
Abstract
Objective:
To evaluate the relative efficacies of trauma-focused cognitive behavior therapy and problem-solving therapy in treating post-traumatic stress disorder in children affected by civil conflict in Aceh, Indonesia.
Method:
A controlled trial of children with post-traumatic stress disorder (N = 64) randomized children to either five individual weekly sessions of trauma-focused cognitive behavior therapy or problem-solving therapy provided by lay-counselors who were provided with brief training. Children were assessed by blind independent assessors at pretreatment, posttreatment and 3-month follow-up on post-traumatic stress disorder, depression and anger, as well as caregiver ratings of the child’s post-traumatic stress disorder levels.
Results:
Intent-to-treat analyses indicated no significant linear time × treatment condition interaction effects for post-traumatic stress disorder at follow-up (t(129.05) = −0.55, p = 0.58), indicating the two conditions did not differ. Across both conditions, there were significant reductions in post-traumatic stress disorder on self-reported (t(131.26) = −9.26, p < 0.001) and caregiver-reported (t(170.65) = 3.53, p = 0.001) measures and anger (t(127.66) = −7.14, p < 0.001). Across both conditions, there was a large effect size for self-reported post-traumatic stress disorder (cognitive behavior therapy: 3.73, 95% confidence interval = [2.75, 3.97]; problem-solving: 2.68, 95% confidence interval = [2.07, 3.29]).
Conclusions:
These findings suggest that trauma-focused cognitive behavior therapy and problem-solving approaches are comparably successful in reducing post-traumatic stress disorder and anger in treating mental health in children in a post-conflict setting. This pattern may reflect the benefits of non-specific therapy effects or gains associated with trauma-focused or problem-solving approaches.
War and civil conflict affect many countries across the globe, with the majority of affected people living in low- and middle-income countries (LMICs) (Brundtland, 2000). There is considerable evidence of increased rates of psychological problems in children who have survived war and civil conflict (Attanayake et al., 2009; Barenbaum et al., 2004; Pat-Horenczyk et al., 2009; Stichick, 2001), with rates of post-traumatic stress disorder (PTSD) and depression being significantly higher in war-affected communities than in communities with no recent history of conflict (Priebe et al., 2010; Steele et al., 2009). More than 80% of the world’s population of young people live in LMICs, and as a result, mitigating the effects of war-related trauma has become a major global public health issue (Collins et al., 2011; World Health Organization [WHO], 2015).
A number of evidence-based child-focused interventions for post-traumatic stress have been validated in the developed world (Chemtob et al., 2002; Cohen and Mannarino, 2008; Stein et al., 2003), with trauma-focused cognitive behavioral therapy (CBT) the treatment of choice for childhood PTSD (Gillies et al., 2012). Numerous attempts have been made to apply this approach in LMICs, and meta-analytic analyses indicate that trauma-focused therapy is effective in reducing PTSD symptoms in children following mass violence in poorly resourced settings (Morina et al., 2017). However, access to such evidence-based treatments is restricted in low resource settings where civil conflicts are disproportionately concentrated (De Jong, 2014; Jakobsen et al., 2013; WHO, 2015).
To address the need for better access to mental health services in LMICs, recent efforts have emphasized task-shifting, in which non-specialists are trained to deliver mental health interventions (Patel et al., 2011). In most task-shifting protocols, lay-counselors who have no prior mental health training or experience are trained in a specified intervention following a strict protocol. Several studies have adopted a task-shifting approach to evaluate the efficacy of psychological interventions in low resource settings with adults (Bolton et al., 2014; Murray et al., 2014; Patel et al., 2010; Rahman et al., 2008) and children (Catani et al., 2009; Jordans et al., 2010; Thabet et al., 2005; Tol et al., 2008). In the case of children, a common approach has been to utilize classroom settings to deliver psychosocial interventions, which has demonstrated moderate effects in reducing PTSD symptoms in Indonesian primary school–aged children when compared to a wait-list control (Tol et al., 2008). This evidence is mixed, however, insofar as the same intervention did not impact psychiatric symptoms in Nepalese children (Jordans et al., 2010). Among Ugandan adolescent girls, group Interpersonal Psychotherapy was found to be more efficacious in reducing depressive symptoms compared with creative play (Bolton et al., 2007). Finally, a trauma and grief-focused psychotherapy program significantly reduced grief symptoms in Bosnian children (Layne et al., 2008), but had no effect on adolescents living in refugee camps in Gaza (Thabet et al., 2005).
Although group-based interventions have the benefit of including more children with fewer resources, they may not be appropriate for delivering exposure-based strategies because activating memories of traumatic experiences can be distressing and need to be dealt with in the context of individual therapy. Exposure-based strategies are principal components of trauma-focused CBT, which is recommended by most treatment guidelines (Foa et al., 2009). Catani and colleagues compared KidNET, a child-friendly trauma-focused individual treatment that incorporates a narrative adaptation of imaginal exposure, with a meditation–relaxation program among Tamil youths exposed to both the war and the tsunami. Both treatments were found to significantly reduce PTSD symptoms and functional impairment at 1 and 6 months post-intervention. While these results are promising, treatments were delivered in the immediate aftermath of the tsunami and the authors could not control for spontaneous remission or non-specific benefits of intervention, as there was no wait-list control condition.
One of the contentious issues in the field of post-conflict mental health is the extent to which one should address traumatic stress or the mental health effects of current stressors. Some models have noted the important role of current stressors in mental health in post-conflict settings and have emphasized the importance of targeting effects of ongoing stressors rather than focusing on past traumatic experiences (Miller and Rasmussen, 2010). Daily stressors include poverty, unemployment, lack of law and order and fragmented social relationships. These factors can increase the risk of mental health conditions (Patel et al., 2009). Accordingly, some intervention programs have attempted to address daily stressors that are commonplace in conflict-affected settings (Fernando et al., 2010; Rahman et al., 2016).
Although trauma-focused and current-centered approaches have been shown to be effective in improving mental health in post-conflict settings, these two approaches have not been directly compared. Accordingly, this study sought to extend the current evidence by assessing the relative efficacies of trauma-focused and problem-solving (PS) interventions delivered by lay-counselors in LMIC with children exposed to conflict. The study was conducted with primary school–aged Acehnese children who were exposed to the civil conflict and living in rural areas facing ongoing adversity, including poor education, poverty and unemployment. Primarily, the study was interested in the efficacy of CBT and PS counseling in reducing symptoms of PTSD, depression and anger. This study focused on these outcomes because they emerge as primary psychological disturbances in post-conflict settings (Brooks et al., 2011; Elbert et al., 2009; Silove et al., 2009). This superiority trial hypothesized that trauma-focused CBT would result in greater reductions in PTSD, depression and anger than PS because of its proven efficacy in youth affected by mass violence in low- and middle-income settings (Morina et al., 2017).
Method
Setting
Aceh suffered a protracted civil war from the 1970s up until the 2004 south-east Asian tsunami that devastated much of the Indonesian province. Motivated by the goal of achieving independence from Jakarta, the conflict was largely dominated by guerilla warfare that was most fierce during the 1990s. As a result of the fatalities arising from the conflict, it is estimated that 15,000-20,000 children were orphaned as a result of the fatalities that occurred in the conflict. Furthermore, Renner (2006) has estimated that approximately 120,000 people were forced to evacuate their homes.
Participants
Participants included conflict-exposed children involved in an after-school program operated by the non-government organization, Centre Mulia Hati (CMH). Inclusion criteria were boys or girls aged between 7 and 14 years, living in the region affected by Aceh’s civil conflict and satisfying criteria for probable PTSD (based on the child’s self-reported University of California, Los Angeles [UCLA] PTSD Reaction Index [RI]), based on the child’s response to an interviewer-administered PTSD self-report measure. Exclusion criteria were severe mental disorders (e.g. early-onset psychosis, drug and/or alcohol abuse, imminent suicide risk). No children were excluded on these criteria. Table 1 presents the sample characteristics of children. All primary caregivers of children invited into the program completed written informed consent approved by the University of New South Wales Human Research Ethics Committee. Power calculations indicated a minimum sample size of 70 participants per treatment arm using the test for paired means to achieve a moderate effect (d = 0.5) on the UCLA PTSD-RI (power = 0.80, alpha = 0.05, two-sided). Participants were initially recruited into the trial on 1 March 2011. This study did not attain its desired sample size, however, due to local authorities shutting the study down after 64 participants had been enrolled. The political unrest occurring in Aceh at the time of the study caused suspicion of Western activities in the region, and as a result, the researchers were forced to leave the region with little warning and recruitment was terminated on 19 March 2012. The final sample resulted in 64 children of mean age being randomized to CBT (18 males, 14 females) or PS (15 males, 17 females). The groups did not differ in terms of mean age (10.50 years, standard deviation [SD] = 0.93, vs 10.25 years, SD = 1.16), t(63) = 0.47, p = 0.64.
Participant characteristics.
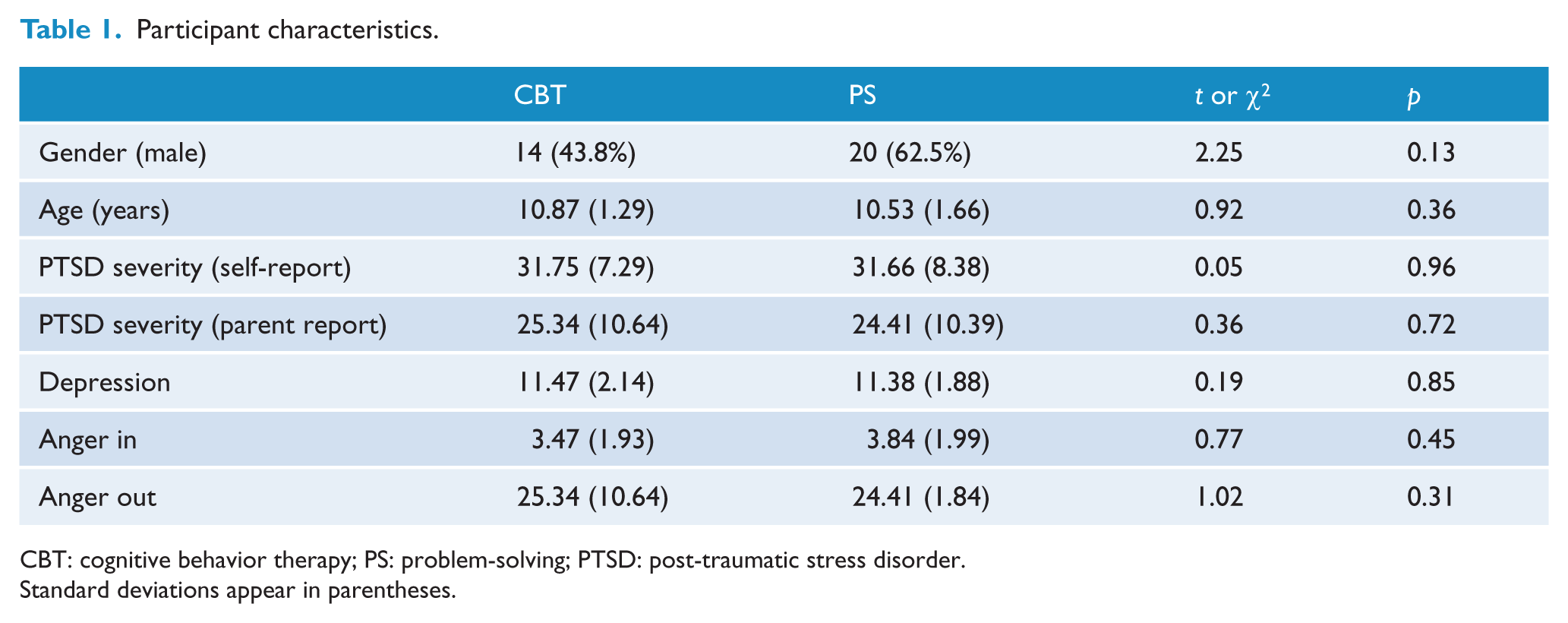
CBT: cognitive behavior therapy; PS: problem-solving; PTSD: post-traumatic stress disorder.
Standard deviations appear in parentheses.
Measures
All measures were completed in interview format due to low literacy levels.
Trauma exposure and PTSD
To capture the extent of children’s exposure to Aceh’s civil conflict, children were asked a series of questions (e.g. ‘did something bad happen to you in the conflict?’, ‘did someone close to you die in the conflict?’). Children reported a range of traumatic events, including being separated from caregivers (37.4%), witness someone being killed or injured (29.3%), having a family member killed (35.4%) or having a close friend killed (32.3%). In reference to these events, the UCLA PTSD-RI (Part III) was used to determine a possible PTSD diagnosis, one of the most widely used instruments for the assessment of traumatized children (Steinberg et al., 2004). Items are categorized to reflect Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) PTSD diagnostic clusters. The measures have demonstrated sound psychometric properties in other settings and have been applied in many cross-cultural settings (Steinberg et al., 2013). Caregivers also completed the UCLA PTSD-RI for their child, and these were used as a secondary outcome measure. Overall, the correlation between child and caregiver reports was low (e.g. at follow-up the correlation between total PTSD scores was 0.36, p = 0.005).
Depression
The Children’s Depression Inventory (CDI; short form) is a 10-item self-rated symptom-oriented scale for children aged 7–17 years (Kovacs, 1992). Children select from three possible responses which best describes how they have been thinking and feeling in the preceding 2 weeks. The CDI has well-established psychometric properties, including sound test–retest reliability, internal consistency and construct validity from a range of cultural populations (Kovacs, 1985, 1992; Yoo et al., 2014).
Anger
Anger was assessed with the Anger Expression Scale for Children (Steele et al., 2009). In all, 20 of the 26 items were included in this study, selected because they assess characteristics of anger expression (anger in, anger out and anger control). This study omitted items related to trait anger in order to not overburden children. The scale utilizes a 4-point Likert scale (almost never to almost always) and is good for the specified four factors, has strong internal consistency and has moderate test–retest reliability (Steele et al., 2009).
Procedure
Randomization to either CBT or PS was conducted at the University of New South Wales, Australia, independent of the study team. Caregivers and children were informed and consented to the randomization procedure. Figure 1 summarizes the participant flow. Initial assessments were conducted at pretreatment and prior to randomization by assessors who were independent and blind to the treatment condition. Posttreatment and 3-month follow-up assessments were completed by treatment-independent assessors. Six received 4-day training in assessment instruments and techniques; to maintain blindness of the assessors, they were kept separate from the lay-counselors. Although the study was terminated prior to attaining the desired sample size, all enrolled children completed the programs and the posttreatment and follow-up assessments. Adverse reactions were monitored and recorded if there was a noted exacerbation of symptoms requiring removal from the program.
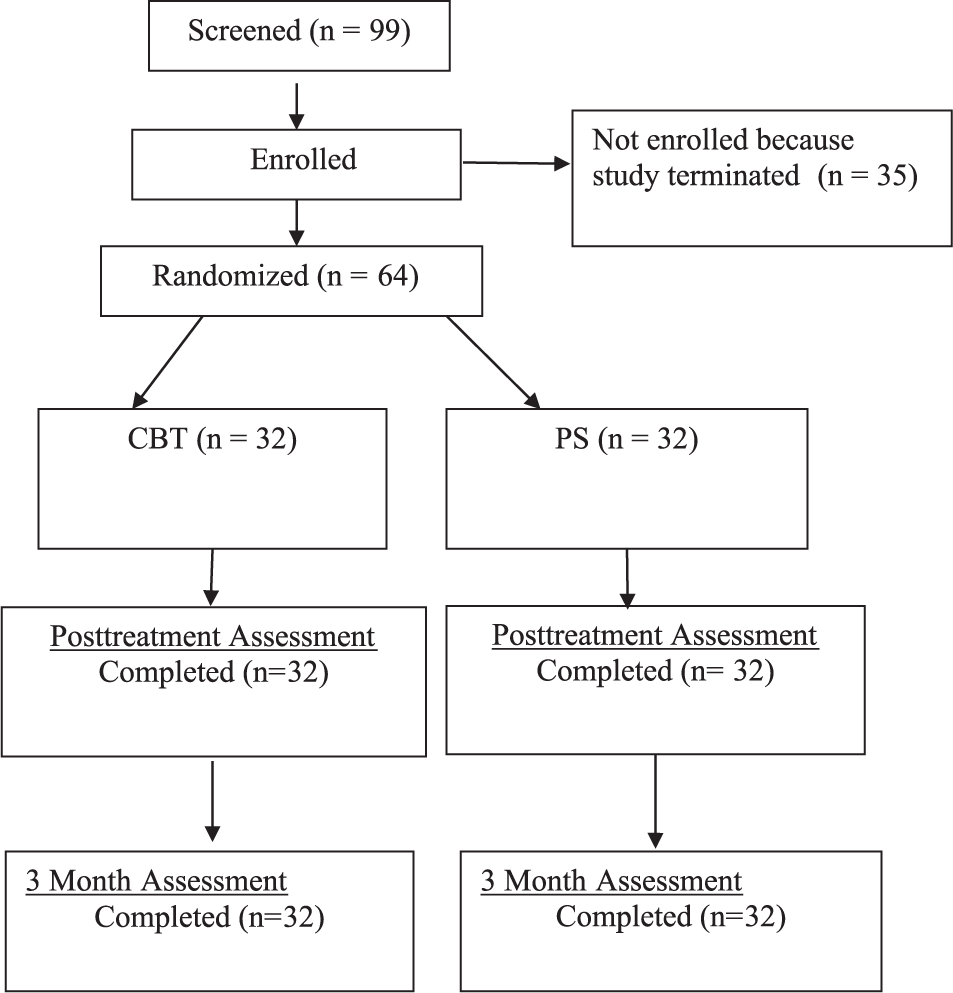
Participant Flowchart.
Treatment conditions
Treatment comprised five weekly 1-hour individual sessions with children and one 1-hour caregiver session. Treatment was delivered by four CMH lay-counselors who had high school education and had worked as part of the child development team of CMH. They did not have any formal mental health training. Lay-counselors received training in CBT and PS counseling over a 2-week period by K.D., followed by 12 weeks of practice with cases (equivalent to one school term). Training involved being aware of adverse reactions or excessive distress during the program. Lay-counselors received weekly Skype supervision (conducted by K.D.) as well as weekly peer supervision and team meetings. All lay-counselors provided each type of treatment, although they only delivered one type of treatment at any one time. Training communicated to all counselors that both treatments were equally effective.
All CBT and PS child sessions presented material in a child-friendly manner and included activities and games. Children were given a workbook that included worksheets they completed with lay-counselors recording their progress. Standardization and treatment fidelity were maintained by having the lay-counselors play videos depicting the key information in each session (i.e. cartoon pictures designed for the treatments with a verbal narrative). The videos depicted a child who witnessed many horrific events during the conflict and was experiencing post-traumatic stress symptoms. When introducing a new strategy, the video was played to the child on portable DVDs, showing how the strategy was used to address the child’s problems. The counselor was instructed to follow each video with discussion with the child about their understanding of the video’s content, how they would apply the educational content of the video to themselves, and to then begin a discussion of how to apply the skills imparted by the video to the child. For example, one video presented a scenario of a child talking about things he avoided and then tried to resume after the conflict; the counselor would encourage the child to identify their avoidance patterns and develop strategies to overcome them. Treatment fidelity was also self-monitored by lay-counselors who followed a basic session-by-session checklist.
CBT
Sessions 1, 2 and 4–6 were child sessions, and Session 3 was conducted with the primary caregiver. Session 1 comprised education about trauma reactions and introduced a basic stress management strategy. The second session introduced basic cognitive restructuring to address maladaptive thoughts believed to be maintaining children’s post-traumatic stress reactions. Specifically, treatment taught children how to investigate the accuracy and helpfulness of thoughts. Following the caregiver session, children commenced graded in vivo exposure to modify avoidance behaviors and fear-based thinking.
Sessions 5 and 6 applied a modified version of prolonged exposure to assist children in processing trauma memories. Based on testimony therapy and Narrative Exposure Therapy, children constructed a chronological narrative of their life with the assistance of their lay-counselor. Significant life events were discussed with particular attention given to events that demonstrate the child’s personal strengths and resilience. The traumatic event provoking the most distress in the child was then discussed in detail in a manner commensurate with prolonged exposure. The aim is to help the child process the event as well as gain a sense of mastery over it and their emotional reaction to the event upon recalling it. Unlike other similar approaches, the narrative component also reviewed historical elements of the child’s narrative, including their family’s history as well as that of their wider community and province. The rationale of including a historical component in the narrative was to help the child appreciate the context of the stressful and traumatic events they have experienced in their life. Where appropriate, this information also served to provide children with evidence that they are not the cause of or to blame for such events, such as family conflict.
Session 6 reviewed the narrative and conducted a prolonged exposure to a second trauma or the same trauma if only one event was identified by the child. The second half of the last session includes a relapse prevention component and a graduation ceremony with the child.
In Session 3, the primary caregiver was educated about child trauma reactions, the treatment their child was receiving and adaptive caregiver strategies.
PS counseling
The same psychoeducation component from CBT was delivered in Session 1 of PS. This session also introduced the PS method. PS focused on distinguishing between controllable and uncontrollable problems, brainstorming potential solutions, identifying strategies that were most achievable and assisting the child to try these strategies. Session 2 reviewed the method and assisted the child in applying it to a current child-identified problem. This structure was repeated in Sessions 4–6, with the final session also including a relapse prevention component. As in CBT, one primary caregiver attended Session 3. This session mirrored the CBT caregiver session with the exception of education about the treatment their child was receiving.
Data analysis
We used hierarchical linear models (HLM) to investigate the impact of the interventions. All analyses were conducted in SPSS version 2.1. We conducted intent-to-treat analyses as HLM allows the number of observations to vary between participants and effectively accommodates missing data (Raudenbush, 2001). Hierarchical linear modeling utilizes a multilevel data structure. The Level 1 model represents within-participant change over time. In this study, the time variable encompassed the pretreatment assessment, the posttreatment assessment (which took place 6 weeks after treatment commenced) and the follow-up assessment (which took place 3 months after treatment commenced). The Level 2 model allows for the prediction of variation in within-participant change over time, and encompasses between-person variables such as treatment group (coded as 1 = CBT and 2 = PS).
We used restricted maximum likelihood estimation with robust standard errors and an autoregressive covariance structure. The use of an autoregressive covariance structure reflects the assumption that correlations between measurements close in time are greater than correlations between measurements further away in time. The first set of analyses focused on pre- to posttreatment change in symptoms. We first tested Level 1 models (i.e. predicting dependent measures using Time) which included both fixed and random intercepts and slopes. The inclusion of random intercepts and slopes reflects the conservative assumption that these parameters vary significantly between individuals. For pre- to post-analyses, we modeled only a linear representation of time. For pre- to follow-up analyses, we modeled both linear and quadratic representations of time. In the second step, we tested multilevel models that encompassed (1) the Level 2 variable representing treatment condition and (2) the interaction between the treatment condition variable and the linear time variable. This allowed us to evaluate whether Level 2 variables affected changes over time in the dependent measures. Fixed-effects parameters were tested with the Wald test (t-test) and 95% confidence intervals (CIs). Outcome measures are reported for both the main (symptom change over time) and interaction (difference over time between the two treatment arms) effects.
Results
There were no reported adverse events during the trial. No children reported, or were observed to experience, marked distress or other adverse reactions to the programs.
Table 2 provides the least-square mean scores for children’s reports of PTSD, depression, anger and caregivers’ reports of PTSD. There were no significant time × treatment interaction effects for PTSD at posttreatment (t76.04 = 0.04, p = 0.97) or follow-up (t(129.05) = −0.55, p = 0.58). There were also no significant time × treatment interaction effects for depression at posttreatment (t(62.47) = −0.61, p = 0.54) or follow-up (t(128.20) = −0.56, p = 0.58). Similarly, there were no significant time × treatment interaction effects for anger at posttreatment (t(118) = 0.35, p = 0.73) or follow-up (t(126.69) = 0.51, p = 0.61). In terms of caregivers’ reports of childhood PTSD, there were no significant time × treatment interaction effects at posttreatment (t(99.32) = −0.29, p = 0.77) or follow-up (t(126.46) = 0.07, p = 0.95). These findings indicate that the two conditions did not differ in their impact on any of the mental health outcomes.
Estimated mean scores for outcome measures and relative effect sizes.
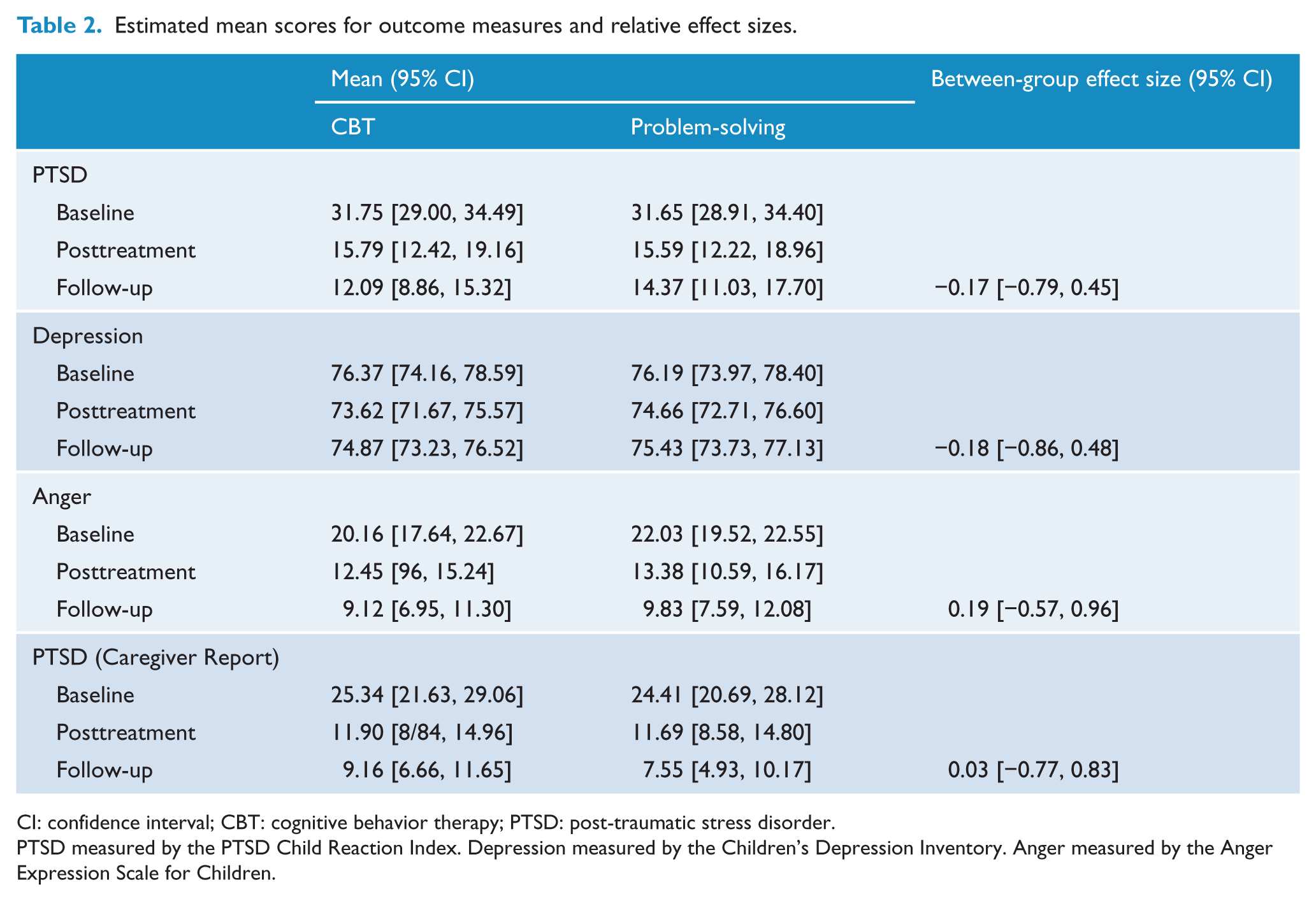
CI: confidence interval; CBT: cognitive behavior therapy; PTSD: post-traumatic stress disorder.
PTSD measured by the PTSD Child Reaction Index. Depression measured by the Children’s Depression Inventory. Anger measured by the Anger Expression Scale for Children.
Analyses revealed that across both conditions, PTSD decreased significantly from pre- to posttreatment (t(76.04) = −7.43, p < 0.001) and follow-up (t(131.26) = −9.26, p < 0.001). There was also a significant positive quadratic slope (t(172.83) = 5.26, p < 0.001), which suggested that this decrease attenuated over time. Analyses revealed that across both conditions, depression did not decrease significantly from pre- to posttreatment (t(62.47) = −1.07, p = 0.29) and follow-up (t(129.14) = −0.91, p = 0.36), nor was there a significant quadratic effect (t173.28 = 1.05, p = 0.30). Across both conditions, anger decreased significantly from pre- to posttreatment (t118 = −4.52, p < 0.001) and follow-up (t(127.66) = −7.14, p < 0.001), as well as a significant positive quadratic slope (t(171.28) = 2.88, p = 0.005), which suggested that this decrease attenuated over time. Caregivers’ reports indicated that PTSD in the child decreased for both conditions at posttreatment (t(99.32) = −6.21, p < 0.001) and follow-up (t(127.92) = −7.94, p < 0.001), exhibiting a significant quadratic effect (t(170.65) = 3.53, p = 0.001).
As Table 2 indicates, the relative effect sizes at follow-up comparing the two arms of the trial were small or non-evident. In contrast, Table 3 indicates that across both conditions, there were large effects from pretreatment to follow-up for self-reported PTSD, anger and caregiver reports of child PTSD. For example, both conditions reported large effect sizes for self-reported PTSD (CBT: 3.73, 95% CI = [2.75, 3.97]; PS: 2.68, 95% CI = [2.07, 3.29]).
Within condition baseline–follow-up effect sizes.
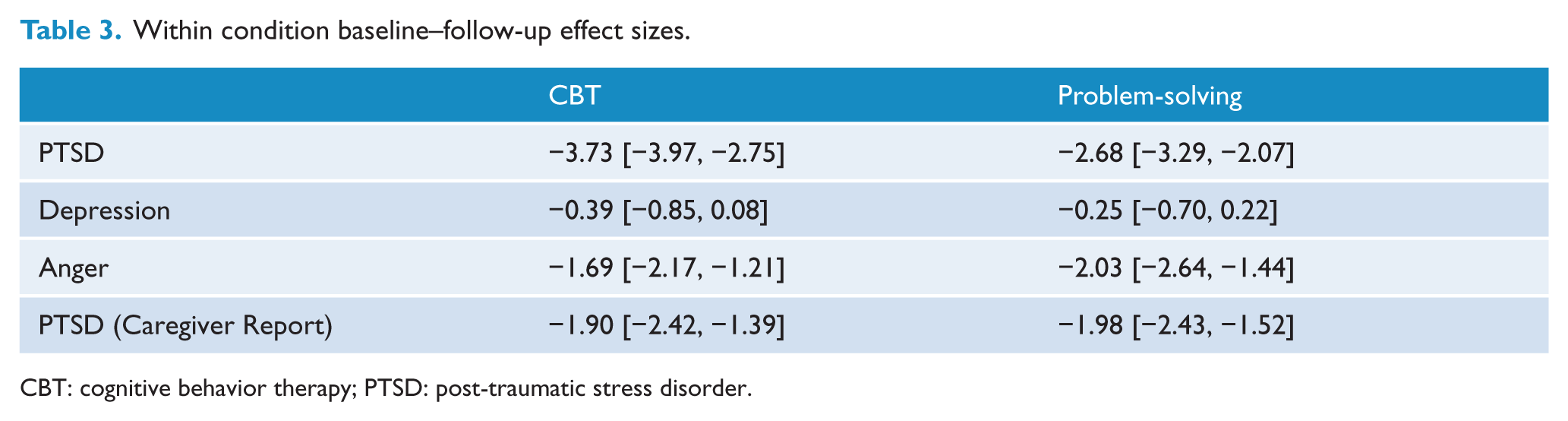
CBT: cognitive behavior therapy; PTSD: post-traumatic stress disorder.
Discussion
The major finding of the study was that CBT and PS resulted in comparably large decreases in PTSD and anger. The effect sizes from pretreatment to follow-up on PTSD were large and underscore the impact of the interventions on PTSD. It is noteworthy that PTSD symptoms decreased markedly across conditions according to both the children’s own reports and the caregiver reports. The confirmation by caregiver reports of significantly decreased PTSD strongly reinforces the conclusion that these interventions impacted both the child’s experienced symptoms and their levels of distress as observed by caregivers. In this context, it is worth noting that the mean score on the UCLA PTSD-RI in the current sample (M = 31.7) is higher than the mean score reported on nationally representative children exposed to multiple traumatic events and attending clinics in North America (M = 27.3) (Steinberg et al., 2013), suggesting that the interventions were beneficial for children with marked levels of PTSD symptoms. We also note that the large reductions in symptoms in both conditions are larger relative to previous trials of children in comparable settings (Tol et al., 2008). We caution that these observed large reductions in this study may be attributed to regression to the mean, the effects of repeated assessments or the lack of stability of measures that are not adequately tested in Aceh.
Interestingly, there were no discernible differences in effects between the two conditions. We commence this discussion by recognizing that the lack of difference between treatment arms may be attributed to the small sample size that occurred because of the premature termination of the study. Having said that, we also note that even with this limited sample, there were very small differences between conditions, which suggests that it is possible that between-group differences may not have been achieved if we had achieved the targeted sample size. We also note that this study trialed two interventions with proven efficacy, and so it is possible that the effect size between the conditions would probably have been larger if we had compared the interventions with an attention-only or wait-list control condition.
The observation that trauma-focused CBT and PS suggests that interventions that emphasize either trauma-focused or PS approaches can have beneficial effects on post-conflict mental. Several explanations are possible for these comparable benefits. First, it is possible that non-specific therapy effects underpinned the gains made by children in both children. Second, although Western models emphasize the primacy of focusing on trauma memories to resolve PTSD (Foa et al., 2009), there is increasing recognition that in settings where people’s immediate needs often involve poverty, overcrowding, hunger and other severe adversities, addressing these issues may have an important impact on their mental health (Fernando et al., 2010; Neuner et al., 2006). It is possible that the children in the PS condition achieved significant benefits from learning PS skills because this arm of the study provided them with strategies to manage some of the anxieties and anger difficulties they experienced. These possibilities remain speculative because the design lacked a comparator condition to allow an index of non-specific effects of intervention.
Interestingly, depression was less amenable to the benefits of either treatment arm in comparison to both PTSD or anger. One could argue that the ongoing poverty and hardship experienced by people in Aceh resulted in depression being more resistant to the strategies taught in either CBT or PS. Depression is prevalent in communities affected by social deprivation, and in the absence of these being improved, it can be difficult for a brief psychological intervention to ameliorate this depressed mood (Patel et al., 2009). It is worth noting that Aceh has a long history of poverty, conditions that have been aggravated markedly by the tsunami and civil conflict (World Bank, 2008). This poverty may have limited the capacity for intervention to ameliorate children’s depressive levels. It is also worth noting that a significant proportion of the children had lost parents or other loved ones, and although prolonged grief was not directly assessed, it is possible that persistent grief reactions may have contributed to ongoing depression.
As noted above, any conclusions arising from this study are qualified by the unexpected small sample size. We also note that we were not able to obtain treatment fidelity ratings because of retribution concerns in the communities. To offset this potential problem, we strived for adherence to treatment protocols by delivering most content on videos presented on portable DVD players. However, the lack of fidelity ratings is potentially problematic because lay-counselors provided both sets of interventions, and we note that the possibility of drift between the two treatment approaches remains a possible explanation for the comparable outcomes of the treatments. The measures that were employed have not been validated in these local regions, and so the extent to which they match local understandings of mental health concerns in Acehnese children remains to be tested. This study lacked a non-intervention control condition which would have provided a reference point against which both active treatment arms could have been compared. There was also no inter-rater assessments of assessors’ scoring, precluding the capacity to index the reliability of the assessments.
These limitations notwithstanding, these outcomes suggest that lay-counselors with no prior health training can be instructed in delivery of psychosocial interventions that are associated with significant reductions in PTSD and anger problems. There were no reported adverse events, suggesting that these interventions are safe to be implemented with children who have been exposed to marked trauma and suffer ongoing adversity. Despite the limitations, our findings underscore the need for more research in diverse populations affected by conflict to determine the optimal intervention strategies to assist children affected.
Footnotes
Acknowledgements
This trial was prospectively registered on the Australian and New Zealand Clinical Trials Registry (ACTRN12611000080921).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded by an Australian Research Council Linkage Grant (LP100100702).