
Abstract
The objectives were to investigate the effect of three different interface types on consumer satisfaction and perceived problems among trans-tibial amputees in the Netherlands. A postal questionnaire (based on the Prosthesis Evaluation Questionnaire) was sent to 353 patients. Responders were classified in three groups of interface types: polyethylene foam (PEF) inserts, silicone liners (SIL), and polyurethane liners (PUL). Differences concerning satisfaction and problems between interface types were computed and adjusted for potential confounding by age, gender, reason for amputation and time since first prosthesis. A total of 220 patients responded (62%). Patients wearing liners reported a significantly poorer durability and higher maintenance time compared with patients using PEF inserts. Sum-scores for satisfaction or problems did not show any significant differences between groups. Analysis of individual items showed a significant difference only for satisfaction with sitting and with walking on uneven terrain in favour of PEF inserts. In contrast to most studies, interface type was included as a possible determinant of customer use, satisfaction, and perceived problems. The perceived differences between the three suspension types are to a large extent small and non-significant. The findings do not support liner prescription as a matter of course for all trans-tibial amputees. A careful analysis of patients' preferences should be made to determine the best course of action. Further studies, preferably prospective, need to be conducted to determine which systems are most comfortable and offer least complaints.
Keywords
Introduction
Until the early 1990s, most patients with a trans-tibial amputation were outfitted with a patellar tendon bearing (PTB) socket with a soft insert of polyethylene foam (PEF). Silicone and, from the mid-1990s onwards, polyurethane gel liners were introduced worldwide in an effort to reduce shear forces and improve the quality of the interface. Silicone and gel liners, due to their presumed ability to better control the artificial limb, are now often prescribed in favour of PEF inserts (Marks and Michael 2001). Liners supposedly add a measure of cushioning, comfort, and pressure dissipation (Cochrane et al. 2001; Datta et al. 1996; Fergason and Smith 1997; Hatfield and Morrison 2001), though several authors (Dasgupta et al. 1997; Datta et al. 1996; Dillingham et al. 2001; Lake and Supan 1997) have drawn attention to persistent stump problems with liners. Liners are now widely prescribed, although little empirical evidence exists to support their presumed surplus value, particularly from the point of view of users.
To gain insight into consumer satisfaction and perceived problems with three different interface types, we conducted a questionnaire survey among trans-tibial amputees in the Netherlands.
Methods
Subjects
A postal questionnaire was distributed among 353 outpatients with a trans-tibial amputation, who were approached either through the magazine of the Dutch Society for Lower-Limb Amputees (n = 196) or through the databases of two prosthetics service units (n = 157). All patients had received a new prosthesis between January 2000 and January 2002. There were no restrictions with respect to socket characteristics, age, gender, co-morbidity, date of amputation, or reason for amputation.
Three interface types were compared: PEF inserts, silicone liners, and polyurethane liners. The sockets accompanying the liners usually follow the total surface bearing principle but, depending on the experience of the prosthetist, may incorporate patellar tendon bearing characteristics (Fergason and Smith 1997).
Questionnaire
The questionnaire (see Appendix) included questions on demographic variables (age, gender, marital status, level of education), reason for amputation, and time since first prosthesis. In addition, several questions concerned use, maintenance, and durability of the prosthesis.
Overall satisfaction with the prosthesis was scored on a 0–10 point numerical rating scale. In addition, satisfaction was measured on a seven-item scale, using four response options ranging from ‘unsatisfied' (0) to ‘completely satisfied' (3). Items referred to the fit of the prosthesis, ability to don and doff, sit, walk, walk on uneven terrain, and walk up and down stairs, and appearance. Perceived problems with the prosthesis were assessed with a seven-item problem scale, consisting of items referring to sweating, wounds, skin irritation, unpleasant smells, unwanted sounds, pain, and swelling. The five response options ranged from ‘not at all bothered' (0) to ‘extremely bothered' (4). Selection of items for the satisfaction and problem scale was based on the Prosthesis Evaluation Questionnaire (Legro et al. 1998).
Analysis
Descriptive statistics were used to present population characteristics and results regarding use, maintenance time, and perceived durability of the prosthesis.
Sum-scores were calculated for both seven-item scales (0–21 points for satisfaction and 0–28 points for problems). A missing value on the satisfaction scale was replaced by the mean score of the subject's other items if a minimum of five of the seven items were completed (walking on uneven terrain and walking stairs were often missing simultaneously), and on the problems scale if a minimum of six of the seven items were completed. The internal consistency of both scales was satisfactory (Cronbach's α = 0.88 for satisfaction and 0.76 for problems).
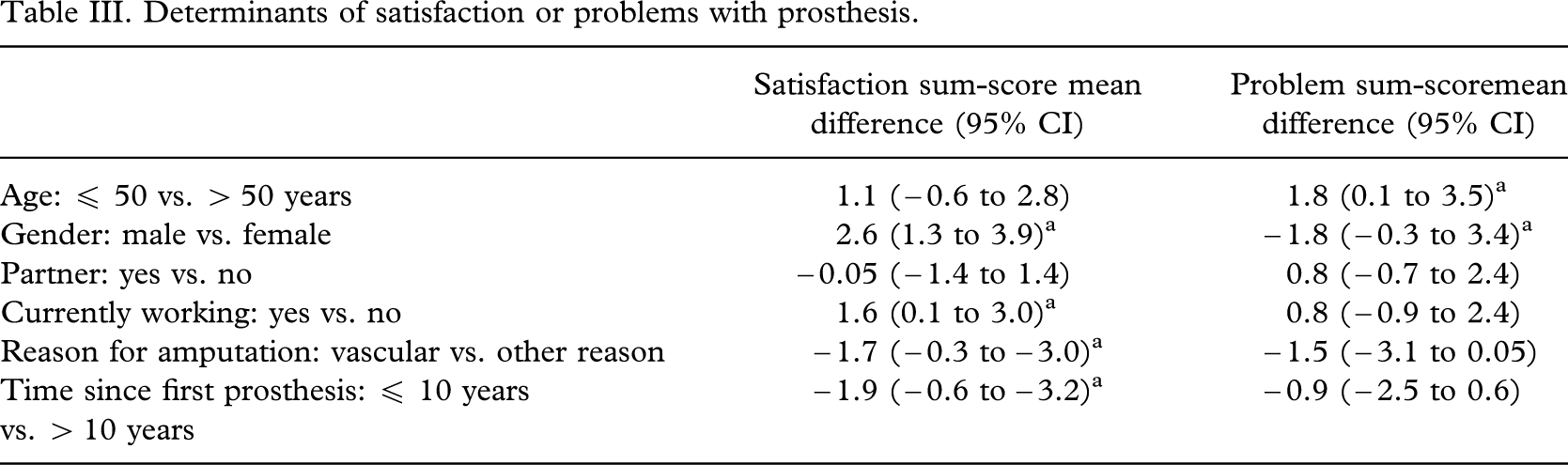
Mean differences in sum-scores on satisfaction and perceived problems were computed for subgroups with the following patient characteristics: age (≤ 50 or > 50 years), gender (male or female), partner (yes or no), currently working (yes or no), reason for amputation (vascular or other), and time since amputation (≤ 10 or > 10 years). These differences were presented along with 95% confidence limits.
Mean differences in sum-scores between PEF inserts and liner type (SIL or PUL) were computed and tested for statistical significance using one-way analysis of variance (ANOVA). These differences were accordingly adjusted for potential confounding by age, gender, reason for amputation, and time since first prosthesis using multivariate linear regression analyses.
Finally, satisfaction and perceived problems were analysed on the level of individual items, for which responses were dichotomized. A response was coded as ‘satisfied' if the participant had scored either ‘completely' (3) or ‘fairly satisfied' (2). For items concerning problems, a participant was denoted as ‘experiencing problems' if they had scored being ‘extremely' (4) or ‘very bothered' (3). Proportions were computed for the total population, and separately for PEF inserts and liner types (SIL and PUL). All analyses were carried out using SPSS 10.1.
Results
Study population (Table I)
Two hundred and twenty-seven (227) questionnaires were returned. Seven responses were too incomplete to utilize; therefore, 220 responses were available for analysis (62%). Most respondents (95%) were able to indicate what type of prosthesis they were using at the time of investigation. The majority of persons were male (60%), had an intermediate or higher education (74.2%), and had no current job (72.6%). Trauma was the most common (42.3%) reason for amputation. The most common prosthetic type was a socket with a SIL liner (43%). PEF inserts and PUL liners occurred to an equal extent (approximately 28% each).
Characteristics of the study population (n= 220).
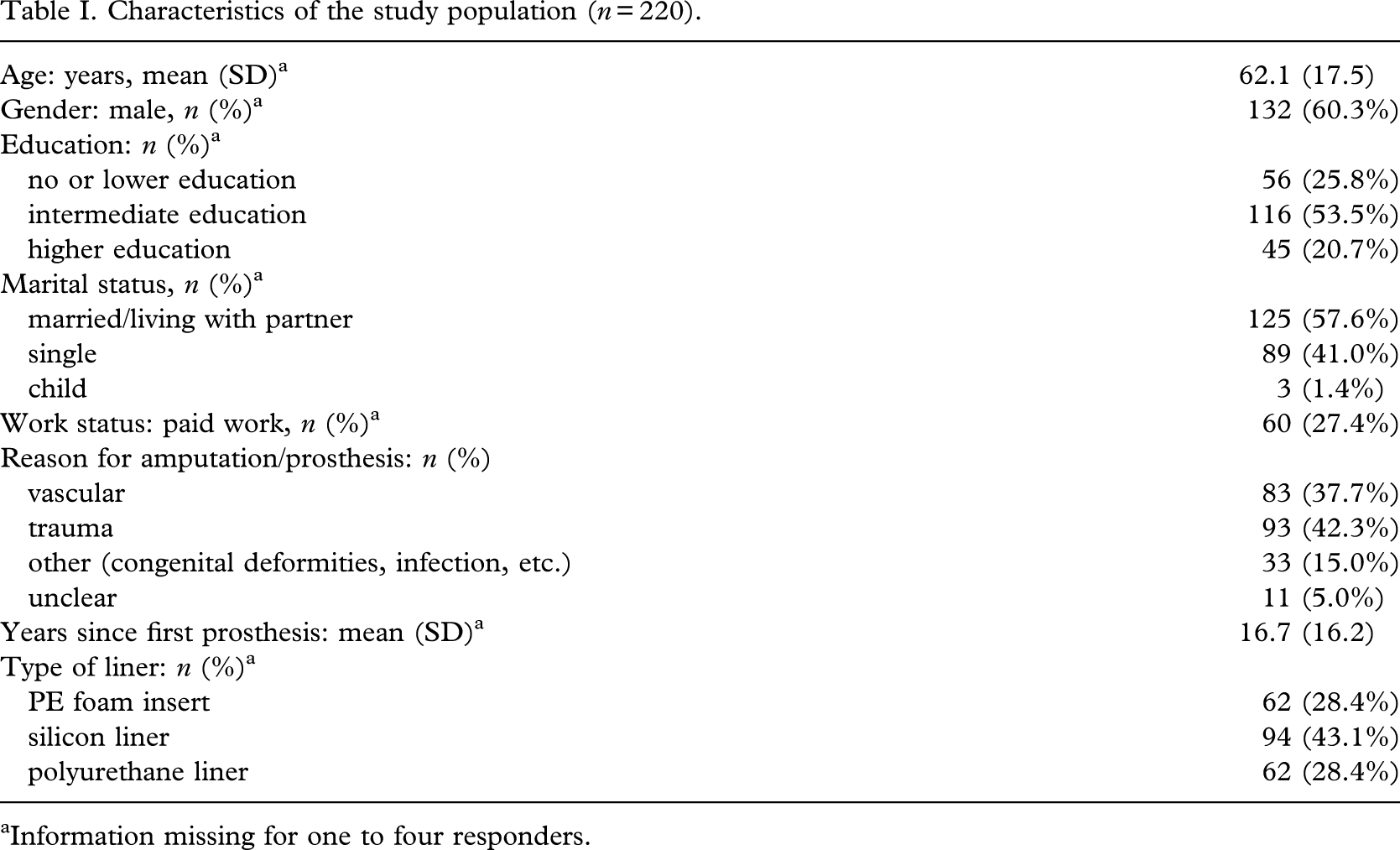
Information missing for one to four responders.
Use and satisfaction
The majority (93%) of persons used the prosthesis extensively (more than 6 h per day). Daily wearing time was not significantly different between groups. Daily maintenance time was significantly longer for both liners compared with PEF. Durability was considered to be significantly poorer for PUL compared with SIL and PEF.
The mean overall satisfaction on a 0–10 point numerical rating scale was 7.0, ranging from 6.9 for PUL to 7.3 for PEF. Differences in sum-scores on the satisfaction scale between inserts and liner types were also small and not significant. Adjustment for potential confounding by age, gender, reason for amputation, and time since first prosthesis further reduced these differences. Male gender, paid work, non-vascular reasons for amputation, and longer time since first prosthesis were associated with significantly higher satisfaction sum-scores, although the differences were small (> 3 points on a scale of 0–21, Table III). Analysis of individual satisfaction items showed a significant difference (P = 0.02) in favour of PEF for walking on uneven terrain and sitting. Differences regarding fit of prosthesis, donning and doffing, walking, stair-climbing, and perception of looks were non-significant (Table II).
Problems with/complaints about prosthesis
Younger age and female gender were associated with a higher problem sum-score, although the differences were very small (< 2 points on a scale from 0–28) and not statistically significant (Table III).
Silicone liners and PU liners were associated with a lower problem sum-score compared with PE foam inserts (Table IV). Mean differences (unadjusted and adjusted for confounding) were very small (< 1 point) and not statistically significant. None of the individual items showed any significant differences between the three groups. The only subitem approaching significance was sweating, which was a somewhat more common problem in users of PEF inserts (36%) compared with SIL and PUL (21% and 24%, respectively).
Discussion
The authors investigated interface type as a possible determinant of customer use and satisfaction. Durability of PUL liners was considered significantly poorer and maintenance time significantly longer with both types of liners, compared with PEF. The authors did not register significant differences between interface types with respect to perceived problems. The only sub-item approaching significance (P = 0.08) was sweating, which was reported more frequently in users of PEF inserts (36%) compared with users of SIL and PUL (21% and 24%, respectively). Excessive sweating is often ascribed to liners but apparently is very common with a PEF insert, too.
Apparently, liners are not always perceived as ‘better' by users, yet this appears to be the general trend in the literature. Views from a UK questionnaire survey reflecting personal experiences among doctors and prosthetists (McCurdie et al. 1997) indicated a clear preference for liners. A recent Dutch study (van der Linde et al. 2004) showed that rehabilitation professionals have favoured a gel liner in the past two years, despite a lack of formal evidence or the presence of a standard for the implementation of new prosthetic components. Hatfield and Morrison (2001) reported improved comfort in patients using polyurethane liners, although nine patients out of 56 chose to discontinue PUL use due to reported worse comfort. Results are difficult to interpret, since the sample encompasses all (primarily trauma-related) amputation levels, and comfort was not measured formally (for example using a visual analogue scale). Moreover, since all patients had a troublesome prosthetic history, the results cannot be generalized to any extent. A recent study (Astrom and Stenstrom 2004) reported that the polyurethane concept provided better socket comfort compared with the conventional system. It should be noted that 80% of the selected patients had stump problems, and for 70% pain was a limiting factor in walking distance, which makes some degree of selection bias likely. In addition, almost one-third of patients were lost to follow-up for various reasons.
Use and satisfaction with prosthesis.
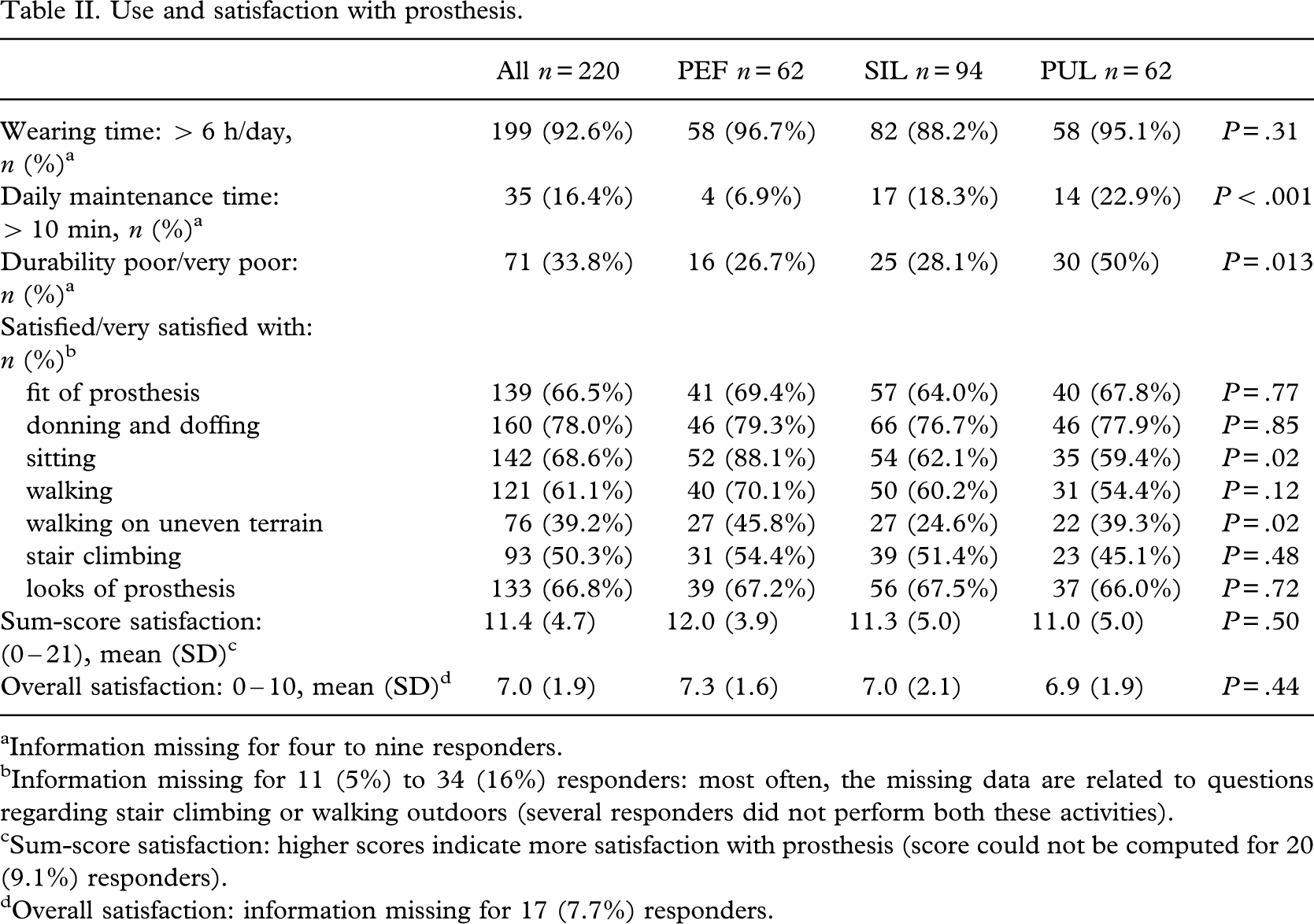
Information missing for four to nine responders.
Information missing for 11 (5%) to 34 (16%) responders: most often, the missing data are related to questions
Problems with wounds, skin irritations, or pains were reported by 14.4% of the patients compared with 43% (Dillingham et al. 2001), 28% (Datta et al. 1996), and 38% (Dasgupta et al. 1997) in other studies. Hachisuka et al. (1998) found that ‘donning and doffing the socket', ‘perspiration', ‘knee flexion and extension', ‘odour from the socket', and ‘staining of the socket' were regarded as good by fewer than 40% of the subjects. Though overall satisfaction with the prosthesis was not significantly different for the three groups, sitting and walking on uneven terrain scored significantly poorer among liner users. A patient accustomed to sitting most of the day may prefer a PTB socket of polyethylene foam, since there is no bunching or wrinkling of a liner at the popliteal fossa. With respect to walking on uneven terrain, one may postulate that a relatively ‘hard' interface such as the PEF offers more direct feedback and therefore more stability in situations requiring optimum security. Fellow researchers (Astrom and Stenstrom 2004; Datta et al. 1996; Dasgupta et al. 1997) did not find significantly improved mobility with liner users either. It is therefore somewhat surprising that most authors are clearly in favour of prostheses utilizing liners. A possible explanation is that clinicians are naturally susceptible to ‘technology driven' developments and tend to use them swiftly in daily practice.
Determinants of satisfaction or problems with prosthesis.
Problems with/complaints about prosthesis.
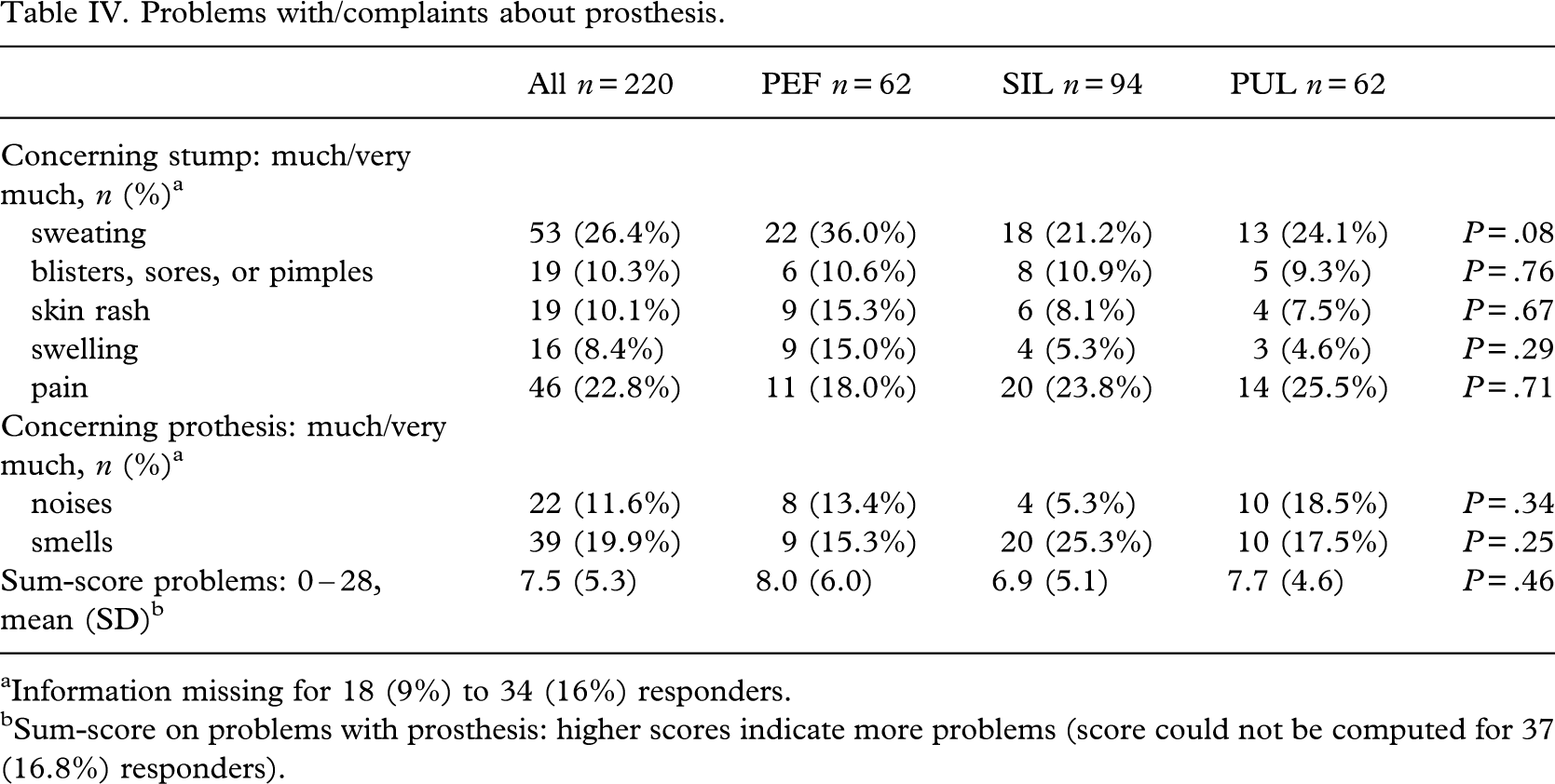
Information missing for 18 (9%) to 34 (16%) responders.
Sum-score on problems with prosthesis: higher scores indicate more problems (score could not be computed for 37
Some limitations of this study that are inherent to questionnaire surveys (Sitzia 1999) should be pointed out. The results of the survey may have been influenced by the patients' expectations and by perceived self-interest or gratitude. Furthermore, response rate was 62%. This may be considered to be satisfactory for a questionnaire survey, but non-response bias cannot be ruled out. Finally, the authors were not able to record the characteristics of non-responders and therefore do not know whether our sample is representative of the trans-tibial amputee population in general.
Conclusion
Evidence to support the (presumed) surplus value of liners is scant. The study's findings show that, with respect to use, satisfaction, and perceived problems, patients using different interface types do not report significant differences to a large extent. The authors therefore believe that liners should not be prescribed as a matter of course for all prosthetic candidates. Some inherent weaknesses of liners first remain to be solved. In developing countries in particular, with high durability and low cost, a prerequisite, PTB or PTB-related prostheses might continue to be the first choice. Most of the literature originates from industrialized nations, which may explain any bias towards technological advances. Further studies, preferably prospective, need to be conducted to determine which systems are most comfortable and offer least complaints.
Footnotes
Appendix: Questionnaire
This survey asks for your views about your current prosthesis. In particular, we are interested in your views on the use and comfort of the so-called ‘interface'. The most common forms of interface are the liners and the hard-foam covers. A liner is a thick synthetic sock that is usually applied in more or less the same fashion as a condom. Foam covers are lightweight, usually custom made by your prosthetist after applying cast. Foam covers are made of less pliable material and retain their form when withdrawn from the stump. If in doubt what kind of interface material you have, please consult the attached colour photographs or, if still in doubt, your doctor or prosthetist.
A. General characteristics. Check the answer that best describes your situation or fill in the blank accordingly.
B. Use and satisfaction. Please tick in each of the following columns the most appropriate answer, based on your experiences of the past 4 weeks:.
How satisfied are you with the following?
C. Prosthesis related problems/complaints. Please tick in each of the following columns the most appropriate answer.
How bothered were you with any of the following problems during the last 4 weeks?