
Abstract
Standing up is an important and common daily activity. It is essential for independence and a prerequisite for walking. Many elderly and many subjects with impairments have problems with transition from sitting to standing. The aim of the present study was to determine whether there was any difference between the characteristics of standing up in trans-femoral amputees and healthy subjects. Five young trans-femoral amputees and five healthy subjects were included in the study. They were asked to stand up. The body motion was recorded using an Optotrak contactless optical system. The force and moment vectors exerted on the seat were recorded by a JR3 six-axis robot wrist sensor. The force under the feet was recorded by two AMTI force plates. The trans-femoral amputees were found to stand up more slowly than the healthy subjects. The angles of the hip, knee, and ankle joints on the amputated side were different from the angles on the healthy side or in the healthy subjects. There was also a great difference in loading between the healthy and the prosthetic foot. It can be concluded that there are differences in standing up between the trans-femoral amputees and the healthy subjects. These differences may indicate a reason for problems many elderly trans-femoral amputees face when standing up.
Introduction
Standing up is an important and common daily activity often done automatically by healthy subjects (Doorenbosch et al. 1994). It is essential for independence and a prerequisite to movements in an upright posture. In spite of the fact that standing up is an action which involves the whole body, the motions of the hip, knee, and ankle joints are most important. Biomechanically, standing up can be more demanding than other activities of daily living because it requires more leg strength and greater ranges of joint motion than walking or stair climbing (Hughes and Schenkman 1996). In the United States, it is a problem for more than two million persons older than 64 years (Lundin et al. 1995). Inability to stand up not only limits patients but also presents a greater burden to those who must care for them.
Studies on standing up can be divided into three main categories. The first category tries to determine body kinematics (Fleckenstein et al. 1988; Kotake et al. 1993; Yu et al. 2000) and kinetics (Bajd et al. 1982; Burdett et al. 1985; Ellis et al. 1984; Kralj et al. 1990; Németh et al. 1984; Pai and Rogers 1991; Rodosky et al. 1989), myoelectric activities (Doorenbosch et al. 1994; Munton et al. 1984; Roebroeck et al. 1994; Stevens et al. 1989), symmetry (Lundin et al. 1995), and normative data (Kralj et al. 1990; Roebroeck et al. 1994), and studies biomechanical models (Bajd et al. 1982; Fleckenstein et al. 1988; Németh et al. 1984; Pai and Rogers 1991; Rodosky et al. 1989). The second evaluates the effects of different parameters such as chair height (Burdett et al. 1985; Ellis et al. 1984; Rodosky et al. 1989), the use of armrests (Arborelius et al. 1992; Seedhom and Terayama 1976), the amount of knee flexion (Fleckenstein et al. 1988), the variation in speed of standing up (Pai and Rogers 1991), the influence of age (Hughes et al. 1994; Ikeda et al. 1991; Millington et al. 1992; Schultz et al. 1992) and different strategies of standing up (Doorenbosch et al. 1994). The third group studies the standing up of subjects with different impairments, such as spinal cord injury (Bajd et al. 1982; Kagava et al. 1995; Kamnik et al. 1999), arthritis (Munton et al. 1984), hemiparesis (Hesse et al. 1994; Yoshida et al. 1983), certain neuromuscular diseases (Butler et al. 1991), functional impairments (Hughes and Schenkman 1996) and low-back pain (Coghlin and McFadyen 1994). No basic studies found on standing up of amputees have been found. However, standing up has been used as a functional test to assess the functional ability of lower-limb amputees (Burger and Marinček 2001).
The main aim of rehabilitation of lower-limb amputees is to enable them to walk again and regain the functional level they had had before the amputation. Before subjects start to walk, they have to stand up. Trans-femoral amputees have lost two main joints of the lower limb—the ankle and the knee. Also, many muscles around the hip joint have been released and may not be fixed to the bone. Prosthetic joints are completely passive, and when performing activities, the subjects have to control them with the remaining muscles. It has been noted from clinical observations that lower-limb amputees at the beginning of their rehabilitation, and some even later, frequently have more problems standing up than walking.
The aim of the present study was to determine whether there was any difference between the characteristics of standing up in trans-femoral amputees and healthy subjects in order to develop later an appropriate training programme and improve their ability to stand up.
Subjects
Five male trans-femoral amputees and five healthy subjects constituted the study group. The authors decided to choose trans-femoral amputees who were young and fit, and should be able to stand up several times without the help of their upper limbs. All of them had had their prosthesis for at least 1 year and walked with it without any problems.
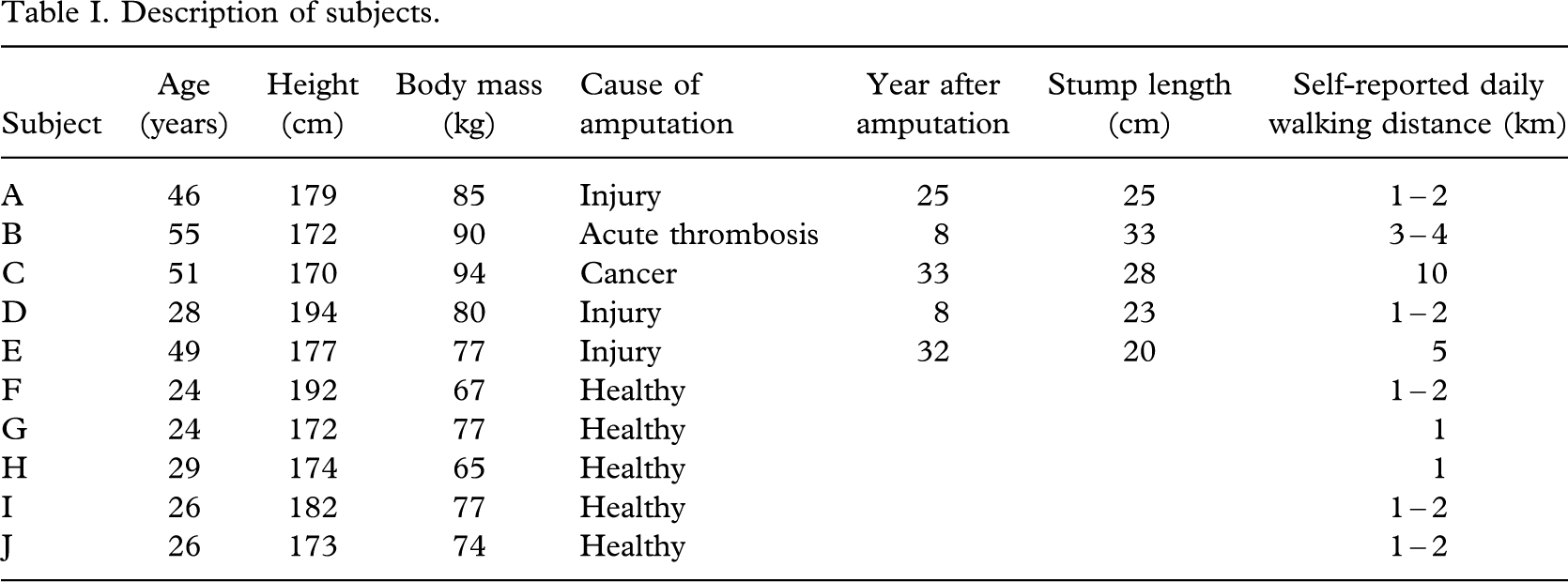
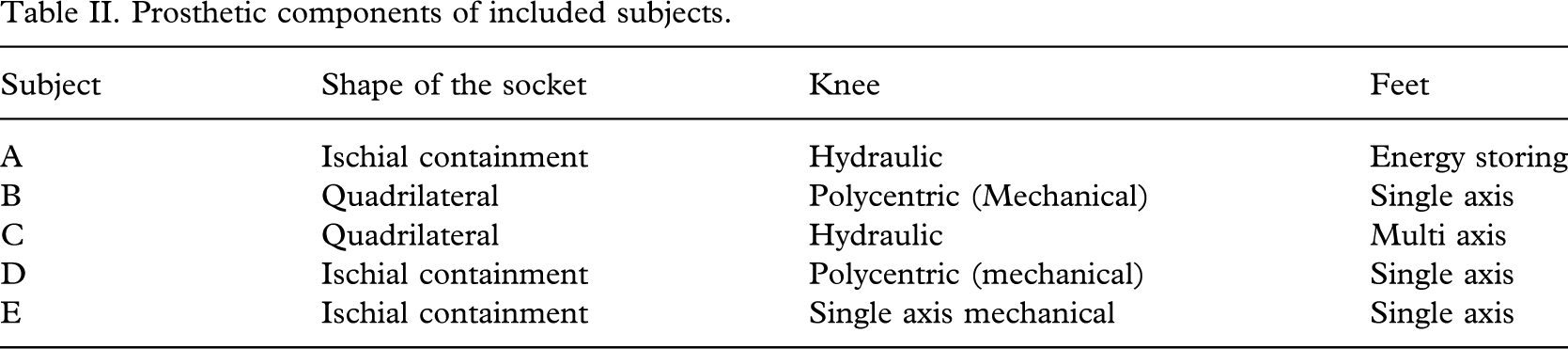
The trans-femoral amputees were 28 – 51 years old. All had an amputation several years before the measurement (8 – 33 years). All were good prosthetic walkers, and three actively played sitting volleyball. Three had an amputation due to an injury, one due to cancer and one due to acute thrombosis (Table I). Prosthetic characteristics are presented in Table II.
Description of subjects.
Prosthetic components of included subjects.
The healthy subjects were 24–29 years old (Table I). None had any history of severe lower-limb trauma or neurological disease. They were all very active: two run regularly up to 2 km, one cycles, and one roller-skates.
Prior to testing, all subjects were informed of the protocol and signed a consent form.
Methods
The body motion was recorded using an Optotrak contactless optical system (Optotrack, Northern Digital Inc., Waterloo, Canada). Infrared markers were attached over the approximate centres of the ankle, knee, hip, and shoulder joints in the sagittal plane. The subjects sat on a commercially available bicycle seat, the height of which was adjusted to 90% of the distance from the floor to the centre of the subject's knee joint. Under the seat was a JR3 six-axis robot wrist sensor (JR3, Inc., Woodland, CA) which measured the force and moment vectors exerted on the seat. The feet were placed on two AMTI force plates (AMTI Inc., Newton, MA).
The subjects had their arms crossed over the chest and found a comfortable position of the seat and the feet. They were allowed to find the most comfortable position for the feet on the two plates. They were asked to stand up as naturally as possible and at their most comfortable speed. Each subject had to do 10 stand-ups. The intervals between the trials were 1–2 min long, giving the subjects time to rest.
The following measurements were performed:
the time to the seat-off (the time from the initiation of the rising manoeuvre to the moment when there was no force measured under the seat); the time from the seat-off to standing (from the time there was no force on the seat to the time the subjects were standing straight and still); the whole time to stand up (from initation of rising to straight and still standing); the angles of the hip, knee, and ankle joints on both sides, and the trunk angle in all three planes (throughout the testing); the force on the seat and both forceplates (throughout the testing).
The signals from the infrared markers and all three force sensors were collected using a sampling rate of 50 Hz. The signals were filtered using the fourth-order Butterworth filter with a 5 Hz cutoff frequency. The statistical comparisons were made using t-tests.
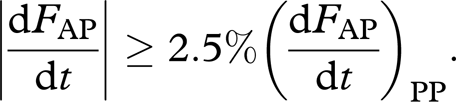
The characteristic events during rising were detected from the time courses of the measured reaction forces (Kralj et al. 1990). The beginning of the standing-up manoeuvre occurred when the derivative of the sum of all anterior–posterior components (F AP) of the reaction forces rose over 2.5% of the peak-to-peak value:
Since, in contrast to Kralj et al. (1990), the seat reaction force was also measured, it was used to determine the seat-off event. The seat-off instant was detected, when the vertical component of the seat force (F S) decreased below 5% of its maximal value:

The occurrence of quiet standing was defined as the instant at which the sum of all vertical components of the reaction forces (F V) settled within 1% of the body gravitational force (F G):

The joint angles were calculated from the trajectories of the ankle, knee, hip, and shoulder markers. A longitudinal axis of the trunk was defined with the help of two points that were located half the distance between both shoulder and hip markers. The trunk angles in the sagittal, transversal, and frontal plane were calculated by projecting the trunk axis on the corresponding planes.
Results
The trans-femoral amputees took more time to stand up than the healthy subjects due to a longer time from the seat-off to standing (Table III).
Times from the beginning of standing up to the seat-off, from the seat-off to standing, and the total time to stand up (average for 10 trials)a.
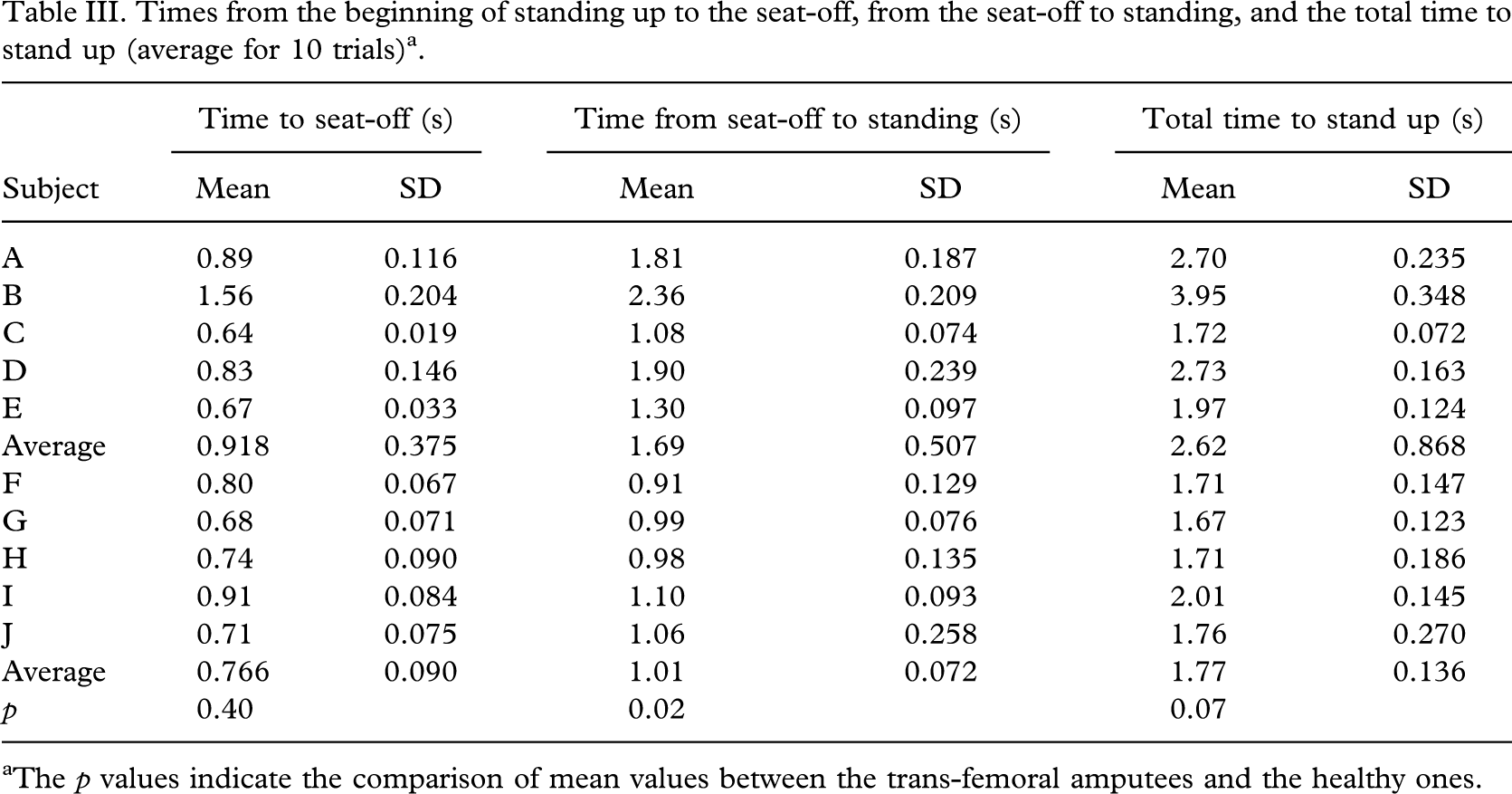
The p values indicate the comparison of mean values between the trans-femoral amputees and the healthy ones.
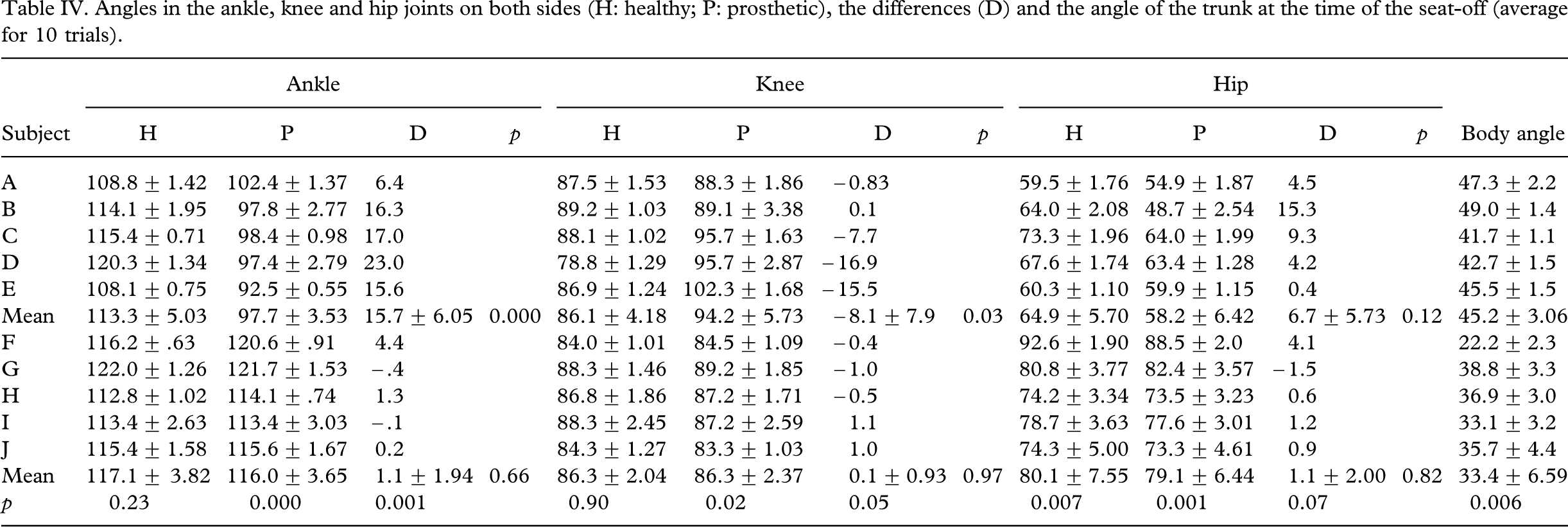
At the time of the seat-off, trans-femoral amputees had both hips and the prosthetic knee more extended than the healthy subjects. The prosthetic ankle was less dorsiflexed (Table IV). All trans-femoral amputees except one had a straighter hip on the amputated side, and three out of five had a more extended prosthetic knee. The angle in the ankle joint on the prosthesis was smaller (Table IV,Figure 1). Their standing up was not as symmetrical as in the healthy subjects (Figure 1).
Angles in the ankle, knee and hip joints on both sides (H: healthy; P: prosthetic), the differences (D) and the angle of the trunk at the time of the seat-off (average for 10 trials).
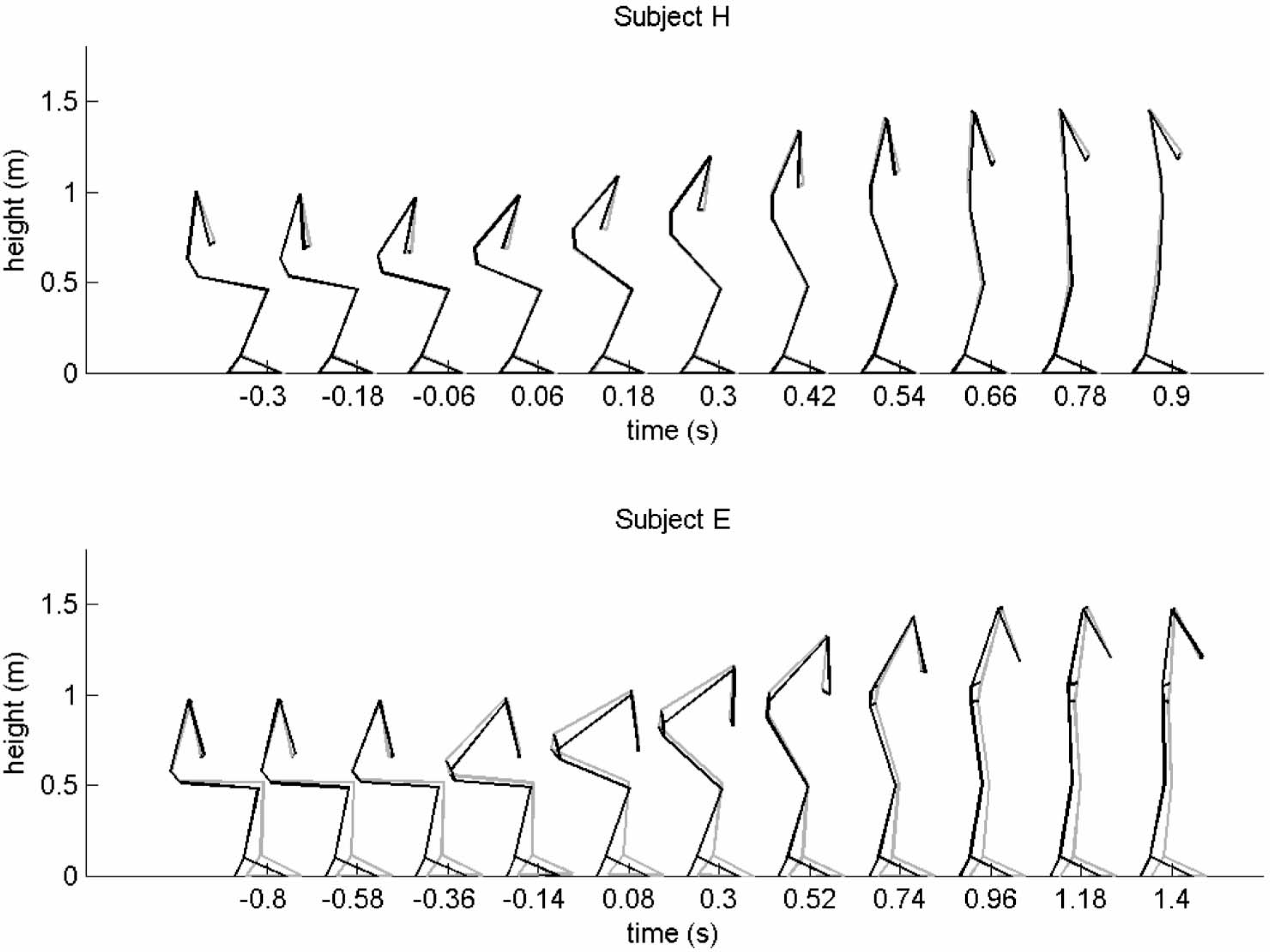
Standing up of a healthy (H) subject and a subject after left trans-femoral amputation (E) in the sagittal plane. While standing up of the healthy subject was symmetrical, the subject after left trans-femoral amputation positioned the prosthesis more forwards than the healthy leg and rotated the trunk backwards to the left side (left: grey; right: black line).
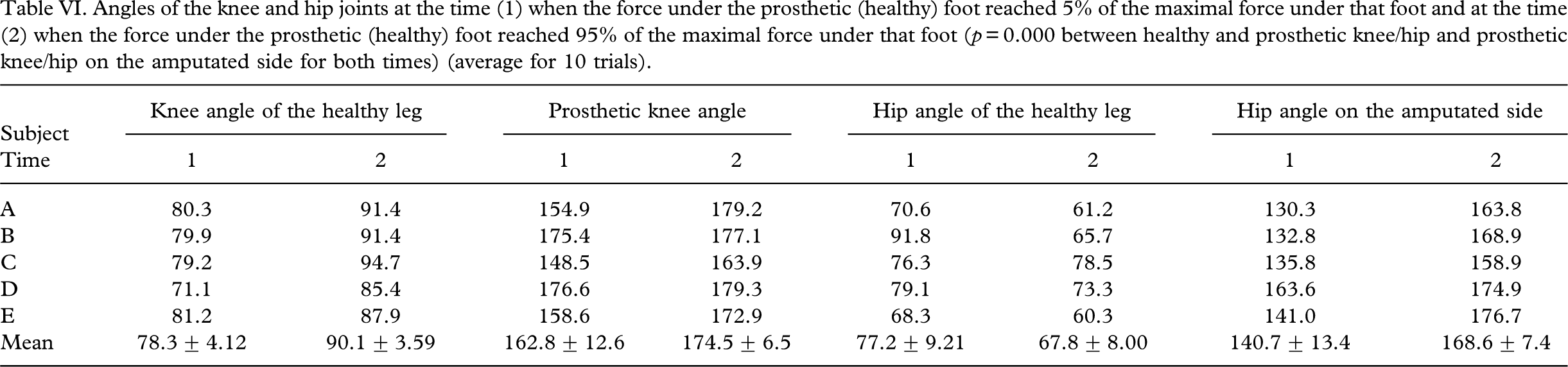
The trans-femoral amputees did not put any load on the prosthesis until they were almost standing up (Figure 2). In all healthy subjects except one, the maximal difference in force between both feet was less than 10% of the maximal force under the feet, while in all trans-femoral amputees, it exceeded 70% of the maximal force under the healthy foot (Table V). There was significant difference between the knee and the hip angles at the time they put 5% or 95% of the maximal load on the prosthetic foot or on the healthy foot (Table VI).
Maximal difference in force under both feet for the healthy subjects and the subjects after trans–femoral amputation in percentage of body weight (p=0.001) (average for 10 trials)a.

Positive numbers indicate that the right leg was bearing more body weight than the left leg.
Angles of the knee and hip joints at the time (1) when the force under the prosthetic (healthy) foot reached 5% of the maximal force under that foot and at the time (2) when the force under the prosthetic (healthy) foot reached 95% of the maximal force under that foot (p=0.000 between healthy and prosthetic knee/hip and prosthetic knee/hip on the amputated side for both times) (average for 10 trials).
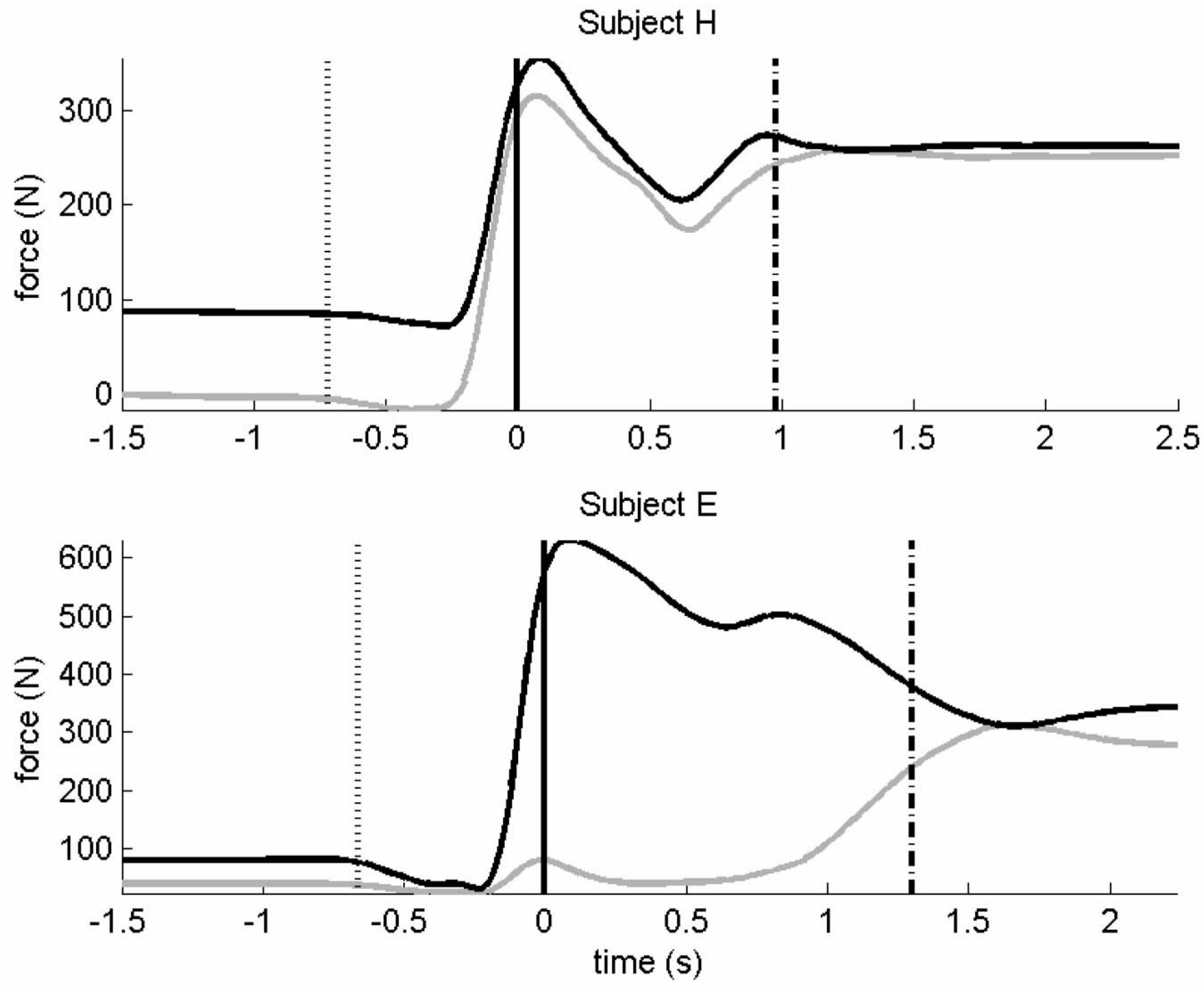
Loading of the left (grey line) and the right (black line) forceplate during standing up of a healthy (H) subject and a subject after left trans-femoral amputation (E). The first vertical line marks the beginning of the standing-up manoeuvre, the second the time of the seat-off, and the last the occurrence of the quiet standing as defined in the methods.
The trans-femoral amputees leaned more forwards at the time of the seat-off (Table IV); later, they leaned slightly more forwards and bent more to the healthy side, and the inclination of the pelvis was greater (Table VII).
Maximal trunk angles (degrees) in all three planes while standing up (average for 10 trials).
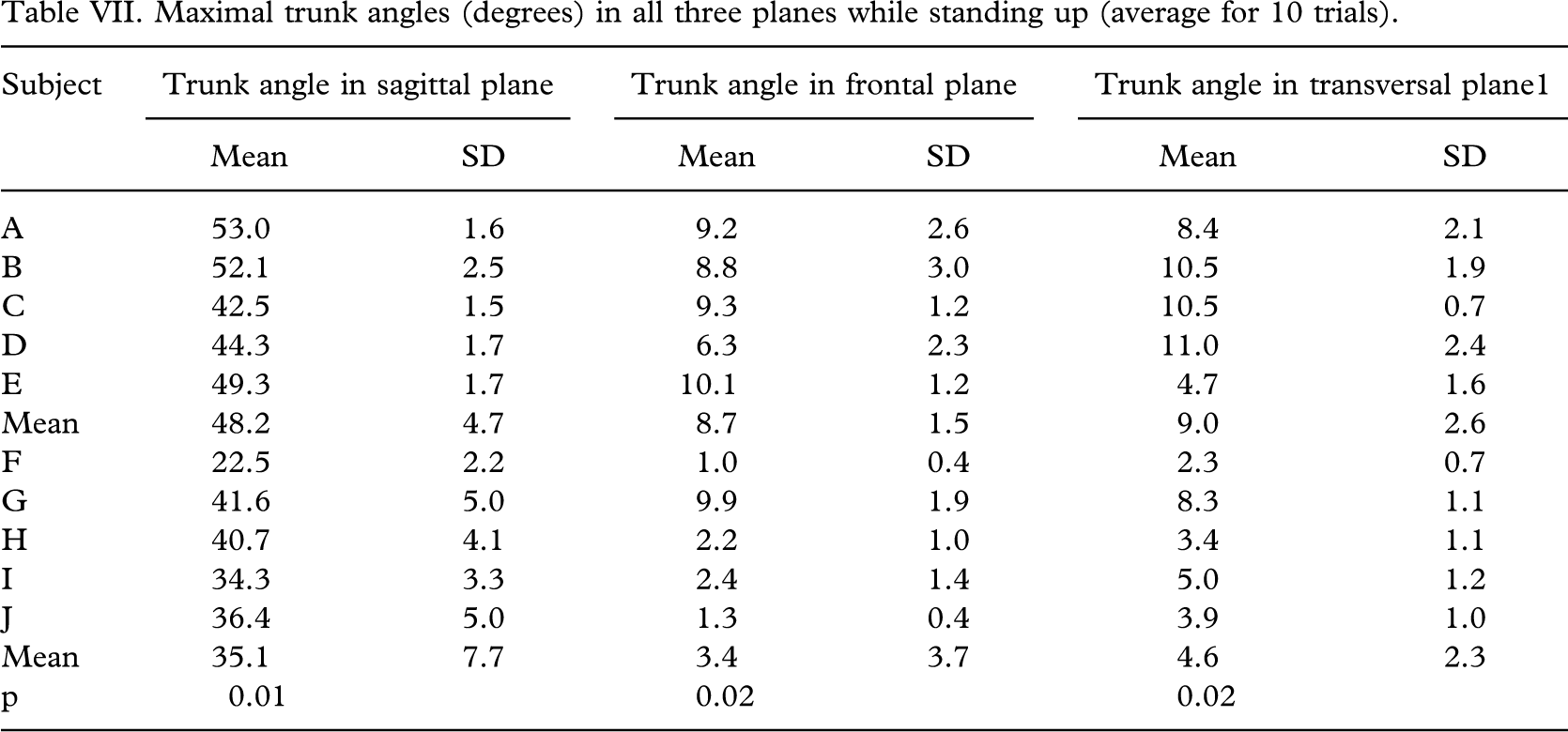
Figure 3 shows the moments of healthy subjects and amputees in the hip, knee, and ankle joints. None of the prosthetic knees exerted any moment while standing up.
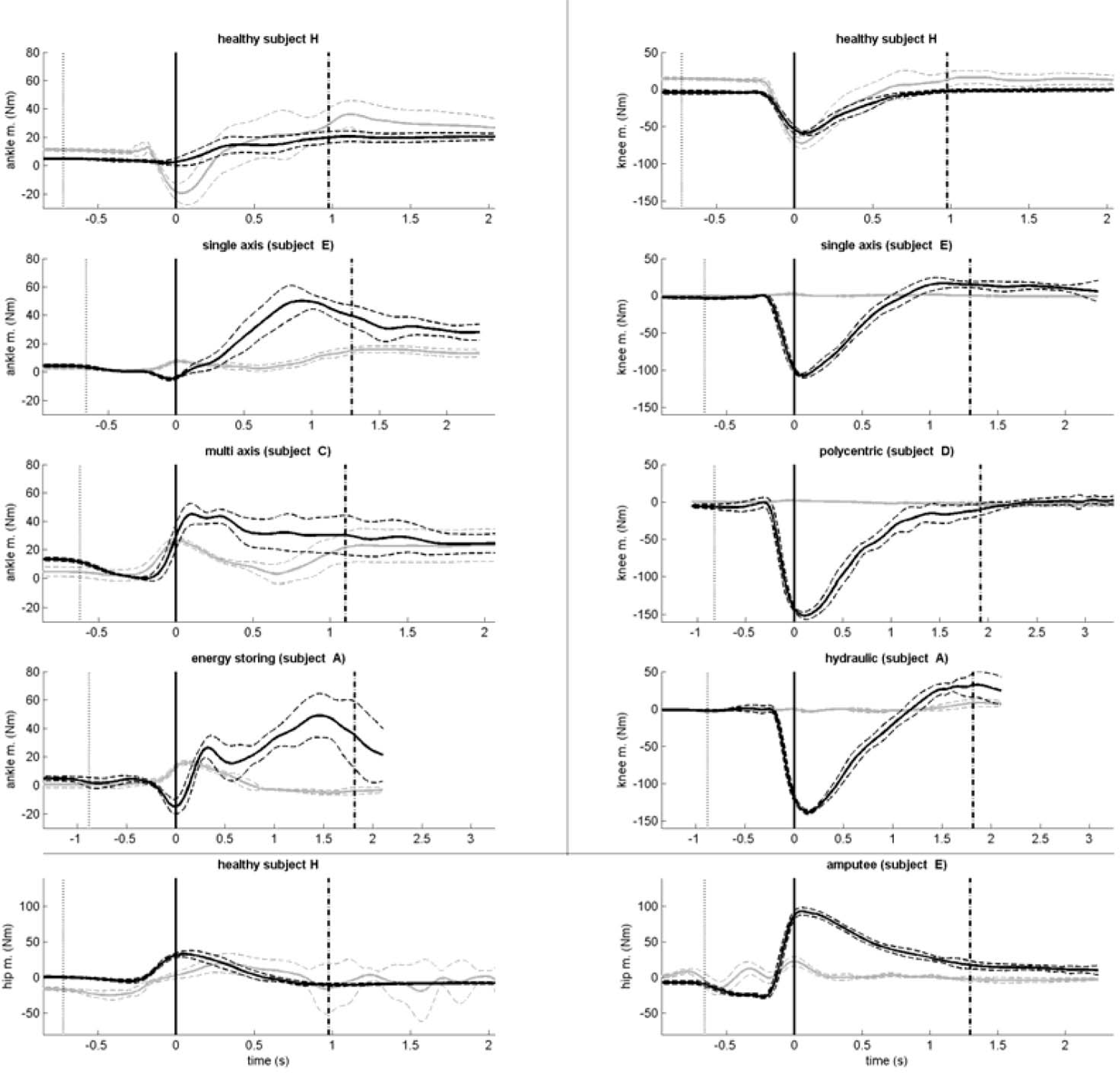
Moments in hip, knee, and ankle joints of healthy subjects and amputees.
Discussion
Several studies have been carried out in recent years on the transition from sitting to standing. The results of those studies are difficult to compare because their protocols, the initial positions of the subjects, and the presentation of the results differ enormously. Most studies did not allow the subjects to use upper limbs (as was the case in the present study); however, some used backrests (Lundin et al. 1995; Yoshida et al. 1983). In addition, the initial knee angle varied from 75° to 110°, of flexion and the foot positioning was different in almost every study. The present study only defined the seat height and the position of the upper limbs; otherwise, the subjects were allowed to take their most comfortable position.
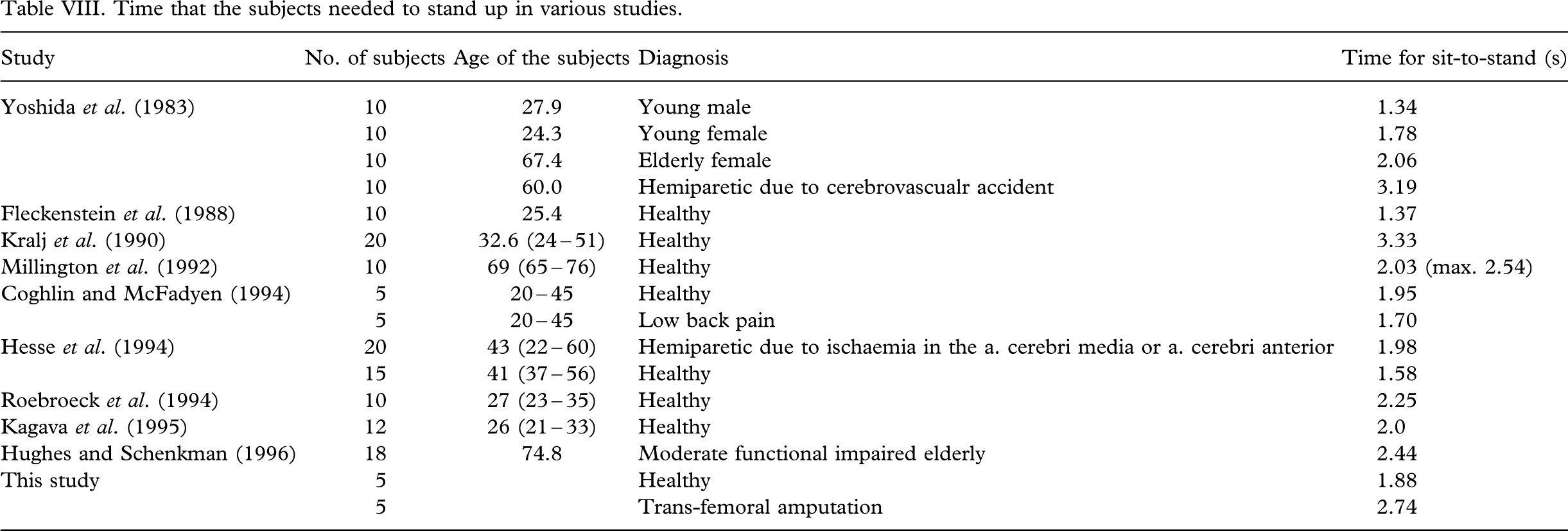
The time that the subjects needed for standing up differed among the studies, and the ranges of normal were very wide (Table VIII). The control group in the present study needed a similar time as the healthy subjects in most above-mentioned studies (Table VIII). In all studies, the subjects with impairments, with the exception of the subjects with low-back pain (Coghlin and McFadyen 1994), needed a longer time to stand up. The trans-femoral amputees in the present study needed the second-longest time among all subjects, but still less than the healthy subjects in Kralj's study (Kralj et al. 1990), although they were slightly older. None of the subjects in the present study was over 60 years, but each took more time to stand up than the elderly subjects (Hughes and Schenkman 1996; Millington et al. 1992; Yoshida et al. 1983). They did not need a significantly longer time from rising to the seat-off, but they did need significantly longer time from the seat-off to standing (Table III). Kotake et al. (1993) found in healthy subjects that the longer it took them to rise, the shorter the time to the seat-off and the longer the time from the seat-off to the maximum flexion of the hip joints, while all other times did not change significantly.
Time that the subjects needed to stand up in various studies.
Most studies assumed that there was symmetry in both lower limbs while standing up. Lundin et al. (1995) found that even in the healthy subjects, there were differences in the peak joint moments between both lower limbs during standing up. In the present study, all healthy subjects except one did not have a significant difference in ankle, knee, and hip joint angles at the time of the seat-off (Table IV) or in the force under both feet (Table V), whereas the differences in these values in trans-femoral amputees were much greater.
Standing up requires surprisingly large moments, particularly at the hip and knee (Fleckenstein et al. 1988; Roebroeck et al. 1994). The trans-femoral amputees cannot and do not exert the knee moments on the side of amputation (Figure 3). Since none of the subjects in the present study had a myodesis of transected muscles acting around the hip, they might have had problems in exerting a great enough moment at the hip. Therefore, they had to find a compensatory mechanism, either mechanical (e.g. higher chair) or physical (e.g. different strategy of rising). This can be achieved by a different position of the body (Doorenbosch et al. 1994) or by a different speed of standing up (Hughes et al. 1994). Full flexion of the trunk does not affect the motion of the knee and ankle, but does decrease the knee and the hip extension moments (Doorenbosch et al. 1994). It also increases the activity of the hip extensors, especially of the gluteus maximus muscle and the hamstrings, but in the healthy, there is also a co-contraction of the rectus femoris and vastus medialis (Doorenbosch et al. 1994; Roebroeck et al. 1994). The last two muscles are cut in trans-femoral amputees. Only a part of the gluteus maximus muscle, which inserts on the greater trochanter, is not cut and can give at least some of the required force. These findings also show that myodesis of muscles, specially biarticular muscles, in trans-femoral amputees is important for walking but also may be even more important for standing up, the prerequisite for walking.
Hughes et al. (1994) described two strategies for standing up, the momentum transfer and the stabilization. In the momentum transfer, a rapid forward motion of the trunk helps knee musculature to extend the knees. This seems an important strategy for trans-femoral amputees who do not have myodesed knee extensors. In the stabilization transfer, the subject tries to shorten or eliminate the unstable phase by repositioning the centre of the mass and base of support by sliding the buttocks forward, flexing at the hips and placing the feet back. Also, the stabilization is important for trans-femoral amputees who have to prevent the passive prosthetic knee from flexing and collapsing during standing up. The present study has demonstrated that the trans-femoral amputees used both strategies: they flexed the trunk significantly more than the healthy subjects at the time of the seat-off, and they also flexed their hips to a higher extent, but they did not put the feet more backwards (Table IV). They needed a slightly, but not significantly, longer time from the beginning to the seat-off (Table III). By using both strategies, they compensated for the lack of knee extensors, which are the most active at the time of the seat-off (Roebroeck et al. 1994). They also had to care about the stability of the prosthetic knee. This is probably the most important factor influencing the fact that they did not put more than 5% of the maximum weight on the prosthesis until the knee was almost completely extended (Table VI). The differences in the prosthetic knee angle at the time of the 95% loading were small among the five measured subjects, and the influence of the knee type did not seem to matter. However, to make any conclusions about the latter, a much larger number of subjects with different knee types will need to be measured. It will also be important to measure the EMG activity of different muscles during standing up. Stevens et al. (1989) found that a preferred initial leg posture results in smaller magnitudes of head movement and ground reaction forces, decreased activity in trapezius and erector spinae, but increased activity of quadriceps and hamstrings.
The results of the present study were limited by the small number of subjects and the difference in age between the healthy subjects and trans-femoral amputees. Also, the EMG activity, which can provide important additional information, was not measured. However, in spite of those limitations, it can be concluded that standing up of trans-femoral amputees was not symmetrical; they started to load the prosthesis when the knee was almost completely extended; and their standing up was much slower. All this may indicate that trans-femoral amputees can have severe problems when standing up. Elderly subjects who have undergone trans-femoral amputation due to vascular problems and have problems with walking can be expected to have even more problems with standing up than the subjects in the present study. The inability to stand up not only severely limits the performance of daily activities but also may impose a great burden on carers. Prosthetic engineers may have to put more effort into the development of a prosthetic knee that will help trans-femoral amputees to stand up more easily.