
Abstract
Objective:
To estimate the Danish epidemiological long-term incidence rates for suicide attempts in the general population of children and adolescents, and to analyze the impact from single and multiple risk factors on the risk of suicide attempts.
Method:
We used longitudinal register data from a total cohort of all individuals born between 1983 and 1989 and living in Denmark to calculate incidence rates. From the cohort, we identified all who have attempted suicide, and matched 50 controls to each case. A nested case–control design was used to estimate the impact from risk factors on the risk for index suicide attempts. We established a link to the biological parents and identified risk factors for two generations. Risk factors were analyzed in a conditional logistic regression model.
Results:
We identified 3718 suicide attempters and 185,900 controls (189,618 individuals, aged 10–21 years). We found increasing incidence rates during the period 1994–2005, and higher incidence rates for girls and the oldest adolescents. Mental illness was the strongest independent risk factor (IRR = 4.77, CI = (4.35–5.23), p < 0.0001), but parental mental illness (psychopharmacological drugs: IRR = 1.27, CI = (1.18–1.37), p < 0.0001) and socio-demographic factors (parents not living together: IRR = 1.38, CI = (1.28–1.48), p < 0.0001) were also significant independent risk factors. Exposure to multiple risk factors increased the risk significantly.
Conclusions:
Suicide attempt is a multi-factorial problem, and a problem on the increase in the period studied. Individuals exposed to multiple risk factors are at the highest risk for suicide attempts, and when spotted or in contact with authorities they should be given proper care and treatment to prevent suicide attempts and death.
Introduction
It is a well-known fact that children and adolescents are at high risk of suicide attempts. Estimates of incidence rates have been made previously, but based on cross-sectional studies and often from clinical populations. A Belgium monitoring study based on accident and emergency department data from one department showed declining incidence rates for adolescents aged 15–19 years in the period 1996–2001, but rising rates after 2001. For 2004, the incidence rate for female adolescents was estimated at 528 per 100,000 and for males about 190 per 100,000 (De Munck et al., 2009). A Norwegian cross-sectional study estimated the 1-year suicide attempt incidence rate during 1998– 2000 at 900 per 100,000, based on a population of school adolescents aged 12–15 years in two counties (Larsson and Sund, 2008). Bridge et al. (2006) reviewed the literature between 1990 and 2005 in order to examine the descriptive epidemiology of youth suicidal behavior. They reported lifetime estimates of suicide attempts among adolescents ranging from 1.3% to 3.8% in males and 1.5% to 10.1% in females, with higher rates in females and in the older adolescent age range; however, they did not report trends in incidence rates. The suicide rate is high in a population of individuals who have previously attempted suicide, and they form a well-defined high-risk group for suicide and premature death (Christiansen and Jensen, 2007), making it highly relevant to study this group of children and adolescents in order to prevent premature deaths and suicides.
Individuals with suicidal behavior or ideation are more often exposed to stressors and risk factors than others. The incidence of mental illnesses is high in a population of young suicidal individuals (Agerbo et al., 2002; Beautrais, 2000). Some mental illnesses are more related to suicidal behavior than others: Affective disorders, substance use disorders and antisocial disorders are the major psychiatric contributors to suicidal behavior in young people (Beautrais, 2000). Other social and family risk factors are also significantly associated with young people’s suicidal behavior (e.g. low socioeconomic status, parents not living together, parental psychopathology, family history of suicidal behavior and stressful life events) (Beautrais, 2000; Bridge et al., 2006). Often, cross-sectional studies are used to estimate risk factors but, in this study, we will use longitudinal register data and a strong epidemiological design (nested case–control) to estimate risk factors for suicide attempts in a national representative sample of children and adolescents who have attempted suicide. The structure of the registers allows us to analyze risk factors from two generations (offspring and parental) and to analyze effects from a large sample. It is a method only possible in some Scandinavian countries, but it has hardly ever been done in the context of suicide attempt.
In her PhD thesis, Beautrais analyzed the impact from multiple risk factors on the risk of suicide attempts in children and adolescents, and she concluded: ‘It is clear that with increasing risk factor exposure for suicide attempts, odds of risk of serious attempt rise dramatically’ (Beautrais, 1996). A recent study analyzed the dose–response relationship between the number of exposures to parental risk factors and the risk of suicide attempts in children and adolescents, and concluded that the increased risk appears to have a multiplicative effect (Christiansen et al., 2011). Not all risk factors raise the risk of suicide attempts with the same impact, and mental disorders seem to have the strongest impact on risk. Neither Beautrais nor the latter study takes this into account. There is a lack of knowledge on the impact of multiple risk factors on risk, and in relation to risk assessment we need a better understanding of how multiple risk factors affect the risk of suicide attempts among children and adolescents.
The aims of this study are to calculate the incidence rates of suicide attempts for children and adolescents; to identify the most substantial risk factors (own or parental) for children and adolescents who have attempted suicide; and to estimate the impact from multiple risk factors on the risk for suicide attempts. We will use Danish register data and a high-quality epidemiological design (nested case–control) to make the estimates. A number of high-quality register-based studies have examined risk factors for suicide in adults (Agerbo et al., 2002, 2006; Qin et al., 2002, 2006), but only a few have analyzed suicide attempt as the outcome variable in a young population (Christiansen and Larsen, 2012; Christiansen and Stenager, 2012; Christoffersen et al., 2003).
Methods
Data sources
Each individual in Denmark has a unique personal civil registration number (CPR), which is used across all registration systems (Pedersen et al., 2006). We used CPR numbers to merge data from various registers, including The Danish Fertility Database (includes all links between children and parents and some socio-demographic information) (Knudsen, 1998), The Danish Registers of Causes of Death (includes all deaths in Denmark) (Juel and Helweg-Larsen, 1999), The Danish National Patient Registry (includes all contacts to medical departments) (Andersen et al., 1999), The Danish Psychiatric Central Register (includes all contacts to psychiatric departments) (Munk-Jorgensen and Mortensen, 1997), The Income Statistics Register (includes all types of income) and The Student Register (includes all levels of finished and on-going education).
Sample
A full cohort of all individuals born between 1983 and 1989 and living in Denmark was sampled from The Danish Fertility Database (Knudsen, 1998). To identify the children or adolescents’ suicide attempt, we adopted a definition as close as possible to the one used by the World Health Organization (Bille-Brahe et al., 1995).
In the present study, we defined ‘suicide attempt’ as contact with a medical or psychiatric department when:
the reason for contact was coded E4 (suicide attempts), and the diagnostic code was one of the following: S617–S619 (open wound of wrist and hand), T36x–T60x, T65 (poisoning/toxic effects by drug, substances etc.) and X60x–X84x (intentional self-harm);
or an f-diagnosis as action diagnosis, and a diagnostic code of T36x–T50x (poisoning by drugs), T52x–T60x (poisoning effects by substances), S51x (wound of forearm), S55x (injury of blood vessels at forearm), S59x (other injuries of forearm), S61x (wound of wrist and hand), S65x (injury of blood vessels at wrist and hand) or S69x (other injuries of wrist and hand) as the secondary diagnosis;
or contact with a psychiatric department when:
given a diagnostic code of X60x–X84x (suicide attempt).
This procedure is inspired by a study by Helweg-Larsen and colleagues (2006). Somatic and psychiatric contacts are assigned to different registers, which is why we merged data from the National Patient Register and the Danish Psychiatric Central Register to create the case population. We searched all records in the registers, which include all inpatient, outpatient and emergency department (somatic and psychiatric) contacts. We only included children and adolescents from the relevant cohorts who were at least 10 years old and attempts made before 2006. The final case sample included 3718 young people who had attempted suicide. For all cases, the date of the first registered suicide attempt was identified (index attempt).
Analysis
The data were analyzed in two different designs. Sex- and age-specific annual incidence rates were calculated by the actuarial method using all index suicide attempts done by the full cohort. Confidence intervals for the rates were also calculated. The date of the index attempt was identified, and by using data from Statistics Denmark we identified all individuals of the same age and sex as the case population in the period 1994–2005. Sex-specific annual incidence rates were calculated for the age groups 10–13 years, 14–16 years and 17–21 years for the period 1994–2005. The differences in the level of incidence rates over time for the two sexes and three age groups were tested by use of chi-squared tests of model parameters in a Poisson regression model (Breslow and Day, 1987). As the incidence rate only includes index suicide attempts, repetitions of suicide attempts are not included.
In order to control for the influence of sex and age on risk for suicide attempts, a nested case–control study was designed to analyze the impact of risk factors on risk for suicide attempts. A high number of randomly selected controls (50 non-attempters) were matched to every attempter (case) by sex and age, on the date of the case’s first suicide attempt (matching date) (Breslow et al., 1983). A total of 189,618 children and adolescents were included in the nested case-control study. The nested case–control data were analyzed using conditional logistic regression with each case and its controls forming a separate stratum. As the controls were selected randomly within the appropriate risk sets and at the time when the case attempted suicide, estimated odds ratios are incidence rate ratios (IRRs) (King and Zeng, 2002). We also reported p-values and 95% confidence intervals (CIs). IRRs were calculated for the three age groups, and for all. We only analyzed information prior to the time of the matching date (i.e. only data from before the case’s index suicide attempt).
All risk factors were coded as dummy variables and analyzed on unadjusted and adjusted levels. The child or adolescent’s contact with a psychiatric department was defined when contact was made as an inpatient, an outpatient or with the emergency department for psychiatric care. Based on the offspring’s contact with the psychiatric department, four groups of diagnoses were created: depressive episode (F32 (ICD-10) and 296.0, 296.2, 296.9, 298.0, 300.4 (ICD-8)); reaction to severe stress and adjustment disorders (F43 (ICD-10) and 307 (ICD-8)); specific personality disorders (F60 (ICD-10) and 301, 302 (ICD-8)); and conduct disorders and emotional disorders (F91, F93 (ICD-10) and 308 (ICD-8)). The four diagnoses were not included in the adjusted analysis as we wished to make estimates of contact with the psychiatric department unadjusted for specific mental illnesses.
It was also possible to extract data about drugs prescribed for individuals in the period 1995–2006. Prescription drugs affecting the central nervous system were defined as an individual being prescribed antipsychotics, anxiolytics, psychoanaleptics, antiepileptic drugs or drugs for substance dependence. A child or adolescent’s contact with the medical department was defined when contact was made as an inpatient, an outpatient or with the emergency department because of abortion, violence, epilepsy, asthma, diabetes, cancer or malformations. An offspring’s adoption was defined when the offspring had been adopted. Primary school was defined when the offspring’s highest completed level of education was primary school. Offense was defined when the offspring had been convicted of any kind of offense. Parental contact with the psychiatric department, the medical department, prescription drugs affecting the central nervous system, offense, suicide attempt and primary school were defined in the same way as for the offspring. Parental death was defined by identifying dead parents. Parental income was created by adding together both parents’ income in the year before the offspring’s attempted suicide, adjusting it to 2006 prices according to the consumer price index and grouping it into four groups: lowest third, middle third, highest third and unknown. Only the lowest third was analyzed. Parental unemployment was defined as at least one of the parents being unemployed more than 20% of the time in the year before the offspring’s index attempt. Parents not living together was defined as biological parents not living in the same family.
Counting up the number of risk factors for each individual gave the distribution of multiple risk factors. The distribution for cases was compared with the distribution for controls. We created four new risk dimensions (factors) by adding related factors together into four new risk dimensions. The first risk dimension accounts for parental social risk factors (contact with medical department, death, offense, not living together, unemployed, low income and adoption of ‘offspring’). The second risk dimension accounts for parental mental illness (contact with psychiatric department, drugs affecting the central nervous system and suicide attempts). The third dimension accounts for the offspring’s social risk factors (contact with medical department, offense and primary school). The fourth risk dimension accounts for the offspring’s own mental illness (contact with psychiatric department and drugs affecting the central nervous system). The four risk dimensions were dichotomized into yes/no categories and coded into dummy variables. Based on the four dummy variables, we created 16 new dummy variables, including first, second and third degree of interaction (i.e. all possible interactions). The risk factors and the 16 new dummy variables were analyzed in a conditional logistic regression model, which returned incidence rate ratios, p-values and 95% CIs.
Results
The epidemiological long-term incidence rates
Figure 1 is a graphic presentation of developments in general incidence rates for the cohort of male and female children and adolescents born between 1983 and 1989. In all age groups, females are at higher levels and children (aged 10–13 years) are at the lowest level. For the lower and middle age groups, incidence rates increased during the period. For the youngest females the incidence rate rose from 7.7 per 100,000 in 1994 to 119 per 100,000 in 2003. For females in the middle age group, the incidence rate rose from 143.3 per 100,000 in 1997 to 291.5 per 100,000 in 2005. The rate was for the oldest females at a level of 259.3 per 100,000 in 2000 and at almost the same level in 2005 (250.2 per 100,000). The same pattern was to be found among males, but at a significantly lower level.
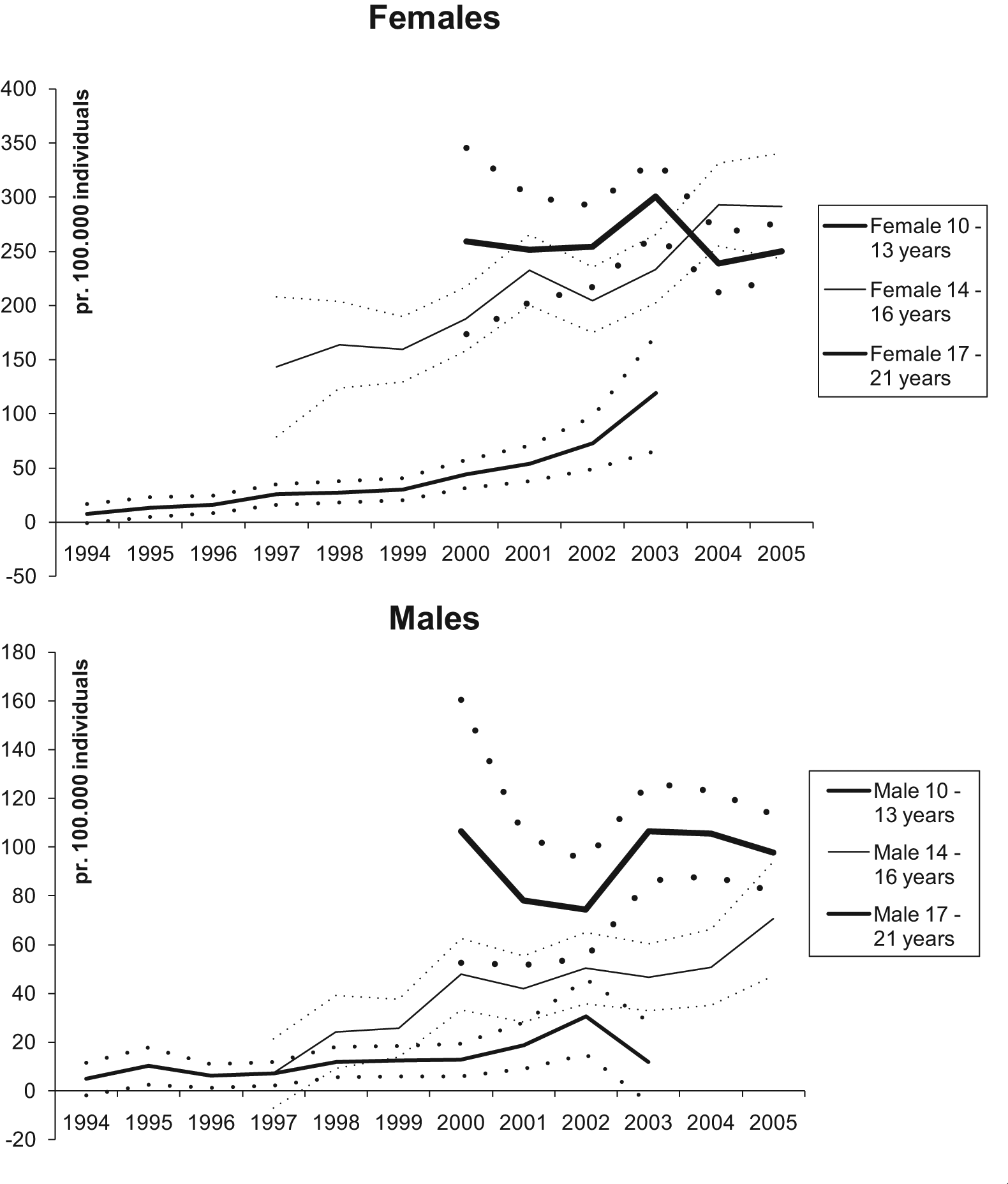
Incidence rates (solid lines) and confidence intervals (dotted lines) of suicide attempts among adolescents/youths aged 10–21 years, covering an 11-year period by age group. (We are analysing a birth cohort of children born between 1983 and 1989: none of them was below 13 years old in the period 2004–2005; none of them was between 14 and 16 years old in the period 1994–1996; and none of them was between 17 and 21 years old in the period 1994–1999).
The test results showed a significant increase in incidence during the period (p < 0.0001), a significantly higher incidence for girls (p < 0.0001) and significantly lower incidence rates for the two youngest age groups compared to the oldest (p < 0.0001).
Risk factors
Unadjusted level
All the risk factors are listed in Table 1 (unadjusted and adjusted estimates) and Table 2 (unadjusted and stratified by age and indicator for significant adjusted estimates). The tables include numbers of cases and controls in each category, the incidence rate ratio, p-value and CI for the rate ratio. For all age groups ‘Contact with psychiatric department’ was a strong risk factor, but it was strongest for the oldest age group (stratified estimate: IRR = 11.2, CI = (10.2–12.3), p < 0.0001). The diagnostic group ‘Disorder of adult personality and behavior’ had the highest risk among the diagnoses analyzed (unstratified estimate: IRR = 23.5, CI = (20.2–27.3), p < 0.0001). ‘Prescription drugs’ was the second highest risk factor for all age groups. Among the rest of the offspring’s own risk factors, ‘Contact with medical department’ and ‘Offense’ had a high impact on the risk. Among parental risk factors, ‘Contact with psychiatric department’ (unstratified estimate: IRR = 2.48, CI = (2.3–2.67), p < 0.0001), ‘Prescription drugs affecting the central nervous system’ (unstratified estimate: IRR = 2.08, CI = (1.95–2.22), p < 0.0001), ‘Suicide attempt’ (unstratified estimate: IRR = 3.33, CI = (2.97–3.74), p < 0.0001), ‘Parents not living together’ (unstratified estimate: IRR = 2.17, CI = (2.04–2.32), p < 0.0001) and ‘Low income’ (unstratified estimate: IRR = 2.04, CI = (1.91–2.17), p < 0.0001) had the highest impact on the offspring’s risk of attempted suicide. Not all risk factors were significant factors for the two youngest age groups, due either to lack of impact on risk or to low statistical power. For the youngest age group, it was not possible to estimate the incidence rate ratio for ‘Primary school’ as they were still too young to have finished primary school.
Risk factors for children and adolescents’ suicide attempts. Crude and adjusted levels for all.
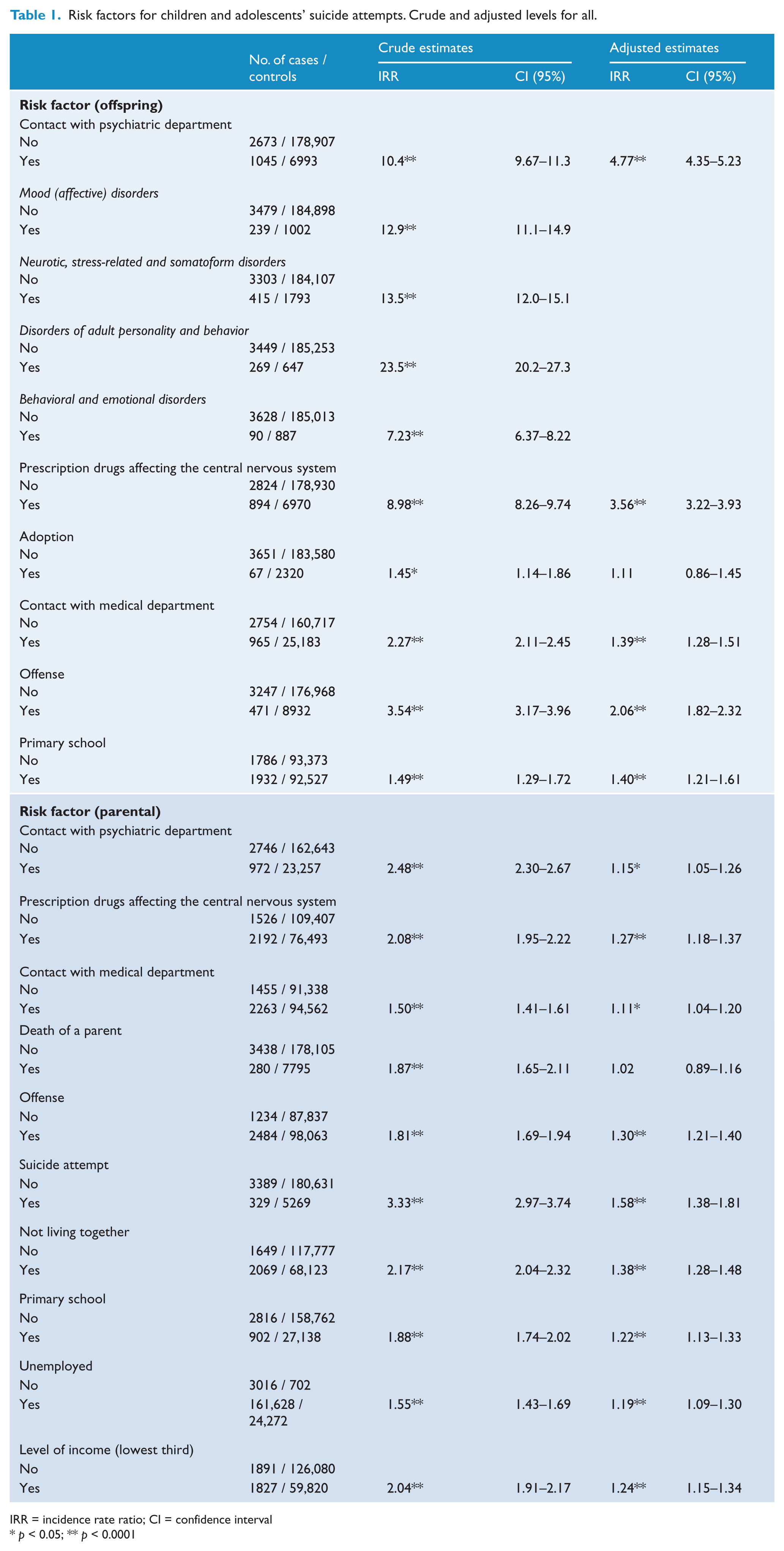
IRR = incidence rate ratio; CI = confidence interval
p < 0.05; ** p < 0.0001
Risk factors for children and adolescents’ suicide attempts by age groups.
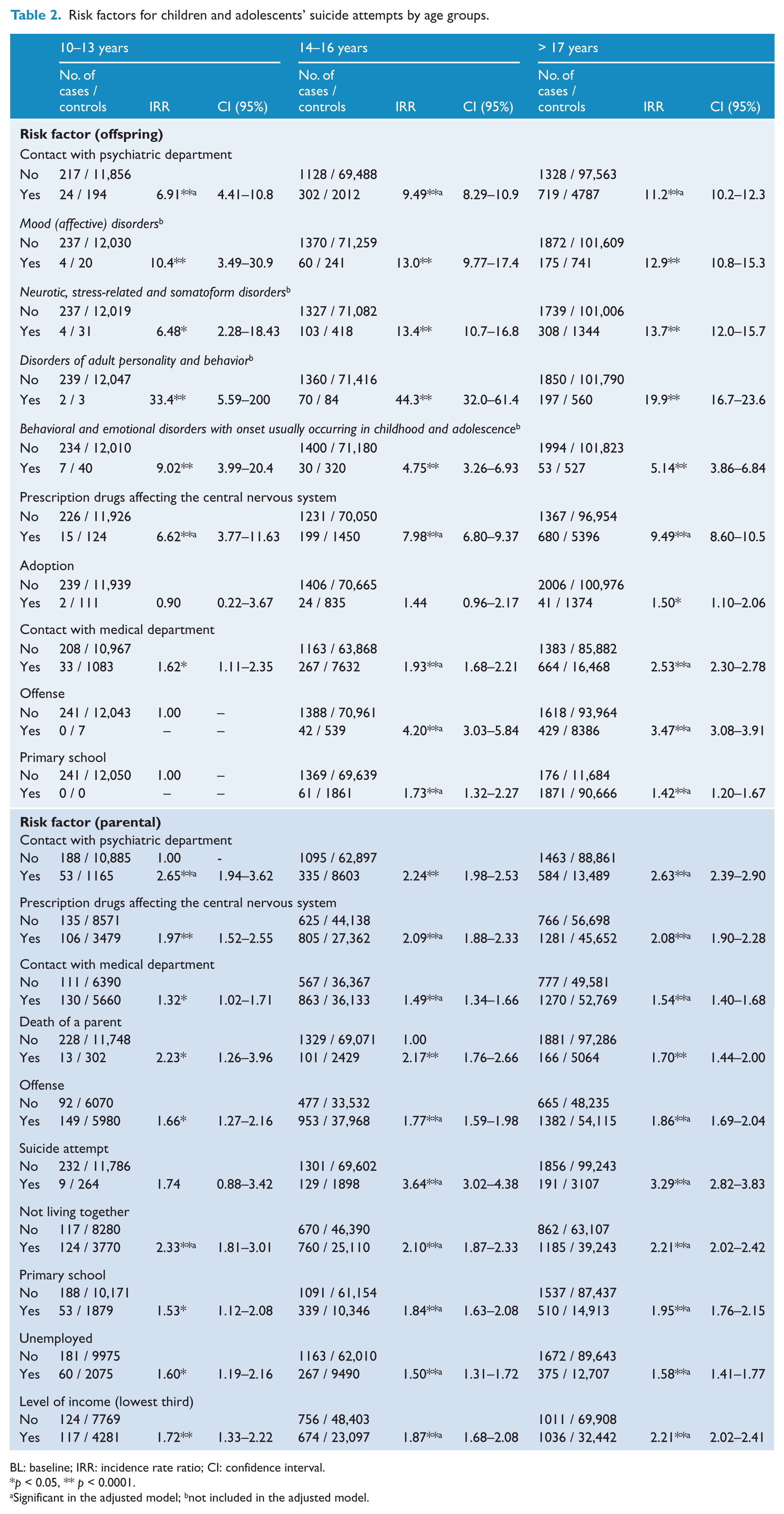
BL: baseline; IRR: incidence rate ratio; CI: confidence interval.
p < 0.05, ** p < 0.0001.
Significant in the adjusted model; bnot included in the adjusted model.
Adjusted level
In the unstratified analysis, only ‘Adoption’ and ‘Death among parents’ came out as insignificant risk factors in the adjusted analysis, and the impact from the factors was generally lowered. ‘Contact with psychiatric department’ was lowered from IRR = 10.4 to IRR = 4.77, ‘Prescription drugs affecting the central nervous system’ was lowered from IRR = 8.98 to IRR = 3.56 and parental ‘Suicide attempt’ was lowered from IRR = 3.33 to IRR = 1.58. The lowering of the factors indicated correlation among the factors but many were still highly significant. For the youngest age group, it was only the child’s own contact with the psychiatric department, use of prescription drugs affecting the central nervous system, parents’ contact with psychiatric services and parents not living together which were significant risk factors in the adjusted analysis. Parental use of prescription drugs affecting the central nervous system was significant in the adjusted analysis at a p = 0.055 level. The significant risk factors in the adjusted model were the same as for the two other age groups, except that parental contact with the psychiatric department was significant only for the oldest age group.
Dose–response
Figure 2 shows the frequency distribution for the number of risk factors that cases and controls are exposed to. Cases are more likely to be exposed to many risk factors, but a significant proportion of the controls are also exposed to many risk factors. This analysis also shows that a significant proportion of the cases are exposed to only a few risk factors. Impact on the offspring’s risk of suicide attempts from the 16 different combinations of the four risk dimensions is shown in Table 3. The presence of the offspring’s mental illness dimension increases risk significantly (none overlapping CI), and multiple risk dimensions increase risk more than being exposed to a few or a single risk dimension. Individuals exposed on all four risk dimensions had an IRR of 25.5 (CI = (19.6–33.1), p < 0.0001) and individuals exposed on three risk dimensions, but not on ‘offspring mental’ risk dimension had an IRR of only 3.95 (CI = 3.04–5.12), p < 0.0001). The table also shows that if the offspring’s mental illness dimension is present, then it is very likely that other risk dimensions are also present, especially for suicide attempters (cases).
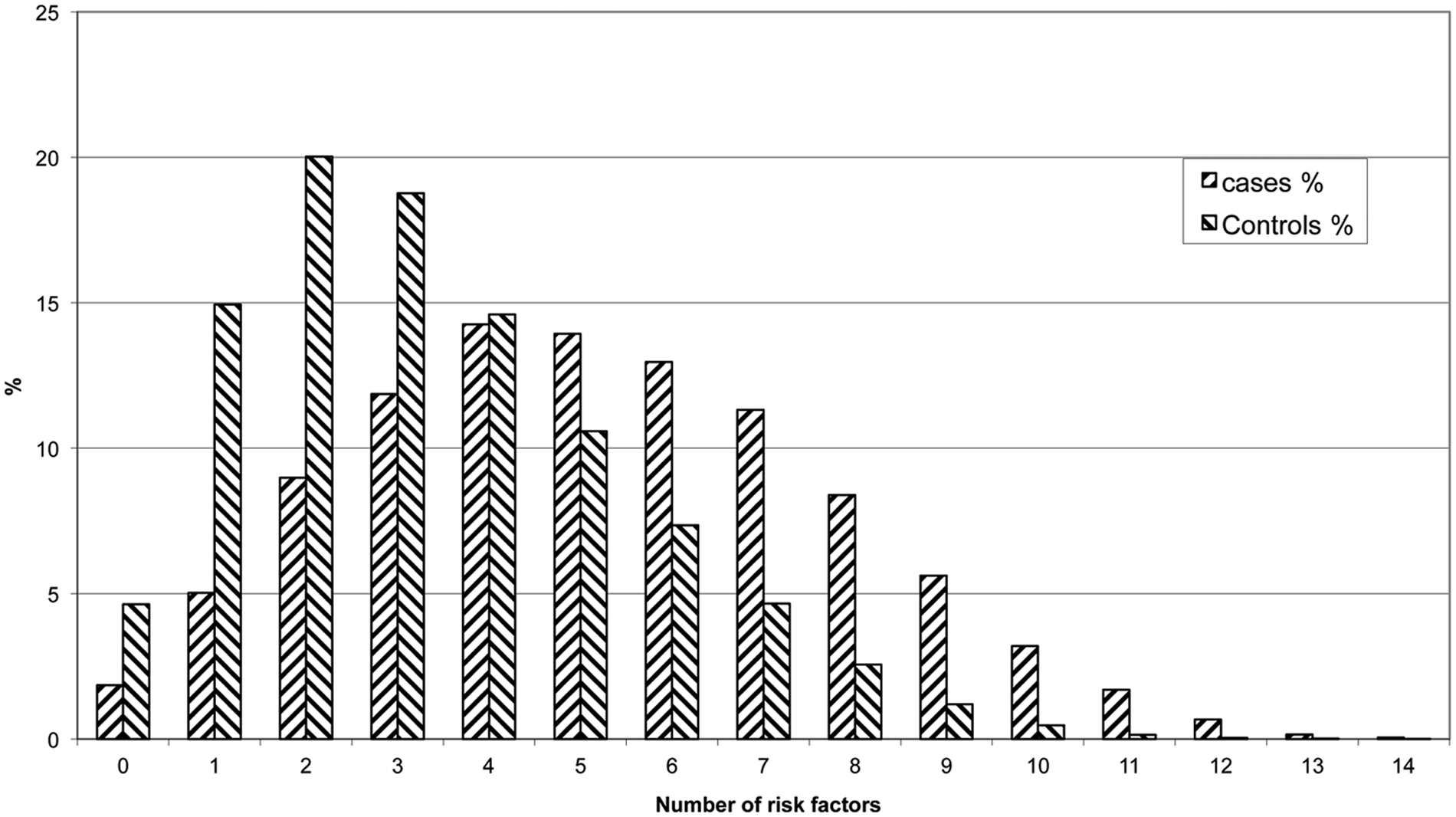
Frequency distribution of the number of risk factors for cases and controls.
All possible combinations of the four risk dimensions (social, mental) for adolescents and parents.
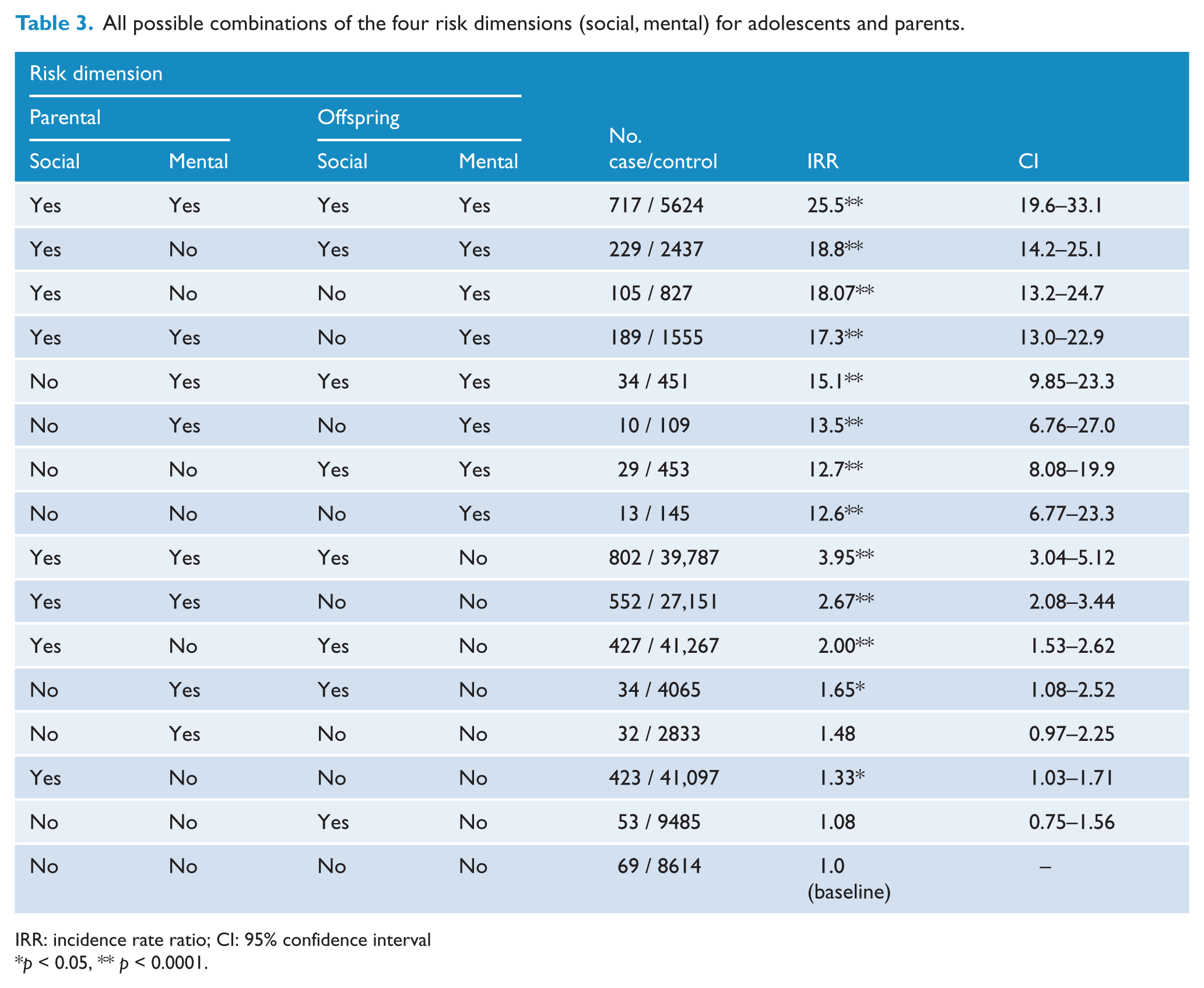
IRR: incidence rate ratio; CI: 95% confidence interval
p < 0.05, ** p < 0.0001.
Discussion
Results in brief
We have estimated the incidence rate for suicide attempts among children and adolescents in this two-generation longitudinal study and found increasing rates during the period 1994–2005, as well as higher rates for females than males. We analyzed risk factors from two generations, finding the offspring’s own mental illness to be the strongest risk factor for suicide attempts; however, parental mental illness and socio-demographic factors are also significant independent risk factors for the offspring’s suicide attempts. The number of risk factors was reduced to four risk dimensions. After analyzing all possible combinations of these dimensions, we found that the offspring’s own mental illness accounted for the biggest part of the risk, but also that individuals exposed to all four risk dimensions were at the highest risk for suicide attempts.
Limitations
We used a cohort design in order to calculate the incidence rates as it was possible to include all individuals from the 1983 to 1989 birth cohorts. We used a case–control design in order to estimate impact from risk factors on risk for suicide attempts. In the case–control design, it is possible to eliminate effects from age, sex and calendar time by the use of matching. The groups of cases and controls were formed on the basis of registers; however, it seems likely that not all incidences of suicide attempts were registered correctly in the registers. Some individuals having attempted suicide might therefore erroneously have been used as controls, as it is not to our knowledge that they have attempted suicide. If these false negatives are similar with respect to risk factors to other suicide attempters, then the incidence rate ratio will be underestimated. It would be even more serious if some cases were false positives and therefore not related to suicide attempts. However, this is unlikely to be the case (Nordentoft and Sogaard, 2005). The increasing incidence rate might be biased owing to changes in registration practice or erroneous registration of suicide attempts. Registration is extensive and often flawed, particularly in terms of contact reason, implying that suicide attempts in some cases are incorrectly recorded and therefore not included in this study (Nordentoft and Sogaard, 2005).
Incidence rates
Since 1989 the Danish Centre for Suicide Research has systematically collected information on all suicide attempts in the county of Funen. Suicide attempts are filed in an official register, Register for Suicide Attempts (Christiansen and Jensen, 2004), and the data used to monitor trends in suicide attempt incidence rates. The register does not contain suicide attempts made by children below the age of 15. Estimates of incidence rates are higher when using data from the Register for Suicide Attempts compared with our estimates, but the patterns are very similar. To our knowledge, this is the first Danish estimate of incidence rates for children below 15 years of age. The pattern of the youngest age group is similar to those of the two older age groups. Our estimates of the incidence rate for suicide attempts in the age group 12–15 years (90 per 100,000 in 2002) are approximately one-tenth of the estimates from Norway (900 per 100,000 for 1998–2000) (Larsson and Sund, 2008). Our estimates include only a proportion of hospitalized suicide attempters, whereas the cross-sectional study from Norway is based on representative samples from all schools in two counties. Other studies show that only a small proportion (5–16%) of adolescents with deliberate self-harm are hospitalized after the episode (Hawton et al., 2002; Rossow and Wichstrom, 1997; Ystgaard et al., 2003).
Risk factors
We chose to include many risk factors in order to create a universal characteristic of children and adolescents who have attempted suicide. Some risk factors may therefore reflect a high degree of heterogeneity, since for some individuals they can be less heavy stressors while for others they can be very heavy stressors; for some individuals they may even be a protective factor. We analyzed the risk factors for three different age groups in order to compare incidence rate ratios. For all age groups, ‘Contact to psychiatric department’ was the strongest risk factor for suicide attempts, followed by ‘Prescription drugs affecting the central nervous system’, which was highest for the oldest age group. Other studies have also found a strong association between suicidal behavior and mental illness in young people (Portzky and Van Heeringen, 2007). Young children may be in a better position to manage their mental illness through contact with adults, support from authorities, schools and networks, and through lower incidence of disorders related to abuse, personality disorders and suicidal behavior. By contrast, teenagers can be more autonomous, have less access to family, authorities, schools and networks, and suffer from mental disorders more strongly related to suicidal behavior. We found the same pattern for ‘Contact with medical department’: teenagers are at the highest risk of suicide attempts after contact due to abortion, violence, epilepsy, asthma, diabetes, cancer or malformations. Similar results were found by the authors in another study (Christiansen and Stenager, 2012). Abortion and violence are incidences related to middle-to-late teenage years and may explain the high incidence rate ratios for the two oldest age groups. Fergusson and colleagues (2006) analyzed the association between abortion and mental health problems in a high-quality longitudinal study of young women. They found significant protective risk ratios (adjusted) for mental problems and suicidal ideations among young women who had not had an abortion, compared to women who had had an abortion. Discussing whether abortion has a harmful effect on mental health, they concluded that it is difficult to disregard the fact that abortion is associated with an increased risk of mental health problems, but that further well-controlled studies are needed on the subject.
Among the highest effects from parental risk factors we found ‘Parental suicide attempts’ and mental illness. Parental psychopathology and suicide attempt (also suicide) might be related events, but a twin study has demonstrated the presence of genetic vulnerability to non-fatal suicidal behaviors which cannot be fully explained by genetically influenced psychopathology (Pedersen and Fiske, 2010). Part of the risk for suicide attempt might therefore be genetically transmitted to the offspring independently of genetically influenced psychopathology and environment. In this study we found that parental mental illness and suicide attempt were independent significant risk factors in the adjusted model, which supports the hypothesis.
The independent significant risk factors for the youngest age group are more related to mental illnesses and the child–parent relation. For the two oldest age groups, other factors are also significant independent risk factors. The problems related to suicide attempts are attributed to more factors the older the offspring is. The interaction between the factors may be complex, as factors can be mediating, confounding and even moderating factors. A Danish longitudinal register-based case–control study found that the mother and father’s suicide and mental illness were independent significant risk factors for the offspring’s suicide and that other socio-demographic factors were insignificant factors (Agerbo et al., 2002). In this study, suicide attempters were more likely to come from disrupted and lower socioeconomic families; similar results were found by Beautrais in her case–control study of 129 suicide attempters (Beautrais et al., 1998).
Dose–response
As can be seen from Figure 2, during the period at risk, cases are more likely to be exposed to many risk factors, and controls are more likely to be exposed to few risk factors. The pathway to suicidal behavior could be through an accumulation of risk, where the risk factors may be static or dynamic in size. In some cases, the dynamic risk factors may be moderated by protective factors. The interaction between risk and protective factors is sparsely described in the literature, despite the fact that such interactions could be important in relation to the design of prevention programs and treatment of suicidal children and adolescents. Being exposed to a high number of different risk factors is an indicator of increased risk of suicide attempts. However, when using this indicator to predict suicidal behavior we must take into account that many false positives may be included as well (individuals who will not attempt suicide despite the presence of multiple risk factors).
As can be seen in Tables 1 and 2, risk factors are not affecting risk with equal impact. In order to analyze interaction between risk factors and accumulation of risk, we reduced the number of risk factors to four risk dimensions. The results are presented in Table 3. An offspring’s own mental illness is a dominant risk dimension, which alone and in combination with other risk dimensions increases the risk significantly. Multiple risk dimensions (with and without the offspring’s mental illness) also increase risk to the highest level, which shows a dose–response relation between the number of risk dimensions and the risk of suicide attempt. If an individual (parent or offspring) is exposed on the mental dimension, the individual is highly likely to be exposed on the social dimension as well, but the probability of the opposite is much lower. It is very rare that the offspring’s mental dimension stands alone.
Conclusion
Suicide attempt is a multi-factorial problem among adolescents, and mental illness is the strongest risk factor for suicide attempt. Still, it is very difficult to predict suicidal behavior for individuals based on group estimates of risk factors, and many adolescents are exposed to such factors without having a suicide attempt. Knowledge about interaction between risk and protective factors might help towards a better risk assessment, and this study contributes to the field by adding that adolescents exposed to multiple risk factors are at the highest risk of attempting suicide, especially if suffering from mental illness as well. Clinicians should incorporate this knowledge in their risk assessment. We would recommend more research on the subject of interaction between risk factors for suicidal behavior in large population-based samples, including psychological risk factors, which was not possible to include in this study.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.