
Abstract
Introduction
There is a growing research base that informs clinicians on the mental health outcomes of children and adolescents who experience weather-related disasters. Research with large sample sizes and psychometrically sound measures have been conducted following hurricanes, cyclones, earthquakes and wildfires (Bal and Jensen, 2007; McDermott and Palmer, 2002; McLaughlin et al., 2009). Modelling of complex aetiological factors is difficult in the post-disaster environment given the understandable focus on service provision, little time to formulate research questions and hone designs and lack of timely funding for research and programme evaluation. Nevertheless, consistent with the model proposed by Pynoos et al. (1995), proximal (or event-related) and distal (pre-disaster) factors associated with children’s post-disaster psychopathology have been identified. Event-related factors that increase the odds of an adverse mental health outcome for a child or adolescent include event exposure, proxies of increased exposure, such as experiencing evacuation, and fear that they or a family member might die (McDermott and Palmer, 2002). Distal personal factors include the individual’s trait anxiety (Lonigan et al., 1994), coping style (McLaughlin et al., 2009) and attribution style (Joseph et al., 1991).
Although some personal distal factors have been elucidated, little research had been dedicated to examining the relationship between the social environment and post- disaster post-traumatic stress disorder (PTSD) in children, despite the former being an important focus in mental health research generally. For example, prospective and cross-sectional studies demonstrate that social capital (community participation and social cohesion, sometimes called ‘connectedness’) is protectively associated with mental health (Almedom, 2005; De Silva et al., 2005; Falzer, 2007; Stafford et al., 2008).
For children and adolescents, as for adults, connectedness appears to be beneficial for physical (Drukker et al., 2005) and mental health (Caughy et al., 2003; Lundborg, 2005; Saluja et al., 2003). However, there has been no research into the relationship between connectedness and PTSD in young people. Climate change is expected to underpin a steady increase in weather-related disasters (International Panel on Climate Change, 2007; Meehl et al., 2007), increasing exposure to traumatic events (Berry et al., 2010) and impacting particularly strongly on society’s most vulnerable, including children (McMichael et al., 2008). It is, therefore, timely to consider factors that might assist children in building resilience to weather-related disaster trauma and in recovering from it.
The aim of this paper is to investigate the relationship between trauma exposure, child connectedness and post-disaster child PTSD in a cross-sectional study controlling for sex, age and school system. If higher levels of child connectedness are protectively associated with child trauma, as we expect, children with higher levels of connectedness will report fewer traumatic symptoms than their less connected peers, independent of other predisposing factors such as event exposure and perception of threat.
Methods
School-based screening was performed 3 months after the 2006 Cyclone Larry disaster. Cyclone Larry was a category 5 cyclone that hit the northern Queensland rural city of Innisfail and surrounding townships and farming area. Miraculously, no lives were lost. Private home damage was extensive: the region’s centre experienced 50% private home damage, and surrounding townships 15–99%. The total insurance cost is estimated at $AUS360 million, not counting ongoing decreased family income.
Procedure
Following a training module, screening was a classroom activity led by school counsellors, aided by the classroom teacher. Students attended their classroom as for any other lesson and were informed the school counsellor would be asking them questions ‘about their cyclone experience’. Following non-disaster-related example questions, including how to correctly answer a multiple response, screening questions were read to students to standardise for reading ability. Consenting students confidentially made responses on their own answer sheet. For more details regarding this procedure, see McDermott and Palmer (2002). This service provision initiative was approved by the Queensland Departments of Health, and Education and Training, and Catholic Education Queensland research and ethics committees. Signed parental consent was required for all assessments.
Participants
The sample frame was all students from grades 4 to 7 in the cyclone-affected area who returned a signed parent consent form. Participants in the present study were 804 children (52.8% girls) aged 8–13 years (mean 10.22, SD 1.24), corresponding to grades 4 to 7 (the older primary school years in Queensland), who voluntarily completed screening questionnaires. Six schools participated, ranging in size from 63 to 389 students, with each grade contributing approximately 25% of the participants. Most parents (81%) reported their children did not have a mental health difficulty during the 12 months prior to the cyclone disaster.
The participation rate was 68.0%. On 10% of the ‘refused consent’ forms, parents wrote that their family was not in the disaster area at the time of the cyclone; we adjusted the response rate accordingly (AdjR/R = 75.5%). As most parents gave no reason for refusing consent, we made no further adjustment. Because of sensitivity about ‘research’ in the post-disaster setting, we did not collect socioeconomic data. However, compared to Queensland as a whole, Indigenous Australians (7.7% of the relevant Heath Service District population, versus 2.3% in Queensland), individuals who spoke a language other than English (8.7% versus 7.7%) and people living with relative socioeconomic disadvantage (36% versus 20%) were over-represented in the sample frame community (Harper et al., 2004).
Measures
Post-traumatic stress disorder
PTSD was measured using the Posttraumatic Stress Disorder Reaction Index (PTSD-RI) (Frederick, 1987), an extensively used 20-item child-report measure of PTSD in children and adolescents. The items are adapted to ask about a specific traumatic event, in this case Cyclone Larry. The psychometric properties of the PTSD-RI are well documented, considered suitable for research purposes and demonstrate satisfactory internal consistency (McDermott et al., 2005), concurrent validity (Pynoos et al., 1993) and discriminant validity (La Greca et al., 1996). Responses were recorded on a 5-point Likert-type scale and summed to generate a total PTSD-RI score (range 0–80) from which a standard case classification was derived (doubtful = 0–11, mild = 12–24, moderate = 25–39, severe = 40–59 and very severe = 60–80).
Child connectedness
Child connectedness was measured using four items, two about participation (friends and clubs) and two about cohesion (trust and belonging). Contact with friends and participation in school activities were measured using items adapted for children from the Australian Community Participation Questionnaire (Berry et al., 2007). The items as adapted were ‘I have friends to play with or hang out with during school breaks’ and ‘I go to a school sport team training, or a rehearsal, meeting or club’. Children indicated their agreement with the former on a 5-point scale ranging from 0 ‘none of the time’ to 4 ‘most of the time’ (mean 3.54, SD 0.97) and with the latter by circling ‘yes’ or ‘no’. Trust in others was an item adapted from the Organizational Trust Inventory (Cummins and Bromiley, 1996). The item as adapted for children was ‘I think most people take advantage of others (like doing things for themselves not others)’. Children indicated their agreement on a 5-point scale as described above (mean 2.56, SD 1.23). A ‘belonging’ item was adapted for children from the sense of belonging subscale of the Interpersonal Support Evaluation List (Cohen et al., 1985). The item as adapted was ‘When I feel lonely, there are several people I could call to talk to’; children responded on the same 5-point scale (mean 2.74, SD 1.43).
Proximal factors: trauma exposure and threat perception
Child exposure to cyclone-related traumatic events was measured by asking children about typical experiences, whether they had witnessed flying debris, experienced home damage, including broken windows, damage to part or their entire roof, or had to live elsewhere as a result of home damage. Perceptions of threat to life were assessed by asking children ‘Did you think you were going to die during the cyclone?’ or that a ‘family member’ may die. As with exposure questions children responded by circling ‘yes’ or ‘no’. They were also asked to rate how frightened they had been during the cyclone by circling a number from 0 to 10 (0 = not at all, 10 = extremely). Finally, children gave their post-disaster global experience of school by endorsing ‘better’ or ‘worse’ to the question: ‘Is going to school better or worse since the cyclone?’
Distal factors
In the post-disaster environment, families were understandably focused on restoration of essential safety, shelter, food and health. Accordingly, research activities were constrained, with the result that our explanatory model could not include measures of pre-disaster coping or personality.
Statistical analysis
PTSD outcomes were child report PTSD-RI total score (continuous variable) and a dichotomous variable: PTSD-RI categories ‘severe or very severe PTSD’ = 1 and other classifications = 0. We computed a continuous connectedness score (see below) and two dichotomous categories: children in the lowest decile of the connectedness distribution were categorised as ‘low child connectedness’ (low = 1, other = 0) and those in the highest decile as ‘high child connectedness’ (high = 1, other = 0). We used chi-squared tests to compare dispersion between pairs of categorical variables, two-tailed t-tests to compare between-group means for categorical with continuous variables, and correlation coefficients to test associations between pairs of continuous variables. We took account of a potential confounder (type of school) and examined possible main effects of age and sex.
Odds ratios (crude and adjusted) were calculated by logistic regression and scale validity and item structures tested via one-factor congeneric modelling (see below). For each of these factor models, we first used exploratory factor analysis to investigate whether all candidate items loaded onto a single latent factor. In each case, they did. Hierarchical multivariate relationships, taking account of factor structures, were tested using structural equations modelling. As there were fewer than 10% missing data for any variable, we imputed missing values using estimation maximisation (EM). Means, SDs and correlation coefficients in the imputed data set were almost identical to those in the data set with missing data; all analyses were therefore conducted using the imputed data set using PASW Statistics 18.0, Stata v11 and AMOS 18. We computed robust standard errors to adjust for possible inflation of estimates due to the school-based clustering of the data.
Results
Child post-traumatic stress
The mean PTSD-RI total score was 21.41 (SD 14.92), with 31.1% students ‘doubtful’, 33.3% ‘mild’, 23.6% ‘moderate’, 9.6% ‘severe’ and 2.4% ‘very severe’. Girls (mean 24.44, SD 0.78) reported higher PTSD-RI total scores than did boys (mean 18.01, SD 0.65, df(802), t = –6.20, p < 0.0001), reporting significantly higher scores in 17 out of 20 items.
Child connectedness
At 70%, most children reported participation in a school sports team, rehearsal, club or meeting and 93.1% stated they had friends to play with during school breaks. Only 6.9% (n = 50) children said they played with friends during school breaks ‘none’ or ‘little of the time’. Three-quarters (76.1%) of children reported that there were several people they could talk to when they were lonely; a large minority (23.9%) stated that this was the case ‘none’ or ‘little of the time’. A smaller but still substantial minority of children (17.7%, n = 128) expressed low trust, stating that people take advantage of others ‘much’ or ‘most of the time’.
Exploratory factor analysis of the four connectedness items produced a one-factor solution. The single-factor structure was confirmed using one-factor congeneric modelling (for a review of these procedures, see Berry et al., 2007). The model fit the data well without modification (χ2 = 1.61, df(2), p = 0.45; RMR = 0.01; GFI = 1.00; AGFI = 0.99; NFI = 0.97; TLI = 1.02; CFI = 1.00; RMSEA = 0.00; AIC achieved its minimum, indicating the model had not been over-fitted). With a standardised weighting of 0.62, having friends to play with loaded most strongly on – and best defined – the factor. Having people to talk to, trusting others and participating in school activities were also significant aspects of child connectedness. A weighted composite score for child connectedness was computed using factor score weights derived from the one-factor congeneric model (composite range = 0.00–2.17, mean 1.72, SD 0.41). To aid interpretation, scores were converted to a 5-point scale, range of 1–5 (mean 4.17, SD 0.75). Scores showed a skewed distribution, with mode = 5, indicating high to very high levels of connectedness among most children.
Low connectedness children reported significantly and substantially worse PTSD psychopathology than did other children (mean 29.77, SD 1.85 versus mean 20.57, SD 0.54, t = 5.125, df(714), p < 0.0001) and were significantly more likely to meet case criteria for severe or very severe PTSD (26.7% compared with 10.12%, χ2 = 40.762, df(714), p < 0.0001). This difference was more marked among children with very severe PTSD (12.2% versus 1.2% in less severe PTSD categories). These children were also significantly more likely to say that school was worse since the cyclone (52.0% compared with 38.5%, χ2 = 4.976, df(1), p = 0.026). Conversely high connectedness children reported significantly fewer PTSD symptoms than did their peers (mean 14.57, SD 1.38 versus mean 22.84, SD 0.56, t = 5.5630, df(802), p < 0.0001) and were significantly less likely to meet case criteria for severe or, especially, for very severe PTSD (2.5% versus 13.0%, χ2 = 7.523, df(1), p = 0.006).
Child exposure to cyclone-related events
Most commonly reported cyclone-related events were seeing flying debris (75.3%), home damage (68.4%), broken windows (39.4%) or loss of part of the roof (33.4%). Forty students (5.2%) reported their home had lost the whole roof. One in 10 children stated that, due to home damage, they had to live ‘somewhere else’ following the cyclone.
We tested the factor structure of the trauma exposure items using one-factor congeneric modelling, as described above. After removal of a non-significant item (losing whole roof) and co-varying two pairs of error terms, the data fitted the model well, indicating a single trauma exposure factor (χ2 = 0.59, df(3), p = 0.90; RMR = 0.00; GFI = 1.00; AGFI = 1.00; NFI = 1.00; TLI = 1.03; CFI = 1.00; RMSEA = 0.00; AIC at minimum). With a standardised weighting of 0.70, ‘other home damage’ loaded most strongly on – and best defined – the trauma exposure factor. Having ‘broken windows’ and ‘losing part of the roof’ contributed strongly to defining the factor. ‘Seeing flying debris’ and ‘having to live elsewhere’ made smaller but still significant contributions. A weighted composite score for child trauma exposure was computed as before (range 0.00–0.60, mean 0.316, SD 0.19) and, for ease of interpretation, scores were converted to a 5-point scale with a range of 1–5 (mean 3.10, SD 1.27).
Child threat perception
As the threat perception one-factor congeneric model was saturated (contained three items, insufficient for fitting), we estimated the error variances and fixed them in the model prior to fitting. The model fitted the data well without modification (χ2 = 0.01, df(4), p = 1.00; RMR = 0.01; GFI = 1.00; AGFI = 0.99; NFI = 0.97; TLI = 1.09; CFI = 1.00; RMSEA = 0.00). With a standardised weighting of 0.93, the child thinking she or he would die loaded most strongly on – and dominated the definition of – child threat perception. Thinking a family member would die and being frightened also loaded strongly on the factor. A weighted composite score for child threat perception was computed (range 0.00–0.97, mean 0.28, SD 0.37). As scores were strikingly bimodally distributed, they were dichotomised about the mean to create high (N = 218, 27.1%) and low (N = 586, 72.9%) threat perception categories for our logistic and structural modelling.
One-quarter (25.8%) of children thought they were going to die during the cyclone, with more (32.8%) fearing a family member might die. One-way analyses of variance indicated that girls reported higher levels of threat perception than did boys (F = 15.87, df(1), p < 0.0001), and felt more frightened on the day of the cyclone (F = 47.67, df(1), p < 0.0001). Younger children experienced higher levels of threat perception than did older children (r = –0.12, p < 0.0001) and reported feeling more frightened (r = –0.14, p < 0.0001). Patterns of associations among variables were stable by sex and age.
What affected the likelihood of children developing PTSD?
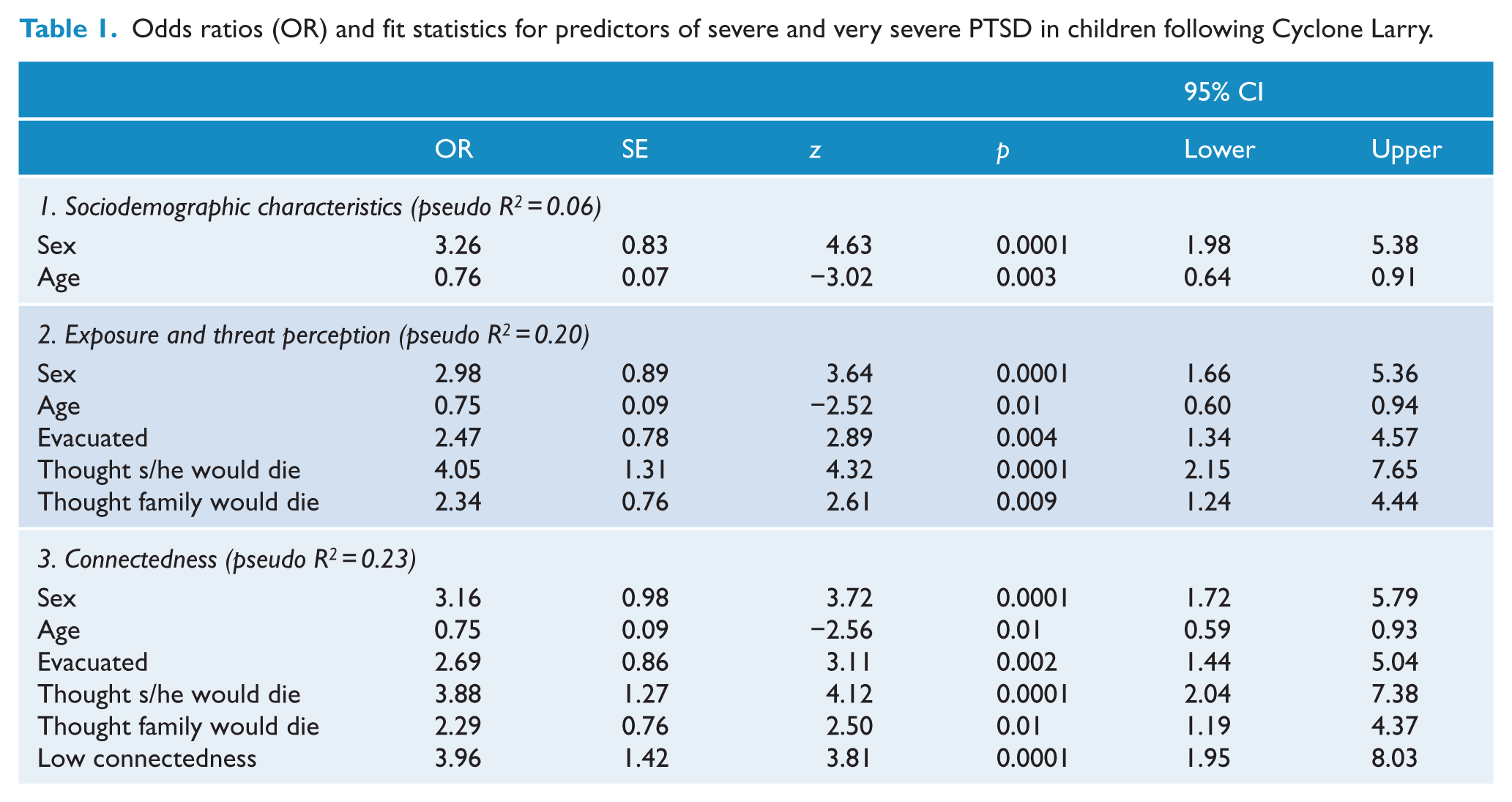
We undertook a hierarchical step-wise logistic regression analysis in which variables were entered in three blocks: (i) sociodemographic controls, (ii) exposures and threat perception and (iii) child connectedness (Table 1). For each block, variables that did not contribute significantly to predicting odds ratios were deleted one by one and the model comprehensively re-evaluated until only significant predictors remained. Child parent-reported pre-disaster anxiety or depressive symptoms were not related to post-disaster PTSD (χ2 = 0.65, df(1), p = 0.42) and were not included in the analysis. In block 1, sex and age each contributed significantly to the model: younger children were more likely to develop severe or very severe PTSD, with girls about three times as likely as boys to do so. In block 2, children who thought they would die were four times as likely as were other children to develop PTSD, while those who thought a family member might die, or who were evacuated, were at about double the risk of PTSD. Seeing flying debris, home damage, losing part or the whole of the roof did not contribute significantly to the model, suggesting that their bivariate associations with PTSD were fully accounted for by the remaining variables. The addition of connectedness in block 3 showed that, taking account of all variables simultaneously, low connectedness children were nearly four times more likely than were other children to develop PTSD. In the final model, all six variables together explained 23% of variance in child PTSD. In a separate model, high connectedness children were nearly 11 times less likely to develop PTSD (details available from the authors). There was no evidence of mediation in either model suggesting that connectedness is an additional, independent predictor of child PTSD.
Odds ratios (OR) and fit statistics for predictors of severe and very severe PTSD in children following Cyclone Larry.
Structural modelling
Our structural equation model included all the one-factor congeneric models for each of the predictor concepts according to our hypotheses. The initial model did not fit the data well (χ2 = 359.18, df(97), p < 0.0001; RMR = 1.30; GFI = 0.99; AGFI = 0.99; NFI = 0.67; TLI = 0.67; CFI = 0.73; RMSEA = 0.06). We first examined parameter estimates to identify non-significant items or pathways. Taking account of all factors, variables and pathways simultaneously, the direct pathway linking cyclone trauma exposure to PTSD was non-significant and was deleted. Following comprehensive re-evaluation of fit, taking part in school activities did not load significantly on the child connectedness factor and its loading pathway was deleted. (The item itself was retained because it was associated with other factors in the model). Finally, the pathway between school system and connectedness was non-significant and was deleted. All other pathways and items were significant. As the model still did not fit the data well, we examined the modification indices. Making one modification at a time, and comprehensively re-evaluating the model after each modification, we introduced 15 additional pathways and co-varied five error terms (see Figure 1). The new pathway connecting school system to cyclone trauma exposure carried a regression weighting of β = –0.20; all the other weightings were trivial. Following these modifications, the data fitted the model well (χ2 = 100.93, df(79), p = 0.05; RMR = 1.68; GFI = 0.99; AGFI = 0.99; NFI = 0.91; TLI = 0.97; CFI = 0.98; RMSEA = 0.02; AIC at minimum).
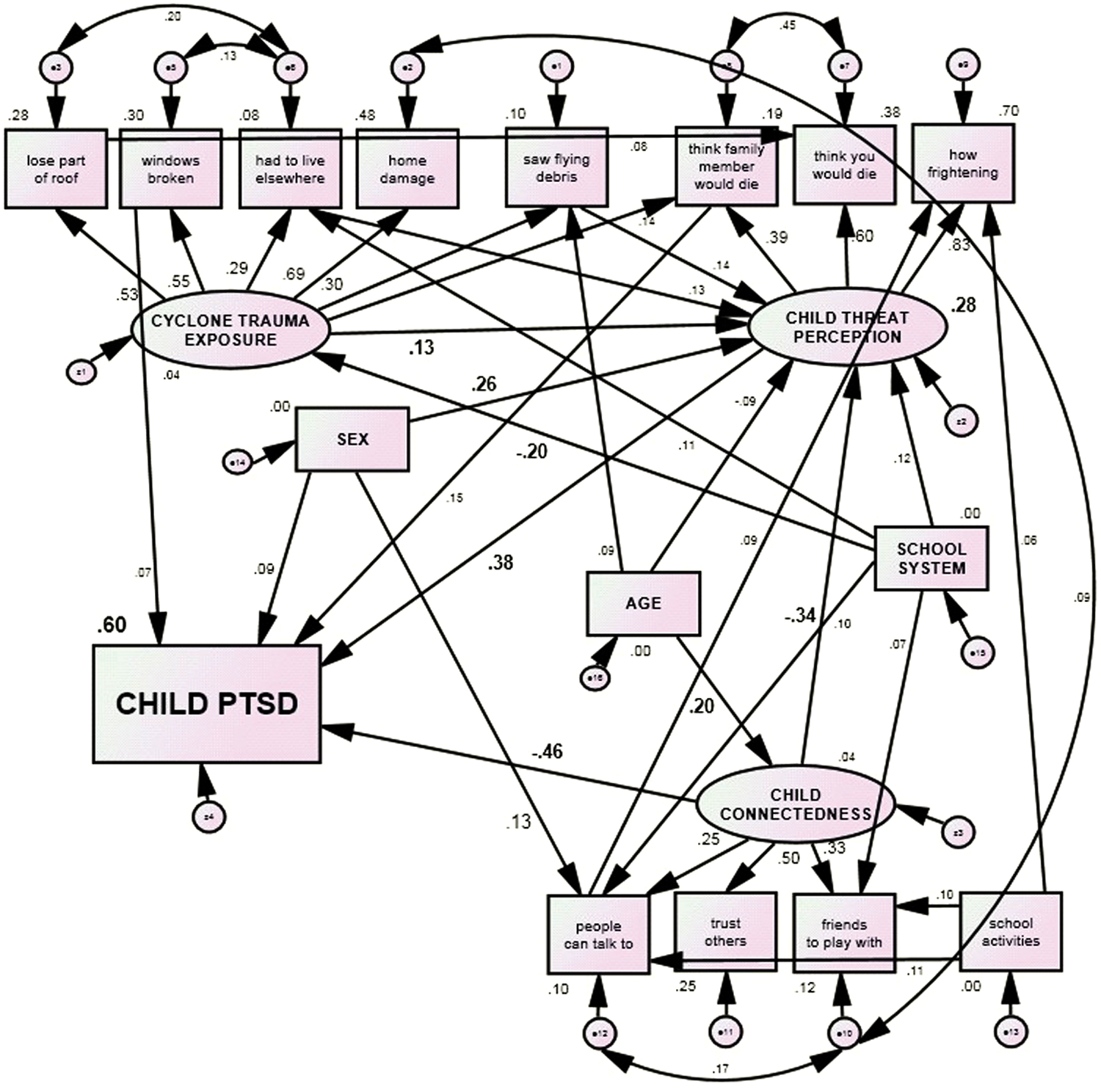
Structural equations model of child PTSD showing all significant pathways.
Figure 2 is a simplified version of the fitted model detailed in Figure 2. For ease of readership, pathways with weightings < 0.20 are not shown, except where they are potentially of substantive interest. The final model accounted for 60% of variance in child PTSD scores.
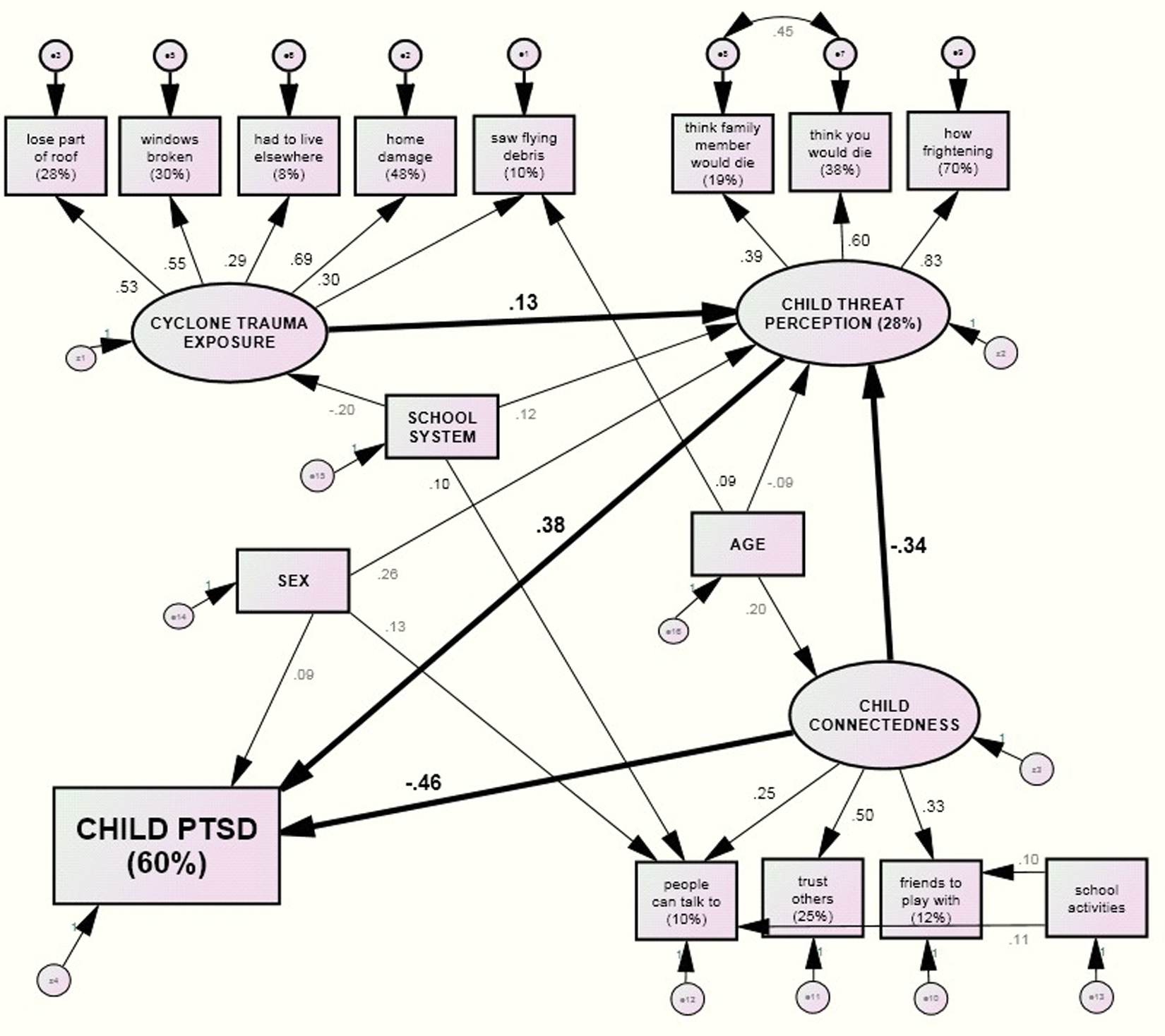
Structural equations model of child PTSD showing most important significant pathways.
Discussion
We aimed to (i) investigate how known and new aetiological factors are related to PTSD in children who experienced Cyclone Larry and (ii) assess whether connectedness may be a suitable target for pre-disaster resilience building. Our logistic model replicated past research that has emphasised the importance of threat perception in the development of post-disaster PTSD. We found strong evidence for the importance of a new concept, connectedness: children with very low connectedness reported significantly and very substantially higher PTSD psychopathology and were significantly more likely to meet case criteria for severe or very severe PTSD than were their peers. The relative ‘psychiatric advantage’ to high connectedness children was even greater.
Our structural model further elucidated these findings: while trauma exposure made a significant (if small) contribution to explaining variance in threat perception, it was not directly related to PTSD or to any other factor in the model. This suggested that greater exposure was related to greater PTSD solely because it generated greater threat perception. Greater threat perception was related to greater PTSD but only moderately so; greater child connectedness was also related to less threat perception, moderately strongly. With small contributions from minor pathways (discussed below), exposure and connectedness explained 28% of variance in child threat perception. As hypothesised, controlling for a large number of variables, greater child connectedness was strongly related to fewer symptoms of PTSD. Indeed, considering its direct and indirect pathway, connectedness was strikingly protectively associated with child PTSD.
Girls were somewhat more likely than were boys to feel threatened during the cyclone and slightly more likely to develop trauma symptomatology. Younger children were slightly more likely to feel threatened during the cyclone than were older children, while older children tended to have greater connectedness. Finally, there was a substantial relationship between a child thinking he or she would die and thinking a family member would die that was not accounted for by their shared loading on the threat perception factor. This suggests the presence of other factors pertaining to children’s fear of death during a natural disaster that are not captured by the present model.
Our findings suggest a new interpretation of how known and new aetiological factors are related: threat perception may be modified by community connectedness. Indeed, being poorly connected could place a child at extreme risk of post-disaster PTSD, while being younger and a girl may well exacerbate this risk. Two additional findings with respect to low child connectedness are potentially important for clinical practice and for building resilience. First, children with very low connectedness were significantly more likely to report fearing that a family member might die during the cyclone than were their more connected peers. Perhaps children who feel less connected to their peers, and distrustful of people in general, are more emotionally dependent on family members than are other young people and, therefore, more sensitive to fear for the well-being of significant others. The second finding was that children with low connectedness were more likely than were their peers to state that school was worse since the cyclone. It is not unusual for communities to ‘pull together’ in the face of disaster. But perhaps this applies primarily, or solely, to those with existing close ties, while the less well connected perceive, in contrast, greater isolation than they did before the disaster.
This cross-sectional research cannot impute causation; however, our findings create new questions about how known and new aetiological factors are related: threat perception may be modified by community connectedness. One of the most significant of these is the need to better understand the construct of child connectedness. While this construct is clearly operationalised in this study, it is a plausible hypothesis that child connectedness is causally related to other important variables which we were not able to measure. The most obvious candidate is attachment style with the primary care-giver(s). One hypothesis is that children who are high on connectedness have secure attachment which allows them to develop meaningful connections outside of their own families. Conversely, children low on connectedness may tend towards anxious or ambivalent attachment styles. Another potential link is a child’s social competence. In order to be able to target social connectedness as a potential preventative, resilience-building intervention, the construct requires further ‘unpacking’ and better understanding. Secondly, it will be important to replicate the role of child connectedness and to investigate whether the importance of this construct extends beyond weather-related disasters to other single-incident (and perhaps repetitive) trauma situations.
There are two other significant areas for future research: increasingly, parenting and family-related factors are being investigated as vulnerability and maintaining factors in the aetiology of PTSD following a single-incident trauma. It is hypothesised that parent–child interactions (including specific mechanisms, such as communication of threat) are critical in determining whether children are likely to perceive threat in a disaster. This is a difficult research question to address, however, because parent–child interactions tend to change quite significantly following a weather-related disaster (Cobham and McDermott, 2010). In order to be able to adequately examine the influence of parent–child interaction style on children’s tendency to perceive threat in potentially dangerous situations, one would ideally know about the interactional style pre-disaster. Finally, some of the unexplained variance of PTSD in our model may be variation in coping with the peri- and post-disaster environment based on gene polymorphisms, either as single gene × environment interactions or more complex genetic models.
Limitations of this study
Not all families agreed to participate in the school-based screening and we did not have data to describe any differences between these families and those who participated. Children and families reported disaster-related events 3 months post-disaster. While it was not possible to collect data immediately post-disaster, this timeframe may create a recall bias. Another limitation concerns our measure of child connectedness. Although all four items were drawn from adult/adolescent instruments with sound psychometric properties, the items have not previously been tested in younger children. Nevertheless, the children were able to answer the questions and our findings were consistent with our hypotheses. Given the potential importance of child connectedness in protecting children from post-natural disaster PTSD, further concept development and instrument validation is required. It would be important to include investigation of parents’ and other children’s perceptions about the connectedness of these children, and also to examine other factors linking children’s connectedness and well-being, such as academic attainment and social, emotional and behavioural problems outside the disaster context. Another limitation worth noting is that, while PTSD caseness was assessed via child-report measure, our measure of pre-existing mental health problems was completed by parents. The magnitude of discrepancy between child and parent report of children’s internalising symptomatology is well documented. Finally, this is a cross-sectional study and we have reported significant associations among factors. However, our design does not allow stronger conclusions about causation.
Conclusion
This is the first time that child connectedness has been identified as a strong predictor for post-natural disaster PTSD in children. Children’s connectedness is potentially modifiable and this construct may, therefore, be useful in designing pre-disaster resilience-building interventions. Although, as noted earlier, there is much research to be done to improve our understanding of connectedness in children and its underlying mechanisms, it is possible to imagine interventions that would result in improved ratings on the four specific and very concrete items used to measure connectedness. Potentially, as such interventions would benefit all children, they could be trialled in a school setting, as a universal public health initiative. Additionally, identifying poorly connected children prospectively may present an opportunity for targeted resilience building in communities or regions at high risk of weather-related disasters. This is in stark contrast to the other known predictors of post-disaster PTSD (such as event exposure), which are outside the control of those concerned with children’s post-disaster welfare.
Footnotes
Acknowledgements
The authors wish to acknowledge the parents and children of the greater Innisfail area of north Queensland who, despite considerable adversity, participated in this project. The support of Dr Aaron Groves and Mr Kevin Freele was also vital. The authors acknowledge crucial collaboration from Education Queensland, Catholic Education and Mater Health Services Brisbane.
Funding
The authors received financial support from Queensland Health.
Conflict of interest
There was no financial involvement by any organisation that may derive a financial interest in the material in this manuscript.