
Abstract
Schizophrenia (SZ) [MIM181500] is a severe, debilitating disorder characterized by delusional beliefs, hallucinations, disordered speech, and deficits in cognition and in emotional and social behaviour. Although family, twin and adoption studies suggest a strong influence of genetic factors upon liability [1], efforts to identify SZ risk genes have achieved only limited success. This reflects the substantial challenges besetting SZ genetic studies, including phenotypic variability within SZ, diagnostic imprecision with respect to closely related disorders, genetic heterogeneity, the small effect of individual risk variants, an unknown degree of gene–gene interaction, and the involvement of a substantial but poorly understood environmental component.
A potentially important limitation of SZ genetic studies is phenotypic and diagnostic heterogeneity. In the absence of confirmed biological markers, SZ classification is based primarily on the severity and relative duration of symptoms, associated functional impairment, and course of illness. No one symptom characterizes SZ, with many occurring in other disorders, such as bipolar disorder or schizoaffective disorder (SA). Clinical variability and the absence of clear boundaries between SZ and SA may confound genetic analyses if distinct aetiological processes characterize the syndromes [2]. An additional diagnostic difficulty in SZ is the high prevalence of comorbid substance abuse, estimated to range from around 15% to 65% [3]. Substance use can produce psychotic syndromes strongly resembling SZ, but aetiological features of the two syndromes may differ. Joint analysis of these two phenotypes may introduce noise and impede the identification of SZ risk loci. Schizophrenia samples with reduced diagnostic heterogeneity – including lower rates of SA and comorbid substance use – may thus offer advantages for identifying SZ risk loci.
Power to detect SZ risk genes may be increased via population sampling strategies that increase genetic homogeneity and/or simplify the complexity of gene–environment interactions. Population groups that are ethnically homogeneous [4] or have high consistency of environmental risk factors [5] may thus be beneficial.
We report here the study design and clinical characteristics of an ethnically and diagnostically homogeneous SZ pedigree sample recruited in the south-Indian state of Tamil Nadu. The hierarchical caste system has long dominated marital and cultural interactions in India, with strict endogamy producing social stratification and barriers to gene flow between groups. This was likely augmented by geographical dispersal and subdivision of the country into different linguistic regions [6]. Generally, Indian population subgroups have adhered to traditional living arrangements and occupational roles, which could increase homogeneity of environmental factors influencing disease risk. Indian SZ prevalence and incidence rates are similar to other populations, with reported point prevalences of 2.6 per 1000 in Agra [7] and 2.5 per 1000 in Chennai (formerly Madras) [8]. Annual incidence rates per 1000 population have been estimated as (0.09/0.11) for urban/rural Chandigarh [9] and 0.41 for urban/metropolitan Chennai [10].
Previous studies suggest that the expression of psychotic disorders in India is characterized by low rates of SA and comorbid substance use. The Madras prevalence study of 100 000 people that detected 360 cases of ‘functional’ psychosis did not detect any cases of SA [8], nor did the subsequent incidence study [10]. Additionally, the Indian site of the International Study of SZ) detected no SA [11]. Low rates of comorbid substance use have also been observed in Indian SZ patients [12, 13].
Methods
Sample recruitment
The SZ Research Foundation, India (SCARF) is a major psychiatric research facility in Chennai, Tamil Nadu, and was the centre for sample recruitment and ascertainment. All relevant institutional ethic committee approvals were obtained and all participants gave written, informed consent.
Initially, we examined all available SCARF medical records to identify families with two or more siblings with SZ, that is, affected sibling pair (ASP) pedigrees. Subsequently, we also recruited trio families, that is, a single affected offspring with both parents. Recruitment was initially focused on Tamil Brahmin pedigrees, and then extended to include geographically proximal caste groups from Tamil Nadu (Mudaliars, Chettiars, and Dalits). Brahmins from the neighbouring states of Kerala, Karnataka and Andhra Pradesh were also included because sufficient evidence existed that genetic distances between these caste groups were small [14]. For each pedigree we collected blood samples for all affected offspring, available parents and unaffected siblings when necessary. Sample collection was extended throughout Chennai and surrounding regions via SCARF's well-established recruitment network of clinicians. In addition to pedigrees identified via treatment facilities, we also identified families whose ill members had never been treated.
Inclusion/exclusion criteria
A completed ASP pedigree was required to include a proband with DSM-IV SZ plus at least one sibling affected with either DSM-IV SZ or SA and available parents. To standardize SA diagnoses, we operationalized the mood syndrome duration criterion at 30% of total illness duration, consistent with other major genetic studies [15]. Trio pedigrees were required to include one individual with a diagnosis of DSM-IV SZ plus both parents. All families consisted of individuals from a single caste group. Additional relatives (i.e. not trio probands or ASP siblings) were defined as affected if they met criteria for DSM-IV SZ, SA or other non-affective psychoses. Participants were defined as unaffected based on the Family Interview for Genetic Studies (FIGS) [16, 17] psychosis screen. Diagnoses were assigned using both DSM-IV [18] and ICD-10 [19] systems. Exclusion criteria for individuals were: (i) age under 18 years; (ii) inability to give informed consent to all aspects of the study; (iii) psychosis judged to be secondary to substance use or a known neurological disorder such as epilepsy; and (iv) severe mental retardation.
Clinical ascertainment
The principal investigators (PI) trained the Chennai clinical team in selecting and prioritizing pedigrees and using diagnostic instruments. The team consisted of psychiatrists, psychologists and social workers, experienced in mental health research. The principal investigators conducted an initial set of training sessions to standardize eliciting of psychopathology, and for longitudinal consistency, regular consensus sessions were conducted throughout the study.
Family Interview for Genetic Studies
For each family, one or more reliable informants were interviewed using the FIGS. These interviews enabled: (i) verification of the entire pedigree's caste membership; (ii) identification of additional, related affected individuals; (iii) formal screening of unaffected individuals using the FIGS Psychosis screen; and (iv) provision of supplemental diagnostic information for the proband.
Diagnostic Interview for Genetic Studies
Affected individuals were interviewed with the Diagnostic Interview for Genetic Studies (DIGS) [20], a comprehensive, semi-structured interview for studies of psychotic, mood and substance use disorders. Interviewers subsequently wrote a narrative that summarized key features of the subject's psychiatric history and mental state, including detailed descriptions of psychotic symptoms.
The DIGS and FIGS were formally translated into the local Tamil language and back-translated into English by clinicians fluent in both languages. For the majority of Tamil participants, interviews were conducted in Tamil. A small number of participants were fluent in English and were hence interviewed in English. Non-Tamil participants’ interview schedules were translated into the relevant non-Tamil language by interviewers fluent in the relevant language, and then back-translated into English. All interview data were translated into English and subsequent narrative reports were also written in English.
Medical records
For affected participants, available medical records (recorded in English) were retrieved. These records provided important information regarding symptoms, age of onset and course of illness.
Best estimate diagnosis
DIGS interview, interviewer narrative, available medical records, and FIGS reports formed the basis for diagnostic review. Diagnoses were assigned using the best estimate final diagnosis procedure [21], with two Chennai psychiatrists independently reviewing all available information and then conferring to assign a consensus diagnosis. Additionally, all cases were independently reviewed in Brisbane by a third psychiatrist (BM). Outstanding questions were resolved through discussion and sometimes involved the collection of further clinical information.
Diagnostic inter-rater reliability
In preparation for this project, we conducted a diagnostic inter-reliability study of 20 psychosis patients (10 Indian, 10 Australian). All available information on each patient (interview data, medical records) was reviewed by each PI. High reliability was achieved, with disagreement in one of 20 cases (κ = 0.886).
Power analyses
Power to detect genetic linkage in the recruited ASP pedigrees was assessed for 10 genetic models (Table 1). Dominant, recessive, and (one) additive penetrance models were specified with: (i) phenocopy rates between 0.068 and 0.44; (ii) locus-specific ratio of risk in slibings, relative to risk in general population (λsibs) from 1.23 to 4.77; (iii) the proportion of linked pedigrees (α) ranging from 0.3 to 1.0 such that (iv) population-wide λsibs varied between 1.21 and 1.67. Models were specified such that the population prevalence of disease (SZ and SA) was within the expected range of approximately 0.6–1.2% based on epidemiological studies conducted in various populations, including the Madras epidemiological studies, which indicate that the prevalence of SZ in Tamil Nadu is consistent with that in other populations. Thus the present λsibs estimates were relevant for this Tamil Nadu population.
Genetic models for linkage power analyses
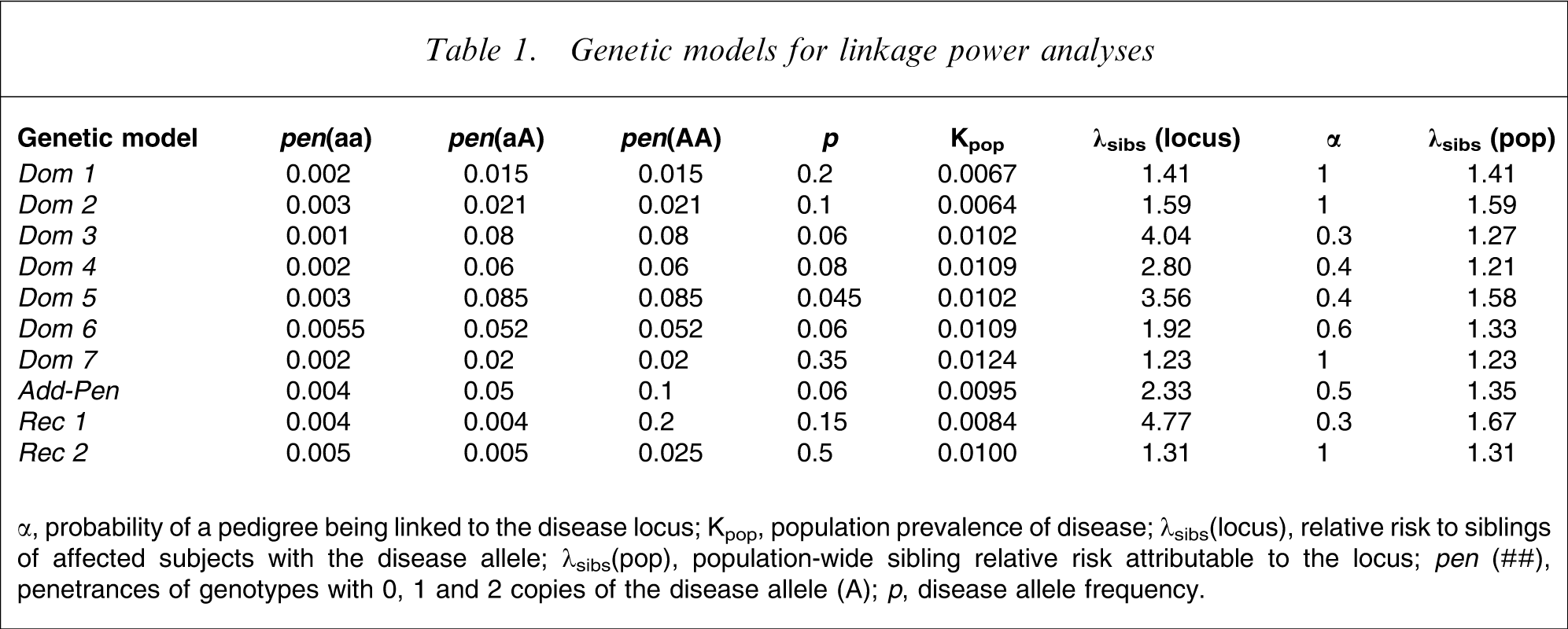
α, probability of a pedigree being linked to the disease locus; Kpop, population prevalence of disease; λsibs(locus), relative risk to siblings of affected subjects with the disease allele; λsibs(pop), population-wide sibling relative risk attributable to the locus; pen (##), penetrances of genotypes with 0, 1 and 2 copies of the disease allele (A); p, disease allele frequency.
For each model, ALLEGRO [22] was used to generate 1000 replicates of the recruited ASP cohort (n = 159 pedigrees). We simulated a 40 cM region with the disease locus at 20 cM. The genetic map was based on the Illumina Linkage IV panel, exemplifying current high-density single nucleotide polymorphism (SNP) linkage maps. This panel contains 5861 SNPs with an average inter-marker distance of 0.64 cM, yielding average information content >97.1%. The simulated region contained 63 evenly spaced, biallelic markers with average minor allele frequency of 0.37, consistent with the Linkage IV panel distribution in Caucasian (Centre d'Etude du Polymorphisme Humain: CEPH) pedigrees. Linkage analyses were conducted with ALLEGRO using the non-parametric exponential logarithm (base 10) of the likelihood ratio of the assumption of linkage compared with that of no linkage (LOD) score [23] (LODexp) and the Spairs score statistic [24].
Results
Pedigree sample
The present study included 1180 individuals from 346 pedigrees. A total of 609 individuals were affected with SZ (n = 604) or a related non-affective psychotic disorder (n = 5). Consensus diagnoses are currently available for 504 affected individuals.
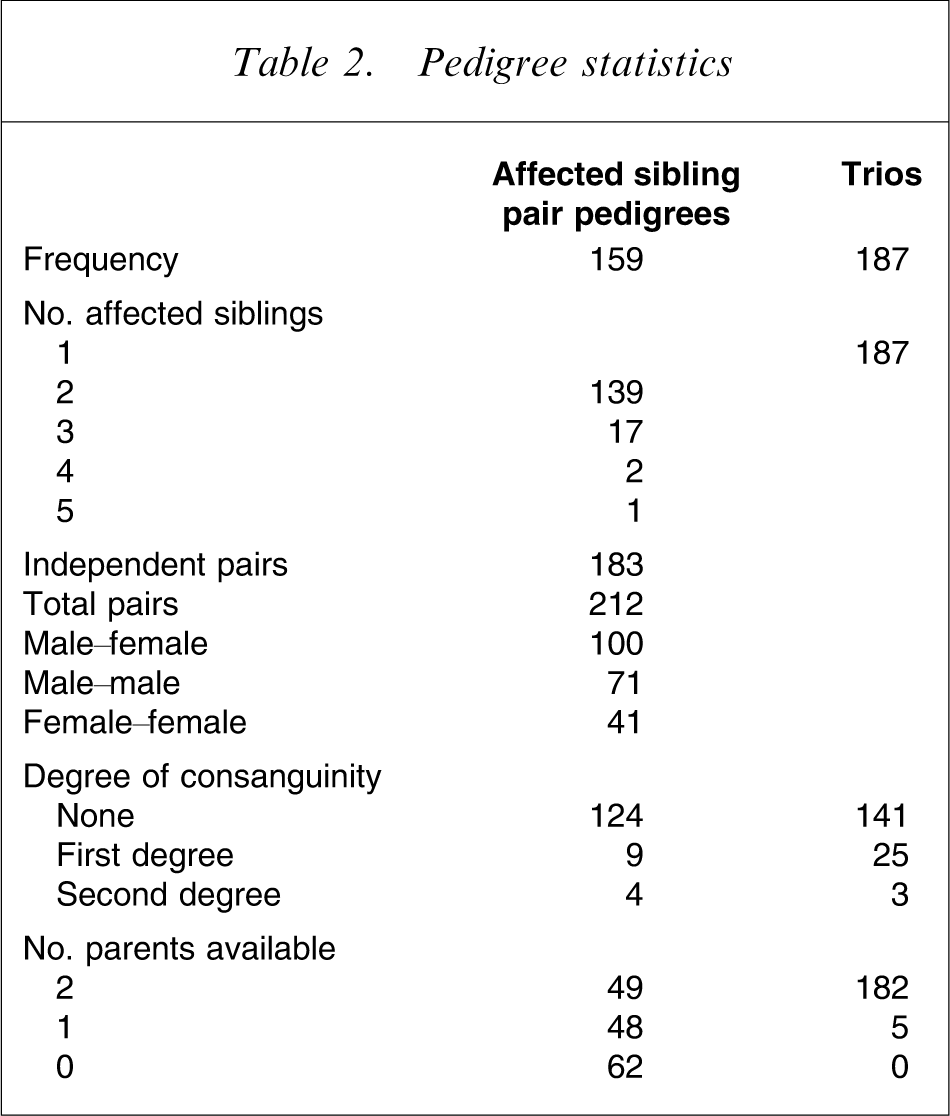
Descriptive pedigree statistics are shown in Table 2. Of 346 total pedigrees, 159 contained at least two affected siblings (ASP) and 187 contained a single affected individual and their parents (trio). The 159 ASP families contained a total of 212 possible sibling pairs and 183 independent pairs. Of the 346 pedigrees, 231 (66.8%) were Tamil Brahmin, 12 (3.5%) were non-Tamil-speaking Brahmin, and 103 (29.7%) were from other Tamil caste groups. Consanguinity data were available for 307 pedigrees. We defined marriage between first cousins and uncle–niece unions as first-degree consanguinity and marriage between second cousins as second-degree consanguinity. A total of 41 pedigrees (13.7%) were consanguineous, the majority (n = 34) being first degree. There was no significant difference in the incidence of consanguinity between ASPs and trios.
Pedigree statistics
Demographic features
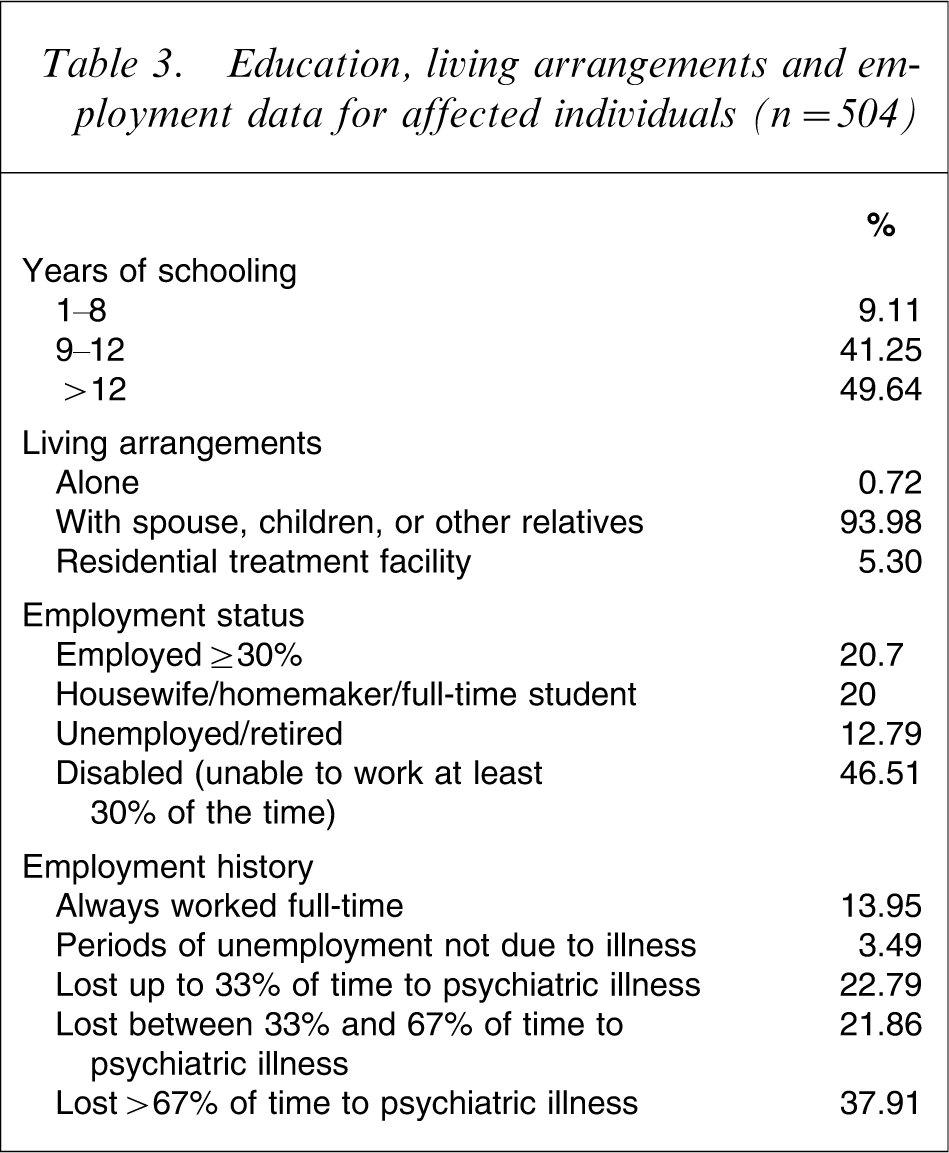
Table 3 shows education, living arrangements, and employment data for affected participants. The majority had graduated from high school, and nearly all lived with close relatives. Almost 50% were disabled and unable to work, and 60% had lost at least 33% of their working life to psychiatric illness, but >40% were working (remunerated/studying/home duties) at least 30% of the time.
Education, living arrangements and employment data for affected individuals (n = 504)
Clinical characteristics
Table 4 shows the frequencies and mean values of salient clinical characteristics in the sample of affected individuals with consensus diagnoses (n = 504). Of this sample, 291 (57.7%) were male, and 213 (42.3%) were female. Mean age of onset was 23.3 years for both male and female subjects, and mean duration was 14.8 years, indicating a chronic course. There was a low prevalence of comorbid medical conditions. Individuals with a history of complicating organic factors such as pre-psychotic epilepsy (n = 16), head injury (n = 9), mild mental retardation (n = 5), and abnormal birth/early development (n = 13) were included only if diagnostic consensus judged these factors unlikely to have caused psychosis. Nearly 30% of affected participants were married, although a majority (approximately 56%) had never married. Male participants were significantly more likely than female participants to have never married (χ 2 1 =8.03, p = 1.8×10−8).
Clinical characteristics of affected individuals
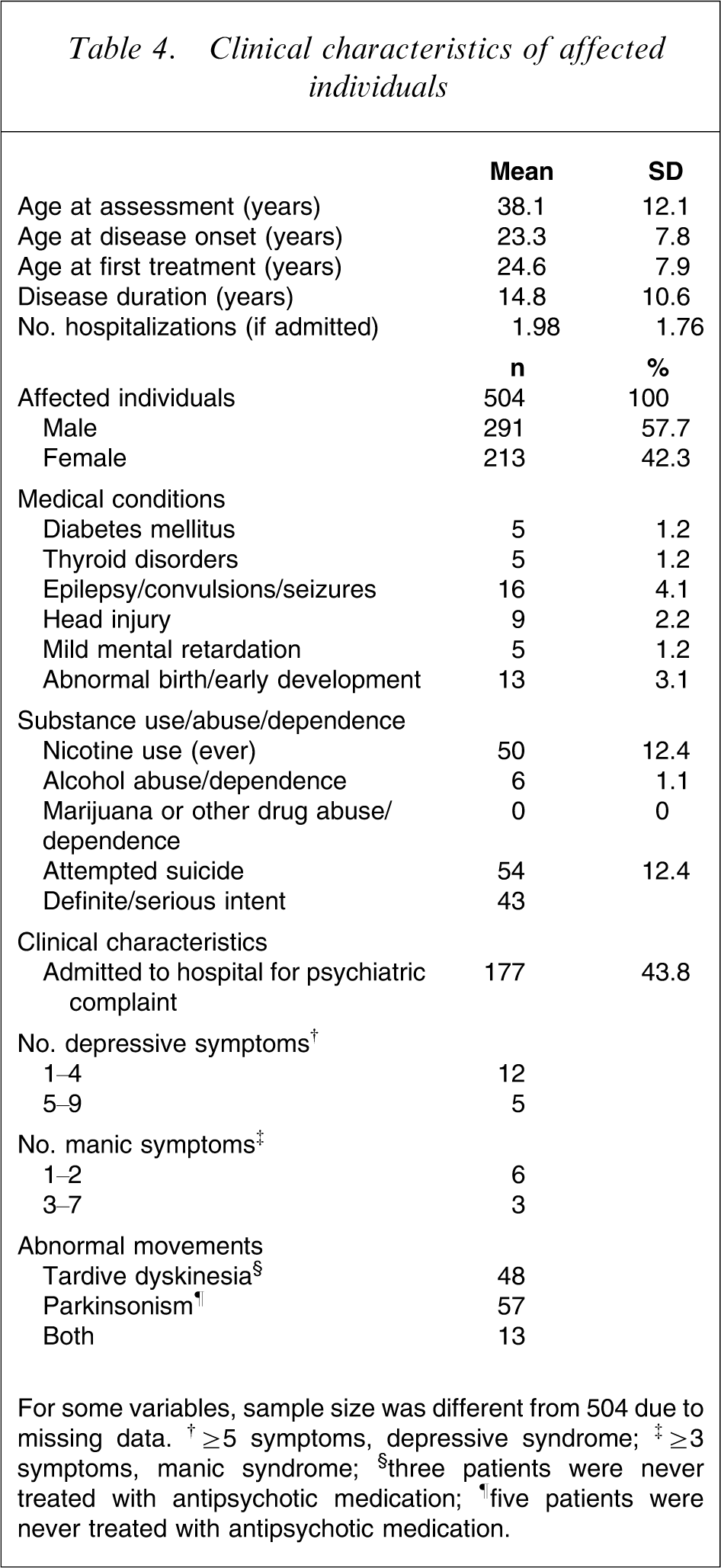
For some variables, sample size was different from 504 due to missing data. †≥5 symptoms, depressive syndrome; ‡≥3 symptoms, manic syndrome; §three patients were never treated with antipsychotic medication; ¶five patients were never treated with antipsychotic medication.
A significant feature of this dataset is the exceptionally low incidence of substance use/abuse including alcohol, cannabis, and other illicit drugs. Nicotine use (ever) was reported by only 12.4% of affected individuals and no individuals reported illicit drug use or abuse.
Using the Abnormal Involuntary Movement Scale (AIMS), 48 people demonstrated tardive dyskinesia (TD), defined as the presence of two or more mild or one or more moderate symptoms from the first seven AIMS items [25]; three of these had never received antipsychotic treatment. Based on the Simpson and Angus scale [26], 57 individuals had parkinsonian symptoms, defined as present if the mean score was >0.3; five of these had never received antipsychotic treatment. Thirteen individuals satisfied criteria for both TD and parkinsonism.
Diagnosis
Table 5 shows the distribution of diagnoses for affected individuals. The present sample almost exclusively consisted of individuals with SZ, and there was a very low prevalence of SA and other non-affective psychotic disorders. ICD-10 appears slightly more restrictive than DSM-IV, with fewer individuals fulfilling ICD-10 criteria for SZ. ICD-10 is more restrictive than DSM-IV in that hallucinations and delusions together account for only one criterion and the schizophrenia syndrome is required to occur before the affective syndrome. For individuals with DSM-IV SZ, the frequency distribution of characteristic symptoms is shown in Table 6. There was a high prevalence of delusions, hallucinations and disorganized behaviour. Negative symptoms were experienced by >90% of affected participants. Bizarre delusions such as the one described as follows were less frequently observed. One of the subjects stated that she was a snake goddess who was married to the Naga Raja (Snake king) with whom she had several snake children. A man (who is her real husband) slew her snake husband to steal the Nagamani (a mythical jewel crowning the sake's head in Indian lore), captured her in the process and has been forcibly living with her since. Another kind of bizarre delusion seen in a number of instances related to the delusion of being pregnant, including one case in which the subject believed that she was pregnant for 21 years. Conversational/commentary auditory hallucinations were also less frequently seen. The most common of these were hearing voices issuing threats or discussing the subject in derogatory terms such as questioning their sexual identity.
Clinical diagnoses of affected individuals
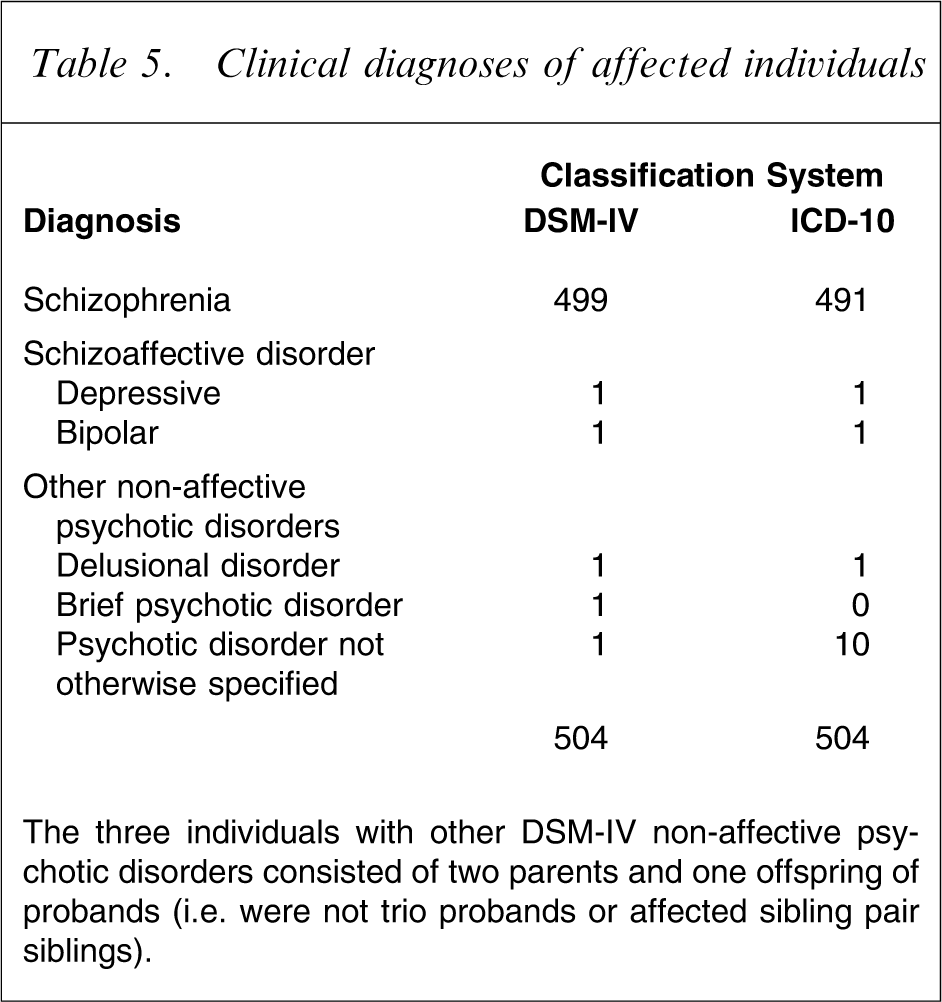
The three individuals with other DSM-IV non-affective psychotic disorders consisted of two parents and one offspring of probands (i.e. were not trio probands or affected sibling pair siblings).
Frequency of DSM-IV symptoms in interview cases of schizophrenia (n = 499)
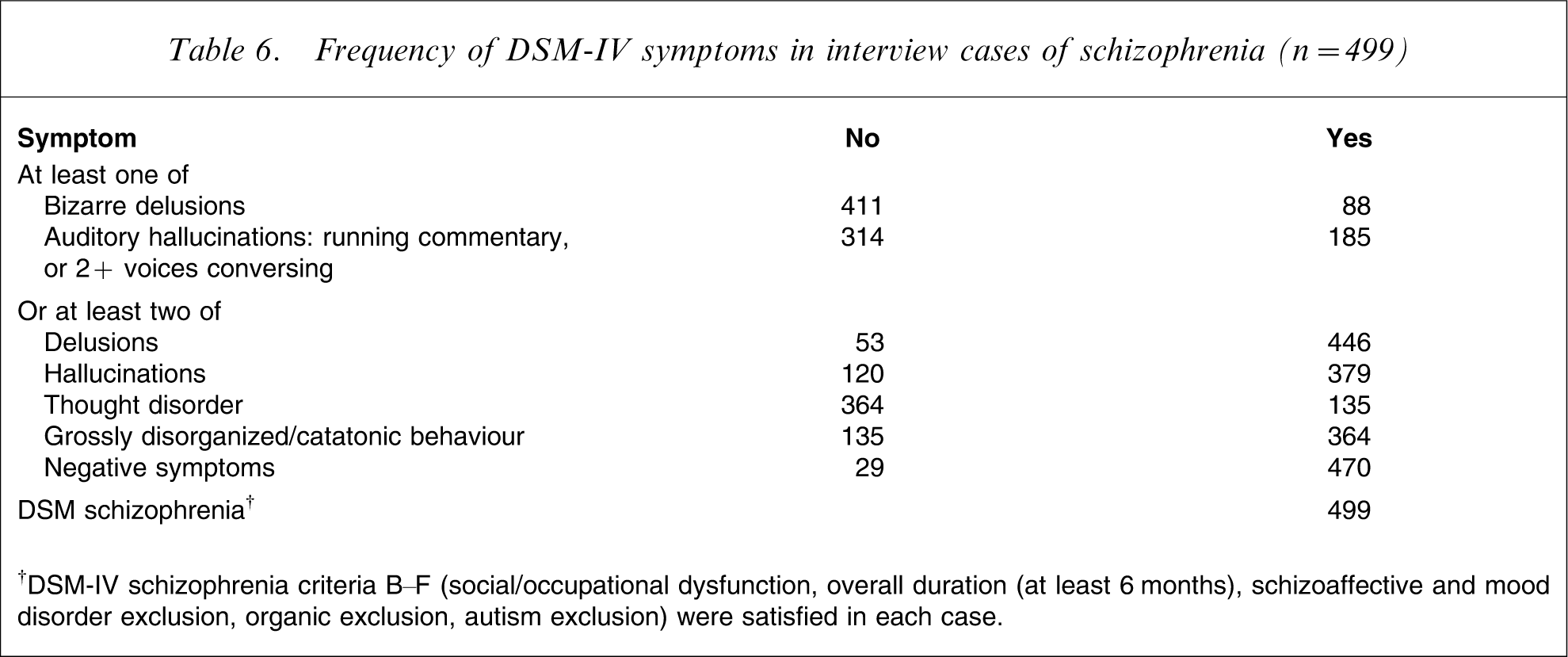
†DSM-IV schizophrenia criteria B–F (social/occupational dysfunction, overall duration (at least 6 months), schizoaffective and mood disorder exclusion, organic exclusion, autism exclusion) were satisfied in each case.
Functioning
We used the Global Assessment of Functioning (GAF) [18] as a quantitative measure of illness severity. We rated both components of the GAF = functioning (GAF) and symptoms (GAS) [27]. The mean lifetime (GAF = 31.9, GAF = 26.4) and past-month scores (GAF = 49.4, GAF = 48.4) indicated serious symptomatology and major functional impairment. Based on t-tests, female subjects had significantly higher past month functioning than male subjects (t = 2.68; p = 0.0076), consistent with previous Chennai studies [28].
Power analyses
Table 7 shows power to detect linkage in the ASP sample for 10 genetic models. Power was highest for the dominant model D2 and the recessive model R1 (Table 1), which had population-wide λsibs of 1.58 and 1.67, respectively. Under these models the sample had approximately 35–45% power to detect significant linkage (LOD = 3.6) and approximately 70–80% power to detect suggestive linkage (LOD = 2.2) at thresholds suggested by Lander and Kruglyak [29], and >90% power to replicate previously reported findings at nominal p < 0.01 (LOD = 1.18). Power was low for models with λsibs<1.3.
Power of the ASP sample (n = 159 pedigrees) to detect linkage
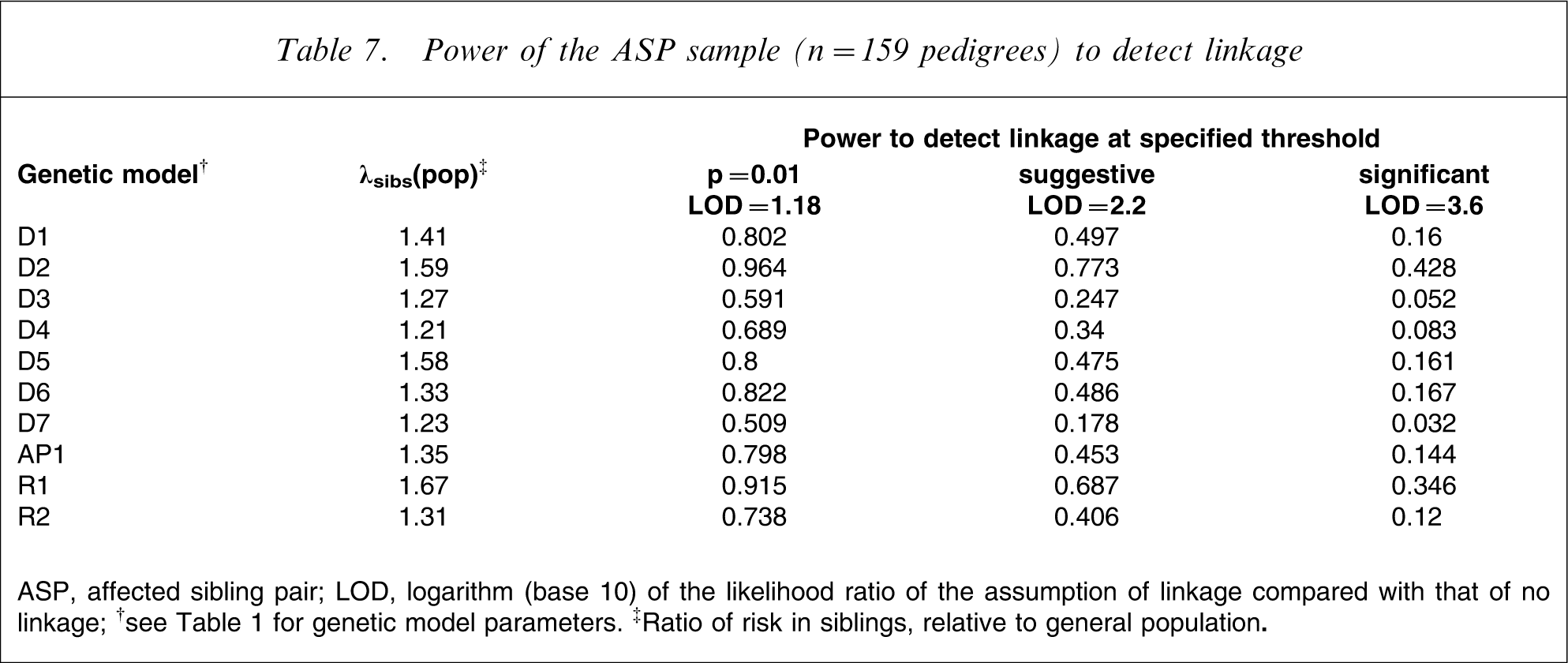
ASP, affected sibling pair; LOD, logarithm (base 10) of the likelihood ratio of the assumption of linkage compared with that of no linkage;
†See Table 1 for genetic model parameters.
Discussion
The present study reports the recruitment and ascertainment of 346 ethnically and diagnostically homogeneous south Indian pedigrees (159 ASPs, 187 trios). The study primarily consists of pedigrees from a single caste group, the Tamil Brahmin, from which we exhaustively recruited ASPs and trios within the defined study region. Subsequently, we expanded the core sample to include other caste groups living in and around Chennai [30]. Population genetic studies supported this ascertainment strategy, demonstrating (i) low genetic differentiation among Tamil castes (RST=0.96% for 45 autosomal short tandem repeat (STR) markers) [14], where RST is the proportion of allele size variance between populations [31]; and (ii) genetic differentiation of these groups from other continental world populations demonstrated by greater genetic distance estimates (Dsw) [32] between all Tamil castes and both European and East-Asian subjects, compared to distances between individual Tamil castes, based on 45 autosomal STRs [14]. The observed low level of consanguinity in the present sample (13%) is consistent with the occurrence of uncle–niece and first cousin unions; the impact of consanguinity will be explored in our planned genetic analyses.
In addition to ethnic homogeneity, the present sample demonstrated high consistency of several demographic and cultural factors. All participants lived in the same geographic and climatic region. In addition, 94% of the affected sample lived with close family members, consistent with Indian cultural tradition, which increases uniformity of the participants’ sociocultural environment. Increased environmental homogeneity may facilitate gene identification by reducing phenocopy rate and increasing penetrance. It is also noteworthy that the proximity of closely related family members enhanced the completeness of collected family data.
A striking feature of the present sample is the very low rate of drug use/abuse, usually a common comorbid factor in SZ. None of the affected participants had used illicit drugs such as cannabis, amphetamine, and cocaine; only 1.1% reported alcohol abuse/dependence, and only 12.4% had ever smoked. These are among the lowest rates ever reported, but are consistent with a previous longitudinal follow-up study of SZ in Chennai [33]. In contrast, the Australian prevalence study of psychosis reported nicotine use in 73.2% of male and 56.3% of female subjects [34], while the World Health Organization 10-country study reported alcohol abuse in 57% of male subjects and, in three of the 10 centres, cannabis and cocaine abuse of 24–41% [9]. A recent SZ genetic study also reported drug dependence (alcohol, cannabis, cocaine, amphetamine) in 24.6–42.3% of male and 16.9–23.5% of female subjects from European and African–American ancestral groups [15]. Interestingly, the largest published linkage study of SZ, which was conducted in 607 ASP Taiwanese pedigrees of Han Chinese descent, also reported low rates of alcohol abuse/dependence (5.2%) and other drug abuse/dependence (3.7%) [35]. These findings suggest a cultural basis for comorbidity of drug and alcohol use with SZ, suggesting lower rates in Asian and Indian populations. In the present sample a potential explanatory factor was the high rate of cohabitation with family members (94%), which may reduce financial independence and the freedom to both purchase and use alcohol and illicit drugs [36]. The low prevalence of drug use is a favourable feature for gene identification, because it reduces phenotypic complexity, simplifies diagnostic evaluation and may reduce the impact of gene–environment interactions upon disease risk.
This sample also demonstrates remarkable diagnostic homogeneity. Of the 504 affected individuals with detailed diagnostic data available, 499 had a consensus diagnosis of DSM-IV SZ. There were only two cases of SA (one bipolar, one depressive) in siblings of probands, and three cases of DSM-IV non-affective psychotic disorders in parents and offspring. Most genetic studies of SZ include SA as part of the ‘core phenotype’. The proportion of SA cases is frequently in the range of 10–20% [15, 37] although lower rates have also been reported [38, 39]. We attribute the present pure SZ cohort at least in part to the focused recruitment on this disorder within clinical networks in Chennai and surrounds. Low rates of SA may also characterize the expression of psychotic disorders in this population [8, 10, 11]. It is not clear whether the prevalence of SA in India is truly lower than in other cultures, or rather reflects an ascertainment or reporting bias. In the present sample, however, individual mood symptoms were documented for every case and multiple sources of observation (individual, multiple family members, medical records) were evaluated by experienced research psychiatrists, two of whom were involved in assigning consensus diagnoses. As a result we are confident that the presence of only two SA cases is a reliable finding. The preponderance of SZ cases in the present sample may reduce genetic heterogeneity and improve power to resolve risk factors specific to SZ.
The majority of individuals in the present sample had a severe illness, with >80% demonstrating moderate to severe deterioration and poor lifetime and past month functioning; in contrast, participants in the Madras (Chennai) Longitudinal Study (MLS) of SZ showed a less severe illness in terms of clinical symptoms and social functioning [33]. Differences in treatment between the two samples likely contribute to these differential outcomes, because the MLS sample was closely followed up and regularly treated, whereas the present sample was not. Another striking feature of the present severely ill SZ sample was that <50% were ever hospitalized. In India, hospital facilities for psychiatric admission are meagre and largely located in urban areas [40], and community services are generally non-existent. Thus, the majority of individuals with SZ are cared for at home by their families. In many cases, hospital admission is sought by families only when patients are violent or aggressive.
Linkage power analyses suggested that this sample has low power to detect significant or suggestive linkage to loci of the effect size typically expected for schizophrenia (λsibs=approx. 1.2–1.3). For such loci, the sample has good power to replicate previously reported linkages at nominal p < 0.01, which will help clarify the extent to which linkage findings converge across different populations. Several features of this sample also suggest its potential enrichment for one or more disease alleles of larger effect (λsibs=1.5–1.7), which are more likely to achieve suggestive or significant thresholds. These include ethnic homogeneity, uniformity of environmental exposures and high diagnostic homogeneity in the presence of very low comorbid substance use. Following linkage, proposed follow-up analyses include family-based association mapping of identified regions using all ASPs and trios. The inclusion of linked pedigrees may increase power to detect associated variants in linked genomic regions [41]. Recruitment of a large case–control cohort is under way; this may be combined with the existing sample to further increase power or used to replicate promising association findings.
The present sample contained more affected men than women, consistent with other samples and epidemiological studies suggesting a higher prevalence of SZ in male subjects [42]. Although an earlier age of onset for male than female subjects is commonly reported [43], we observed no gender difference in age at illness onset. But this finding is consistent with those from other familial samples [44, 45]. We observed significantly higher past-month functioning in women. This may reflect substantially lower pressure for women to achieve and perform in the occupational sphere in India [28]. Affected women were also more likely to marry, which may relate to their higher level of functioning, but cultural factors favouring marital status for women may also be involved. We also detected a high average level of education, with nearly 50% of probands achieving >12 years of formal education. This reflects the fact that the samples were primarily drawn from urban settings and recruited from the Brahmin community, which has always placed a strong emphasis on education. These data are unlikely to represent the educational status of either the Indian schizophrenia population or the Indian general population.
In conclusion, we report the ascertainment and clinical characteristics of an ethnically homogeneous schizophrenia pedigree sample from southern India. Consistent with previous studies, the present sample demonstrated extremely low rates of SA and comorbid substance use. We also observed high uniformity of participants’ sociocultural environment. These features may assist efforts to identify SZ risk loci.
Footnotes
Acknowledgements
We thank the patients and family members who participated in this study and the staff of Sowmanasya Hospital, Tiruchi for their support. This study was supported by the Australian National Health and Medical Research Council grant 143027.