodes, i.e., the need for maintenance, repairs and replacements to a trans-femoral and a trans-tibial prosthesis and frequency of new sockets prescribed over the same period of use by established adult amputees. The study showed that the trans-femoral amputees needed 0.96 new prostheses, 3.27 new sockets, 2.31 major repairs, 3.36 component changes and 21.85 minor repairs. Younger trans-femoral amputees aged less than 60 years needed 1.1 new prostheses, 3.15 new sockets, 2.06 major repairs, 4.23 component changes and 20.49 minor repairs. Younger trans-femoral amputees needed significantly more changes of prosthetic components (p = 0.04). The associated study on 73 trans-tibial amputees showed that they needed 1.4 new prosthesis, 2.9 new sockets, 3.2 major repairs and 14.1 minor repairs over the same 10-year period. The introduction and prescription of modular prosthesis as opposed to conventional limbs used earlier has possibly allowed components to be easily replaced thus reducing the need to replace a whole new prosthesis.
Introduction
Rehabilitation following an amputation includes provision of the initial prosthesis, physiotherapy and gait re-education and a programme for life-long maintenance of the prosthetic needs. Planning of this service needs to consider the natural history of maintenance needs for replacement, repairs and adjustments to the prosthesis. This study aims to assess the frequency of new prosthesis provision, repairs and adjustments to sockets and prosthetic components to established amputees.
In 1999, Datta et al. published the results of a retrospective survey to assess the provision and maintenance needs of trans-tibial amputees attending their centre, by studying the number of prosthetic episodes. Their study was able to provide valuable insight into the prosthetic requirements of unilateral trans-tibial amputees irrespective of mobility levels. However, there are no studies that assess the similar prosthetic needs of trans-femoral amputees. There are significant differences between trans-femoral and trans-tibial amputations and the prosthesis. It is apparent that the trans-femoral stump has a proportionately larger muscle mass which is likely to undergo volume changes due to atrophy over time (Jaegers et al. 1995) whereas the trans-tibial stump is generally more bony.
A trans-femoral prosthesis has a larger number of components than a trans-tibial prosthesis as it incorporates a knee mechanism. These differences could account for some differences in the prosthetic maintenance needs. Trans-femoral amputees require larger energy consumption than a trans-tibial amputee (Gonzalez et al. 1974; Waters et al. 1976; Huang et al. 1979). This in turn can reduce mobility grades and usage of the prosthesis.
The results of the study by Datta et al. (1999) were broadly applicable throughout the UK to trans-tibial amputees but due to reasons mentioned above they would not necessarily be applicable to a trans-femoral amputee. Furthermore, it could be questioned whether the development of new technologies or changes in clinical practice may influence episodes in the maintenance of prostheses.
Patients and methods
A retrospective case note review was carried out of trans-femoral and trans-tibial amputees attending the Disablement Services Centre (DSC) at the Royal National Orthopaedic Hospital at Stanmore. The Disablement Services Centre at Stanmore is a regional centre for prosthetic rehabilitation and serves a population of approximately 2 million. It manages an amputee population of approximately 1450 and receives approximately 195 new referrals every year. The policy of the centre has been to avoid placing any limitations on prosthetic components that may be prescribed to the amputee population if needed.
The inclusion criteria for patients in the study were: Unilateral trans-femoral and trans-tibial amputees; Age >16 years; Prosthetic use for mobility for at least 10 years at the time of the study; and The amputees had to be attending the centre between 1993 and 2002.
Patients using only a cosmetic prosthesis were excluded. The rationale for excluding
amputees <16 years of age was that their prosthetic changes are likely to have been
influenced by developmental growth because they had not yet achieved skeletal maturity.
Each of the case notes of patients who met the eligibility criteria was manually reviewed.
An electronic data collection form was devised to collect relevant information from the case
records of the included amputees. A record was kept of the various types of prosthesis used
and the major components that needed replacing. A record was also made of the number of
prostheses that was used concurrently and the mobility grades whenever they were documented.
Mann-Whitney U tests were carried out to test for statistical significance between younger
(<59) and older (≥60) patients and between traumatic and vascular amputees. To enable
comparison of the results of this study on trans-femoral and trans-tibial amputees with
those of the study carried out by Datta et al. (1999) on trans-tibial amputees we utilised similar
definitions of the 4 different types of prosthetic episodes. However it was considered
necessary to include a section on component changes as this was specifically relevant to
trans-femoral prostheses. Five different types of prosthetic episodes were analysed: New prosthesis: A new duplicate prosthesis was issued when an
existing prosthesis was considered to be beyond economical repair. Sometimes a new
prosthesis was also issued to suit the patients changed functional or specific needs
such as high activity, water activity limb etc.; New socket: A new socket was issued when the old socket was no
longer fitting well or the socket was damaged. Attendances for fitting of a new socket
or prosthesis were considered to be a single prosthetic episode; Major repair: Any repair that needed the prosthesis to be retained
overnight at the centre. Minor repair: All repairs that were carried out at the centre on the
same day. These included repairs such as adjustments to the socket, adjustments to the
knee or ankle; Component changes: Replacement of major components such as a knee
mechanism, shin or foot and ankle unit. Simple replacement of belts or straps were
included under minor repairs.
Results
Patient records of a 100 trans-femoral (84% male: 16% female) and 73 trans-tibial (82% male: 18% female) amputees that met the inclusion criteria were included in the study. The mean age for the trans-tibial amputee was 55.2 years (range 18 – 86) and for trans-femoral amputees was 61.6 years (range 26 – 94). Trauma was stated as the cause leading to amputation in 60% of both trans-femoral and trans-tibial amputees (Table I). Almost all (98%) of the trans-femoral amputees and all trans-tibial amputees had at least 2 prostheses for use concurrently.
Diagnostic categories.
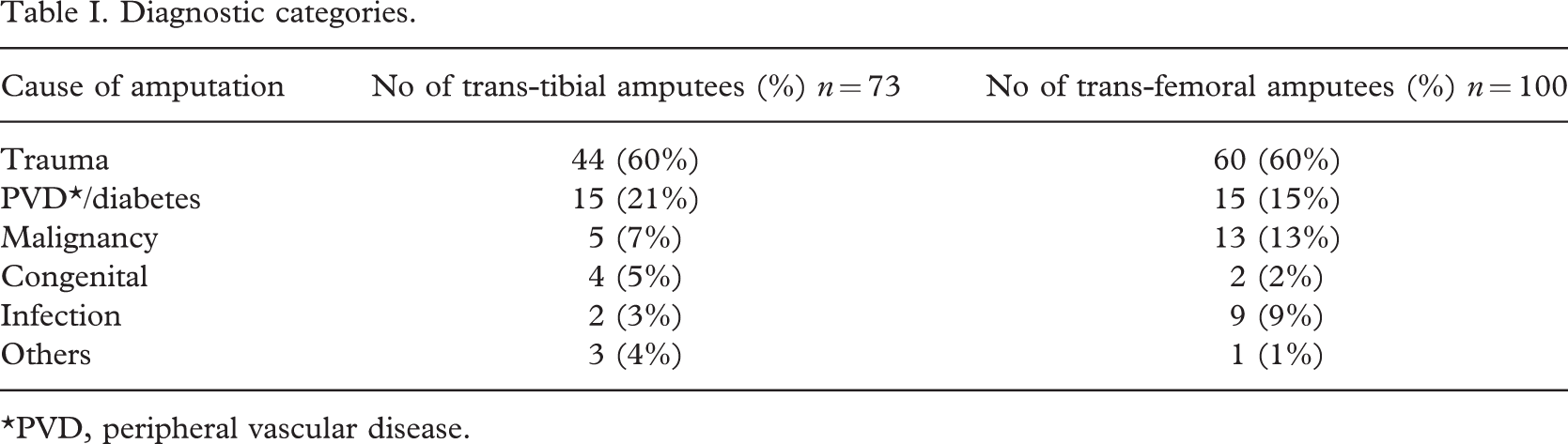
∗PVD, peripheral vascular disease.
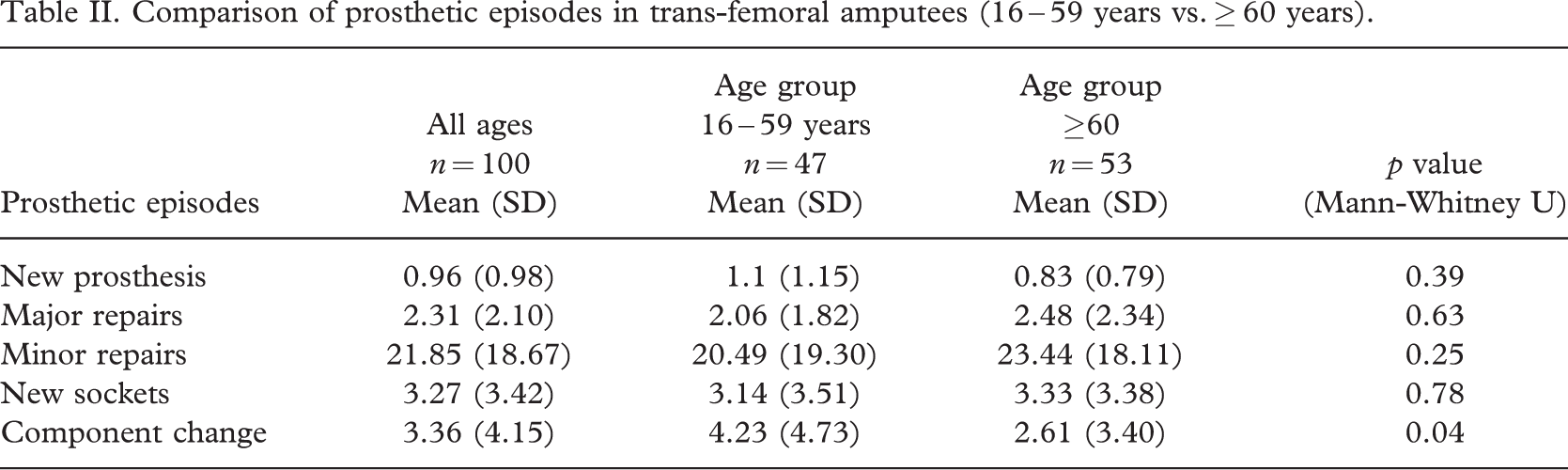
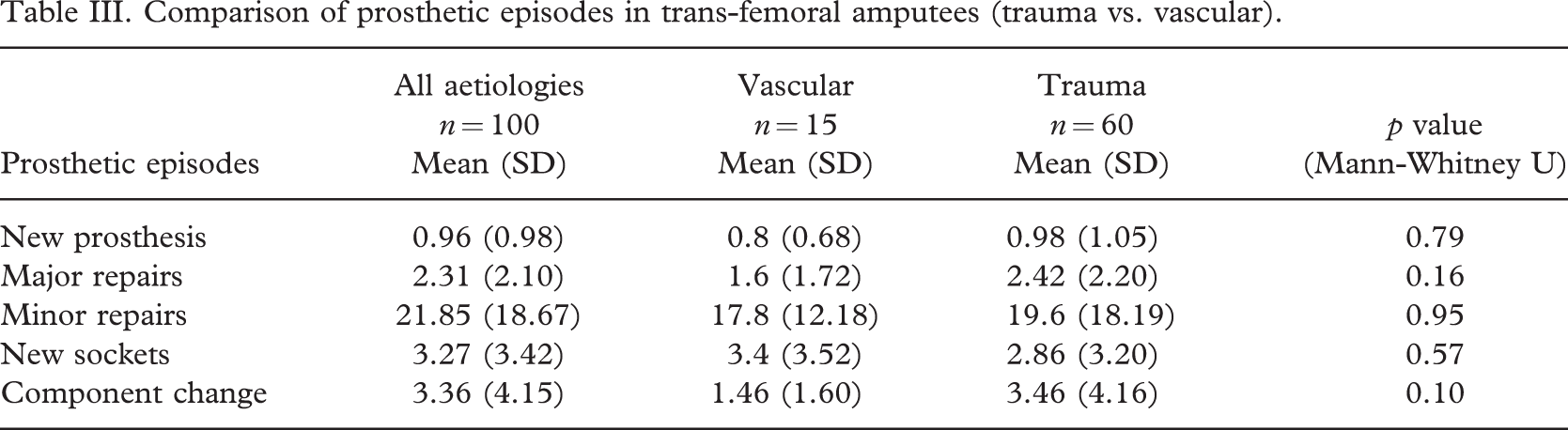
Over the ten-year period of the study each of these unilateral trans-femoral amputees needed 0.96 new prosthesis, 2.31 major repairs, 21.85 minor repairs, 3.27 new sockets and 3.36 component changes. There was no statistically significant difference in the need for new prostheses, new sockets or repairs when the results of amputees <60 years of age were compared with those ≥60 years. However, there was a statistically significant difference in the need for new components with amputees below 60 years needing more component replacements. Amputees aged below 60 years needed an average of 4.23 major component changes compared to 2.61 for those aged 60 years and over. Table II shows the means and standard deviations for the resulting numbers in each prosthetic episode for the age groups and Table III shows the comparison between the traumatic and dysvascular amputees. This showed that there was no statistically significant difference in any of the 5 categories but showed a trend for more repairs and component changes but fewer new sockets in the traumatic amputee group.
Comparison of prosthetic episodes in trans-femoral amputees (16 – 59 years vs. ≥ 60 years).
Comparison of prosthetic episodes in trans-femoral amputees (trauma vs. vascular).
The documentation of mobility grades was found to be inconsistent and in a few patients the mobility grades deteriorated during the 10-year duration of the study. Therefore no attempt was made to analyse the data on mobility grades.
The results of the prosthetic maintenance needs for the 73 trans-tibial amputees are shown in Table IV. Over the ten-year period of the study each unilateral trans-tibial amputee needed 1.44 new prostheses, 3.16 major repairs, 14.19 minor repairs and 2.89 new sockets.
Comparison of prosthetic episodes in trans-tibial amputees at DSC Stanmore (16 – 59 years vs. ≥ 60 years).
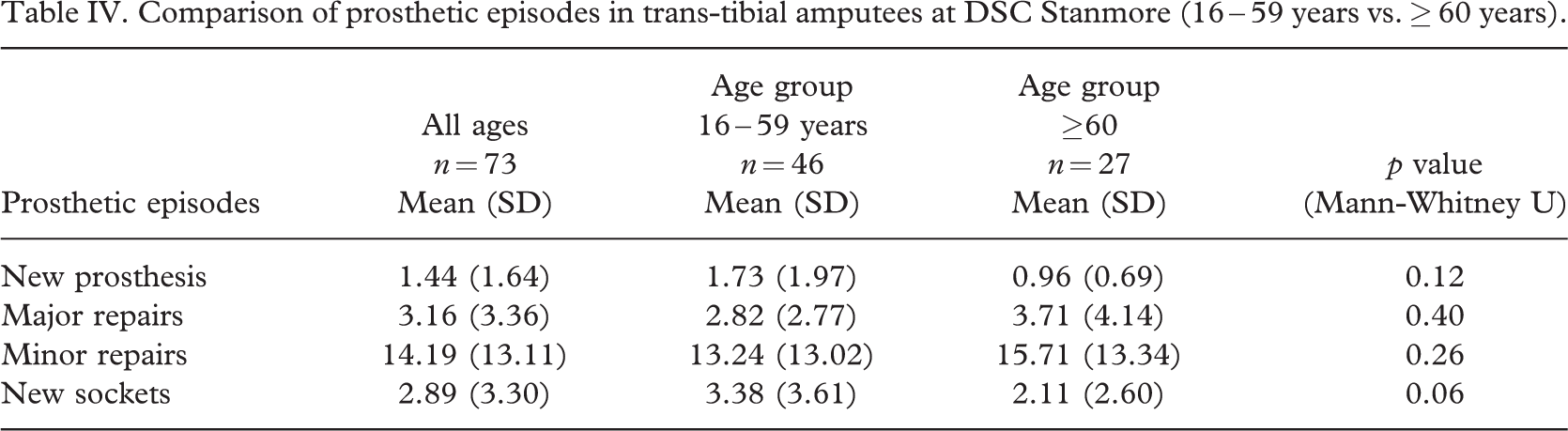
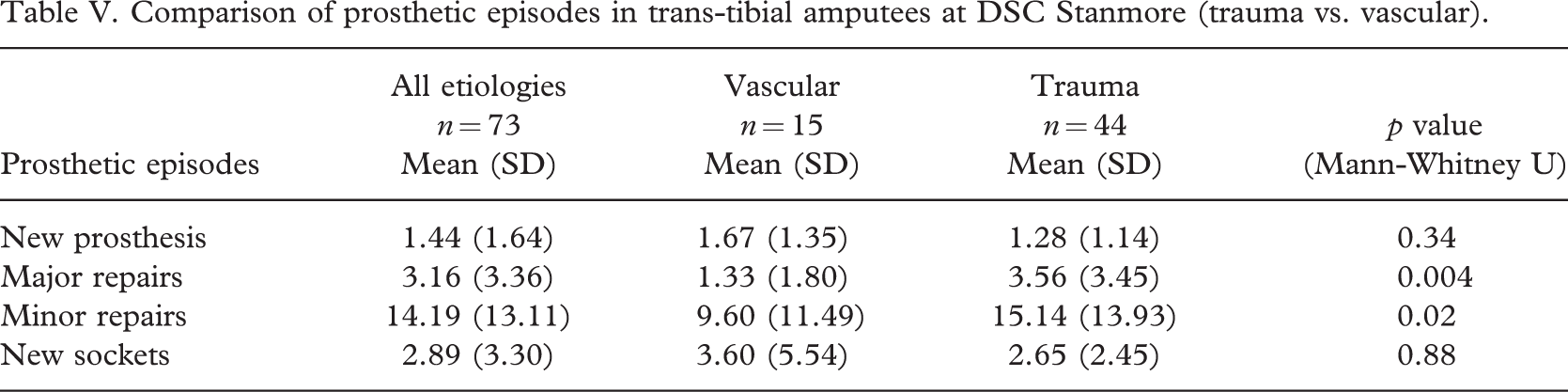
Further analyses of the trans-tibial prosthetic episode results show that there is a trend towards statistical significance with younger amputees needing more new sockets than older (>age 60 years) amputees (Table IV). When the data are compared by diagnosis causing amputation (Table V) there were clear statistically significant differences. The traumatic trans-tibial amputees needed more major and minor repairs than dysvascular trans-tibial amputees (see Figure 1).
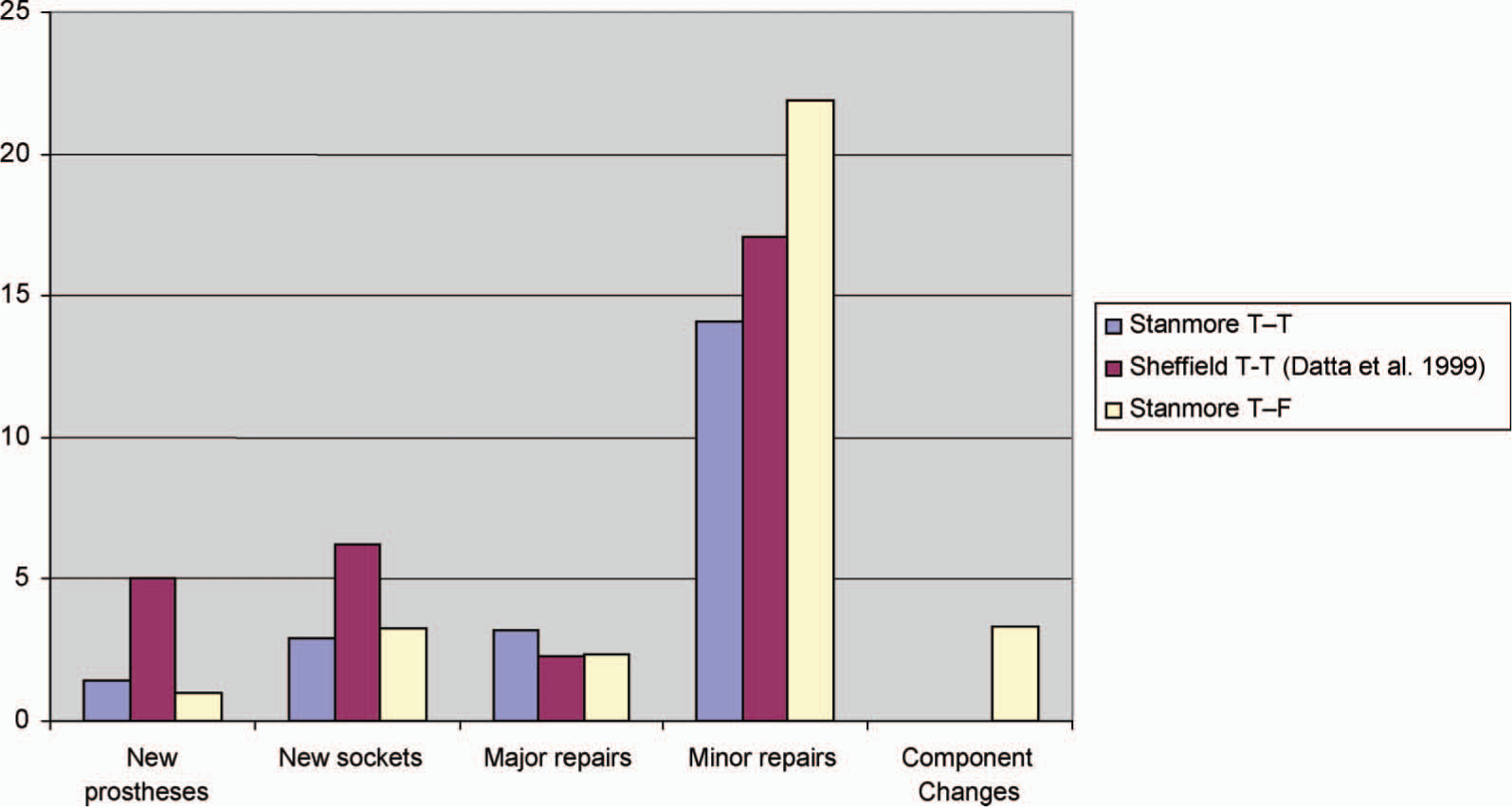
Graph comparing results of trans-tibial prosthetic episodes across 2 centres and the trans-femoral episodes at the DSC Stanmore.
Comparison of prosthetic episodes in trans-tibial amputees at DSC Stanmore (trauma vs. vascular).
Trans-tibial prostheses were 4 times more frequently replaced and sockets were twice as frequently replaced in the cohort studied by Datta et al. (1999) than in the present study's trans-tibial group. However, when it came to the provision of new prostheses in this sample at the DSC Stanmore, both trans-femoral and trans-tibial replacements were fewer than those observed by Datta et al. (1999).
Discussion
The most significant finding of our study on trans-femoral amputees was that they needed an average of only 0.96 new prostheses over a 10-year period. This could be due to the greater number (3.36) of major components replaced. Thus a trans-femoral prosthesis may have had a new knee, as well as a new foot and ankle at different times over the 10-year period. The increase in the number of component changes in the modular build of the prostheses accounts for the reduction in the number of new prostheses prescribed. This form of maintenance is more rational as it is specifically targeted to the need. A trans-tibial modular prosthesis on the other hand has fewer individual components, and could have been easily and economically replaced each time a socket needed renewing and the nature of the service contract permitted it. The authors recognize that over a 10-year period various components of the originally prescribed limb may have been changed and thus the original prosthesis will have been entirely replaced in parts. However, the sum total of the different types of prosthetic episodes as defined by the authors' criteria would have accounted more accurately to the amputee's needs than if s/he was provided with new limbs when only a single component needed replacement.
All amputees at the rehabilitation centre were at the time eligible for and were prescribed 2 prosthesis with the second limb generally as a spare and duplicate. A study by Keetarut (1989) showed that two-thirds of the amputees did not routinely use the second limb. If the socket fit is poor it is likely that the spare limb would also require a new socket. With the use of modular components, repairs could if required be done on the same day. These reasons may explain the poor use of the second limb. The present study included all episodes whether they occurred to the first or the spare limb.
Lifestyle and increased activity affects the product life of the prosthesis. Dysvascular amputees are likely to have associated cardiovascular and other systemic disease affecting their activity levels. It was also anticipated that the younger adult amputees were more active and would therefore need more repairs or replacements. However, the reason that younger patients with trans-femoral amputations (<60 years) did not need more repairs or new prostheses is almost certainly because of the significantly larger number of replacements of major components that were required. A statistical trend towards more repairs and component changes in the traumatic group possibly reflects the increased activity in these patients when compared to the dysvascular amputee. There was a statistically significant difference in the tans-tibial amputees in this study with the traumatic amputees needing more major and minor repairs than the dysvascular amputees. The preponderance of traumatic amputees (n = 60) over dysvascular amputees (n = 15) in the cohort studied can be explained by the fact that most dysvascular amputees, with their reduced life expectancy (Stewart et al. 1992) did not survive the whole 10-year period of the study to meet the inclusion criteria.
It would however be erroneous to conclude that the DSC at Stanmore was more reluctant in prescribing new prostheses. It is believed that the reason for this difference between the results from the study by Datta et al. (1999) lies in the fact that the two studies assessed a different 10-year period with only half the period overlapping. During this time there have been changes following the publication of the McColl Report (UK Department of Health and Social Security [DHSS]1984) leading to regionalisation of the service and modernisation. The study period by Datta et al. (1999) was 1988 – 1997 whereas the10-year period for the present study was 1993 – 2002. In the earlier years a greater number of conventional limbs were used as opposed to a larger number of modular limbs used currently. Furthermore, the earlier national contracts of service from the prosthetic manufacturers, where a new trans-tibial socket may have cost only marginally less than a new prosthesis inadvertently encouraged over-prescription. The cost, clinical practice, prosthetic components and prescriptions have changed and standards of service have been developed (British Society of Rehabilitation Medicine [BSRM]2003). A greater range of prostheses are currently available and the service has been rationalized in the National Health Service (NHS) in the UK since 1991.
While it could be argued that this study measures ‘provision’ rather than ‘need’, if the prescription was on the basis of ‘need’, as was the practice at Stanmore, then it also reflects the prosthetic need of the amputee population at the centre.
Product life
The primary issue for the manufacturers of prostheses is the safety of the prosthetic components used. For the last two decades, the International Standards Organisation (ISO) working group has studied the relationship between structural strength and activity of amputees. During this period the nature of the components has changed from more rigid conventional systems to flexible modular ones. This has also resulted in a 10% increase of load generated and possibly associated with increased activity and changes in lifestyle (ISO 1999).
Data collected by the ISO and the UK Department of Health on reported failures of components helped develop the ISO 10328 standards for safety of prostheses. These standards (ISO 1996) are associated indirectly to body mass and activity. The current standard requires 3 million cyclical applications of load to satisfy the required fatigue strength. Ironically, it has been noted that a foot post-person typically takes 5 million steps per year whereas any other able bodied subject takes 1.5 million steps in a year. For insurance purposes, the German system equates 3 million cycles with 3 years of prosthetic life and the UK system equates it to 5 years. With improvement in design and manufacture, many highly functional manufacturers' warranties are for 3 years with extended warranties available for 5 years. Clearly many parts of modular components may survive longer. The authors recognise that components manufactured by different companies may have different durabilities.
A pilot study (Ross and Reece 2006) to assess two typical amputees' usage of prostheses over a 3-month period showed a variation of 2000 – 40,000 steps per week highlighting the issue of correlating structural safety of the modern prosthesis to the life cycle of the device and its relation to the amputee's lifestyle, behaviour pattern and activity. Despite a very low rate of reported failure, an attempt to recycle prosthetic components could risk increased malfunction and structural failures.
Components are tested for their durability in laboratories by testing the number of repetitive cycles of use it can withstand. In practice there may be other factors such as stump volume changes and fitting problems that may influence the need for a new prosthesis. While the laboratory analysis and manufacturers' guarantee periods are useful indicators of the anticipated durability of prosthesis they do not replicate a ‘real-life’ scenario. Prosthetic components are not automatically replaced as soon as the guarantee period has expired.
Other authors (Narang and Jape 1982; Hoaglund et al. 1980) confirmed that prosthetic maintenance programmes are expensive and it is important to monitor by continuous analysis. Amongst other changes in the service provision, the wider use of modular prostheses has had a direct influence of the maintenance regime with fewer new prostheses but increased numbers of repairs and change of components. The present study depicts a more ‘real-life’ estimate for the current need for maintenance and for the provision of new prostheses. For individual amputees, their lifestyle and activity level would need to be factored. The study also questions the replacement and maintenance cycle previously recommended (Datta et al. 1999). At a time when the NHS is introducing reforms for financial flows (Department of Health [DoH]2002) by introduction of ‘payment by results’ and the NHS National Purchasing and Supply Agency (2006) is piloting the introduction of contract currency, tariffs will be required for annual care and maintenance of prostheses for the amputee population. The ‘real-life’ estimate of prosthetic use is likely to assist a more accurate estimate of costs to assist contract currencies.
Conclusion
Trans-femoral amputees in this study on an average needed a new prosthesis every 10 years while trans-tibial amputees needed a new prosthesis every 7 years. The product life cycle may be a key future parameter for the safe prescription of the duration of use of prosthesis. The trans-femoral amputee requires more change of prosthetic components whereas the trans-tibial traumatic amputee requires more repairs compared to the older vascular amputee. However, by calculating an average for a 10-year period one is able to arrive at an approximate estimation of the prosthetic needs of trans-femoral and trans-tibial amputees.
Footnotes
Acknowledgements
The authors would like to thank Richard Nieveen, Charlie Nyein, Linda Marks and Professor LynneTurner-Stokes for their constructive criticisms of the project especially during the pilot study stage, and Sue Walker for her assistance with searching the database for eligible patients. They are grateful to Deepak Datta whose paper in 1999 inspired us to carry out this study.