
Abstract
A high incidence of trauma among homeless people is well-documented, particularly in the USA [1–3]. Studies have confirmed similarly high rates of trauma among homeless people in Australia [4–8]. Hodder et al. found that 93% of homeless adults in inner Sydney reported at least one major trauma in their lives and many reported multiple traumas [4], [5]. In comparison, 57% of the general Australian population report one lifetime trauma and only 32% report two or more traumas [9].
Studies on trauma among homeless people indicate that traumatic experiences often precede homelessness [7]. Homeless people commonly report a history of childhood physical and sexual abuse [1], but homeless people also report traumatic experiences during homeless episodes [2]. Furthermore, it has been suggested that homelessness itself is traumatic [10–12].
Given the high incidence of trauma and common experience of multiple traumas in the homeless population, one might expect a high prevalence of post-traumatic stress disorder (PTSD) [13]. This is particularly the case because commonly reported experiences in the homeless community are known to increase the risk of PTSD (e.g. a history of childhood trauma, rape, other psychiatric disorders, inadequate support systems, low socioeconomic status) [4], [13], [14]. Surprisingly few studies have assessed PTSD among homeless people. Nevertheless, the few international studies provide compelling evidence that PTSD is very common.
In a large study of homeless adults, North and Smith found that 18% of men and 34% of women met criteria for a lifetime diagnosis of PTSD [14–19]. This finding is consistent with other studies on homeless adults [20–23] and adolescents [3], [24–27]. But all these studies have been conducted internationally.
In Australia to date, no PTSD prevalence studies have been conducted among homeless adults. But Martijn investigated PTSD among homeless youth in Sydney, finding that 36% met criteria for a diagnosis [6]. In comparison, the 12 month prevalence of PTSD in the Australian general adult population is 1.5% [9]. Martijn's study included a small convenience sample of adolescents engaged in services for homeless youth. Hence, the results may not be representative of homeless adults in Australia. Nevertheless, the study indicates that the prevalence of PTSD among homeless youth in Australia is high compared to community samples and is consistent with international findings. Based on these findings, a PTSD prevalence study among homeless adults in Australia is warranted.
It is also important to determine whether PTSD precedes homelessness or is a consequence of being homeless. Studies that have investigated the temporal relationship between PTSD and homelessness are limited, but there is some evidence to suggest that the onset of PTSD commonly precedes the onset of homelessness. North and Smith found that of those with a history of PTSD, 71% of men and 74% of women developed PTSD before the year they first became homeless [14]. This finding was supported in the Martijn Australian study of homeless youth [6]. Of those with PTSD, the index trauma preceded homelessness in 50% of cases and was the precipitant for homelessness in another 30% of cases [6]. Together, these findings indicate that PTSD most often precedes homelessness. Nevertheless, PTSD onset in relation to homelessness has not been investigated in an Australian adult sample. Hence the provision of further local data is of considerable importance.
The aim of the present study was to determine the prevalence and timing of trauma experiences and PTSD among homeless adults in Sydney. The following three hypotheses were made: (i) the majority of homeless adults in Sydney will report a lifetime history of trauma; (2) PTSD prevalence will be higher in the homeless than population estimates in the community; and (3) PTSD onset will precede homelessness more often than it follows homelessness.
Methods
Participants
Participants were homeless adults, aged ≥18 years in Sydney, Australia. A person was considered homeless if they had inadequate access to safe and secure housing [28]. This included people living in situations below a minimum standard of a small rented flat with separate bathroom and kitchen and an element of security of tenure. Three levels of homelessness were identified. Primary homelessness refers to people without conventional accommodation (e.g. people living on the street). Secondary homelessness refers to people who move frequently from one form of temporary shelter to another (e.g. between refuges). Tertiary homelessness refers to people living in boarding houses for ≥13 weeks [28]. Current homeless status was based on where the participant had slept the previous night.
Of 103 people selected to take part, 12 were ineligible because they were either housed or intoxicated (12%) and of the remainder, 21 refused to participate (recruitment rate 77%). Of 70 people interviewed, 14 were ineligible on interview predominantly because they were disorientated or acutely psychotic and unable to answer questions. Fifty-six people completed the interview.
Participants were recruited from eight homeless services, providing accommodation or supportive day services. All 70 participants were paid $20 to compensate them for their time. The University of Sydney Human Research Ethics Committee approved the study.
Materials
A computer-assisted face-to-face structured interview was conducted. The interview provided information on orientation, demography, personal history, medical and psychiatric history, psychopathology, homelessness, and trauma. A timeline was used to determine the participant's recall of when major issues first arose (e.g. homelessness, mental health problems etc.). First homelessness was defined as the first night in which participants had inadequate access to safe and secure housing. Traumas were defined according to Criterion A for PTSD in DSM-IV-TR and codes for onset established the time of onset. Continued trauma from the same perpetrator (e.g. sexual abuse) was considered to be one trauma.
The structured interview consisted of the following measures: (i) Composite International Diagnostic Interview Auto (CIDI-Auto) Version 2.1 Section A (Demographics) and Section K (obsessive–compulsive disorder (OCD) and PTSD) [29], which was administered primarily to diagnose PTSD (the CIDI is a reliable and valid diagnostic interview [30] and the CIDI-Auto is considered an acceptable substitute and gives time of onset of PTSD [31]); (ii) Mini-Mental State Examination (MMSE; Orientation Component) [32], which was used to test orientation to time and place (the MMSE has satisfactory reliability and construct validity [33]); (iii) Depression, Anxiety, Stress Scales (DASS), second edition, Short Form [34], which is a reliable and valid screening tool [35]; (iv) Psychosis Screening Questionnaire, considered an effective screening tool in homeless populations [36]; (v) South Oaks Gambling Screen [37], which is a well-established measure to screen for pathological gambling [38]; (vi) Alcohol Use Disorders Identification Test [39], considered a reliable and valid screening instrument [40]; and (vii) Drug Abuse Screening Test [41], which has sound psychometric properties [42].
Procedure
Participants were randomly sampled at each participating service. The method of random sampling necessarily varied depending on the homeless service. In services that provided accommodation, bed numbers were randomly chosen from an envelope. In services that provided supportive day services only, every third person who accessed the service was asked to participate. In a service that sought out homeless people on the street, the first potentially homeless person at a randomly determined point within the city was chosen. All participants were interviewed in a private and safe room.
All interviews were conducted over a 16 month period from 27 May 2004 to 26 September 2005. The mean duration of interviews was 108 min (SD = 46, range = 30–295 min). Participants were offered a short break mid-way through the interview and took breaks as needed. All information, instructions, questions, and rating scales in the interview were read aloud to counter illiteracy.
Data analysis
The data analysis was performed using SPSS 13.0 (SPSS, Chicago, IL, USA). Prevalence rates of PTSD and OCD were compared to normative data. When possible, clinically significant levels of psychopathology where diagnoses were not made, are reported. Group comparisons involved appropriate parametric and non-parametric t-tests. Assuming a large effect size, the sample size was sufficient for 0.80 power to detect effects with the statistical tests used [43]. Unless stated otherwise, n = 56.
Results
Sample characteristics
Demography and housing history
The mean age of the sample was 38.7 years (SD = 10.8, range = 18–73 years) and 71% were male (four of whom identified themselves as transgender). Aboriginal people were overrepresented in the sample (14%). Most of the sample was born in Australia, had never been married, had at least one child, received a government benefit of some kind, were currently unemployed, had completed ≤10 years at school, and were currently secondary homeless (Table 1).
Subject details
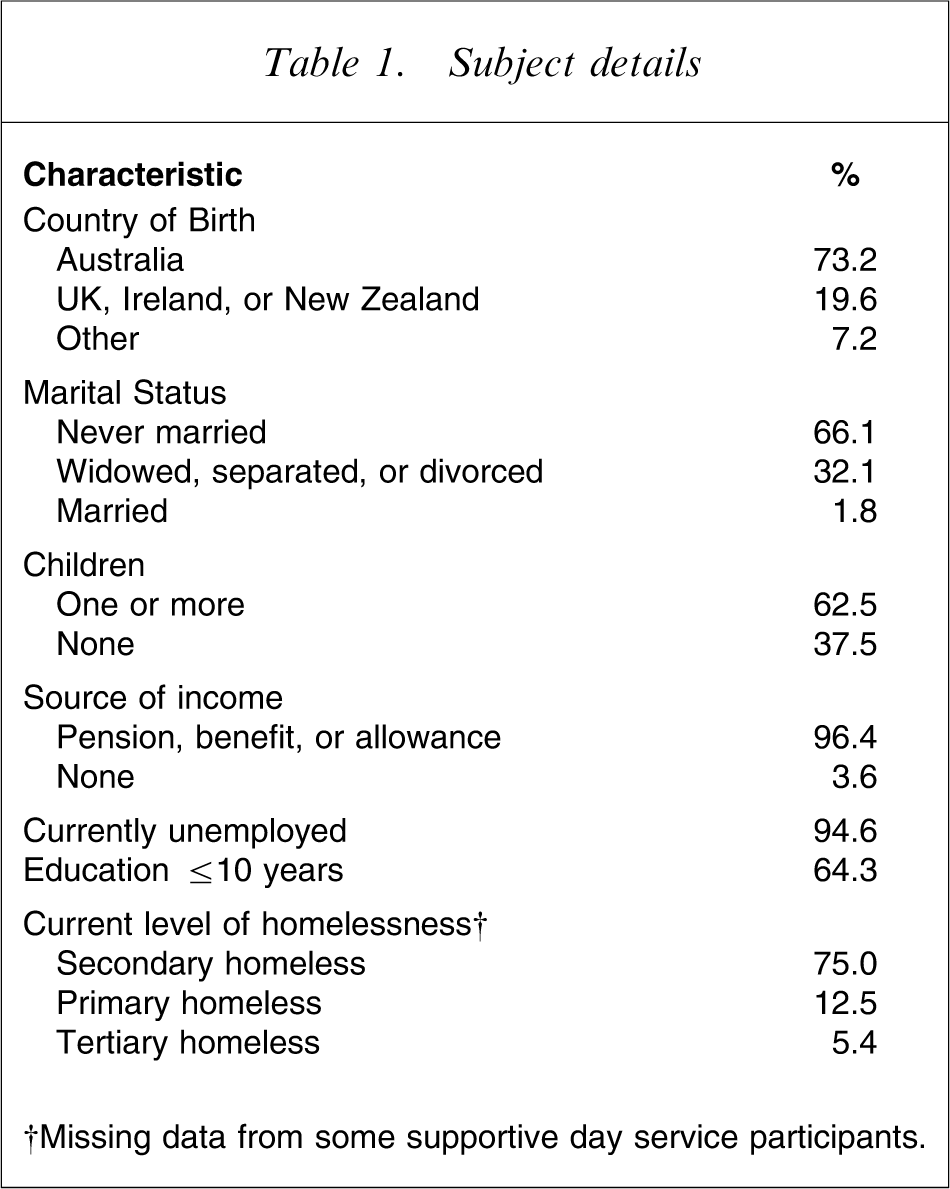
†Missing data from some supportive day service participants.
The mean age of the first homeless episode was 25.7 years (SD = 11.6, range = 4–62 years). Typically, participants had been primary homeless in their first episode (63%) and had remained homeless since (63%). Most had lived with their family of origin beforehand (64%) and first became homeless because it had been necessary to leave due to abuse or a relationship breakdown (50%).
Psychiatric history
Most participants stated that they had seen a mental health worker (86%). Alcohol and depression were the most common reasons for treatment. Most people reported that they had been given a psychiatric diagnosis (61%). Depression was the most common. Only three participants stated that they had been diagnosed with PTSD (5%), although more than half of the sample (54%) had discussed traumatic events with a mental health worker, and for 30% trauma had been the focus of treatment.
Psychopathology
Almost half of the sample screened positive for psychosis (48%, 25/52), although an additional 14/70 were excluded due to disorientation or psychosis. Nineteen per cent were classed as harmful or hazardous drinkers (8/42) and 44% as alcohol dependent (19/43). That represents a total of 64% (27/42) with likely alcohol problems. Drug use (excluding alcohol) was also elevated, with 70% classified as having a substance use problem, abuse or dependence (30/43). Nearly 40% of the sample were probable pathological gamblers (17/42). Rates of depression, anxiety, and stress were very high (Table 2), with upward of 40% (17/42) falling in the extremely severe range on the DASS. Interestingly, 19% of the sample met criteria for a current diagnosis of OCD (8/42).
DASS Short Form results (n = 42)
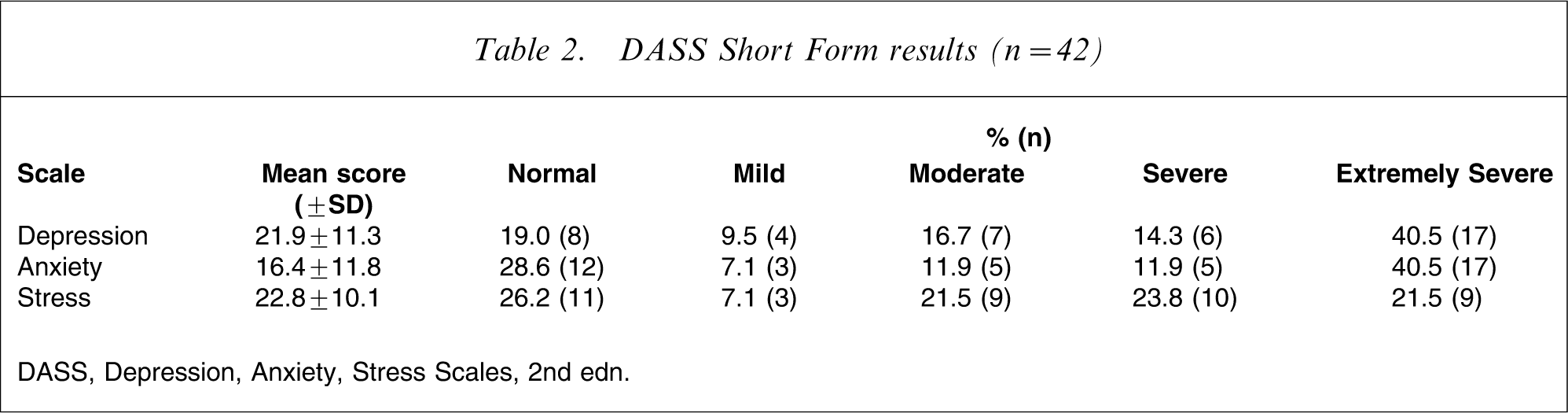
DASS, Depression, Anxiety, Stress Scales, 2nd edn.
Trauma experience
Trauma incidence
All but one participant stated that they had experienced at least one traumatic event in their lifetime (98%, 55/56). The vast majority had experienced two or more traumatic events (93%, 52/56). Participants reported on average six trauma experiences. Trauma in childhood was common. The mean age of the first trauma experience was 12.4 years (SD = 9.0, n = 55). Most participants experienced trauma prior to 16 years old (71%, 40/56).
Types of trauma
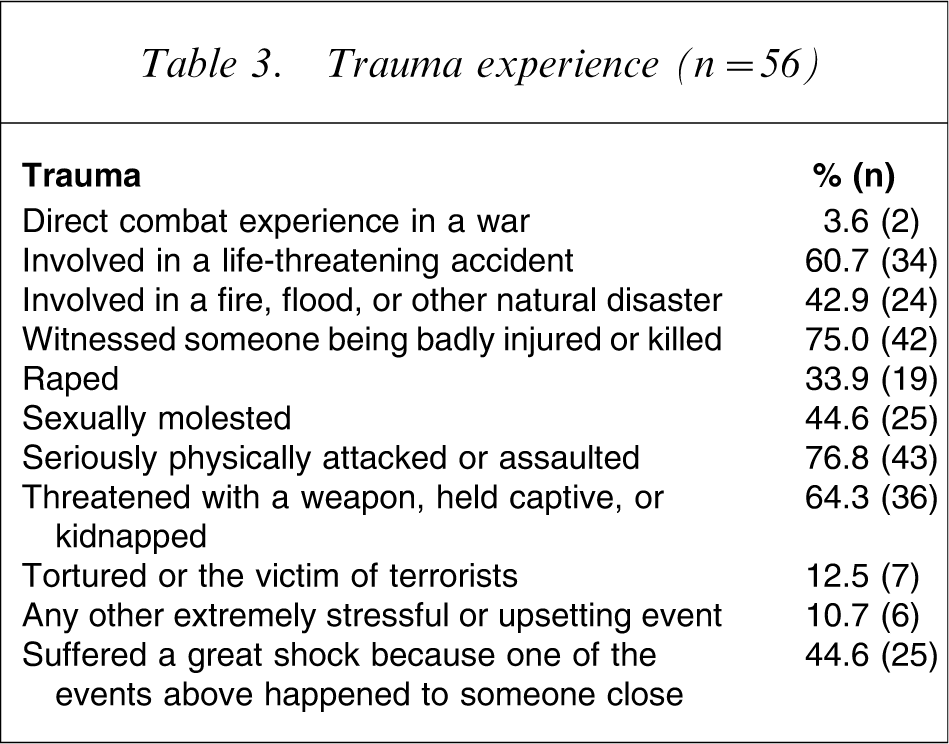
The types of trauma experienced are reported in Table 3. Being seriously physically attacked or assaulted was the most common trauma, closely followed by witnessing someone being badly injured or killed. Although rates of rape and sexual molestation were lower, 23% (13/56) of the entire sample considered these to be their most traumatic experience.
Trauma experience (n = 56)
Trauma and homelessness
In 82% of cases (45/55) the first trauma occurred before the first homeless episode and in another 4% of cases (2/55) the first trauma and the first homeless episode coincided. The first trauma was, on average, 13.5 years before first homelessness (SD = 12.6, n = 55). When asked if being homeless was a traumatic experience, most participants considered that it was (60%, 25/42); a common reason for this being fear due to lack of security.
Post-traumatic stress disorder
Prevalence
According to either DSM-IV or ICD-10, 79% of the sample met criteria for a lifetime diagnosis of PTSD (44/56); of those, half currently met criteria (22/44; i.e. symptoms in the previous 6 months; Table 4). The 12 month prevalence of PTSD was slightly higher (41%, 23). There were no differences in rates of PTSD between men and women (Cramér's V = 0.1, p = 0.74). There was some discrepancy in the diagnoses between DSM-IV and ICD-10, with 32% of the sample (14/44) being diagnosed by one set of criteria but not by the other (Table 5).
PTSD lifetime diagnosis (n = 56)
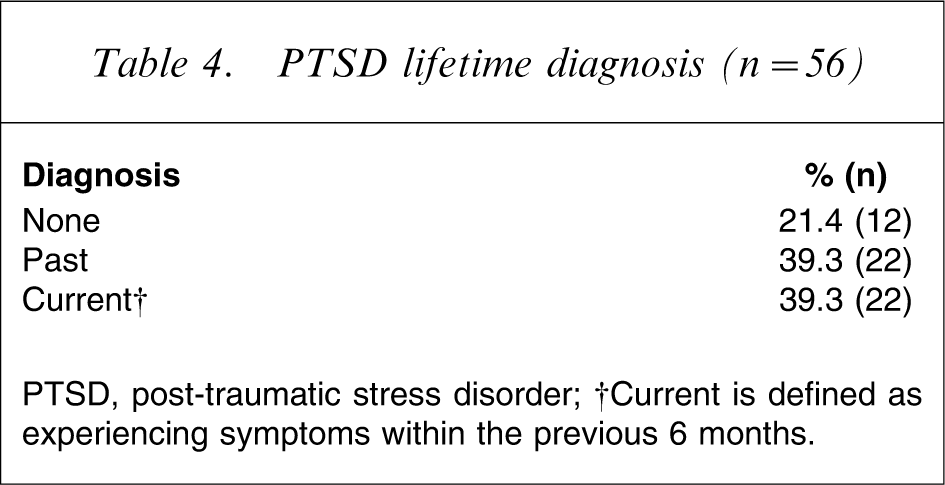
PTSD, post-traumatic stress disorder.
†Current is defined as experiencing symptoms within the previous 6 months.
PTSD lifetime diagnosis: DSM-IV vs ICD-10 (n = 56)
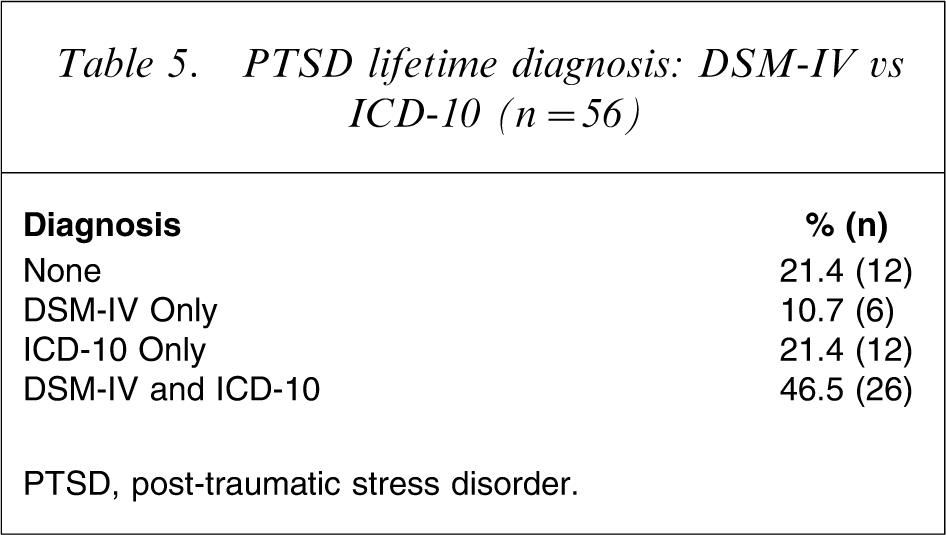
PTSD, post-traumatic stress disorder.
Comorbidity
Of those who met criteria for current PTSD: 55% (12/22) screened positive for psychosis; 69% (11/16) scored in the severe or extremely severe range for depression; 50% (8/16) scored in the severe or extremely severe range for anxiety; 31% (5/16) met criteria for a current diagnosis of OCD (i.e. symptoms in the previous 6 months); 56% (9/16) scored in the severe or extremely severe range for stress; 56% (9/16) were probable pathological gamblers; 63% (10/16) screened positive for harmful or hazardous drinking or alcohol dependence; and 88% (15/17) screened positive for a substance use problem, abuse or dependence. Nevertheless, for each of these variables there were no significant differences between those with and those without current PTSD.
PTSD and homelessness
Overall it was found that of those with a lifetime diagnosis of PTSD, in 59% of cases (26/44) PTSD onset occurred before the age of first homelessness and in 11% of cases (5/44) PTSD onset occurred at the age of the first homeless episode. PTSD onset was, on average, 4.9 years before the age of first being homeless (SD = 14.0). Of those who met criteria for current PTSD and were asked if being homeless was a traumatic experience, 81% (13/16) considered that homelessness was traumatic.
Discussion
The primary aim of the present study was to determine the prevalence and timing of trauma and PTSD among homeless adults in Sydney. It was predicted that the majority of participants would report a lifetime history of trauma and that PTSD prevalence would be higher than estimates in the general population. We also predicted that PTSD onset would precede homelessness more often than not. All three hypotheses were confirmed.
Despite careful attention to the methodology, there were a number of limitations that should be borne in mind. First, we did not use a control group of age-matched or low-income housed participants [20], [24], [44–46]. Nevertheless, in the present study the rates of trauma and PTSD were so high, that it is likely that a domiciled control group would have only accentuated this finding. Another limitation of the study was that due to the cross-sectional design, it was not possible to draw a conclusion regarding causality between trauma and homelessness. Nonetheless, the fact that PTSD precedes homelessness in the majority of cases, means that homelessness causing the high rates of PTSD is unlikely. In addition, the sample size was small and participants were recruited from a convenience sample of locations. While we assessed a range of other psychopathology, we assessed only diagnoses for PTSD and OCD and both were elevated. But we cannot provide diagnoses for other disorders. Nonetheless, it is worthwhile to highlight that the high levels of PTSD and trauma were observed in the context of extremely high levels of psychopathology across all variables measured within the sample, consistent with the extensive literature [5]. Because psychopathology was measured using questionnaires, however, it is likely that they would overestimate the presence of disorders in this sample.
These limitations not withstanding, the study was the first to examine PTSD among homeless adults in Australia and it had a number of strengths. Participants were sampled from a range of homeless services. Every attempt was used to approximate random sampling to ensure a representative sample. Consequently, the sample included primary, secondary, and tertiary levels of homelessness. This is particularly advantageous because most homelessness studies rely on samples from shelter populations, making it difficult to generalize the results [47]. An additional strength was that extensive in-depth interviews included measures with sound psychometric properties.
All but one of the participants had experienced a traumatic event (98%), with the vast majority having experienced more than one traumatic event (93%). Participants reported an average of six traumas. These rates are considerably higher than in the Australian population, in which 57% report one lifetime experience of trauma and only 32% report at least two traumas [9]. These results are consistent with other homeless studies conducted overseas [2] and in Australia, among adult samples [4], [5], [8] and adolescent samples [6], [7].
In the current sample the lifetime prevalence of PTSD was 79%. The 12 month prevalence was 41%, which is 27-fold higher than in the Australian community [9]. Other studies have found elevated rates of PTSD in homeless youth in Australia [6] and overseas, in both homeless adults [20–23] and adolescents [3], [24–27]. Nonetheless, the prevalence rates in the present study are surprisingly high in comparison to previous studies, for example North and Smith [14]. One explanation for this is that diagnoses were made according to either DSM-IV or ICD-10. There were discrepancies, with 32% of the sample being diagnosed by one set of criteria but not by the other. Discrepancy between DSM-IV and ICD-10 diagnoses of PTSD has been noted previously and arises from the differing sets of criteria [48]. In the current study 11% of cases met DSM-IV criteria only and 21% of cases met ICD-10 criteria only. Considering DSM-IV diagnoses alone, the lifetime prevalence rate in the current study drops from 79% to 57%, which is in keeping with international findings and still well above community estimates.
In addition to finding high rates of trauma and PTSD, the study also found that in 70% of cases, PTSD onset preceded or coincided with first homelessness. In fact, PTSD onset occurred, on average, nearly 5 years before homelessness. The finding that PTSD more often precedes homelessness is consistent with one large study on homeless adults in the USA [14] and a small study on Australian homeless youth [6].
It is also noteworthy that this sample, like other homeless research, was characterized by a range of psychological problems. There was a high prevalence of psychosis, alcohol and other drug use problems, probable pathological gambling, depression, anxiety, and stress. These high rates of comorbidity can be explained generally by studies on the prevalence of mental illness in homeless individuals, which show that rates are much higher than in community samples [47], [49]. The very high rates of psychosis were also documented in other Australian marginalized samples [50].
It can be concluded from this study that homeless adults in Sydney report exceptionally high rates of multiple trauma. The prevalence of PTSD in this group is 27-fold higher than in the Australian population, and PTSD more often precedes homelessness than follows it. It is surprising then that so few in the sample (5%) reported that they had been diagnosed with PTSD, even though approximately half reported discussing their trauma history in treatment. But the wide-ranging psychological difficulties experienced in this sample emphasize the fact that while trauma is known to be a causal factor in PTSD, the experience of multiple trauma is associated with a broad range of psychopathology, including psychosis, drug and alcohol and other psychological problems.
It seems that the experience and consequences of trauma are frequently overlooked among the homeless in our society. This leads to the unfortunate situation in which traumatized individuals find themselves in a re-traumatizing environment (i.e. homelessness), creating a vicious cycle of declining mental health.
The present results suggest that finding accommodation for homeless people is likely only to be part of the solution. The homeless adults who we interviewed had multiple mental health needs and a long history of repeated trauma that, without treatment, are likely to impede their ability to maintain housing in the future. Services for homeless people need to take these serious mental health problems into account. Importantly, it seems that PTSD may go underrecognized among the homeless, and those involved in their mental health care should routinely assess for the presence of PTSD.
Footnotes
Acknowledgements
The authors wish to thank Professor Alex Blaszczynski for his valuable contribution to this research study. This research was supported by Mission Australia, Vincentian Village, and the Women and Girls’ Emergency Centre. Participants were paid with funds acquired in a Postgraduate Research Grant awarded to KT by University of Sydney.