
Abstract
Today there is considerable evidence that child survivors of road traffic accidents (RTAs) can suffer from significant and long-lasting behavioural problems and mental disorders such as post-traumatic stress disorder (PTSD), depression, and anxiety. Previous studies have found that around 10–35% of children after RTA develop PTSD or suffer from clinically relevant post-traumatic stress symptoms (PTSS) that may last more than 1 year 1–4. Despite this growing interest in mental health problems of traffic-injured children, the effects of RTA on health-related quality of life (HRQOL) of children and adolescents have received almost no attention. Sturms et al. conducted three studies in traffic-injured children, but most of those children had minor injuries and were treated in outpatient settings 5–7. Therefore, it is unclear whether their results can be generalized to children with more severe injuries needing inpatient treatment. Sturms et al. reported significant problems in the children's motor functioning and autonomy, especially during the first months after the accident. Children from families with low socioeconomic status and who had more severe injuries were at particularly high risk of a reduced HRQOL. To date, additional determinants of HRQOL in children after RTA have not been studied in detail. From studies in other groups of injured children, however, we know that many factors may influence HRQOL, including age and sex of the child [8, 9], type of injuries [10, 11], functional status [9], symptoms of acute stress disorder [12], personality [9], and quality of family relations [8].
Although previous studies have clearly shown that PTSS are frequent in children after RTA, the specific impact of these symptoms on HRQOL has not been examined in detail. At the same time, the pertinent literature in adults suggests an association of PTSD with lower QOL in survivors of different types of trauma or illness 13–15. Notably, two prospective studies among adult patients with physical trauma [16, 17] reported that PTSD had a substantial impact on short- and long-term HRQOL. These findings were supported by the only study on this issue among adults who had experienced an RTA [18]. That study, however, was cross-sectional in design and therefore conclusions about causal associations between PTSD and HRQOL cannot be drawn. Finally, there is one prospective study by Holbrook et al. in injured adolescents aged 12–19 years that included a group of patients with RTA [12]. Findings of that study showed that acute stress disorder before discharge from hospital was associated with significant HRQOL deficits at follow up.
Taken together, there is little knowledge on HRQOL of children and adolescents after RTA who had injuries needing inpatient treatment. Moreover, although a previous study in traffic-injured adults suggest that PTSS may be important predictors of HRQOL, this issue has never been prospectively examined in children. Therefore, the objectives of the present study were twofold. The first was to delineate self-reported HRQOL in children and adolescents during the first year after an RTA, and to contrast their HRQOL with that of a healthy reference group. Based on the aforementioned findings, we hypothesized that children and adolescents after RTA would have a reduced HRQOL in the initial phase after the accident but show improvement over 1 year. The second was to examine predictors of HRQOL. Specifically, we were interested in the long-term impact of PTSS on HRQOL in traffic-injured children. Based on findings in adults, post-traumatic stress in children was expected to predict lower HRQOL at follow up.
Methods
Participants and procedure
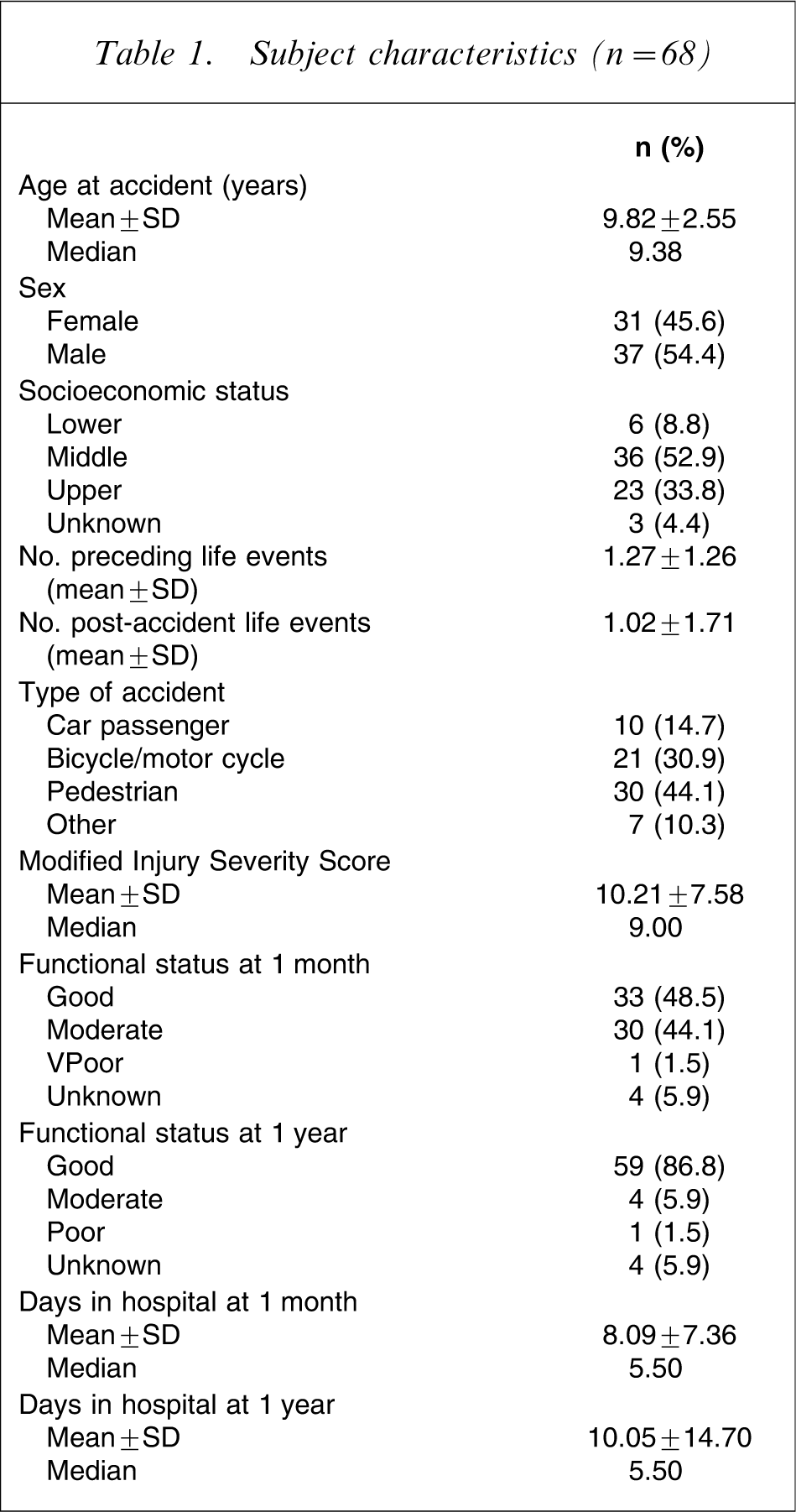
Participants were consecutively recruited for a period of 24 months in four children's hospitals in the German-speaking part of Switzerland. Children between 6.5 and 14.5 years and their parents were asked for participation in the study within the first 2 weeks after occurrence of an RTA if the following criteria were met: (i) hospitalization of at least 24 h; (ii) no severe brain injury; (iii) no evidence of mental retardation; (iv) fluency in German. Of 116 children who met these criteria, 38 (12 girls, 26 boys; mean age = 10.4 years) did not participate, mainly because the study seemed too time consuming. Due to incomplete data, 10 children had to be excluded from further analyses. Therefore, the final sample consisted of 68 children (response rate 58.6%). There were no significant differences between study completers and those who did not participate with regard to age (t = −1.61, p = 0.11) and sex (χ2=1.98, p = 0.16).
Ethics committee approval for the study was granted by all participating hospitals and after complete description of the study, written informed consent was obtained from the parents and those patients who were older than 12 years. Assessments were conducted 1 month and 1 year after the child's RTA. The children were assessed by means of a standardized face-to-face interview. Most interviews were conducted in the patients’ homes. Demographic and medical variables were retrieved from patient hospital records.
Measures
Injury severity
Severity of injuries was rated based on hospital records by a surgeon using the Modified Injury Severity Scale (MISS), a highly reliable and widely used scale [19]. The MISS allows the rating of the severity of injuries in different bodily systems. MISS values range from 1 to 75 (death), with scores ≥25 indicating a severe injury.
Functional status
Information on functional status with regard to physical activities of daily life was obtained from the surgeons. Functional status of the patients was assessed by a single item 1 month and 1 year after the accident using a 3-point Likert severity scale: 0 = good functional status, 1 = moderate functional status, and 2 = poor functional status. This measure has successfully been used in two earlier studies with paediatric patients [20, 21].
Health-related quality of life
Child HRQOL was assessed with the German version of a short form of the Toegepast Natuurwetenschappelijk Onderzoek-Academisch Ziekenhuis Leiden (TNO-AZL) Children's Quality of Life (TACQOL) questionnaire, Child Form [22]. The TACQOL is a multidimensional generic instrument designed for HRQOL assessment in medical research. It contains five health status scales: physical functioning, basic motor functioning, autonomy, cognitive, and social functioning. In addition, two scales assess general mood: positive emotional functioning and negative emotional functioning. Following the TACQOL protocol children were asked to note problems in any of the mentioned domains and whether they felt bothered by these problems. On all TACQOL scales, higher scores represent a better HRQOL. Internal and external validity of the TACQOL have been confirmed in previous studies with healthy and clinical samples [22]. The TACQOL short form includes the original seven scales, but uses only four items per scale instead of eight for all scales except one (physical functioning). The short form of the TACQOL was constructed by the original authors by using data from the Dutch reference study [22]. The results supported an internal and external validity of the short form that is comparable to the original TACQOL. Internal consistency coefficients in the present study were acceptable and similar to those of the reference study. To obtain a reliable measure of overall quality of life, we also computed a total score by summing the items across all scales and dividing the sum by the number of scales. Before summing, the physical functioning scale was divided by 2 because it contains the double number of items compared to the other scales. Thereby, all scales contributed to the sum score with equal weight. The distribution of the total score was normal at 1 month and at 1 year (Kolmogorov–Smirnov goodness of fit test). Reference data for this study were provided from a community sample of 1048 Dutch children [22].
Child post-traumatic stress symptoms
The Child PTSD Reaction Index (RI) by Frederick et al. [23] was used to assess PTSS. The RI contains 20 items that address school-aged children's fears following a traumatic event, symptoms relating to memories of the event, avoidance, and general functioning. A total score is obtained by summing across all items. Scores >24 are interpreted as clinically relevant. The internal consistency of the RI is good [24], and there are strong associations of RI scores with diagnostic criteria of PTSD in the DSM [25]. In the present study a German version of the RI was used. The scale achieved good internal consistency coefficients in this sample (α = 0.82 at 1 month, and α = 0.79 at 12 months).
Life events
The occurrence of 12 major life events, such as change of domicile, unemployment or parental separation was assessed using the mothers as informants. A sum score was computed by counting the number of life events. Life events were retrospectively assessed at initial assessment for the 12 months preceding the accident, and at follow up for the time period following the accident.
Socioeconomic status
Socioeconomic status was calculated by means of a sum score reflecting paternal occupation and maternal education (range = 2–12 points). Three social classes were defined as follows: scores 2–5 = lower class, scores 6–8 = middle class, scores 9–12 = upper class. This measure has been shown to be a reliable and valid indicator of socioeconomic status in our community [26].
Statistical analyses
Data were analysed using SPSS for Macintosh, release 11 (SPSS Chicago, IL, USA). Analyses were performed with two-sided tests, with p < 0.05 considered significant. χ2 analyses were used to compare nominal variables. Comparisons of TACQOL scales with published reference data were determined using one-sample t-tests. Moreover, we calculated effect sizes with Cohen's d to express the amount of difference between patients and the reference group and between the two assessments at 1 month and at 1 year for the TACQOL scales [27]. Because some variables were not normally distributed Spearman–Brown rank correlations were calculated to measure associations between the TACQOL total score and various predictors. Wilcoxon matched-pairs signed-ranks tests were used to compare HRQOL scores at 1 month and at 1 year. Finally, a linear regression model was set up using the normally distributed TACQOL total score as the dependent variable. Predictors were chosen on the basis of significant bivariate correlations with the dependent variable.
Results
Sample characteristics
Subject characteristics (n = 68)
Health-related quality of life at 1 month and 1 year
Quality of life (TACQOL scores) vs time after the accident
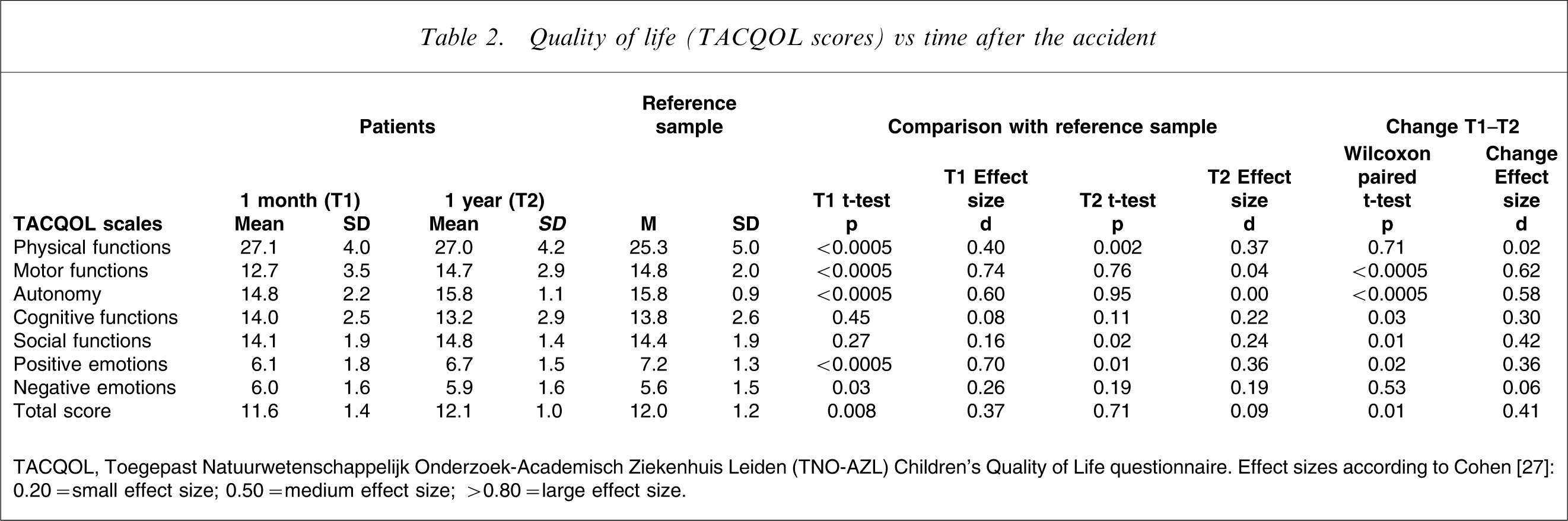
TACQOL, Toegepast Natuurwetenschappelijk Onderzoek-Academisch Ziekenhuis Leiden (TNO-AZL) Children's Quality of Life questionnaire. Effect sizes according to Cohen [27]: 0.20 = small effect size; 0.50 = medium effect size; >0.80 = large effect size.
Predictors of health-related quality of life
Spearman correlation (r) between predictor variables and child overall HRQOL (TACQOL total score) vs time
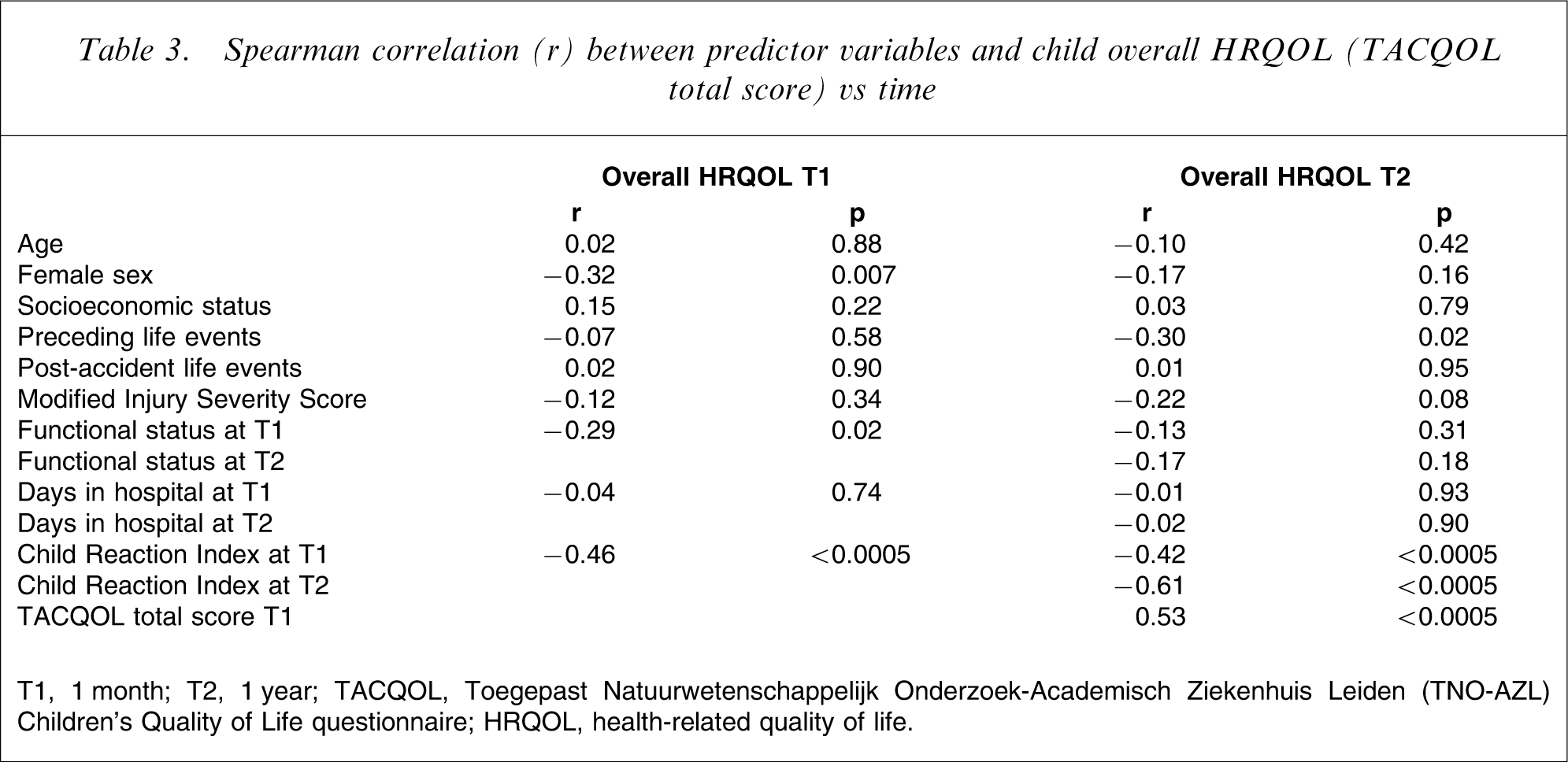
T1, 1 month; T2, 1 year; TACQOL, Toegepast Natuurwetenschappelijk Onderzoek-Academisch Ziekenhuis Leiden (TNO-AZL) Children's Quality of Life questionnaire; HRQOL, health-related quality of life.
Regression analysis predicting child HRQOL (TACQOL total score) at 1 year
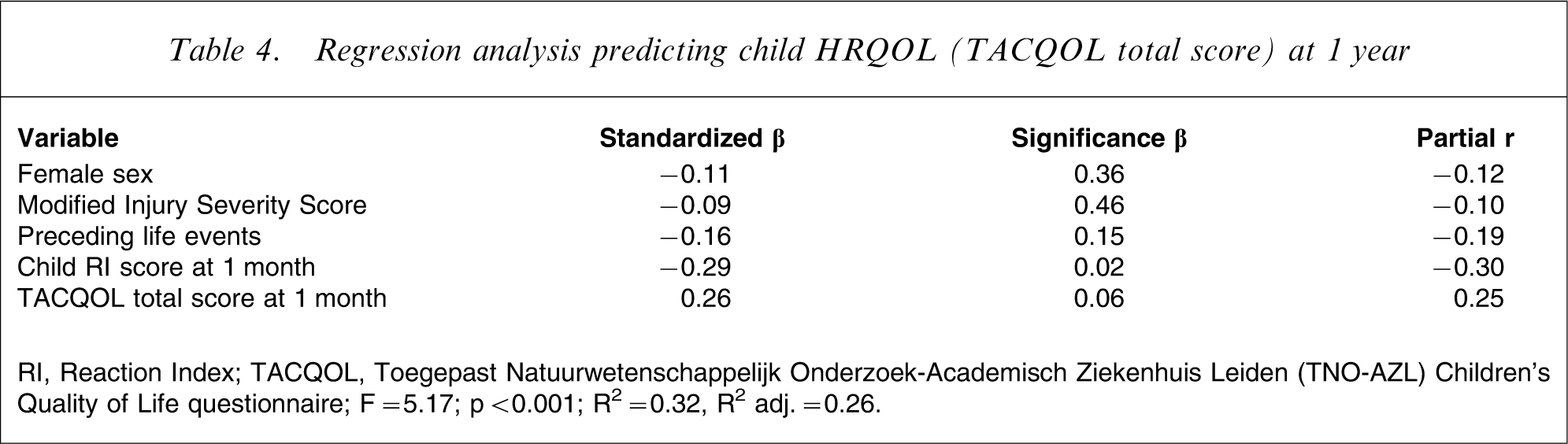
RI, Reaction Index; TACQOL, Toegepast Natuurwetenschappelijk Onderzoek-Academisch Ziekenhuis Leiden (TNO-AZL) Children's Quality of Life questionnaire.
F = 5.17; p < 0.001; R2=0.32, R2 adj.=0.26.
Discussion
This prospective 1 year follow-up study in children and adolescents after RTAs found several domains of HRQOL to be markedly compromised, but impairments were found only at 1 month after the accident. Specifically, compared to a community reference group, children reported reduced motor functioning and autonomy and impairments in some parts of emotional functioning at 1 month. All these impairments were short-lived, because the children's scores 1 year after the accident were well within or even above normal ranges. These results are consistent with our initial hypothesis and are similar to previous findings by Sturms et al. in children with less serious injuries 5–7. The present effect sizes, however, were higher, possibly because of a greater injury severity in the present sample. Remarkably, all dimensions of HRQOL were above or within normal ranges at 1 year. Thus, long-term HRQOL consequences of RTAs are usually not present in patients without severe brain injury.
The present study analysed the importance of initial PTSS and demographic and medical characteristics in predicting HRQOL in children after RTAs. Multiple regression analysis showed PTSS at 1 month after the accident to be crucial in influencing HRQOL at follow up. This is consistent with the hypothesis and strongly confirms previous findings in adults with different types of trauma 14–18, [28]. The present results are also in line with the study by Holbrook et al., who found acute stress disorder to predict HRQOL deficits in injured adolescents with different types of physical trauma [12]. The present study is now the first to prospectively show a negative effect of early PTSS on HRQOL among children after RTAs. The present results suggest that the impairment associated with PTSD extends beyond the symptoms of the disorder to multiple domains of HRQOL. One may assume that reduced HRQOL is secondary to PTSS but, as noted by Schnurr et al., the effect of PTSD on HRQOL may not simply be unidirectional as suggested by the literature, but symptoms of PTSD and HRQOL may interact mutually over time [29].
Interestingly, based on multiple regression analysis, demographic variables such as age or sex of the child, and medical characteristics such as injury severity and length of hospital stay did not influence long-term HRQOL. This confirms earlier findings with regard to PTSD in children after RTAs [1, 2, 30]. Finally, quality of life ratings at 1 month, although statistically not significant, showed a noticeable tendency to influence HRQOL at 1 year. This suggests that HRQOL in children may show a substantial stability of over time, a fact that has been underlined by Vollrath and Landolt, who showed that child personality, as a stable construct, is an important predictor of HRQOL in children with unintentional injures [9].
Despite the statistical significance of the present findings, regression analysis explained only 32% of the variability in child HRQOL. Thus, variables not included in this study may be of particular importance. Probably, pre-traumatic psychopathology and HRQOL, characteristics of the family, child and parental accident-related appraisals, and the psychological adjustment of mothers and fathers may be other important determinants of HRQOL in children after RTA.
The strengths of the present study are its multidimensional and highly standardized assessment of HRQOL in a prospective design, thus overcoming shortcomings of previous studies. Moreover, the role of various variables for the prediction of HRQOL at follow up was examined using multivariate statistics. Nonetheless, some limitations merit note. First, the sample size was small and the response rate of 59% is an issue potentially limiting the generalizability of the findings; but participants and non-participants were comparable with regard to demographic characteristics. Moreover, the participation rate is consistent with or even better than that of other studies in this field. Still, we do not know whether participants and non-participants systematically differed regarding PTSS or HRQOL. Second, the TACQOL is a generic measure of HRQOL not specifically designed for children after RTA. It may therefore lack sensitivity for specific problems of this group. The TACQOL, however, has been used successfully in children with a variety of different medical conditions and has been shown to be a valid and reliable measure allowing comparison with healthy references. Third, appropriateness of Dutch HRQOL reference data for the present sample of Swiss children can be questioned, but because the Netherlands and Switzerland are European countries with similar social structures, a major cross-cultural bias seems unlikely. This is confirmed by a recent European study in children with chronic conditions that found HRQOL to be very similar in central European countries [31]. A final limitation of the present study is the fact that we had no data on pre-existing psychiatric morbidity in the present patients, which has been proven to be an important risk factor for psychological adaptation after RTA [32]. In spite of these limitations, the present data provide strong evidence for a long-term negative influence of early PTSS on quality of life in children experiencing RTAs.
The present data suggest some possible issues for future research activities and clinical management. Most importantly, based on the present findings it seems possible to identify patients at risk for diminished HRQOL early during recovery by routinely screening for PTSS in the first weeks after the accident. Possibly, and this needs to be studied in future, early treatment of PTSD symptoms will improve quality of life outcomes in children after RTA. As highlighted by Holbrook et al. [12], the return of injured children to pre-injury quality of life depends not only on optimal medical care but also on awareness and timely interventions regarding PTSS.
Footnotes
Acknowledgements
This research was funded by grants from the Gebert Ruef Foundation, the Hugo and Elsa Isler Foundation, and the Anna Mueller Grocholski Foundation. We thank all the children and parents who participated in this study.