
Abstract
Background
The relationship between cardiovascular risk factors (CVRF) and migraine is controversial and might be different in both genders. These associations were evaluated in Brazilian middle-aged men and women from the Longitudinal Study of Adult Health (ELSA-Brasil).
Methods
The cross-sectional relationship between our main outcome, which was migraine headache (definite, probable and overall), and CVRF was evaluated in the total sample and according to gender. We calculated frequencies and odds ratios (95% CI) for this relationship using binary and multinomial logistic regression analyses in crude, age-adjusted and multivariable models adjusted by potential confounders.
Results
Of 14,953 individuals who completed the data about headache and CVRF, the frequency of one-year migraine was of 29.5% (22.5% in women and 7.0% in men). In the multivariable-adjusted regression analyses, an inverse association between hypertension (OR, 0.53; 95% CI, 0.36–0.79), metabolic syndrome (OR, 0.65; 95% CI, 0.43–0.99) and definite migraine were confirmed for men, but not for women. In the opposite direction, a positive association between migraine headaches (definite, probable and overall) and dyslipidemia (overall migraine OR, 1.25; 95% CI, 1.13–1.38) was observed only for women, but not for men.
Conclusions
A gender influence on the relationship between migraine and CVRF was verified in the ELSA-Brasil.
Introduction
The relationship between migraine headaches and major established cardiovascular risk factors (CVRF) is conflicting (1–26). As a migraine pattern, traditional CVRF are also influenced by gender. Despite this fact, most previous studies have not focused on the influence of gender on the relationship between migraine and CVRF.
Earlier observational studies have reported positive associations between hypertension and migraine in selected samples and mostly in women (1–3). Conversely, several population-based studies have shown inverse or even null cross-sectional associations between hypertension and migraine headaches in middle-aged and elderly populations including both genders (4–9). Besides hypertension, some population-based studies also reported a relationship between high systolic blood pressure (SBP) or diastolic blood pressure (DBP) and migraine with diversified findings as well (4,5,7,10).
Regarding lipids, most cross-sectional observational studies, including population-based studies, have reported positive associations between hypercholesterolemia and migraine headaches in different age strata for both genders (7,11–13). Controversial findings about the relationship between obesity and migraine headaches were reported by several studies with conflicting results (14–20). Previous cross-sectional analysis in the ELSA-Brasil, in which body mass index (BMI) and abdominal obesity were evaluated, daily migraine was associated with higher BMI levels in individuals without abdominal obesity measured by waist circumference (20). The relationship between migraine status and diabetes has been evaluated by some population-based studies with divergent findings, as well (3,8,21–23). Two prevalence studies performed in middle-aged and elderly populations, which included both genders, found no significant associations between migraine and diabetes (3,8). Conversely, two other large studies based on representative samples of the United States (US) population evidenced a positive cross-sectional relationship between migraine and type 2 diabetes (21,22). Recently, a prospective evaluation conducted among middle-aged women, who provided information on migraine and were free from diabetes at baseline, did not confirm an association between migraine and incident type 2 diabetes (23).
Few cross-sectional and no representative studies have associated migraine headache with metabolic syndrome (MS) (24,25). More consistent findings that reported a positive association between migraine and the incidence of MS did not mention the influence of gender in their findings (26).
The relationship between CVRF and migraine headaches may be influenced by several methodological issues, in particular the characteristics of the population under study may explain divergent results reported by previous studies. Thus, we aimed to evaluate the cross-sectional relationship between migraine and most classic CVRF such as hypertension, dyslipidemia, diabetes, MS, insulin resistance and smoking among middle-aged women and men participants from the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) baseline assessment. The ELSA-Brasil is a cohort of 15,105 civil servants aged 35 to 74 years that was designed to investigate factors associated with the development and progression of cardiovascular diseases (CVD) and diabetes (27).
Methods
Design and population study
This is a cross-sectional analysis using data from the baseline assessment of ELSA-Brasil. It is an ongoing prospective multicenter cohort study involving civil servants living in six cities (Belo Horizonte, Porto Alegre, Rio de Janeiro, Salvador, Sao Paulo and Vitoria) whose baseline assessment occurred between 2008 and 2010; the first follow-up period (four years after baseline) is finishing. Further details about the cohort are described elsewhere (28).
In brief, all active or retired employees of six institutions aged 35–74 years were eligible for the study. Exclusion criteria were current or recent (<4 months prior to the first interview) pregnancy, intention to quit working at the institution in the near future, severe cognitive or communication impairment, and, if retired, residence outside of a study center’s corresponding metropolitan area. Compared to the Brazilian general population, ELSA-Brasil participants present with higher monthly income, high levels of educational attainment and more access to health care. However, they were selected according to study goals including a similar number of participants with occupation classified as unskilled, technical/clerical and faculty and professional staff permitting a gradient of socioeconomic position across the sample (28).
Approvals from all institutional review boards were guaranteed.
Migraine definition
All participants who answered “yes” to the question “In the last 12 months, did you have a headache?” at the ELSA-Brasil baseline evaluation were invited to answer a detailed headache questionnaire based on the International Headache Society criteria (IHS-2004) that was adapted, validated and previously used in Brazil (8,29).
Briefly, it investigates pain frequency, duration, quality, location, intensity, triggering and accompanying symptoms, such as nausea or vomiting and the presence of aura. Based on this questionnaire, we classified participants as having definite migraine if they fulfilled criteria for IHS codes 1.1 (migraine without aura) or 1.2 (migraine with aura). We classified individuals who answered “yes” to the question about headache and fulfilled all criteria for migraine but one as probable migraine. Participants with other headaches or without headache were considered as having no migraine.
Further, we collected information about prophylactic medications for migraine based on evidence level A (established as effective for migraine prevention and should be offered to patients with migraine to reduce migraine attack frequency and severity) or level B (possibly effective for migraine prevention and should be considered for migraine prevention), according to the 2012 guidelines of the American Academy of Neurology (30). Thus, for the present analysis we considered the following medications: level A: antiepileptic drugs (divalproex sodium, sodium valproate, topiramate), beta-blockers (propranolol, metoprolol, timolol) and level B: antidepressants (amitriptyline, venlafaxine) and beta-blockers (atenolol, nadolol).
Socioeconomic status (SES)
Age was reported as mean ± SD and categorized into four strata (35–44; 45–54; 55–64 and 65–74 years old). Race was classified by the interviewer in four categories: white, brown, black and others (Asian or indigenous). Education was classified in three categories: up to incomplete high school, high school to incomplete graduation and complete graduation. Monthly family income (transformed from Brazilian currency to US$) was classified into three categories: < US$1245; US$1245 to US$3319 and ≥ and US$3320.
Measures of cardiovascular risk
We evaluated main traditional CVRF based on the personal interview guided by the standardized questionnaire for the ELSA-Brasil (27,28). Resting BP was measured three times in the seated position after five minutes’ rest with an OMROM digital sphygmanometer (model HEM-712-C). Measurements were taken after at least 12 hours without ingestion of caffeine and one hour without smoking, with participants seated and their arm level with the heart. The mean of the two latest BP measurements was considered as the value for hypertension definition. Participants with SBP ≥140 mmHg and/or DBP ≥90 mmHg and/or under medication to treat hypertension were classified as having hypertension. The anthropometric parameters are measured using standard equipment and techniques.
Venous blood samples were obtained after a 12-hour overnight fast. The serum obtained after centrifugation was used for hormone and biochemical measurements. Analyses were carried out using an automated analyzer. For measurement of fasting and post-load glucose, we used the hexokinase method (ADVIA 1200, Siemens); for fasting and post-load insulin, immunoenzymatic assay; for glycate hemoglobin, high-pressure liquid chromatography; for total and high-density lipoprotein (HDL) cholesterol, and triglycerides, enzymatic colorimetric assay (ADVIA 1200, Siemens); low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald equation except for cases with elevated triglyceride levels, for which a enzymatic colorimetric assay was used (ADVIA 1200, Siemens); high-sensitive C-reactive protein (hsCRP), immunochemistry (nephelometry, Siemens).
Diabetes was defined as previous medical history of diabetes and/or use of medication to treat diabetes, and/or a fasting plasma glucose ≥126 mg/dl, and/or a two-hour plasma glucose ≥200 mg/dl), and/or a hemoglobin A1C (HbA1C) ≥ 6.5%. Insulin resistance was estimated using the homeostasis model assessment for insulin resistance (HOMA-IR) based on the formula: fasting glucose (mg/dl) × insulin (µIU/ml)/405 HOMA-IR values.
In addition, dyslipidemia (LDL cholesterol ≥130 mg/dl and/or lipid-lowering drugs) and MS (≥three criteria: waist measurement >88 cm for women or >102 cm for men, HDL cholesterol <50 mg/dl for women or <40 mg/dl for men, a SBP ≥130 mmHg or ≥85 mmHg, serum triglyceride levels ≥150 mg/dl, and fasting plasma glucose ≥110 mg/dl) diagnoses were defined according to National Cholesterol Program-Adult Treatment Panel III (NCEP ATP III) criteria (31).
Statistics
Baseline characteristics focusing on previous history of traditional CVRF and biomarkers were compared according to migraine headache status (no headache, definite migraine, probable migraine and overall migraine). Categorical variables were presented in proportions using the Chi-square test and continuous variables were presented in means (standard deviation) or median (interquartile range) using analysis of variance (ANOVA) or Kruskal-Wallis test whenever applicable.
We also calculated odds ratios (OR) for the association between each CVRF (hypertension, diabetes, dyslipidemia, MS, insulin resistance (HOMA above 75th percentile) and smoking status) with each migraine subgroup using a “no migraine headache” subgroup as reference. We performed binary and multinomial logistic regression analyses in crude, age-adjusted and multivariable models adjusted by potential confounders such as age, gender, race, educational level, marital status, family income, use of migraine prophylaxis and antihypertensive medication. We performed stratified analyses to explore different patterns according to gender. For all analyses, p values less than 0.05 were also considered as significant. All cases with missing information about headache that corresponded to 1.0% (152 from 15,105 cases) were excluded from our main analyses.
The statistical analyses were performed with the statistical software SPSS version 22.0.
Results
Baseline characteristics of 14,953 participants from the ELSA-Brasil, according to migraine status.

Some proportions might not add up to 100% due rounding or missing values (at most 0.3%). Overall migraine includes probable and definite migraine subgroups. All biomarkers are expressed in median and interquartile (IQ) range. aP value < 0.001 compared to the non-migraine subgroup. bP value <0.05 compared to the non-migraine subgroup. cDefined as presence of hypertension if systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, history of hypertension diagnosed by physician, or current treatment. dDyslipidemia was assessed according to the National Cholesterol Program-Adult Treatment Panel III (NCP-ATPIII) guidelines as follow: LDL cholesterol ≥130 mg/dl or use of lipid-lowering drug. eDiabetes was defined as previous medical history of diabetes, use of medication to treat diabetes, a fasting plasma glucose ≥126 mg/dl), a two-hour plasma glucose ≥200 mg/dl), or an HbA1C ≥ 6.5%. fMetabolic syndrome was assessed according to the National Cholesterol Program-Adult Treatment Panel III (NCP-ATPIII) guidelines as follow: ≥ three criteria: waist measurement > 88 cm for women or 102 cm for men, HDL-cholesterol < 50 mg/dl for women or < 40 mg/dl for men, a systolic blood pressure ≥ 130 m Hg or ≥ 85 mm Hg, serum triglyceride levels ≥ 150 mg/dl, and fasting plasma glucose ≥ 110 mg/dl. ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; LDL: low-density lipoprotein; HDL: high-density lipoprotein; HOMA-IR: homeostatic model assessment-insulin resistance; USD: United States dollars.
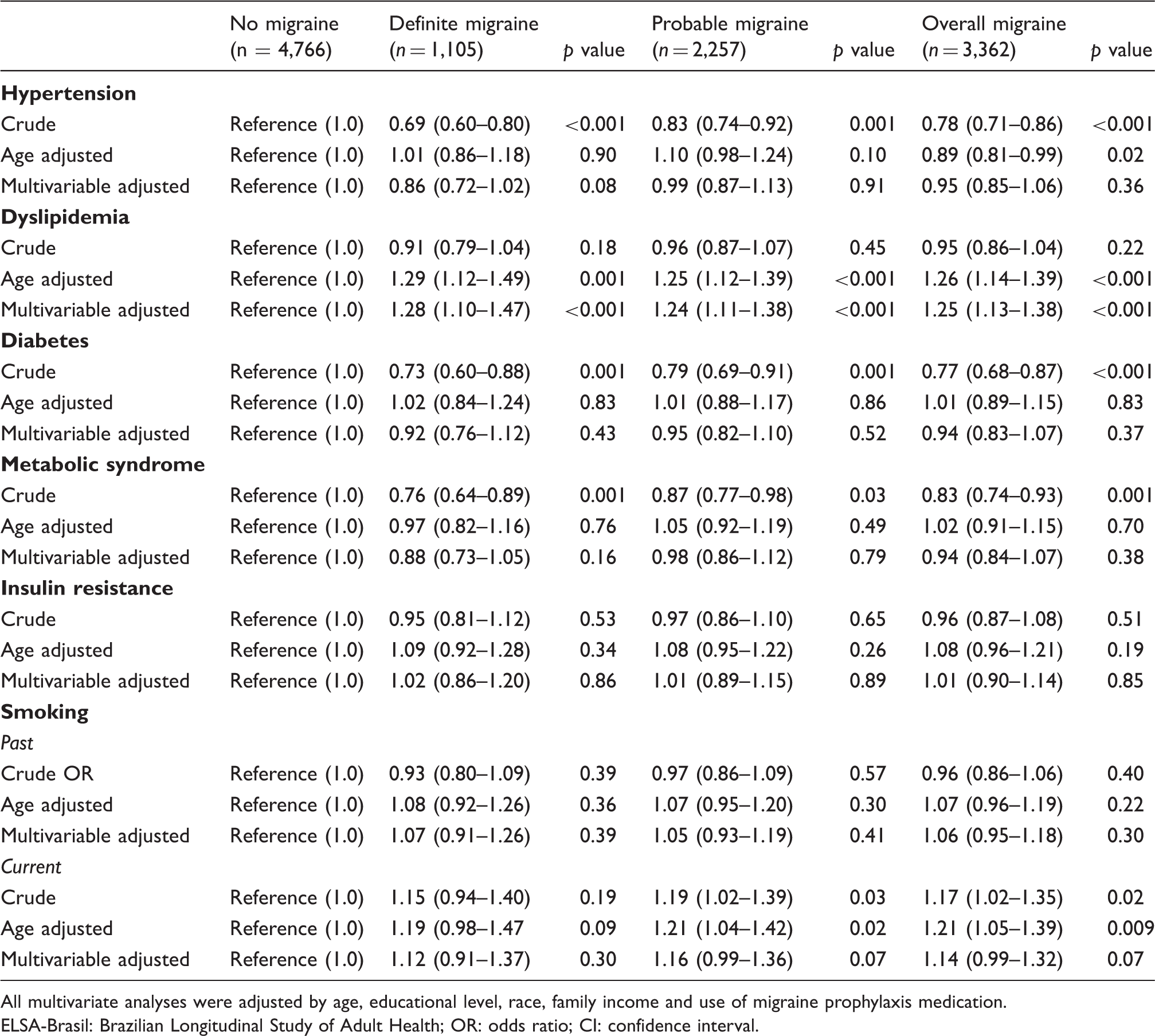
After adjusting by age, sex, educational level, race, family income, and use of migraine prophylaxis medication, we observed significant negative associations between definite migraine and hypertension (multivariable OR, 0.80; 95% confidence interval (CI), 0.68–0.93), as well as, MS (multivariable OR, 0.84; 95% CI, 0.72–0.98). In the opposite direction, significant positive associations between dyslipidemia and all migraine categories (definite, probable overall) were found for the total sample, and the OR for the association between overall migraine and dyslipidemia was 1.17; (95% CI, 1.08–1.27). In a stratified analysis by gender, similar results were replicated for the inverse association between hypertension (OR, 0.53; 95% CI, 0.36–0.79), MS (OR, 0.65; 95% CI, 0.43–0.99) and definite migraine (but not probable and overall) among men, but not for women. The positive associations between migraine headaches (definite, probable and overall) and dyslipidemia were confirmed only for women, but not for men. The OR for the relationship between overall migraine and dyslipidemia was 1.25; (95% CI, 1.13–1.38). Diabetes, insulin resistance and smoking did not present significant associations with migraine headaches in multivariable models. Additional adjustment for antihypertensive medication use did not significantly alter our findings. Finally, excluding all individuals who had other headaches from the control group (non-migraine headache) did not materially change our findings either.
Discussion
In this cross-sectional analysis of the ELSA-Brasil performed among 6825 men and 8128 women, a high frequency of migraine was found in about 29% of participants, predominantly in women (22.5%). Similarly, other previous Brazilian studies performed in population-based studies (32–35) or clinical settings (36) reported one-year migraine prevalence ranging from 20.4% to 36.8%. Additionally, the relationship between CVRF and the presence of migraine in the last 12 months was partially influenced by gender in the ELSA. After multivariable adjustment for multiple confounders, hypertension and MS were both negatively associated with definite migraine (but not with probable and overall migraine) only in men. Likewise, we encountered a positive association between dyslipidemia and all migraine categories (probable, definite and overall) in women, but not for men.
Previous studies have described conflicting results regarding hypertension and migraine (1–9). Some previous observational studies that reported a positive relationship between hypertension and migraine headaches were performed in smaller, circumscribed samples or in populations with higher proportions of women compared to the ELSA-Brasil population (1–3). In the Italian Longitudinal Study of Aging (ILSA), which was restricted to a total of 312 elderly males and females, migraine associated with hypertension was observed (1). The Danish Twin Registry (DRT), which aimed to evaluate sex-specific conditions associated with migraine, evaluated a random sample of 31,865 middle-aged individuals, almost 70% of them women. In this study, an OR of approximately 1.50 for the relationship between hypertension and migraine was reported, regardless of gender (2). In the cross-sectional analysis of the Genetic Epidemiology of Migraine (GEM) study, performed in 5755 middle-aged women and men, a positive association between overall migraine and hypertension was observed in a subgroup of smoking women (OR, 1.38; 95% CI, 1.0–2.0) (3).
On the other hand, the most recent population-based studies have described negative or no significant associations between migraine and hypertension in middle-aged individuals and the elderly (4–9). In the Reykajavik Study, a population-based cohort that included 10,366 men and 11,171 women during 1967–1996, no significant associations with hypertension and migraine were found. However, migraine was associated with lower SBP and higher DBP than controls during periodic evaluations. The Epidemiology Vascular Ageing (EVA), a prospective cohort of 1373 elderly individuals after four years of follow-up, demonstrated that SBP higher than 140 mmHg was associated with decreased risk of having lifetime migraine. Similar to our findings, this decreased risk was more pronounced among males (OR, 0.30 95% CI, 0.11–0.83) compared to females (OR, 0.62 95% CI, 0.39–0.99). Hypertension frequency tended to be lower among migraineurs, as well (5).
Previous Brazilian cross-sectional studies have also reported inverse associations between hypertension and migraine in clinical and non-clinical settings, reinforcing the results described here (6–8). In the study by Wiehe et al., which was performed in 659 women and 515 men randomly selected from an urban city in the south of Brazil, high-normal to severe hypertension was negatively associated with migraine. After multivariable adjustment, they found a risk of having migraine decreased by approximately 50% among hypertensive individuals. These results were not presented by gender (6). In the Sao Paulo Ageing & Health Study (SPAH) performed among a population of 1450 low-income elderly, an inverse relationship between hypertension and migraine was also reported; however, it was restricted to elderly women (OR, 0.58 95% CI, 0.38–0.90) (7). Conversely, we found similar OR, but restricted to men who had definite migraine.
A cross-sectional evaluation performed in Brazilian outpatients using 24-hour ambulatory BP monitoring, did not show higher BP levels in women with chronic migraine compared with women without migraine headaches (8).
A putative association between hypertension and hypoalgesia could partly explain the negative association between migraine and hypertension or BP (37). However, we cannot speculate about this effect of causality because our findings were cross-sectionally evaluated.
We also observed a marginally negative association (OR 0.65; 95% CI, 0.43–0.99) between definite migraine and MS in men. In the opposite direction, previous studies reported a positive association between migraine and MS or its components. However, most of them were cross-sectionally conducted in small samples and mostly comprised women (24–26). Most reliable findings come from the Nord-Trøndelag Health Study (HUNT 2) study, in which the relationship between migraine (including with aura) and no migraine headache diagnosed at baseline and the incidence of MS was evaluated among 7020 males and 6760 females after 11 years of follow-up. They found a relative risk (RR) of developing MS to be about 1.50 among migraineurs compared to those individuals with no headache, regardless of gender. The highest RR was reported among those migraineurs with aura who were current smokers (RR, 2.10; 95% CI, 1.53–2.89) (26). Divergences between our findings and those from the HUNT 2 study could be attributed mainly to study design and the presence of aura. These findings suggest a link between migraine with aura and an increased risk of emerging CVRF (and consequently CVD) as reported by some previous cross-sectional and prospective analyses performed on population-based studies (38–40).
Contrasting with the cardiovascular profile found in male migraineurs, our findings support a consistent positive relationship between all migraine categories and dyslipidemia only in women, based on a dyslipidemia definition that included LDL cholesterol ≥130 mg/dl and lipid-lowering medication use. When we evaluated the lipid profile analyzing total cholesterol and LDL cholesterol separately and without any information about use of medication to treat dyslipidemia, we found no differences according to migraine status, regardless of gender. Most observational studies, including population-based studies, have reported positive cross-sectional associations between hypercholesterolemia, particularly increased total cholesterol or LDL cholesterol levels and migraine headaches in different age strata, irrespective of gender (7,11–13).
Regarding glucose metabolism, we did not find any statistical association between diabetes or insulin resistance and migraine in multivariable-regression models. Similarly, other cross-sectional and prospective studies did not confirm some association between diabetes and migraine (2,7,23). Only a few population-based studies evidenced cross-sectional positive associations between migraine and diabetes (21,22).
Odds ratios (95% CI) for cardiovascular risk factors according migraine status in 14,953 participants from the ELSA-Brasil.

All multivariate analyses were adjusted by age, sex, educational level, race, family income and use of migraine prophylaxis medication. Insulin resistance was defined as HOMA-IR above 75th percentile (3.00). ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; OR: odds ratio; CI: confidence interval; HOMA-IR: homeostatic model assessment-insulin resistance.
Odds ratios (95% CI) for cardiovascular risk factors according migraine status in 8,128 women participants from the ELSA-Brasil.
All multivariate analyses were adjusted by age, educational level, race, family income and use of migraine prophylaxis medication. ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; OR: odds ratio; CI: confidence interval.
Odds ratios (95% CI) for cardiovascular risk factors according migraine status in 6,825 men participants from the ELSA-Brasil.

Insulin resistance was defined as HOMA-IR above 75th percentile (3.00). All multivariate analyses were adjusted by age, educational level, race, family income and use of migraine prophylaxis medication. ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; OR: odds ratio; CI: confidence interval; HOMA-IR: homeostatic model assessment-insulin resistance.
STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies.

Information given separately for exposed and unexposed groups. An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Despite variances due to definitions of migraine and CVRF, population and environmental factors, several studies have also reported different patterns for the relationship between CVRF and migraine according to gender (2–5,7–9). Except for lipid profile and obesity, men presented with worse CVRF profiles than women. Differences between our findings and those reported by previous studies, which evidenced a positive association between some CVRF (1–3) and migraine, could be explained by the healthier status of the ELSA-Brasil sample that includes only civil servants with better access to health care compared to the general population. Also, our participants have lower frequency of CVRF at baseline compared to other studies (1–3). Another aspect that we have to consider is the lower frequency of CVRF in young and middle-aged women compared to men of similar age. Finally, migraineurs were younger and had a lower burden of CVRF than non-migraineurs in our sample (see Table 1). Longitudinal information about the ELSA-Brasil follow-up will be very useful to elucidate gender differences on the relationship between migraine and CVRF that will be established over the years.
Our study has some limitations. Although ELSA-Brasil is an ongoing prospective cohort, here we present data from cross-sectional baseline data that did not allow us to make causal inferences about the relationship between migraine and CVRF such as hypertension, dyslipidemia, glucose metabolism, MS and smoking. Further, the ELSA headache questionnaire collected all potential migraine cases in the last 12 months, thus we cannot rule out the possibility of including participants with a previous past history of migraine among controls. Further, we found significant associations only with definite migraine and some CVRF as hypertension and MS in a sub-sample of men. Despite the lack of significance, the relationship between overall and probable migraine with CVRF was in the same direction in males. We could speculate that definite migraine cases that fulfilled all IHS criteria might have a stronger association than probable cases in which a higher possibility of misclassification cannot be ruled out.
Strengths of the study lie in the large sample of the adult population including comparable proportions of men and women in similar age ranges. Although not representative of the Brazilian population, we included participants of six cities in three different regions of the country. These population characteristics permit us to explore some differences regarding gender, for example. Besides that, diabetes diagnosis was made not only by previous medical history of diabetes, use of medication or fasting plasma glucose ≥126 mg/dl, but was also based on two-hour post-load glucose ≥ 200 mg/dl or an HbA1C ≥ 6.5%. Finally, we recorded all medication about hypertension, dyslipidemia and migraine prophylaxis that were considered in our multivariable analyses.
Our findings suggest a possible gender influence on the relationship between migraine and cardiovascular risk factors. Hypertension and metabolic syndrome were negatively associated to definite migraine, particularly among male participants, but not in women. On the other hand, dyslipidemia was positively associated with all migraine categories (probable, definite and overall) in women, but not in men. Further information about the relationship between migraine and CVRF will be available during the ELSA-Brasil study follow-up.
Clinical implications
Despite variances due to definitions of migraine and cardiovascular risk factors, population and environmental factors reported in previous publications, a possible gender influence on the relationship between migraine and cardiovascular risk factors is suggested at the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) baseline assessment. Hypertension and metabolic syndrome were negatively associated with definite migraine, particularly among male participants. On the other hand, dyslipidemia was positively associated with all migraine subtypes in women.
Footnotes
Funding
The ELSA-Brasil baseline study was supported by the Brazilian Ministry of Health (Science and Technology Department) and the Brazilian Ministry of Science and Technology (Financiadora de Estudos e Projetos and CNPq National Research Council) (grants 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ).
Conflict of interest
None declared.
Acknowledgments
The authors thank the research team of the ELSA-Brasil study for their contributions.