
Abstract
Background:
Sit-to-stand movement is an essential function for participation in many activities of daily living. Although this movement is one of the most important functional tasks, there is limited research investigating strategies of sit-to-stand movement in transtibial amputees.
Objectives:
To examine movement strategies of the sit-to-stand task in persons with transtibial amputation and healthy non-amputated individuals.
Study design:
Cross-sectional study.
Methods:
A total of 12 male unilateral transtibial amputees and 19 healthy male subjects participated in this study. Sit-to-stand movement was evaluated in terms of weight transfer time, weight-bearing symmetry, sway velocity, and rising index by using Balance Master System.
Results:
Participants in both groups exhibited similar weight-bearing transfer time (p > 0.05). Transtibial amputees demonstrated significantly greater weight-bearing asymmetry, higher sway velocity, and lower rising index than healthy subjects during the sit-to-stand transfer movement (p < 0.05).
Conclusions:
Transtibial amputees were unable to use the same movement strategies during a sit-to-stand task as healthy individuals; therefore, they had to develop new strategies to perform this task.
Clinical relevance
Little is known about the altered movement strategies during sit-to-stand task in transtibial amputees. The results of the study might provide some new insight into the motor components of the sit-to-stand movement in persons with transtibial amputation for both clinicians and researchers.
Background
Going from a seated to a standing position, in another words sit to stand (STS), is an essential movement for participation in many activities of daily living such as ambulation. 1 Since healthy individuals perform 60 STS movements in a daily routine, 2 it is considered to be a key determinant of functional fitness and independence. 3
STS has been described as the most demanding functional task among all daily activities.3,4 Moving from a sitting to a standing position requires sufficient muscle force to vertically accelerate the body’s mass against the pull of gravity, 5 and postural control must be maintained from the time of the initiation of movement to the end of the task. 6 Therefore, the ability to perform this task successfully depends on enough muscle strength and sufficient postural balance control.7,8
Considering the musculoskeletal requirements of the STS movement, it can be speculated that it is one of the difficult daily tasks for lower limb amputees. Muscle strength and proprioceptive feedback play a primary role in postural balance control during ambulation. 9 Strength and proprioception are both impaired following transtibial (TT) amputation.9–13 However, it is found that people with TT amputations for any reason had to perform the STS activity 43 to 56 times in a day, which is almost similar to healthy individuals.14,15
The lower limb amputees (both transfemoral and TT) were found to rely on their sound limb more than the amputated limb during everyday activities including STS task due to impairments which some of them mentioned above.9,16–23 In a recent review of the literature, Gailey et al. 20 have reported that asymmetrical loading of body weight distribution may lead to secondary physical impairments such as osteoarthritis and osteoporosis in this population. One of the important focuses of amputee rehabilitation should be avoiding the non-amputated limb from the secondary musculoskeletal impairments in the scope of preventive rehabilitation.
As far as we know, there is little research on movement strategies of the STS task in unilateral transtibial amputees (TTA).16,22 Furthermore, they just focused on weight distribution asymmetry. However, for a successful STS movement, not only symmetrical weight bearing on both extremities but also sufficient postural balance control and strength of legs are required.
Since the STS activity is the most mechanically demanding task 4 and is performed by TTA in a day almost similar times to healthy individuals,14,15 the preferred motor strategies to perform this task should be well identified in order to provide a valuable insight into motor control and to develop an appropriate STS training program to improve their ability to stand up properly.
The purpose of this study, therefore, was to examine movement strategies of the STS task by means of weight transfer time, rising index (force exerted by legs), sway velocity, and weight-bearing symmetry among the persons with TT amputation and healthy non-amputated individuals.
Methods
Participants
A total of 12 male unilateral TTA and 19 healthy male subjects (aged 24–54 years) took part in this study. TTA were recruited from patients attending the Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Department of Orthotics and Prosthetics. Inclusion criteria for TTA included ability to understand the study protocol, unilateral involvement, and ability to walk without an assistive device. All amputees were required to have a comfortable fit of current prosthesis for a period of at least 6 months. The healthy volunteers were recruited from partners of the amputees and hospital staff. Study participants were excluded if they had any known neurological or orthopedic disorders, had a body mass index (BMI) value higher than 30.00 kg/m2, had stump pain, or were not able to stand up without relying on arm or other external assistance. All subjects signed an informed consent before participating in this study. The study was approved by the Ethics Committee of the Dokuz Eylul University.
STS assessment
The Balance Master System (NeuroCom version 8.1, International, Inc., USA) was used to evaluate the STS movement, and assessment procedure was completed according to the manufacturer’s instructions. 24 The Balance Master System is a tool to provide quantitative assessment of balance ability and specific movement characteristics during functional activities. 24 This system has been used in the previous studies.25,26 All STS movements were performed on a long force platform comprising two force plates. Force sensors under the force plates measure the vertical forces exerted by the subjects’ feet. The participants were seated on an armless and backless chair (seat height of 406 mm), with arms resting by the sides. In a sitting posture, while facing the monitor, they kept both legs at shoulder width and placed feet symmetrically and parallel to each other on each force plate.
Prior to testing, sitting posture and movement pattern during STS task were explained to the subjects who practiced several trials to become familiar with the test. 24 The participants were informed to follow the instructions (sit steady until the “Go” sign appears at the top of the monitor, stand up as quickly as possible, then the monitor changes to show the “Hold Steady” sign and maintain your upright position) from the monitor to start and complete the STS trial. The participants were asked to stand up as fast as possible without the help of the upper limbs and then maintain upright posture for 5 s. STS procedure was repeated three times and the mean score was recorded. None of the subjects needed an interval between the trials to rest. Because each amputee’s prosthesis was fitted and aligned for use with everyday shoes, all STS tests were performed with all amputees wearing their own shoes that they regularly used with prosthesis. All the amputees who participated in the study preferred to wear hard-soled dress shoes.
There are some critical events in this test which are measured by software of the system. “Rising phase” of the STS test starts at the onset of center of gravity (COG) progressing forward and ends at the first point where COG is greater than 90% of the end COG position. Another critical event “Standing” is determined by completion of COG forward progression.
The measured parameters of STS on the NeuroCom Balance Master were 24
Weight transfer time is the time in seconds between the onset of the movement and the arrival of the COG over the feet. The arrival of COG over the feet is determined by full weight bearing on the feet.
Rising index is the maximum amount of force exerted by the legs during the rising phase. The force is expressed as a percentage of the patient’s body weight.
Sway velocity is the average amount of COG sway during the rise to stand and for the first 5 s following the rise. Sway is expressed in degrees per second.
Weight-bearing symmetry is the relative amount of weight borne by each leg during the rise to stand up and for the first 5 s after the rise, expressed as a percentage. It was calculated using the following formula

where S and P represent sound (or dominant side for healthy subjects) and prosthetic limb (or non-dominant side), respectively. Limb dominance in healthy subjects was determined by asking which limb they prefer to kick a ball.
Assessment of knee extensor strength
The subjects’ maximum isometric knee extensor strengths (KESs) were tested by using handheld dynamometer (HHD, PowerTrack II, Jtech Medical, Salt Lake City, UT, USA). All strength measurements were performed by the same examiner. Examiner with previous experience using the HHD had sufficient strength to resist the subjects’ muscle contraction. Measurements were taken bilaterally with the help of another researcher to stabilize the patients. Subjects sat on an armless chair with the hip and knee in approximately 90° of flexion and without foot contact to the floor. Subjects were asked to straighten the leg to push against HHD maximally 2–3 s and to stop after 4–5 s. 27 Subjects were not allowed to use arms and lean back during the test. Examiner applied counterforce to the subjects’ KESs. The HHD was placed just proximal to the malleolus or distal stump and direction of the counterforce was perpendicular to the limb being tested. All measurements were repeated three times for each limb and maximum value was recorded. According to the test procedure, they were given 1 min of rest between the repetitions. Measured force values for KESs were given in kilogram.
Figure 1 shows the positions of the KES measurements. Transducer of the HHD was placed on the distal end of the stump to measure the KES of amputated limb. KES in sound limb of TTA was assessed at two different positions. At one of the positions, it was measured at the same level with amputated limb (Position 1, P1), and at the second position, the measurement was repeated at the proximal point of malleolus, anterior surface of the distal tibia (Position 2, P2). In healthy subjects, transducer of the HHD was placed on as P2 of the sound limb of TTA. Measurement was taken bilaterally for dominant and non-dominant side. To define the P1 point on the sound limb, a plastic tape was used. The distance from the center of the HHD on amputated limb to the knee joint axis was measured, and then the center of the HHD was placed at the same level on the sound limb.
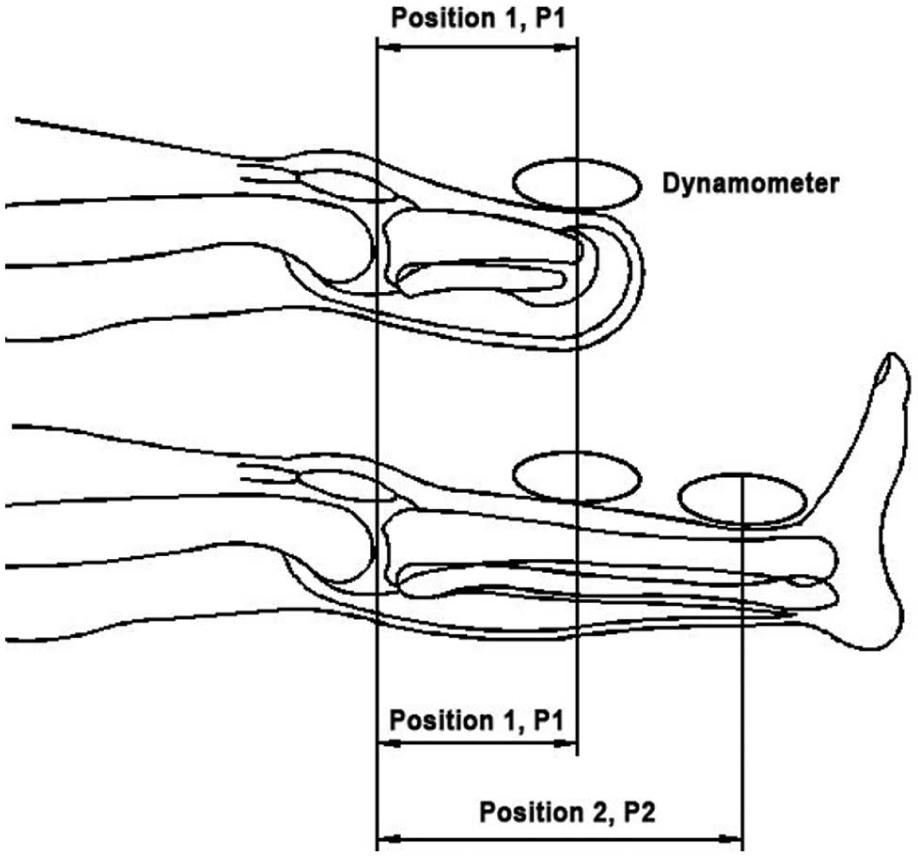
Positions of the knee extensor strength measurements.
Statistical analysis
The statistical analyses were performed by using SPSS 15.0 for Windows. Level of significance was set at p < 0.05. Data were summarized as means and standard deviations (SDs). Equality of variances was tested by using Levene’s test. Normality of the data distribution was tested by the Kolmogorov–Smirnov test. The data were normally distributed and therefore parametric analysis was used. To compare demographics, STS movement parameters and KES values between TTA and healthy subjects, independent samples t-test was performed. The KES values of the healthy subjects were used for analysis as means of KES in the dominant and non-dominant sides. The KES differences between sound limb and amputated limb were examined by independent samples t-test.
Results
The data were analyzed for 12 TTA and 19 healthy non-amputated subjects. All amputations were unilateral (mean ± SD years as an amputee = 7.36 ± 6.92, range = 1–23 years), 8 (66.7%) caused by trauma and 4 (33.3%) resulted from a vascular disease. Five amputees were amputated on the right side (41.7%) and seven (58.3%) were amputated on the left side. Mean stump length was 13.71 ± 3.00 cm (range = 9.0–21.0). Mean stump length as a percentage of the sound limb was 36.00 ± 8.01 (range = 25.28–53.85). Amputees had experience in prosthesis use for at least 6 months (mean ± SD years as a prosthesis user = 4.33 ± 6.35, range = 0.5–22.5 years). Eleven (91.7%) amputees were fitted with a patellar tendon-bearing supracondylar socket and only one (8.3%) with a patellar tendon-bearing supracondylar–suprapatellar socket. The foot type of 11 amputees was solid ankle cushion heel (SACH) foot, and one amputee had a C-Walk foot (the 1C40 Otto Bock C-Walk foot).
Demographic data of the TTA and healthy subjects are presented in Table 1. All participants were sedentary (did not have regular sport or exercise habits) and had never received any kind of balance and STS training. At the time of the investigation, all amputees were able to walk without assistive device (e.g. cane, walker) as well as stand up several times without arm support. No subjects had any complaint of knee or stump pain during the tests.
Demographic data of transtibial amputees and healthy subjects.
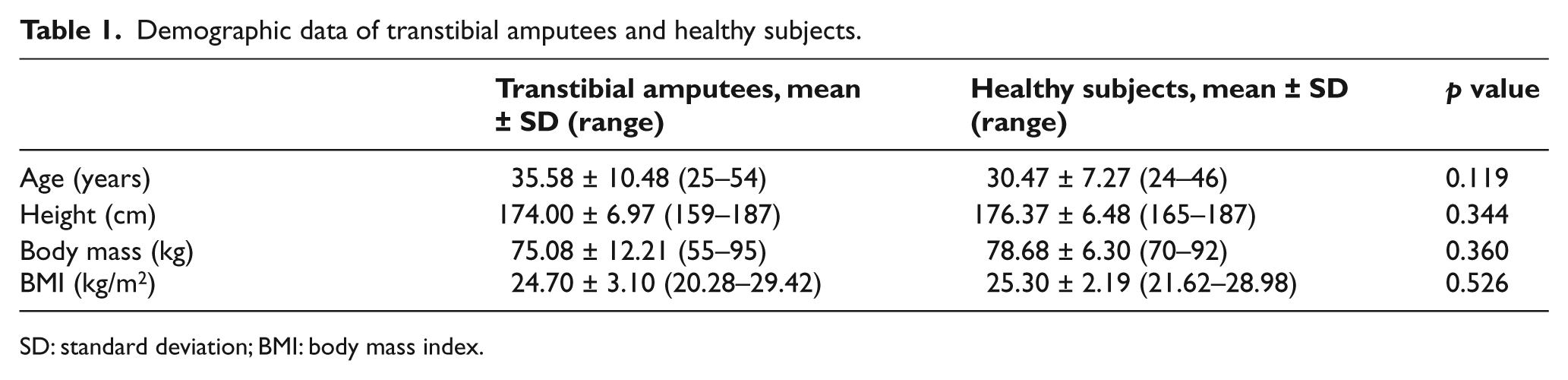
SD: standard deviation; BMI: body mass index.
STS parameters
The comparison of STS parameters between TTA and healthy subjects is shown in Table 2. During the STS movement, participants in both groups exhibited similar weight-bearing transfer time (p > 0.05). Weight-bearing symmetry values were almost twice as high in TTA compared to healthy subjects, indicating significantly more weight-bearing asymmetry than healthy ones (p < 0.05). The results showed that amputees had a significantly increased sway velocity and generated significantly lower rising index than healthy subjects during the STS movement (p < 0.01).
Comparison of sit-to-stand (STS) parameters between transtibial amputees and healthy subjects.
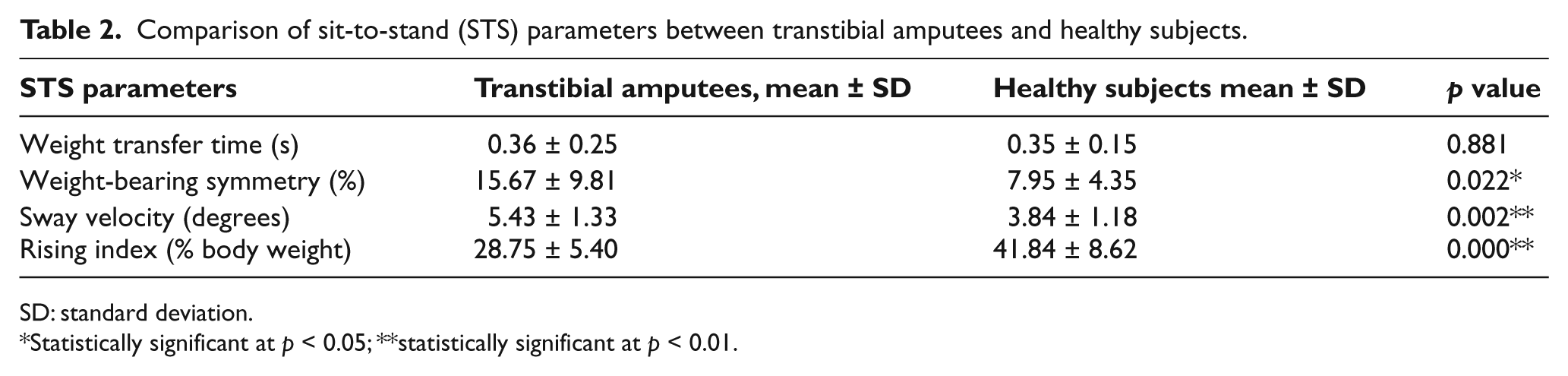
SD: standard deviation.
Statistically significant at p < 0.05; **statistically significant at p < 0.01.
KES values
As shown in Table 3, the KES of the amputated limb was lower than the sound limb (p < 0.01). On the contrary, TTA had KES of sound limb similar to the healthy subjects (p > 0.05).
Comparison of knee extensor strength (KES) values between transtibial amputees (amputated limb vs sound limb) and healthy subjects.
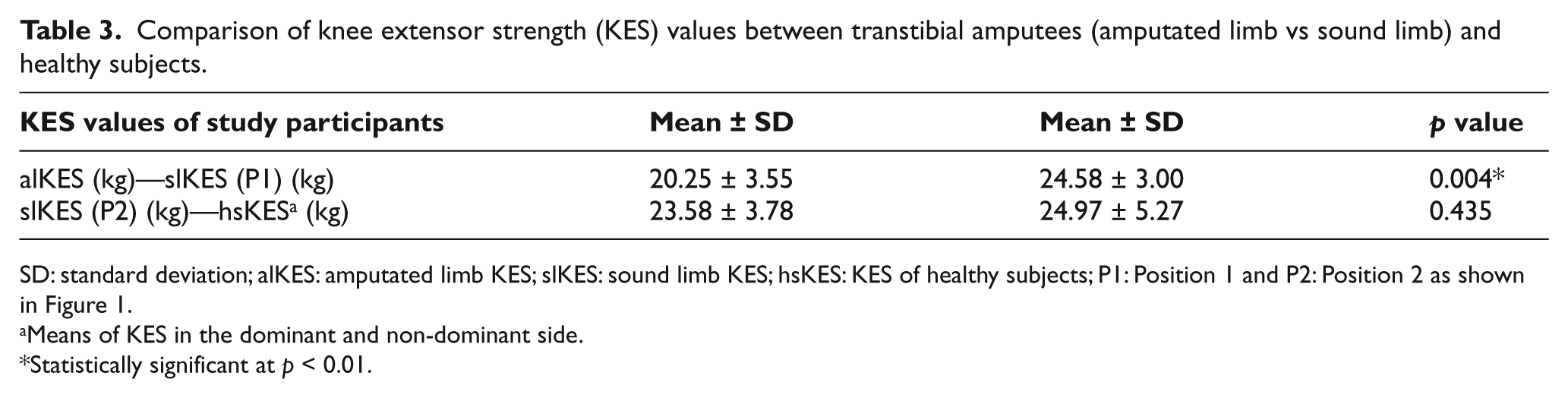
SD: standard deviation; alKES: amputated limb KES; slKES: sound limb KES; hsKES: KES of healthy subjects; P1: Position 1 and P2: Position 2 as shown in Figure 1..
Means of KES in the dominant and non-dominant side.
Statistically significant at p < 0.01
Discussion
Few studies investigating the biomechanics and movement strategies of STS task in lower extremity amputees have been reported in the scientific literature, although it is the most frequently used task in daily living. 2 Moreover the results of the limited number of studies are difficult to compare because the characteristics of their subjects, the methods they used, and the presentation of their results differ largely. 23 There are only two studies which address weight-bearing asymmetry during STS task in TTA.16,22
The results of this study not only supported weight-bearing asymmetry in persons with TT amputation but also indicated a difference in movement strategy during STS activity, including sway velocity and rising index parameters of STS activity.
Weight-bearing symmetry
One of the most focused problems of unilateral lower extremity amputees during daily living activities in scientific literature is weight distribution asymmetry.16,21,23 The TTA in this study demonstrated 15.67% asymmetry tending to load their sound limb. This result means that TTA in this study bore approximately 42% of their body weight on amputated side and approximately 58% on their sound side, which is different from the control group. The study of Agrawal et al. 16 indicated increased loading on the sound limb in TTA by approximately 27% during STS task.
Agrawal et al. 16 discussed that muscle weakness of amputated limb could influence the weight-bearing symmetry either by reducing the load on the amputated limb or by increasing the force generation capacity of sound limb muscles. The KES results of this study, which showed significantly lower strength of knee extensor muscle group of amputated limb than sound limb, support the suggestion of the previous study. Nevertheless, Agrawal et al. 16 did not measure any strength value of lower extremity of their participants that we can compare with.
On the contrary, healthy subjects tend to load the feet symmetrically during transitioning activities such as stand from sitting.23,28 Minor deviations in symmetry is accepted as normal since Highsmith et al. 21 and Burger et al. 23 showed that the healthy control subjects in their studies had 7% and 5% asymmetry values, respectively. Parallel to the previous studies, the control subjects in this study chose to perform the STS task by 7.95% (dominant side: approximately 54% of body weight; non-dominant side: approximately 46% of body weight) asymmetry. It is possible that the dominancy in lower extremities of the control subjects could cause these minor differences in weight-bearing symmetry.
Weight transfer time
Widely different ranges of time have been reported in the literature for the time required to stand up from a sitting position. The weight transfer time in this study represents the time from the seat to the arrival of the COG over the feet. This period is a preparation for standing which usually occurs very quickly. The muscle activity in this short period is performed mostly by the trunk and hip flexors. 24 Therefore, weight transfer time measured by the current method does not give any clue for the activity of muscles of lower extremity. Since the TTA preserve trunk and hip flexors, weight transfer time scores between TTA and healthy individuals were similar in this study.
The study of Burger et al. 23 categorized the time required to stand up as time to seat off, time from seat off to standing, and total time to stand up. The time to seat off period was described as the time from the initiation of the rising maneuver to the movement when there was no force measured under the seat which represents the similar period with weight transfer time in this study. Although the difference in time to seat off between amputees and healthy individuals in the study of Burger et al. was not significant statistically, amputees took longer time to seat off than healthy ones. In this study also, weight transfer time scores were similar between the two groups. The amputee subjects in this study were recruited from the TTA who had non-affected trunk and hip flexor muscles. Amputees in the study of Burger et al. were transfemoral amputees who had shorter moment arm of hip muscles because of amputation. 23 As the activation of the quadriceps and hamstring muscle groups were considered to be the prime movers for the STS movement, lower strength of these muscle group caused by shorter moment arm might result in longer time to seat off. 29
Rising index
Rising index is considered to be an important indicator of lower extremity extensor muscle strength. 24 In rising phase, the legs must extend and push down against the surface to produce counterforce sufficient to raise the body to a standing position. TTA in our study performed lower rising index score than healthy individuals indicating lower extensor muscle strength of lower extremity. The lower KES results of the amputated limbs supported the finding of lower rising index in TTA during STS task. Lower rising index generation by amputated limb muscles could be a potential contributor to the STS asymmetry, which also leads to altered STS movement strategies in this group of patient.
Sway velocity
The results of the postural sway values showed that TTA had greater sway velocity indicating worse postural control compared to healthy individuals during STS task. Impairment in balance control was an expected result due to compromised somatosensory input, muscular activity, and its force generation capacity.30,31 Most of the studies investigating postural control behavior of lower leg amputees have mainly focused on sway at upright stance or during dynamic conditions by using a moving platform. The results of these studies are contradictory, but most of them reported diminished postural control in amputated individuals especially during dynamic tasks.32,33 The data of our study on impaired postural control in TTA during STS task confirmed the previous studies.
The impaired postural control can be another important factor influencing the weight-bearing symmetry. These associations between asymmetry and postural control have been indicated for stroke patients in the study by de Hart et al. 34 Furthermore, it was suggested that increased weight-bearing asymmetry caused increase in postural instability in healthy subjects. 35 Knowledge of the relation between the weight distribution and postural stability is important to improve rehabilitation strategies for different group of patients, especially unilateral affected pathologies such as unilateral TT amputations. The result of our study effectuated a new focus about this possible relationship by demonstrating significant difference in postural sway values and weight-bearing symmetry between TTA and healthy subjects during STS task. We did not estimate the relationship between sway velocity and weight-bearing symmetry in the study, but we suggest investigating this relation in TTA during STS task for further researchers. Therefore, new rehabilitation approaches including combination of the balance training and weight-bearing exercises to improve STS task in TTA can be investigated in future studies.
Limitation of study included the diversity of amputation reasons such as trauma and vascular disease. It would be beneficial to include amputees who have the same cause of amputation in future studies.
Conclusion
In conclusion, this study revealed different movement strategies of the STS task in TTA. The TTA participants tended to load their sound limb more than the amputated one with more impaired postural control and reduced force exerted by the legs compared to healthy non-amputated individuals. Minimizing the weight-bearing asymmetry and maintaining an appropriate STS movement together may help preserve the healthy condition of the sound limb. Further studies are required to develop STS training protocols specific to TTA, which has not been described yet, based on the findings of ours and previous studies.
Footnotes
Declaration of conflicting interests
The authors report no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.