
Abstract
The clinical and functional results of traditional techniques for trans-femoral amputation are often poor. The ISPO consensus conference on amputation surgery in 1990 at Glasgow recommended myodesis as an important integral part of surgical procedure and should be carried out as much as possible. Muscle stabilization provides a stable functional amputation stump. This improves the prosthetic management and walking ability. A technique of myodesis for trans-femoral amputation has been developed in Dundee, especially for elderly dysvascular patients. The functional and clinical results of this technique were studied in 33 patients, who underwent the surgical procedure. Data regarding patient demographics, postoperative morbidity, mortality and functional status were obtained from a prospectively recorded pro forma. Fourteen patients out of 33, who were operated using this technique, were fitted with artificial limbs. Of these, 11 (78.5%) were still using the prosthesis at a mean follow-up of 40 months. There was 100% primary wound healing. Two patients underwent further revision surgery for delayed stump problems. Good clinical and functional results were obtained using this technique. It is particularly suited for the elderly dysvascular patients, whose stumps are shorter and bone quality poor. The low rate of stump problems and consequent revision surgery enables a more comfortable stump for non-prosthetic users.
Introduction
Trans-femoral amputation in the elderly dysvascular patient is usually associated with a high incidence of stump problems, revision rates and poor functional results (Nehler et al. 2003; Pernot et al. 2000; Davies and Datta 2003; Vallabhaneni et al. 2001; Pohjolainen et al. 1990; Pinzur et al. 1992). Traditionally described techniques of trans-femoral amputation result in abduction and flexion deformity of the residual bony stump in its soft tissue envelope due to the unopposed action of the abductors and hip flexors (Gottschalk 1999) (Figure 1). This deformity can be clinically obvious by the prominence of the residual bone in the anterolateral aspect of the distal part of the stump. This not only causes problems with limb fitting but also leads to a lurching gait. This deformity is particularly worse in elderly dysvascular patients due to the short nature of their stumps. Recent understanding in the biomechanics of trans-femoral amputation has highlighted the importance of surgical technique in improving functional outcomes. Attaching the counteracting muscles to the residual bone during trans-femoral amputation can lead to a biomechanically more stable stump and is said to improve limb fitting and better functional results. Such a technique of myodesis has been developed for the elderly dysvascular patient, in the Dundee Limb Fitting Centre. This technique is presented here along with its clinical and functional results.
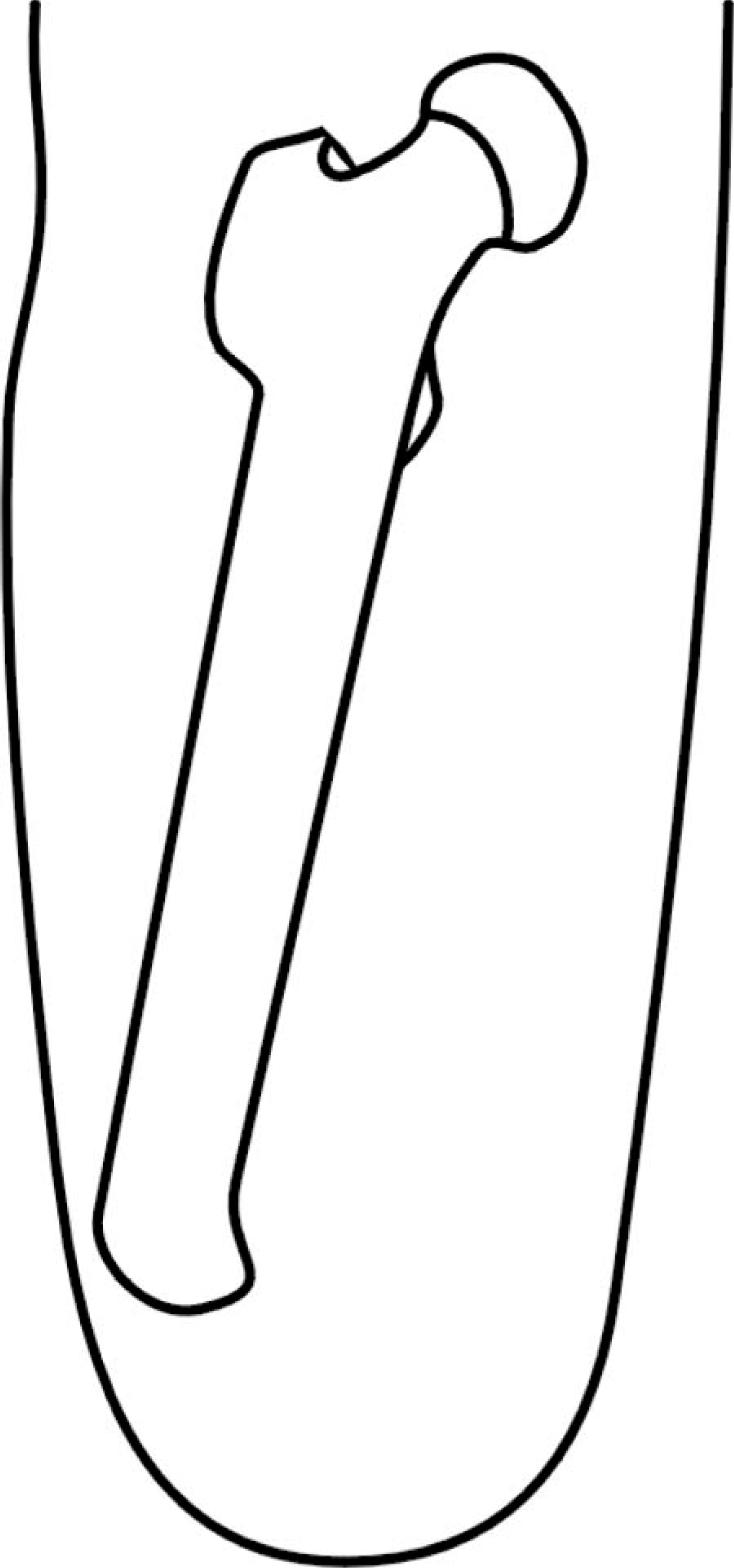
A schematic diagram showing the abduction deformity of the residual bone in the stump.
Methods
This was a cohort study of all patients referred to the Dundee Limb Fitting Centre for trans-femoral amputation, July 1996 to July 2001. Details regarding patient demographics, post-operative morbidity and mortality and functional status were obtained from a prospectively recorded database. The patients were examined for any prominence of the residual bone in the anterolateral aspect of the distal part of the stump. The power of various muscle groups in the stump was also evaluated by the physiotherapists using the Medical Research Council (MRC) grading. According to this scale, Grade 0 refers to complete paralysis. Grade1 is assigned when only a flicker of muscle contraction can be felt. Grade 2 is assigned when the muscle is strong enough to move the appropriate joint with gravity eliminated. Grade 3 is assigned when a muscle can move the joint against gravity, but not against the examiner's resistance. Grade 4 is assigned when there is some degree of weakness. Grade 5 refers to normal power.
Pre-operative investigations to determine the level of trans-femoral amputation included: thermography, skin blood flow and clinical examination. Skin temperature higher than 30.4°C at the site of planned skin incision and a capillary skin blood flow greater than 2.5 ml per 100 g tissue per min were taken as good prognostic indicators for healing of a trans-femoral amputation.
The surgeon and physiotherapists assessed all patients post-operatively for suitability of limb fitting. Patients with significant co-morbidities such as cardiac and respiratory problems were not fitted with prosthesis. Similarly, patients with significant physical problems such as presence of arthritis in the contralateral limb, persistent problems with the stump, bilateral trans-femoral amputations and those who failed to progress, in spite of adequate rehabilitation, were deemed unfit for prosthetic fitting.
Operative technique
The skin incision is made approximately 8 cm distal to the planned level of bone resection. It is fashioned in a fish mouth pattern such that the radius of anterior and posterior flaps is equal (Figure 2). All the muscles are cut at the level of skin and bone is cut proximally. The nerves are ligated, cut and allowed to retract and haemostasis is achieved. The edges of the bone are smoothed to prevent any prominent ends from creating a painful stump. A 2 mm drill is used to make two drill holes in the distal end of the bone, one anteromedially and one anterolaterally for the myodesis. The adductors and the medial hamstrings are tied to the anteromedial hole; the vastus lateralis and lateral hamstrings are tied to the anterolateral hole (Figure 3). The quadriceps muscle bulk is brought over the distal end of the bone and attached to the hamstring muscles. All muscles are tied under adequate tension such that a well-balanced stump is created. Pre-operative positioning of the patient with a sandbag under the affected hip will allow assessment of balance of the stump. The wound is closed in layers and skin closed with staples.
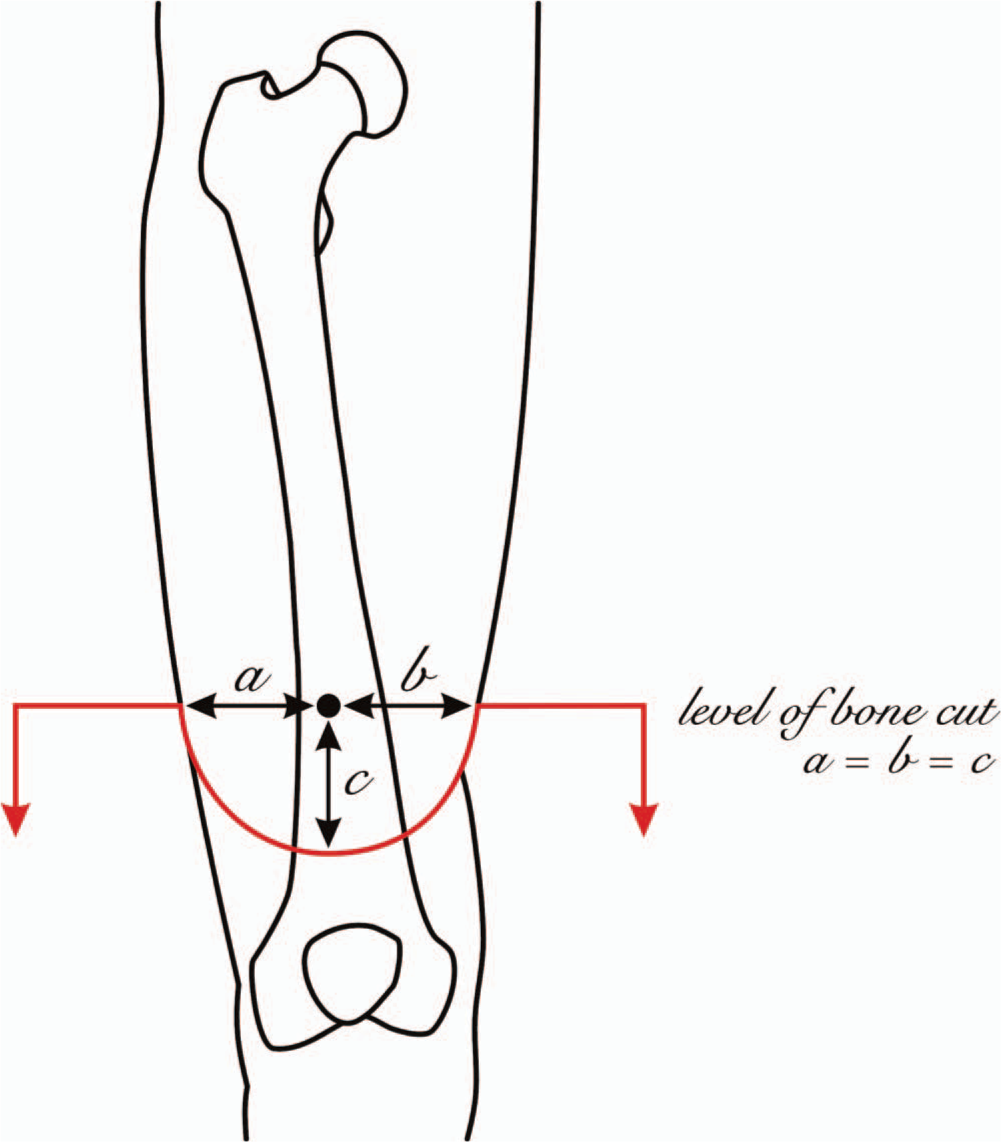
Planning the skin incision: The semicircular line indicates the fish mouth flap over the thigh.
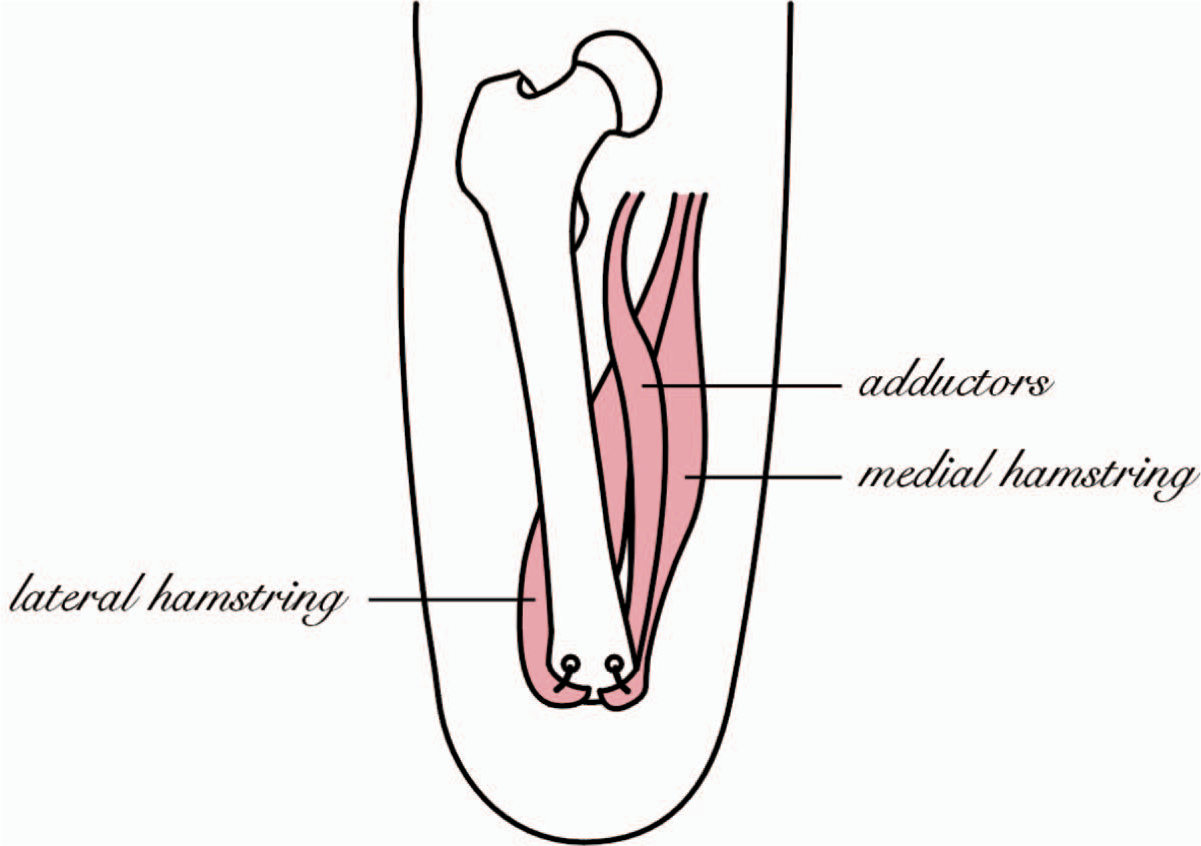
The technique of attaching the adductors and medial and lateral hamstrings to the distal end of the residual bone.
Results
Thirty-three patients were subjected to 34 trans-femoral amputations during the period July 1996 to August 2001. Average age of the patients was 69 (range 42 – 89). The indication for trans-femoral amputation was peripheral vascular disease with or without diabetes in all these patients. Of these, four were revisions from trans-tibial to trans-femoral amputations. There were 20 males and 13 females. The average follow-up period was 40 months (range 13 – 76 months).
Prosthetic limbs were made for 14 of the 34 trans-femoral amputations. One patient in this group suffered from prolonged wound leakage postoperatively but this settled without any further complications. Displacement of the residual bone within the soft tissue envelope was noted in another patient. The displacement was causing pressure necrosis of the skin leading to a revision for this patient. Two patients had pain in the stump due to neuroma formation. Three patients needed alterations or new limbs made due to change in size of the stump. Eleven out of 14 patients (78.5%) were still ambulatory at last follow-up, while three were totally wheelchair bound. Of the 11 who were still using their prosthesis, eight patients were walking with the aid of a walking frame for short distances and wheel chair for long distances. Three patients were walking with two crutches.
Of the 19 patients who did not receive prosthetic fitting, the reason for not fitting prosthesis was significant co-existing cardiorespiratory problems in 12 patients, five patients failed to progress satisfactorily in spite of rehabilitation, one patient was a bilateral trans-femoral amputee and one patient had arthritis in the contralateral hip. Apart from one patient who needed a subsequent stump revision to a higher level, no other stump problems were seen in this group of patients.
Out of the 34 stumps, six stumps had a grade 4/5-muscle power (MRC grading) in the adductor muscles. Of these, two patients were fitted with prosthesis, while the other four did not have prosthetic fitting. The quadriceps, hamstring, abductor and adductor muscle strength in all the other stumps was 5/5.
Discussion
There was a 100% primary wound-healing rate using this technique of trans-femoral amputation. A well-balanced stump was obtained in all but one patient. Some 78.5% of patients who had limbs fitted were still mobile with their prosthesis at a mean follow-up of 43 months. Of the patients provided with a prosthesis, 78.5% did not need any alterations made to the limbs after their initial fitting. The low rate of stump problems and consequent revision of the stump enabled even non-prosthetic users to have a stable stump, which was more comfortable for wheelchair use and nursing in bed.
Gottschalk (1999) obtained similar good clinical and functional results with his technique of myodesis for trans-femoral amputation. Twenty patients were followed up over two years. All were prosthetic users and there were no stump breakdowns. However, only six patients in this series had amputations because of vascular problems. In his technique, a long medial skin flap is used. The adductor magnus muscle is detached at its attachment brought over the distal end of the femur and sutured to its lateral aspect. The quadriceps is attached posteriorly to the femur and the hamstrings are attached to the adductor muscles. However, because of the short nature of the stump in patients with peripheral vascular disease, it may not be possible to preserve the full length of the adductor magnus muscle to perform the technique as described by Gottschalk. Skin closure can also pose a problem in patients with peripheral vascular disease. Due to multiple previous attempts at vascular reconstruction, they are often left with unhealthy scar tissue on the medial side of the thigh. A medially based flap may not be feasible in such a case. However, by using a fish mouth incision as described in the current technique, the unhealthy skin on the medial side of the thigh can be sacrificed without compromising stump closure.
The technique of myodesis for trans-femoral amputation has been well documented in literature. Earlier techniques describe using four drill holes to attach the four groups of thigh muscles to the distal end of the residual bone. This may be suitable for young patients who have good bone stock but not in elderly patients who frequently have osteoporotic bone. Using two drill holes in these patients as described in the present technique decreases the risk of intra-operative fracture while making the drill holes.
A technique of myodesis aimed to restore the normal alignment of the femur, provides significant biomechanical advantage over conventional techniques of trans-femoral amputation. Traditional techniques of trans-femoral amputation involve sacrificing the hamstrings and hip adductor muscles and maintaining the femur in a central position within the soft tissue envelope. This results in displacement of the residual bone into a position of abduction and flexion due to the unopposed action of the hip abductor muscles and hip flexors (Figure 1). The resulting loss of alignment of the femur causes a significant decrease in lever arm of the hip abductor muscles leading to a lurching gait. This demands a further increase in energy expenditure in the dysvascular trans-femoral amputee, who normally has a pre-existing compromise in cardiorespiratory reserve. This can be the reason most elderly dysvascular patients give up walking after trans-femoral amputation. A study of literature indicates a wide variation in the proportion of prosthetic candidates successfully resuming daily activities with prosthesis after major lower limb amputations (Nehler et al. 2003; Pernot et al. 2000; Davies and Datta 2003; Vallabhaneni et al. 2001; Pohjolainen et al. 1990; Pinzur et al. 1992). In one prospective audit of all lower limb amputees in patients with peripheral vascular disease, it was found that only 42% of patients who received prosthesis maintained or improved their mobility. They concluded that the outcome of amputation is worse than widely perceived despite improvements in prosthesis and rehabilitation (Vallabhaneni et al. 2001).
The displacement of the bone in the stump following conventional techniques of trans-femoral amputation can also pose problems with limb fitting. Improvements in prosthetic technology alone have failed to stabilize the residual femur in the stump.
Attaching the counteracting muscles to the residual femur can stabilize the hip muscles and maintain the femur in its normal alignment thus minimizing any gait abnormality. There is MRI and electromyographic evidence that muscles anchored to bone surgically can maintain its nerve supply and function (Jaegers et al. 1995; 1996). This is confirmed clinically in the present study where the muscle strengths of the adductors and hamstrings were found to be well preserved. It also creates a stump which is more suitable for limb fitting as seen in the present series, where there was a relatively low incidence of limb fitting problems.
Conclusion
The fish mouth skin incision and the technique of attachment of the adductor muscles to the bone make the Dundee technique of myodesis particularly suitable for elderly dysvascular patients. Good clinical results have been obtained using this technique. The theoretical advantage of maintaining the femur in its normal anatomical alignment is shown to translate into good functional results with a high proportion of patients still using the prosthesis at final review. This technique must be considered for the elderly dysvascular patient in order to maximize their biomechanical advantage during the gait pattern, improve limb fitting and consequently preserve their mobility as much as possible. It also provides a stable, trouble-free stump for non-prosthetic users, making it more comfortable for wheelchair use and nursing in bed.
Footnotes
Acknowledgements
The authors thank Mr Ian Christie, Web Publisher/Illustrator, University Department of Orthopaedic and Trauma Surgery, TORT Centre, Ninewells Hospital and Medical School, for his help in creating the illustrations.