
Abstract
Research on child emotional health in the post-natural disaster environment has attempted to investigate complex outcome models inclusive of both disaster-related factors such as exposure, as well as psychological constructs inherent to the individual. The latter include coping style [1], causal attribution [2], threat perception [3] and high trait anxiety [3,4]. This is consistent with contemporary formulations of child and adolescent mental health that emphasize interactions between proximal factors, for example peer interactions, and distal factors such as the individual's innate resilience and vulnerability. Few post-disaster studies have included family resilience as a potential variable that may influence the individual's vulnerability to post-traumatic stress disorder (PTSD), or indirectly moderate other significant factors such as their threat perception or social connectedness.
An ecological approach to resilience in children takes into account the protective mechanisms of the child– environment interaction [5], including the family and the broader ecology. Family resilience can be defined as the ability of a family to respond positively to an adverse situation and emerge from the situation feeling strengthened, more resourceful, and more confident compared to the prior state [6]. A number of models of family resilience have been proposed. Using a systems approach, Walsh proposed three characteristics of resilient families: belief systems, organizational patterns, and communication/problem-solving [7]. Belief systems encompass the capacity to make meaning from adversity, a positive outlook, transcendence and spirituality (e.g. faith, rituals, purpose, and appreciation). Organizational patterns include the flexibility to adapt and re-stabilize, connectedness with others, and economic resources. Communication/problem-solving includes clear consistent information, emotional expressiveness and collaborative decision making. In contrast, Lietz found that a non-sequential process model best fitted the experience of resilient families, and emphasized the differing focus of the family at different stages following adverse events including survival, adaptation, acceptance, growing stronger, and helping others [8]. Family strengths, consistent with the characteristics identified by Walsh, are drawn on at different stages. Both of these models incorporate a sense of belonging and connectedness rather than isolation, and process and resources rather than being overwhelmed.
We hypothesize that major disasters can cause extensive disruption to family processes as both the individual members of the family and the family unit as a whole respond to the crisis situation. It is clear then that the resilience capabilities of families can act as either a risk for maladaptation or be protective and support optimal adaptation during such adversity [9]. To date, there is a paucity of empirical data on family resilience following natural disasters and its relationship to the development of PTSD in children following natural disasters. The aim was to investigate whether parent report of family resilience predicted children's post-disaster psychological functioning, specifically whether low family resilience was associated with elevated levels of disaster-induced PTSD and general emotional symptoms, independent of distal PTSD-related factors such as previous history of the child experiencing a mental illness, community connectedness and proximal factors such as event-related exposure and threat perception. Further, whether this was a main effect and/or whether it moderated other significant factors in the final model.
Methods
North Queensland, Australia is a tropical cyclone-prone area. During late March 2006 Cyclone Larry developed for several days in the Coral Sea and then crossed the coast with an estimated intensity of a category 5 tropical cyclone. Consistent with a very severe cyclone, regional towns experienced 15–99% infrastructure damage, and the financial implications of widespread crops destruction meant that the livelihood of residents was impaired for many months after the disaster. The total insurance cost was estimated at $AUD360m. Although physical injury was common, in many cases occurring during the clean-up phase not the cyclone, no lives were lost.
Procedure
Following the cyclone the government departments of Queensland Health, and Education Queensland undertook mental health screening of school students to identify individuals with a persisting disaster-related mental health problem. This procedure has been previously conducted following natural disasters in Australia and met with parent and teacher approval [4,10]. For logistical reasons screening took place 3 months after the cyclone. Screening was a classroom activity, proceeding only with informed, signed, parent consent and was conducted by school counsellors. Teachers remained with their class during the activity. Questions were followed by an opportunity for students to discuss their cyclone experience with their class, teacher and counsellor.
Participants
The sample consisted of 568 children who attended public primary schools, whose parents consented to complete the family resilience questionnaire and other measures. Of this group 441 parents (77.6%) completed the family resilience measure. Questionnaire non-completers generally did not answer any family resilience questions and so data recovery, for example using mean item substitution, was not possible. The children of non-participating families did not significantly differ from participating family children on gender, age, or measures of the child's general or post-traumatic psychopathology. Of participating children 55.2% of the sample was female; the average age was 10.2 years (SD = 1.3, range = 8–15 years). Participants were approximately equally divided across the four primary school years. Given understandable subject sensitivity concerning data collection in a post-disaster environment individual race and socioeconomic class data are not available. Relative to Queensland as a whole, however, people living with relative socioeconomic disadvantage (36% vs 20%) and Indigenous Australians (7.7% vs 2.3%) were overrepresented in the disaster area [11].
Measures
The Family Resilience Measure (FRM) is a nine-item, parent-report questionnaire that begins with the statement, ‘How well do these match the way things are in your family?’ [12]. The FRM focuses on the family dealing with adversity by getting on together, talking about worries, being there for each other, accepting one another and counting on relatives ‘when things get tough’. The remaining questions deal with family traditions such as undertaking activities together and practical family functioning such as spending on food and clothing before ‘buying other things’. Parents rated the nine FRM statements on a 5 point Likert scale on whether they agreed ‘not at all’ to ‘very much’. The range of possible scores is 9–45, with higher scores indicating higher family resilience. Cronbach's alpha for the FRM for this sample was 0.83, suitable for research purposes.
The PTSD Reaction Index (PTSD-RI) is a well established child and adolescent self-report measure of PTSD symptoms, extensively used in natural disaster settings [13,14]. Traumatic event specificity is created by including the trauma designation, in this case ‘the cyclone’ in the wording of questionnaire items. The PTSD-RI has 20 items. Respondents apply a 5 point Likert-like scale to validate the presence of symptoms over the preceding month. The PTSD-RI yields a total PTSD-RI score as well as doubtful, mild, moderate, severe and very severe PTSD categories. The PTSD-RI has been successfully used before with Australian students of similar age [4]. To assist with reliable measure completion all students completed non-disaster-related training questions and all PTSD-RI items were read aloud to students to control for variations in reading ability. The PTSD-RI has acceptable psychometric properties for research use [1,3,4,13], and the Cronbach's alpha for this sample was 0.90.
The Strengths and Difficulties Questionnaire (SDQ) parent-report version, emotional subscale [15,16], was included to screen for non-PTSD internalizing psychopathology. The emotional subscale consists of five questions relating to feelings of unhappiness, worries, fears, feeling nervous and somatic complaints. Items are rated on a 3 point scale: not true, somewhat true, or certainly true, and a subscale total score generated. Normative Australian data are available for the SDQ and subscales [17]. The SDQ has psychometric properties that make it suitable for research purposes [16] (sdqinfo.com) and the internal consistency (Cronbach's alpha) for this sample was 0.81.
Other screening questions included child report of their disaster experience, perception of threat, and questions relating to the cyclone aftermath and recovery. Again these items have been previously used with children in the post-disaster period [4,10], questions were read aloud to students and clarification of items was encouraged. exposure questions were self-report, yes/no format questions such as, ‘Did you see flying debris?’, ‘Was your home damaged?’, and ‘Did your home lose part of its roof?’. Perception of threat was assessed by two questions, ‘Did you think you were going to die during the cyclone?’ and ‘Did you think a family member might die during the cyclone?’ A single child self-report item measured how frightened children felt on the day of cyclone on a 10 point scale with 10 indicating ‘extremely frightened’. Children also completed a brief, four-question measure of community connectedness derived from the Australian Community Participation Questionnaire [18], the Organizational Trust Inventory [19] and the sense of belonging subscale of the Interpersonal Support Evaluation List [20]. Children indicated their agreement with statements concerning their contact with friends, for example ‘I have friends to play with or hang out with during breaks at school’, trust in others, sense of belonging and participation in school activities. Respondents applied the same 5 point Likert-like scale as the PTSD-RI to validate the statements. Exploratory factor analysis (maximum likelihood extraction) of the four items produced a single-factor model; model fit data (χ2 = 1.61, df(2), p = 0.45, root mean square error of approximation = 0.00) indicated that the measure was suitable for research purposes. A total community connectedness score was created; children in the lowest 10% of the connectedness distribution were categorized as ‘low child connectedness’.
Statistic analysis
The FRM was analysed as a continuous variable (total score) or a case (abnormal) versus non-case nominal variable. Similarly the PTSD-RI total score was analysed as a total score or a categorical ‘severe or very severe PTSD’ versus all other responses. The latter was used in a logistic regression model of the predictors of PTSD. For child connectedness, children in the lowest 10% of the connectedness distribution were categorized as ‘low child connectedness’. We used χ2 tests for pairs of categorical variables, two-tailed t-tests for categorical with continuous variables, and correlation coefficients for pairs of continuous variables. We took account of potential confounders, such as type of school, and possible effect modification by age and sex. Odds ratios (crude and adjusted) were calculated on logistic regression. There were fewer than 10% missing data for any variable; we imputed missing data using full information maximum likelihood estimation. Means, standard deviations and correlation coefficients in the imputed dataset were near-identical to those in the dataset with missing data. Analyses were conducted on the dataset with imputation using SPSS 15.0 for Windows (SPSS, Chicago, IL, USA), State v9.2 (STATA, College Station, TX, USA) and AMOS 7.0 (Spring House, PA, USA).
Results
Participating children experienced significant exposure to Cyclone Larry including reporting seeing ‘flying debris’ (341/438, 77.8%), experiencing damage to their home such as roof damage (165/452, 36.5%) or loss of their roof (17/447, 3.8%), and many perceived that they may have died during the cyclone (109/425, 25.6%). Consistent with this level of exposure, most of the sample experienced some PTSD symptoms; 64 individuals (11.3%) were in the severe–very severe PTSD category on the PTSD-RI. On the SDQ-Emotional subscale the mean score was 1.66 ± 2.16, with 56 participants (12.5%) reaching case criteria on this subscale, but the mean emotional symptoms score reported in this sample was less than that reported in an Australian community sample by Mellor [17]: SDQ-Emotional mean score 2.3 (SD = 2.0) in 7–10-year-olds, 2.0 (SD = 2.1) in 11–13-year-olds.
The mean Family Resilience score was 40.25 (SD = 4.40, range = 22–45). Applying published cut-off scores, 53 families (28.6%) scored in the poor family resilience range while 71.4% scored in the good/very good range. This sample had significantly more respondents in the good/very good levels of family resilience compared with the published sample (t = – 9.65, p < 0.001) [12].
Bivariate associations with family resilience
Consistent with measuring family not individual attributes, there was no significant relationship between the family resilience total score and child age (t = – 0.615, df = 439, p = 0.538), or school grade (F = 0.892, df = 3, p = 0.446, Table 1). There was a trend for a lower family resilience report by parents of female student participants (t = 1.753, df = 439, p = 0.081). A lower family resilience score was associated with meeting case criteria for child emotional problems on the SDQ (t = – 2.919, df = 425, p = 0.003) and longer duration of child mental health difficulties (F = 5.801, df = 408, p = 0.000). Family resilience total score was not associated with child PTSD category (t = – 0.340, df = 439, p = 0.734) or child self-report of threat perception to themselves (t = 0.367, df = 407, p = 0.714). Children who were concerned that their parents may have died during the cyclone disaster, however, were significantly more likely to have lower family resilience scores (t = 2.663, df = 407, p = 0.008).
Bivariate associations with family resilience
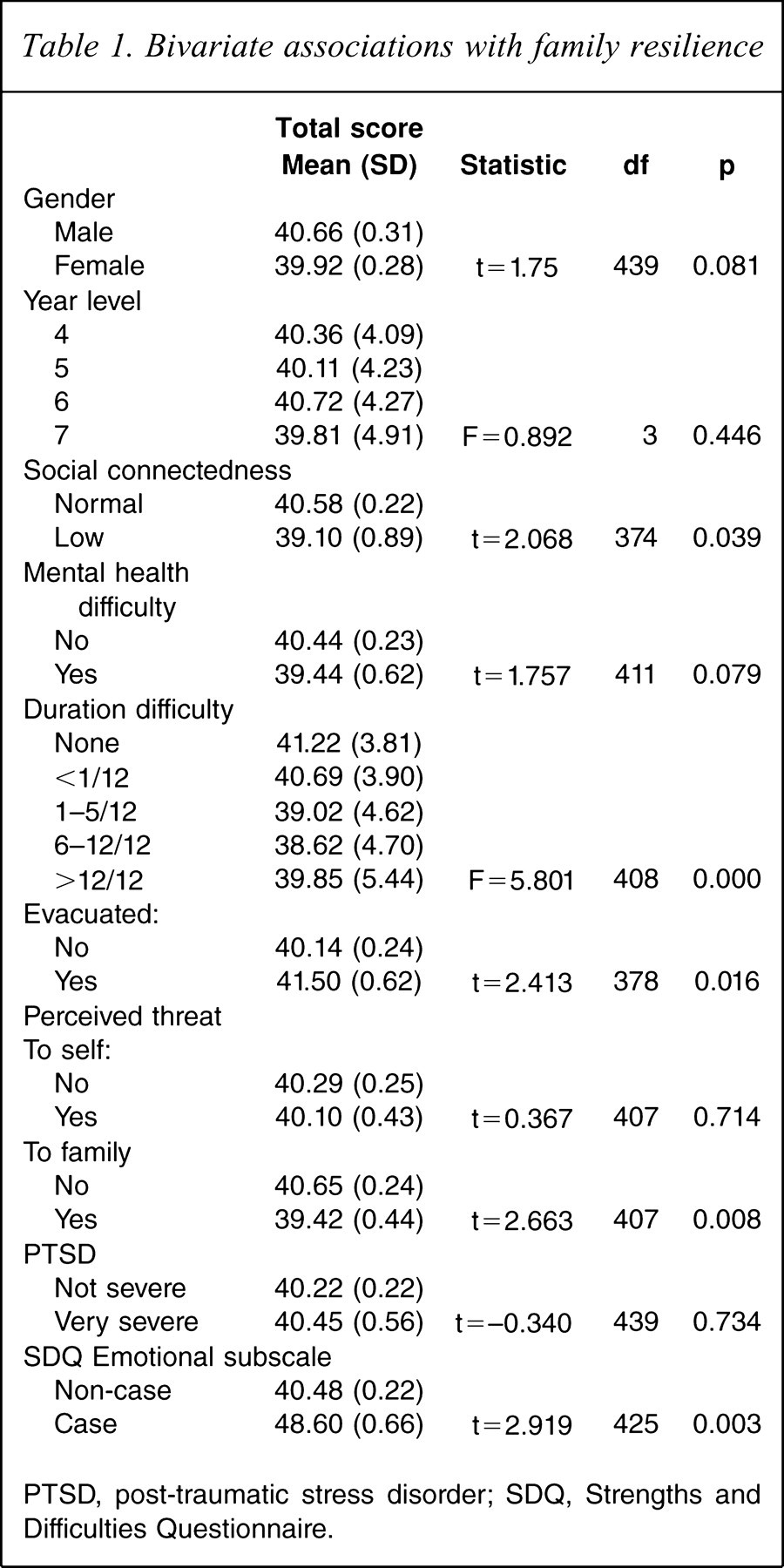
PTSD, post-traumatic stress disorder; SDQ, Strengths and Difficulties Questionnaire.
Modelled relationships between disaster-induced PTSD and family resilience
In this sample the previously published relationships between event exposure, threat perception and disaster-induced severe–very severe PTSD case status were replicated (Table 2, model 1), providing evidence that children's emotional responses to this disaster were typical. For example there were significant odds ratios (adjusted for age and gender; ORadj) for PTSD if the participant perceived that they may have died during the cyclone (ORadj = 4.79, 95% confidence interval (CI) = 2.21–10.43). There was no significant relationship between child PTSD and previous mental health problem, duration of problem, SDQ emotional health case status or family resilience (Table 2, model 2). SDQ emotional health case status was a trend (ORadj = 2.49, p = 0.096). The final model included all variables significant at the p < 0.10 level. In the final model (Table 2, model 3) PTSD case status was independently statistically associated with female gender, perceived threat to self and lower social connectedness. Duration of mental health difficulties was not significant. Family resilience did not independently contribute to the model (ORadj = 0.57, 95%CI = 0.13–2.44). Indeed, although the final model accounted for approximately 30% of the variance of PTSD case status (likelihood ratio (LR) χ2(7) = 69.91, p ≤ 0.000, R2 = 0.305), removal of the family resilience variable minimally changed the model R2 (from 0.305 to 0.299), and on an LF test (model without family resilience nested within final model) there was no evidence that family resilience is a risk factor for disaster-induced PTSD (LR χ2 1 = 1.79, p = 0.181).
Logistic regression: multivariate relationships with child PTSD
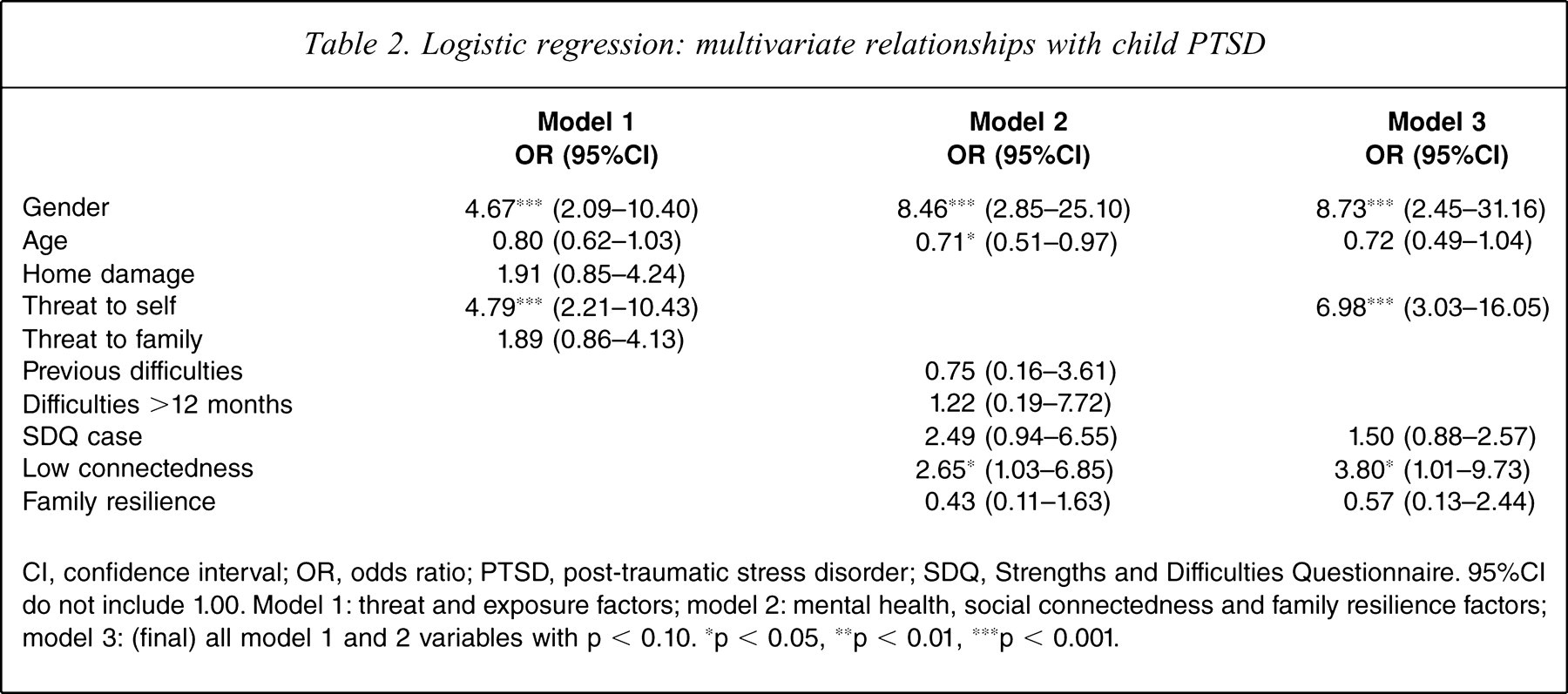
CI, confidence interval; OR, odds ratio; PTSD, post-traumatic stress disorder; SDQ, Strengths and Difficulties Questionnaire. 95%CI do not include 1.00. Model 1: threat and exposure factors; model 2: mental health, social connectedness and family resilience factors; model 3: (final) all model 1 and 2 variables with p < 0.10. ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001.
These data do not provide evidence for a main effect for family resilience in predicting disaster-induced child PTSD. Effect modification was tested for family resilience and age, gender and threat perception by comparing crude and adjusted ORs. There was no effect modification of age by resilience (interaction term ORadj = 0.83, 95%CI = 0.31–2.18, p = 0.700), gender (test of homogeneity of ORs χ2 1 = 0.35, p = 0.552), or threat perception (test of homogeneity of ORs χ2 1 = 0.87, p = 0.352).
Discussion
PTSD causal models are conceptualized as multifactorial, encompassing both event-related and distal variables, the latter including both protective and vulnerability factors. Data from children who experienced Cyclone Larry replicated the importance of threat perception and exposure as well as a new protective factor, the child's report of their social connectedness (McDermott, Cobham, Berry et al: unpublished data, 2010). In the present study we have expanded the conceptual model of PTSD to include family resilience and past history of mental illness, both conceptualized as potential vulnerability factors. Consistent with this, in the present sample low family resilience was significantly associated with emotional problems on the SDQ and the duration of child mental health problems ≥12 months.
There is face validity that membership of a family with low resilience may confer a vulnerability to the child experiencing disaster-induced PTSD, through low flexibility when faced with adversity, inconsistent problem solving, a diminished sense of belonging to a traumatized community or psychological processes including feeling less emotionally contained, more threatened, fearful, abandoned and unsupported, or by a direct process such as family resilience being associated with less direct exposure to the disaster. In the present sample, however, low family resilience was not related to disaster-induced child PTSD or with event-related factors such as experiencing evacuation. Further, family resilience did not modify the effect of other significant factors such as the perception of threat to self. We also report no significant association between children's past mental illness history and disaster-induced PTSD. Although this finding needs replication the analysis suggests that children with existing mental health problems and those of low-resilience families are not at elevated risk of disaster-induced PTSD in the short term. Indeed, the present findings provide some evidence that the aetiological model of child PTSD may differ from usual child and adolescent conceptualizations. The subgroup of children with existing mental health problems may not be an at-risk group, rather all children, but especially girls, may be vulnerable to disaster-induced PTSD given sufficient exposure and perception of threat to self. The relationship of social connectedness to family resilience and why connectedness but not family resilience was associated with disaster-induced PTSD require further investigation. The present results raise two questions: is family resilience unrelated to PTSD in children following natural disasters, or is our understanding of the aspects of family functioning that constitute resilience still in its infancy? For both the parent-report measures used in the present study, the SDQ-EM and FRM, the mean scores in this sample were lower (i.e. more normal) than published norms. It may be that surviving a disastrous event may lead to a systematic reporting bias in which parents consider aspects of child and family functioning more normal. Further research is needed to refine and test available measures of family resilience against the theoretical models proposed, and to demonstrate real-world applicability.
There are limitations to the present study: the measure of family resilience and its lack of relationship with post-disaster symptoms does not preclude other family factors being identified, such as parenting style and parent mental health factors that may contribute to a model of child disaster-induced PTSD. The comprehensiveness of the causal model being investigated in the post-disaster scenario is always a challenge. Individuals, especially parents, are rightly focused on returning family life to normal and contending with the hierarchical needs of adequate shelter and safety for family members, rather than being engaged in research. Further, research is relatively sparse considering factors that post-date rather than pre-date the disaster.
In the present study the measure of family resilience focused on the families’ ability to deal with adversity. The drive to researching this area is to identify factors that may confer resilience and that therefore could be used as preventative interventions in disaster-prone areas. Future research directions should focus on alternative aspects of family and parent functioning that are hypothesized as independent contributors, and these may include a family history of anxiety disorders, past parental traumatic experience and abnormal family functioning. Research is also required to investigate whether family resilience may be a predictive factor for medium- and long-term psychosocial functioning or relate to treatment adherence and outcome.
Footnotes
Acknowledgements