
Abstract
Objective:
The frequency and emotional response to bullying victimisation are known to be associated with adolescent mental ill health. A potentially important under-investigated factor is the form of bullying. Four common forms of bullying behaviours are name-calling, physical threats or harm, rumour spreading and social exclusion. To more comprehensively understand bullying victimisation in adolescence, we examined the association of all three factors (frequency, emotional response, form) to psychological distress and emotional wellbeing.
Method:
A stratified, random sample of adolescents (n = 10, 273; mean age = 14.33 years, standard deviation = 1.68 years) completed validated measures of bullying victimisation (Gatehouse Bullying Questionnaire), psychological distress (K10) and emotional wellbeing (Mental Health Inventory) in classroom time. Associations between the form of bullying victimisation and mental health outcomes were examined.
Results:
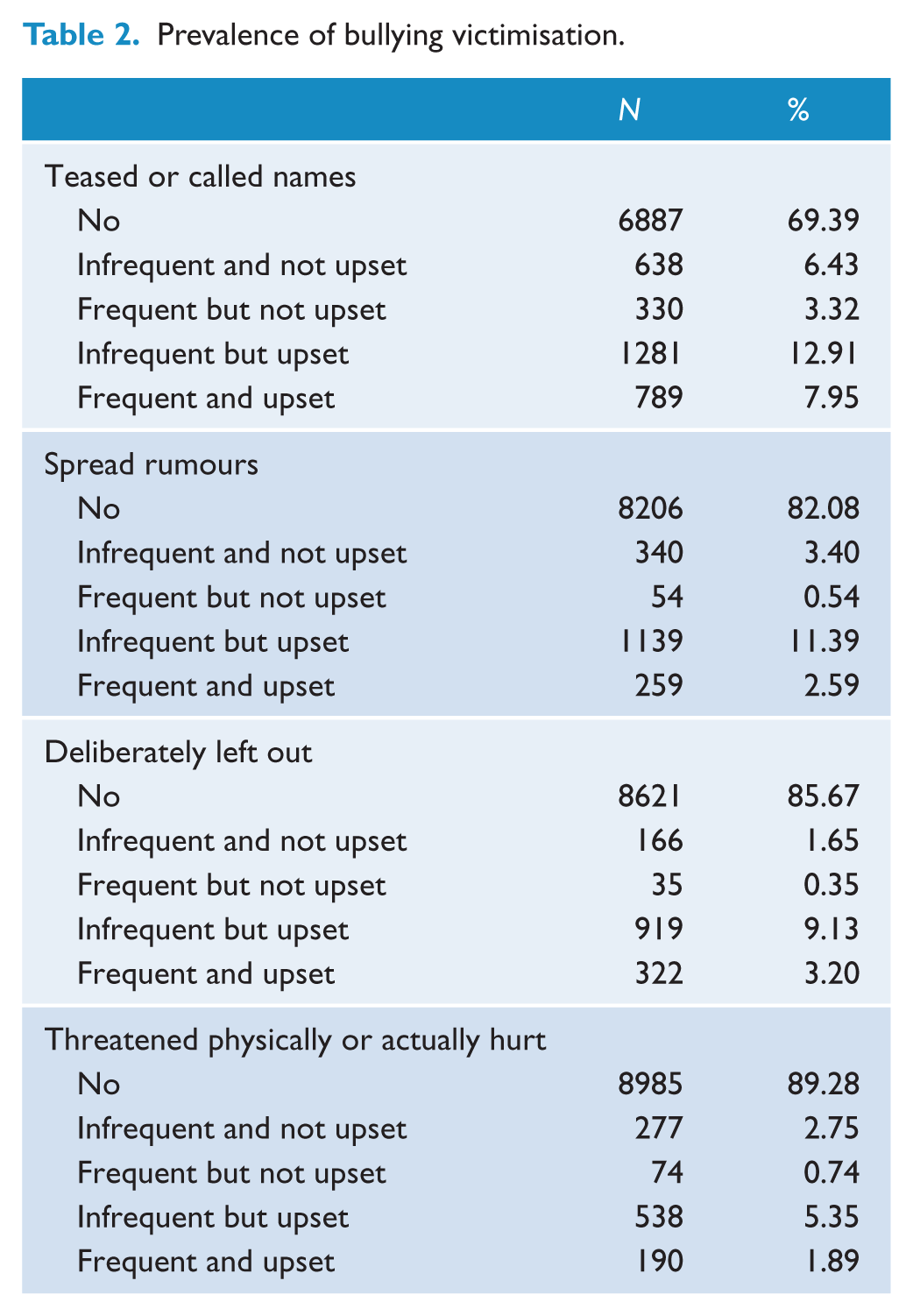
Adolescents reported a high prevalence of all four forms of bullying: teased or called names (30.6%), rumour spreading (17.9%), social exclusion (14.3%) and physical threats or harm (10.7%). Victimisation was independently associated with significantly higher levels of psychological distress and reduced levels of emotional wellbeing for all forms of bullying. In particular, social exclusion had a strong association with mental ill health. Adolescents who experienced frequent bullying that was upsetting reported higher psychological distress and reduced emotional wellbeing.
Conclusion:
Different forms of bullying victimisation were independently associated with psychological distress and reduced emotional wellbeing. In particular, frequent and upsetting social exclusion requires a targeted and measured response by school communities and health practitioners.
Bullying is experienced by 10–25% of adolescents during a school term (Nansel et al., 2001; Olweus, 1993). Girls are more likely to experience bullying victimisation, and rates generally decrease over the course of adolescence (Craig et al., 2009). It negatively affects health and wellbeing (Arseneault et al., 2010), including depression and anxiety symptoms, increased psychosomatic symptoms, suicidal behaviours and poor academic achievement (Cook et al., 2010; Hinduja and Patchin, 2010; Kaltiala-Heino et al., 2000; Nansel et al., 2001). Longitudinal evidence increasingly suggests a causal link between bullying victimisation and the onset of emotional problems (Bond et al., 2001). Bond et al. (2001) found that existing emotional problems were not significantly associated with future experiences of victimisation. Furthermore, studies have also found that bullying victimisation in childhood and adolescence is associated with poor mental health outcomes in adulthood (Copeland et al., 2013; Takizawa et al., 2014).
Bullying is a distinct form of aggression that is intentional, repetitive and occurs in the context of a power imbalance between the perpetrator and victim (Olweus, 1993). It includes direct behaviours such as verbal bullying (teasing and name-calling) and physical bullying (physical threats or harm), as well as indirect behaviours often referred to as relational bullying (spreading rumours and social exclusion) (Smith et al., 2002). Repeated incidents consolidate the power relationship which makes it difficult for a victim to resolve the situation on their own (Pepler and Craig, 2009; Thomas et al., 2015).
The frequency of exposure to bullying victimisation is one factor that influences a young person’s psychological distress and emotional wellbeing. For example, students who were repeatedly victimised reported more severe depressive symptoms, perceived their situation as more threatening and felt less able to control what was happening, compared to those who were victimised once (Hunter et al., 2007). Evidence also suggests that adolescents differ in their emotional reactions to being bullied: some are unaffected and others are upset or angered by the experience (Rigby, 2007). Compared to boys, girls are more likely to report being emotionally hurt by bullying experiences (Rigby and Bagshaw, 2001). The emotional response to bullying victimisation is therefore likely to be related to mental health and wellbeing and is largely unexplored. Combinations of both frequency and emotional response to bullying victimisation are also likely to influence reported psychological distress and wellbeing.
In addition, the form of bullying victimisation is often overlooked and poorly understood. Research examining the prevalence of bullying often assumes all forms of bullying have a similar association with mental ill health (Nansel et al., 2004). However, adolescents may find some forms of bullying more distressing than others. Some authors report physical bullying is the most harmful (Maunder et al., 2010), whereas others suggest relational bullying is the most distressing (Chen et al., 2011; Rigby and Bagshaw, 2001). Therefore, prevalence studies alone may not reflect the magnitude and nature of health and social problems arising from bullying. It is also necessary to examine how different forms of bullying are associated with mental health problems. By investigating both bullying frequency and the emotional response to the experience, we may better understand the relationship between bullying victimisation and adolescent mental ill health.
Researchers argue that mental health encompasses both the frequency and intensity of psychological distress as well as characteristics of psychological wellbeing. This dual continuum model views psychological distress and emotional wellbeing as related but distinct constructs and has been applied to research on adolescents (Tsang et al., 2012). Distress is related to symptoms of anxiety and depression, whereas wellbeing encapsulates interest in and enjoyment of life and is characterised by the presence of positive affect and emotions (Tsang et al., 2012). While the two constructs are considered orthogonal in theory, empirically they are inversely correlated, a disjuncture that is likely due to how the constructs are measured (Green and Salovey, 1999). However, the psychometric argument for measuring both psychological distress and emotional wellbeing is to reduce floor and ceiling effects, where a high proportion of respondents score at the extreme ends of the scale (Bech et al., 2003). A strength of this approach is that it recognises that an individual can report little psychological distress, but may be experiencing low levels of emotional wellbeing. A number of studies have examined the relationship between bullying and psychological distress and emotional wellbeing (Kaltiala-Heino et al., 2000; Nansel et al., 2001). However, few studies have examined these outcomes simultaneously. In order to more holistically understand the relationship between bullying victimisation and mental health, it may be valuable to examine associations with both psychological distress and emotional wellbeing.
The primary aim of this study was to examine the associations between different forms of bullying victimisation (teasing and name-calling, threats of harm or actual harm, rumour spreading, social exclusion) with psychological distress and emotional wellbeing. We expected that all forms of bullying victimisation would be associated with mental ill health. We also hypothesised that bullying victimisation that (1) was higher in frequency and (2) elicited a negative emotional response would be associated with higher levels of psychological distress and reduced levels of emotional wellbeing. A second aim of this study was to explore whether these relationships were different for males and females, and across ages.
Method
Participants and procedure
Data were collected from Victoria, Australia, in the inaugural Victorian Adolescent Health and Wellbeing Survey, known as ‘HowRU?’. The survey was conducted in 2009 as part of a suite of data for the Victorian Child and Adolescent Monitoring System. Data collection involved a two-stage sampling strategy. In the first stage, all schools in Victoria, Australia, were stratified into local government areas or school regions; and schools were randomly selected from each strata based on a probability proportional to each community’s grade-level size. Overall, 220 schools from Government, Independent and Catholic education sectors took part. In the second stage, one class from Grades 7, 9 and 11 at each school was randomly selected. Passive informed consent from parents was conducted for the majority of schools; however, active parent consent was required by some Catholic schools. Informed assent was sought from students on the day of the survey. The students took 60 minutes to complete the survey, and it was conducted online. Trained research staff supervised students while they completed the survey. Victorian health and education authorities granted ethical approval of the study.
Initially, 13,501 students were approached, of which 37 students declined to participate and 739 parents declined to provide consent. Of the remaining participants, 2047 were absent on the day of survey. A total of 10,678 students participated in the study, and 405 provided invalid data and were subsequently excluded. The final sample consisted of 10,273 students (76% of students approached). Approximately half (49.34%) were male. The mean ages were 12.51 (standard deviation [SD] = 0.64), 14.46 (SD = 0.59) and 16.42 (SD = 0.60) years for Grades 7, 9 and 11, respectively. Detailed sample characteristics are shown in Table 1, and the distribution of each bullying victimisation variables is shown in Table 2.
Sample characteristics.
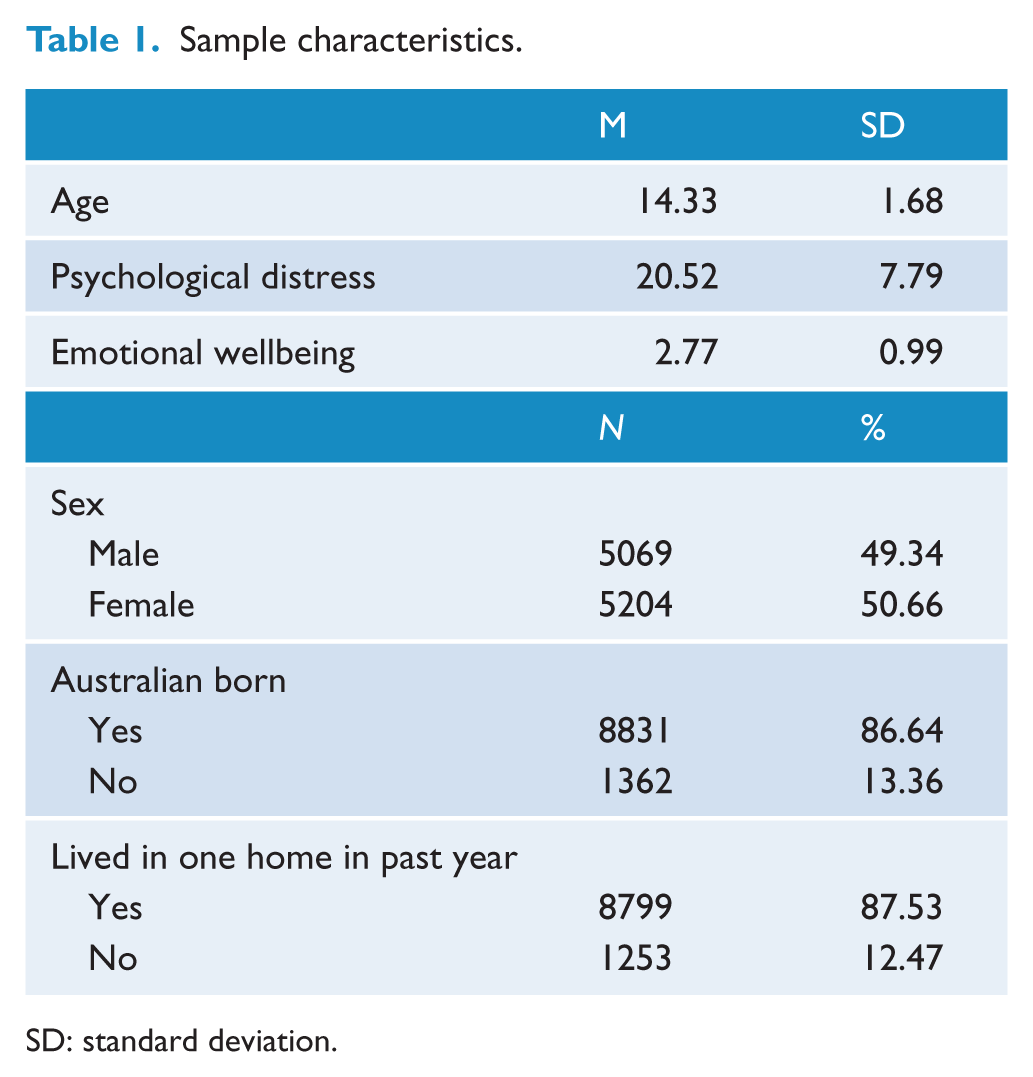
SD: standard deviation.
Prevalence of bullying victimisation.
Measures
We examined demographic questions including age, sex, country of birth and whether students currently lived in two or more homes. Bullying victimisation, psychological distress and emotional wellbeing were also examined.
Bullying victimisation
The Gatehouse Bullying Questionnaire (GBQ) is a 12-item scale used to assess students’ experiences of bullying victimisation and is a reliable tool for measuring bullying in schools (Bond et al., 2007). Participants are asked about four forms of bullying victimisation: being teased or called names (verbal bullying), had rumours spread about them (rumour spreading), been deliberately left out (social exclusion) and been threatened physically or actually hurt (physical bullying). The students responded to each item (‘yes’ or ‘no’) to establish whether the action had occurred ‘recently’. Those who responded ‘yes’ answered two follow-up questions: (1) how often the action had happened (‘less than once a week’, ‘about once a week’ or ‘most days’) and (2) whether they were upset or angry when it happened (‘not at all’, ‘a bit’, ‘or a lot’).
Students were grouped as not having experienced victimisation if they responded ‘no’ to the first item for each form of bullying. These students formed the reference group in the following analyses (responses coded ‘0’). Those who responded ‘yes’ to the first item for each form of bullying victimisation were scored to assess the frequency and emotional response to the experience. The first follow-up question was used as a measure of bullying frequency. Students were classified as having experienced bullying that was frequent if they indicated that it happened ‘most days’, whereas those reporting bullying victimisation ‘about once a week’ or ‘less than once a week’ were grouped as infrequent. The second follow-up question was used to measure adolescents’ emotional response to the bullying experience. Responses of ‘a bit’ and ‘a lot’ were labelled as upset, and the response ‘not at all’ was classified as not upset. Students were then categorised into four groups according to whether they experienced frequent or infrequent bullying victimisation and whether it was upsetting or not upsetting. Students responses were coded ‘1’ if the victimisation was infrequent and not upset, coded ‘2’ if the victimisation was frequent but not upset, ‘3’ if it was infrequent but upset and ‘4’ if it was frequent and upset.
Psychological distress
Student’s psychological distress was measured using the Kessler-10 (K10), an instrument suitable for screening adolescent populations (Andrews and Slade, 2001). The K10 consists of 10 items measuring the level of anxiety and depression symptoms experienced over the previous four weeks. Each item is answered on a 5-point scale (1 = ‘none of the time’; 2 = ‘a little of the time’; 3 = ‘some of the time’; 4 = ‘most of the time’; 5 = ‘all of the time’). Scores can range from 10 to 50, where higher scores indicate increased levels of psychological distress. The scale has shown good reliability in other studies of Australian adolescents (Furkukawa et al., 2003). In the current study, internal consistency of this scale was excellent, α = 0.90.
Emotional wellbeing
A 14-item subscale from the Mental Health Inventory was used to assess emotional wellbeing and is acceptable to use with adolescents (Heubeck and Neill, 2000). This subscale comprises items about general positive affect (e.g. ‘how much of the time have you felt the future looks hopeful and promising?’) and emotional ties (e.g. ‘how much of the time have you felt loved and wanted?’). Items use the past month as the reference period and are rated on a 6-point scale (from ‘all of the time’ to ‘none of the time’). Responses are averaged across all 14 items, where higher scores indicate greater emotional wellbeing. The internal consistency of this scale was excellent, α = 0.94, which is also consistent with other studies of Australian adolescents (Bond et al., 2014).
Data analysis
Two sets of multiple linear regression models were used to examine the association of bullying victimisation with psychological distress and emotional wellbeing. In the first model, psychological distress and emotional wellbeing were regressed on demographic variables and the four bullying victimisation items – verbal bullying, rumour spreading, social exclusion and physical bullying. Each bullying variable was dichotomised into ‘yes’ and ‘no’ responses. This allowed for the direct comparison of the effect of each form of victimisation.
In the second model, psychological distress and emotional wellbeing were regressed on the demographic variables and the four bullying victimisation variables. Each variable was entered into the model as categorical variables, with five different response levels – ‘not bullied’, ‘bullied, infrequently and not upset’, ‘bullied, frequently but not upset’, ‘bullied, infrequently but upset’ and ‘bullied, frequently and upset’. This allows detailed comparisons of the effect of each form of victimisation behaviour as well as the effect of frequency and subjective feeling about the incident. The interaction terms of bullying victimisation and sex, and of bullying victimisation and age, were entered into the model and were tested using Wald’s test (Casella and Berger, 2002). This was conducted to explore if the relationship between each form of bullying victimisation and the two dependent variables, psychological distress and emotional welling, was different between sexes and across ages. Given there were four interaction terms for each interaction, Wald’s tests were used to simultaneously test whether the four regression coefficients were zero. Since these analyses were exploratory in nature and there were eight interactions for each dependent variable, the significance level for the Wald’s test was set to 0.00625 (1/8 of 0.05). Only significant interactions were included in the final model. Of the initial sample, 15.04% of cases had missing data for the variables of interest. Missing values were imputed based on 20 datasets (Rubin, 2008). Two sets of supplementary analyses were conducted to evaluate the robustness of our results. First, the analyses were repeated with complete cases only and results were compared to the results from the imputed dataset to evaluate the appropriateness of the imputation. Second, the analyses were repeated with a different coding scheme for the bullying victimisation variables. Under this coding scheme, with regard to frequency of bullying victimisation, responses of ‘most days’ were coded as frequent; with regard to emotional response, responses of ‘a lot’ were coded as upset. A similar result under different coding schemes will indicate our results were robust and not sensitive to changes of cut-off point.
Results
Sample characteristics and prevalence of bullying victimisation are shown in Tables 1 and 2. Verbal bullying was the most common form of bullying victimisation (30.61%), physical bullying the least common (10.72%). Results from the first set of regression analyses showed that after controlling for demographic variables, each form of bullying victimisation was significantly associated with psychological distress (R2 = 0.12). Comparison of the regression coefficients and the corresponding 95% confidence intervals (CIs) indicated that students who reported social exclusion, b = 3.26, p < .001, 95% CI [2.80, 3.72], had significantly higher levels of psychological distress compared to those who reported being verbally bullied, b = 2.23, p < .001, 95% CI [1.83, 2.67], had rumours spread, b = 2.13, p < .001, 95% CI [1.69, 2.57], or physically bullied, b = 1.96, p < .001, 95% CI [1.44, 2.49]. Each form of bullying victimisation was also significantly associated with reduced emotional wellbeing (R2 = 0.09). Those who reported social exclusion, b = −0.36, p < .001, 95% CI [−0.42, −0.30], had significantly reduced levels of emotional wellbeing compared to those who were verbally bullied, b = −0.24, p < .001, 95% CI [−0.29, −0.19], experienced rumour spreading, b = −0.12, p < .001, 95% CI [−0.18, −0.07], or physical bullying, b = −0.17, p < .001, 95% CI [−0.24, −0.10].
Table 3 shows the results of the second set of regression analyses, where the four forms of bullying victimisation were entered into the regression models with five levels of responses for each. The full regression models accounted for 14.18% of variance in psychological distress and 9.53% of variance in emotional wellbeing. After controlling for demographic variables (age, sex, being born overseas and living in two or more homes), the four forms of bullying victimisation and their interactions with sex and age accounted for 11.98% of the variance in psychological distress and 6.64% of the variance in emotional wellbeing. Similar to the results of the first set of regression analyses, all four forms of bullying victimisation in general were significantly associated with psychological distress and emotional wellbeing (p < .05). In the model examining psychological distress, the interaction between age and social exclusion was significant (Wald’s test p < .001). Regression coefficients from the model indicated that social exclusion had a stronger association with psychological distress in older adolescents. In the model examining emotional wellbeing, the interaction between age and social exclusion was significant (Wald’s test p < .001). Regression coefficients from the model indicated that social exclusion was more strongly associated with reduced emotional wellbeing in older adolescents. The interaction between sex and having rumours spread was significant (Wald’s test p < .001). Regression coefficients from the model indicated that rumour spreading was more strongly associated with psychological distress in adolescent females, compared to males.
Regression coefficients from the second set of models.
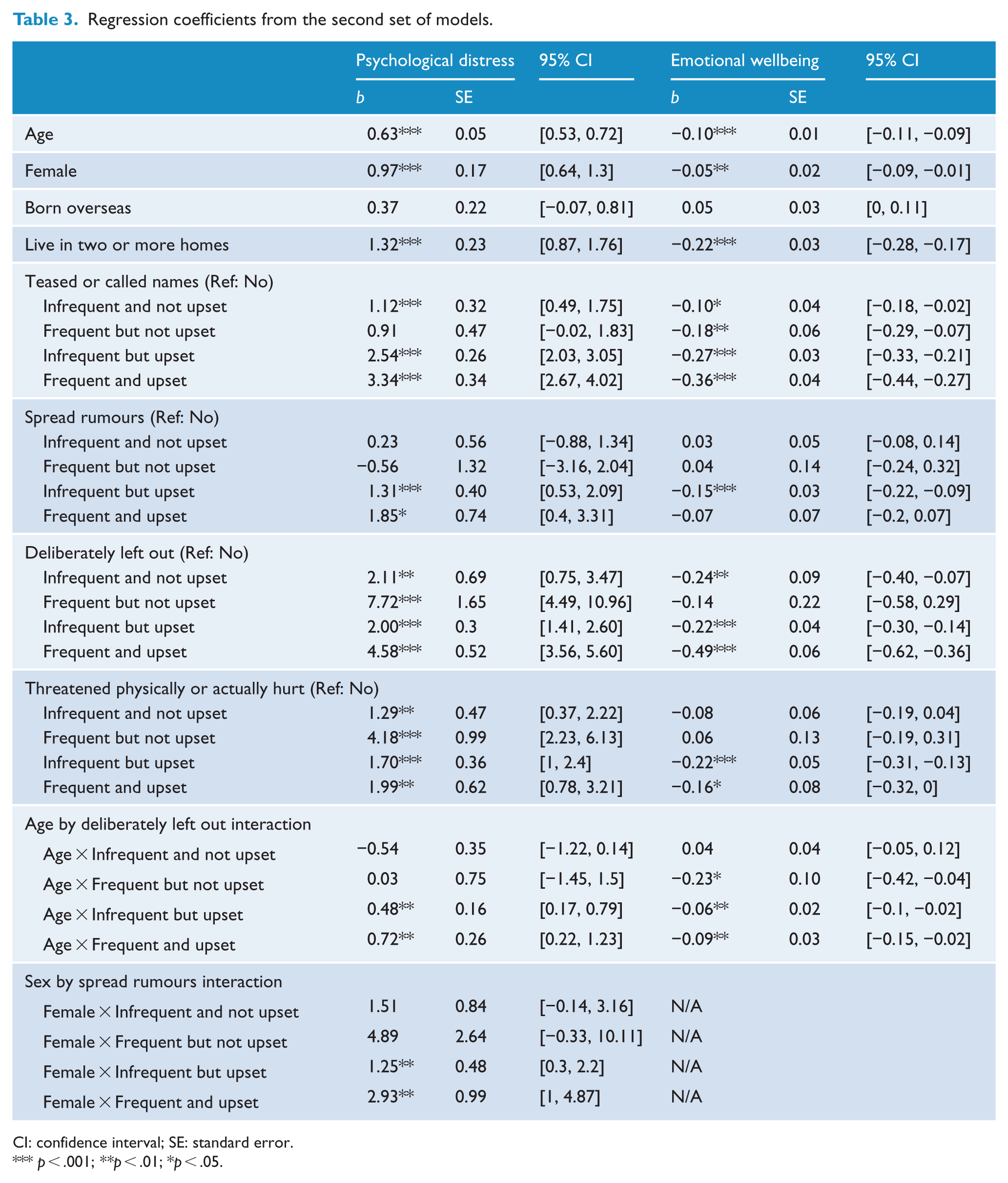
CI: confidence interval; SE: standard error.
p < .001; **p < .01; *p < .05.
All analyses were rerun using complete cases. The results were similar to the results from the imputed dataset and the same conclusions were drawn. Given that analyses using the imputed dataset can produce smaller standard error and adjust for the observed missing data mechanism, results from the imputed dataset are reported. The analyses were also rerun using a different coding scheme for the bullying victimisation variables. The results from the analyses were similar to those from the original analyses. Since the coding scheme used in the original analyses was consistent with the coding documented by the scale developer (Bond et al., 2007), results from the original analyses were reported.
Discussion
This study examined how the frequency, emotional response and form of bullying victimisation were associated with the mental health of school students. While there are now many studies that have reported on the relationship between bullying and mental ill health in adolescents (Cook et al., 2010; Kaltiala-Heino et al., 2000; Nansel et al., 2001), this study extends the existing literature in three ways. The first model showed that each form of bullying victimisation was associated with poor mental health. Of particular note, social exclusion had a strong association with adolescents’ psychological distress and low emotional wellbeing. The second model showed that physical bullying that was upsetting was associated with high levels of psychological distress and reduced emotional wellbeing, regardless of frequency. In addition, frequent or infrequent rumour spreading was most strongly associated with psychological distress in females. This result supports a previous study that found females are more likely to be involved in relational forms of bullying compared to males (Wang et al., 2009). Being deliberately left out frequently even if it was not upsetting was significantly associated with psychological distress. These results suggest that recurrent social exclusion, even if it does not elicit a negative emotional response, is still associated with mental ill health. Furthermore, social exclusion that was upsetting irrespective of frequency was associated with psychological distress in older adolescents.
A previous study also found that relational bullying (exclusion and rumour spreading) was most strongly associated with mental health problems, independent of direct forms of bullying victimisation (Baldry, 2004). Another study reported physical bullying is perceived as more harmful (Maunder et al., 2010). However, the latter study used student ratings of the severity of different bullying behaviours, which carries the disadvantage of forcing respondents to differentiate between items that they may consider equivalent, and it is likely that not all responses were indicative of real experiences. A recent study of Taiwanese adolescents found that both ‘passive’ forms (which included name-calling and relational bullying) and ‘active’ forms (physical threats and harm) of bullying victimisation were associated with mental ill health (Yen et al., 2014). Our findings further support previous research that also found social exclusion has a strong association with mental health problems, but they also show that all forms of bullying victimisation are independently associated with poor mental health.
Social exclusion has received less attention in bullying research. It is important to highlight because indirect forms of aggression such as social exclusion may be an alternative strategy to direct aggression because it may be less likely to invoke negative consequences for the perpetrator (Archer and Coyne, 2005). Social exclusion is a behaviour that is subtle and difficult to detect, and therefore less likely to prompt a response from an adult. This may result in the behaviour persisting for longer than other forms of bullying and makes self-defence more difficult, increasing the consequent stress and isolation (Vaillancourt, 2005). Adolescents may be particularly sensitive to social exclusion because it deprives them of participating in their social networks. During adolescence, acceptance and popularity in the peer group are increasingly important as young people individuate from their parents (Marini et al., 2006). Social exclusion also becomes more prevalent and hurtful in adolescence as young peoples’ social-cognitive skills develop. It is possible that social exclusion decreases status in the peer group, which may be affecting mental health. Therefore, social exclusion may have a negative association with adolescents’ mental health because of the increased salience of peer relationships and sensitivity to peer rejection during this developmental period. This study found that social exclusion was strongly associated with mental ill health in older adolescents, which contrasts with a previous study that found ‘passive’ forms (which included verbal and relational behaviours) of victimisation were strongly associated with poor mental health in younger adolescents (Yen et al., 2014). It is plausible that this inconsistency may be due to differences in measurement approaches. The finding needs to be replicated in future studies.
The second important finding was that a student’s negative emotional response to name-calling, rumour spreading and physical threats or harm was associated with mental ill health. Even when the behaviours were infrequent, a negative emotional response was associated with higher levels of psychological distress and reduced levels of emotional wellbeing. An adolescent’s emotional response to bullying victimisation may be influenced by a range of factors: the behaviours themselves, the resilience of the student and the support from other peers all play a role (Cowie and Berdondini, 2002). This finding highlights the importance of assessing students’ emotional response to bullying as a way of determining the extent to which bullying victimisation may influence their mental health. Examining only the presence and frequency of bullying victimisation overlooks important information on adolescents’ initial emotional response to the victimisation they experienced.
The third finding from this study was that adolescent exposure to bullying victimisation was associated with both psychological distress and reduced emotional wellbeing. Researchers have developed opposing arguments as to whether these two constructs are sufficiently distinct (Green and Salovey, 1999; Tsang et al., 2012). However, it is likely they have overlapping features that are largely influenced by how the constructs are measured. This study highlights that social exclusion is a particularly concerning form of bullying that should be targeted in prevention work. Most researchers agree that we need to better understand why adolescents who experience bullying victimisation show early signs of mental health problems. One hypothesis is that individuals vary in their stress reactivity and may be hyper- or hypo-sensitive to stress, which contributes to a decline in mental health (Arseneault et al., 2010). Our results suggest that this association may also be related to a combination of the frequency and the early emotional response associated with the victimisation. Further research is required to identify protective factors that help young people overcome experiences of bullying. This knowledge would help clinicians and educators support the most vulnerable students.
Bullying is identified as a modifiable risk factor for mental illness (Scott et al., 2014), and over the last three decades, prevention programmes have received increasing attention. The focus of intervention is on increasing awareness about bullying and decreasing its prevalence. The emphasis is mostly on classroom-curricular approaches and school-wide strategies that involve students, staff and parents. However, there is large variability in the reported effectiveness of such programmes (Smith et al., 2003; Ttofi and Farrington, 2009; Vreeman and Carroll, 2007). The Olweus Bullying Prevention Program in Norway (Bauer et al., 2007; Olweus, 1993) and the KiVa programme in Finland (Kärnä et al., 2011) are examples of interventions that report reduced rates of bullying. There is a strong emphasis on programmes that pursue school-wide approaches and focus on establishing a positive school culture and climate. This strategy acknowledges the role the school environment plays in exacerbating or protecting against bullying (Olweus, 1993). Bullying is a complex and multi-faceted behaviour that necessitates further evidence-based inquiry regarding the most effective approach to intervention.
There is dispersed discussion on intervention strategies specific to relational bullying (Geiger et al., 2004; Shute et al., 2002). Leff et al. (2010) conducted a review of relational aggression programmes and concluded that more systematic investigations are required. Social exclusion and other forms of relational aggression have been seen as part of the normal pains of peer relationships. However, frequent and on-going social exclusion deserves a targeted and measured response given the associated negative effects. A school environment that values positive peer relationships and promotes inclusion, tolerance and respect may help to address relational forms of bullying. The current trend is to move towards ‘whole-school’ approaches that embed bullying interventions into other school initiatives designed to promote social and emotional learning and engage all members of the school community – students, staff and parents. This approach may be effective in targeting behaviours including social exclusion, but it awaits further evaluation involving randomised longitudinal designs.
Limitations
Like all epidemiological studies, there are missing participants which is a common limitation of school-based surveys (Kristjansson et al., 2013). It is likely this group would be overrepresented by those who may have experienced bullying victimisation, given that bullying adversely affects educational attendance and school engagement (Moore et al., 2015). While the study involved a representative sample of adolescents, there are confines to comparing the prevalence of different forms of bullying behaviours given that there was no precise timeframe referenced. We also acknowledge that cyberbullying is a new dimension that was not explicitly captured by the Gate House Bullying Scale. Future studies should, where possible, include ‘traditional’ and ‘cyber’ bullying elements (Thomas et al., 2015). Our enquiry was also limited to bullying victimisation and did not include any items that measured perpetration. Evidence suggests that students who are both victimised and also perpetrate bullying are at the highest risk of psychosocial problems (Kaltiala-Heino et al., 2000; Marini et al., 2006). In our survey, students were not orientated to a definition of bullying. There is on-going debate as to whether scales should include a definition of bullying prior to the items to reduce measurement error. Finally, these data are cross-sectional, so the direction of the relationship between negative emotional response to bullying victimisation and psychological distress cannot be determined. For example, students who have pre-existing mental health problems may be more likely to have negative emotional responses to bullying (Arseneault et al., 2010). However, there is a growing body of research that shows bullying victimisation uniquely contributes to mental health issues, over and above symptoms prior to the onset of the victimisation (Bond et al., 2001; Moore et al., 2015).
Conclusion
We found that different forms of bullying victimisation were associated with psychological distress and reduced emotional wellbeing. In particular we found bullying victimisation that was both frequent and elicited an emotional response had a significant association with adolescents’ mental health. Overall, social exclusion – being deliberately left out by peers – had the strongest association with psychological distress and reduced emotional wellbeing. We found that both the frequency of bullying and the emotional response to these experiences were factors that influenced the relationship between bullying and mental ill health. These results again highlight the seriousness of bullying and the importance of prevention work. There is a strong need to further develop school-wide programmes to better target relational forms of bullying that especially address social exclusion.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
The Victorian Adolescent Health and Wellbeing Survey was funded by the Department of Education and Early Childhood Development, Victoria, Australia. Hannah Thomas is supported by scholarship from the Bryan Foundation and Clear Thinking, Australia. Data analysis was supported by Australian Research Council Discovery Project DP130102015. Jason Connor is supported by a National Health and Medical Research Council of Australia Career Development Fellowship (1031909).