
Abstract
Keywords
At the 2006 Census 28% of New Zealand families with one or more dependent children were headed by a sole parent; a large increase from 10.4% in 1976 [1, 2]. The only existing nationally representative study of sole parents’ health status shows that they tend to experience poorer health – especially mental health – than partnered parents [3]. Other smaller studies focusing on sole parents who receive benefits have highlighted an elevated risk of poor mental and physical health among this group [4, 5]. This is consistent with a range of international studies [6–8]. Australian research, for example, points to particularly high rates of mental health problems among sole parents who receive welfare benefits in that country [9].
This paper extends the New Zealand evidence base on the mental health of sole parents, using data from a nationally representative, population-based mental health survey. We describe the 12 month prevalence of diagnosable mental disorders among sole parents compared to partnered parents, by severity and type of disorder. We then quantify the excess risk of specific, diagnosable mental illnesses experienced by sole parents, and estimate the extent to which this excess risk is associated with differences between sole parents and partnered parents in demographic variables, physical health, socioeconomic position (SEP) and co-residence of another adult (as a proxy indicator of social and practical support) [10].
We hypothesize that the disadvantaged SEP of sole parents (as measured by income and employment status) accounts for most if not all of their excess risk of mental illness. We further hypothesize that co-residence with another adult and physical health status will be additional, albeit minor, determinants of the excess risk (if any) of poor mental health for sole parents.
Methods
New Zealand Mental Health Survey
The New Zealand Mental Health Survey was a nationally representative household survey of 12992 adults aged ≥16 years, with a stratified multistage clustered sample design. One adult was sampled per household selected. Face-to-face interviews were carried out between October 2003 and December 2004 by specially trained interviewers, in English. The interview was based on version 3.0 of the Composite International Diagnostic Interview (CIDI), which yields DSM-IV or ICD-10 diagnoses, including lifetime, 1 month and 12 month prevalence of anxiety, mood, substance use and eating disorders and suicidality. Sociodemographic and physical health status information was also collected. The response rate achieved was 73.3%. More detail regarding survey methods is provided elsewhere [11].
Analysis
Data were weighted to account for the clustered sample design, different probabilities of selection and differential non-response. All prevalence estimates reported are the population-weighted estimates. Marginal frequencies were calculated using the SURVEYFREQ procedure, and multivariable models including all two-way interaction (cross-product) terms were analysed on multiple logistic regression using the SURVEYLOGISTIC procedure in SAS (version 9.1.2; SAS Institute, Cary, North Carolina, USA).
Explained fractions
The proportion of the elevated risk of mental illness experienced by sole parents that was mediated by physical health status, SEP, co-residential adult (social support) or any combination of these variables was estimated using the ‘explained fraction’ approach: Explained fraction=[(ORa−1) – (ORb−1)]/(ORa−1), where ORa is the OR for the model adjusting only for demographic variables, and ORb is the OR for models including additional non-demographic variables as relevant (for explanation of the different models, see Table 4).
Definitions
Parents were defined as respondents aged 16–64 years living with either their own or their partner's child (or children), with the youngest child in the household aged under 16 years. Partnered parents were those who self-reported that they lived with their ‘legal husband or wife’ or their ‘partner or de facto, boyfriend or girlfriend’. Sole parents were the remaining parents.
Mental disorders were defined in terms of 12 month prevalence, using the CIDI version 3, a widely used computer-assisted structured interview that produces valid and reliable psychiatric diagnoses. More specifically, the CIDI generates DSM-IV diagnoses by determining whether the respondent has ever in their lifetime met the criteria for the disorder, then determines the last time the person had an episode or key symptoms of the disorder (irrespective of treatment). If this was within 12 months of interview, this is classified as a ‘12 month disorder’. Diagnoses included were anxiety disorders (panic disorder, agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, post-traumatic stress disorder, obsessive–compulsive disorder), mood disorders (major depressive disorder, dysthymia, type I and type II bipolar disorder) and substance use disorders (alcohol abuse, alcohol dependence, drug abuse, drug dependence, marijuana abuse, marijuana dependence). Suicidal ideation (defined as having ‘seriously thought about committing suicide’) in the past 12 months was included as a separate outcome. Prevalence of rare conditions such as schizophrenia and other psychotic disorders could not be reliably estimated from this household survey. Organic brain syndromes such as dementia were also excluded from data collection [11].
‘Serious’ mental disorder was defined as the combination of a CIDI 12 month diagnosis and either significant role impairment or impaired functioning, with at least two areas of role impairment on the Sheehan Disability Scale, or a score of ≤50 on the Global Assessment of Functioning Scale [11].
Chronic physical illness was defined as a doctor-diagnosed physical condition lasting ≥6 months. Income (measured in quartiles) was defined as household income from all sources, adjusted for household size and composition using the modified Jensen scale [12]. Labour market attachment was dichotomized as employed (if respondents indicated that they were ‘employed’ or ‘self-employed’) or not employed (unemployed or not in the labour force). SEP was defined in terms of income and employment status. Co-residence of another adult (as a proxy measure for social support) was dichotomized as supported (living with one or more other people in the household who are aged ≥16 years) or not supported (living without another adult in the household).
Co-variates considered but not included in the final multivariable analyses were neighbourhood deprivation (New Zealand Deprivation Index 2001 quintile), education and main welfare benefit receipt (i.e. unemployment or domestic purposes). None of these variables added explanatory power over and above the variables already included in the models.
Results
Descriptive findings
The sample included 1216 sole and 3681 partnered parents of dependent children. Sole parents were more likely than partnered parents to be young, female, of Maori or Pacific ethnicity, and to be receiving a domestic purposes benefit or an unemployment benefit as their main source of income. The descriptive findings are summarized in Tables 1–3.
DSM-IV 12-month prevalence diagnoses among sole parents vs age group (unadjusted rates,†%)
†Calculated from frequencies using PROC SURVEY FREQ, SAS.
n=1261 for sole parents.
DSM-IV 12-month prevalence diagnoses among parents (unadjusted† and adjusted rates‡,%)
†Calculated from frequencies using PROC SURVEY FREQ, SAS.
‡Age, sex and ethnic group standardized to the total New Zealand 2001 Census Population.
DSM-IV 12-month prevalence diagnoses among sole parents vs gender and benefit receipt (unadjusted rates†,%)
†Calculated from frequencies using PROC SURVEY FREQ, SAS.
‡Receiving unemployment or domestic purposes benefit at the time of the survey.
n=1261 for sole parents.
Overall, 43% of sole parents met the criteria for a DSM-IV diagnosable mental disorder in the past 12 months, compared to 19% of partnered parents. After adjustment for differences in age, sex and ethnic group, sole parents remained much more likely to have met the criteria for a DSM-IV disorder in the past 12 months compared to partnered parents (Table 2). After demographic adjustments, 7% of sole parents met the criteria for a serious mental disorder, compared to 3% of partnered parents. Twenty-four per cent of sole parents had an anxiety disorder; 15%, a mood disorder; 6%, a substance use disorder; and >5% had experienced suicidal ideation in the past 12 months – in each case at least twice the rate observed in partnered parents (adjusting for the demographic variables).
Sole parents were three times more likely (9.8%, 95%CI=5.4–17.2) to experience comorbidity of DSM-IV diagnosable mental disorders (mostly anxiety and mood disorders) than partnered parents (3.3%, 95%CI=1.9–5.8), once adjusted for age, gender and ethnic group differences between sole and partnered parents.
Among sole parents, men and women were equally likely to have any mental disorder (Table 3), whereas female partnered parents were more likely to meet the criteria for any mental disorder than their male counterparts. Sole parents receiving a main welfare benefit (unemployment or domestic purposes) were more likely than sole parents who were not receiving a welfare benefit as their main source of income to have a 12 month mental disorder, although this difference did not reach conventional levels of statistical significance (perhaps reflecting relatively small numbers in the latter category). Sole parents aged 45–64 years were less likely to have a 12 month mental disorder than those aged 25–44 years, although again the differences were not statistically significant.
Counterintuitively, sole parents who met the criteria for the DSM-IV diagnoses were more likely than their partnered counterparts to have seen a health-care worker about their mental health. For example, 86.6% (80.7–92.6) of sole parents with a serious disorder had seen a health-care worker about that condition in the previous 12 months, compared to 83.2% (76.1–90.4) of partnered parents.
Multivariable modelling
A series of stepwise models was built for each outcome measure, adding covariates in turn as shown in Table 4. All possible interaction terms were included but retained only if statistically significant. The ORs represent the excess risk of the outcome in each model for sole versus partnered parents. The main multiple logistic regression results are summarized in Table 4.
Multivariable ORs for mental health outcomes as a function of parental status and covariates
OR, odds ratio.
n=1261 for sole parents and 3681 for partnered parents.
Sole parents were 2.6-fold more likely to have any 12 month mental disorder than partnered parents, after adjusting for age, sex and ethnicity. Further adjusting for physical health status had a small effect, while adjusting for income and employment (SEP) reduced the excess risk to just over twice that of partnered parents, with income accounting for most of the reduction. Inclusion of co-residence of another adult in the household in the model reduced the excess risk further, but even with all measured covariates included, sole parent were still 1.8-fold more likely to experience (any) mental illness than their partnered counterparts.
Sole parents were at a greater risk of (any) serious mental disorder than partnered parents (OR=almost 3 after demographic adjustment). Adjustment for SEP reduced these odds as much as did the presence of another adult in the household (to 2.1). With all variables included in the model, sole parents were still 1.6-fold more likely to experience a serious mental illness than partnered parents.
Examining specific types of mental illness, the excess risk experienced by sole parents was least for anxiety disorders (2.2-fold after demographic adjustment). Further adjusting for SEP reduced this to approximately 1.6, while adjusting for a co-resident adult had a smaller effect. Adjusting for all variables, the OR was only just statistically significant at the 95% level, with the point estimate suggesting a relatively small residual risk (approx. 1.5).
Of all the interactions tested, the only one found to be statistically significant was in the anxiety model, where a strong interaction between sole parenthood and chronic physical disease was found. Because of this interaction it is likely that the ORs for anxiety shown in Table 3 are underestimated for sole parents without a chronic physical condition(s), and over-estimated for those with such a condition. Because the number of sole parents with chronic physical disease in the sample is small, we did not carry out a stratified analysis (to estimate the OR separately for each physical condition group). The anxiety ORs shown in Table 3 thus represent the effect of sole parent status ‘averaged’ across the two groups (those with or without a chronic physical condition). Because these ORs are in the same direction, it is unlikely that this simplification of the model has any consequence in terms of the conclusions drawn.
Sole parents had a greater excess risk of mood disorders (OR=2.6 after demographic adjustment) than anxiety disorders compared to partnered parents. While both adjustment for SEP and (separately) for a co-resident adult substantially reduced this excess risk, even with all covariates included in the model, sole parents remained 1.8-fold more at risk of mood disorders (mainly depression) than partnered parents. The greatest excess risk, however, was for substance abuse, which consists mainly of alcohol abuse and dependence (Ors>3). Furthermore, neither SEP nor a co-resident adult strongly influenced this excess risk, such that after adjusting for all included covariates, sole parents remained more than threefold more likely than partnered parents to experience a substance use disorder.
Sole parents were approximately 2.5-fold more likely than partnered parents to have suicidal thoughts (after demographic adjustment). This was reduced to approximately 1.7 by both SEP and co-resident adult adjustment separately. With all covariates included, the OR was no longer statistically significant, although the point estimate was compatible with a small residual elevation of risk (approx. 1.2).
Explained fractions
The explained fraction estimates are summarized in Table 5. Table 5 shows that the skewed socioeconomic distribution of sole compared to partnered parents explains only approximately one-third of the former group's excess risk of mental illness. The proportion accounted for by low SEP, however, varies with the type of illness, ranging from one-quarter for substance use disorders to approximately half for anxiety disorders and suicidal ideation. In all cases, income makes a far greater contribution than employment status.
Proportion of the excess risk of mental illness experienced by sole parents mediated by various factors
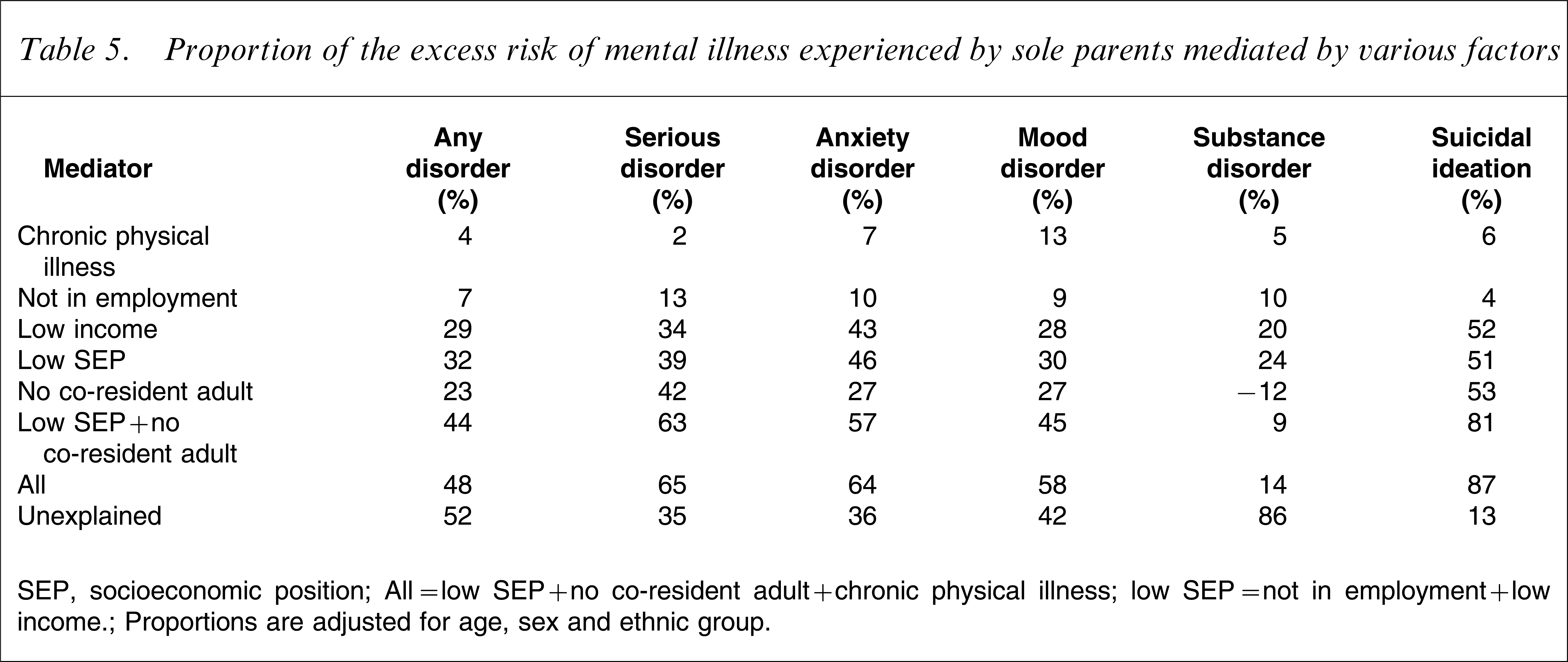
SEP, socioeconomic position.
All=low SEP+no co-resident adult+chronic physical illness; low SEP=not in employment+low income.
Proportions are adjusted for age, sex and ethnic group.
Lack of a co-resident adult in the household makes an independent contribution to the excess mental health risk of sole parents as SEP, explaining approximately one-quarter of the excess overall. The pattern varies across different disorder types, with the greatest contribution being to the risk of suicidal ideation and serious mental disorder. For serious mental disorder, low SEP and the absence of a co-resident adult each make an equal contribution (approx. 40%). Interestingly, presence of a co-resident adult appears to increase the risk of substance disorder for sole parents.
Poor physical health status makes only a minor contribution to sole parents’ excess risk of poor mental health – except with regard to mood disorders, where poor physical health explains approximately one-tenth of the excess risk. The combination of SEP and co-residence, together with the small independent contribution from physical illness, explains approximately half of sole parents’ excess risk for any mental disorder; approximately two-thirds of the excess risk for serious and anxiety disorders; almost all (87%) of the excess risk for suicidal ideation; but little (14%) of the excess risk for substance abuse or dependence.
Discussion
Key findings
This study quantifies for the first time in New Zealand sole parents’ excess risk of mental illnesses, ranging from more than threefold for substance use disorders to twofold for anxiety disorders. The present findings refute the widely held view that such risk elevation results simply from sole parents’ disadvantaged social position. Instead, equalizing the demographic and socioeconomic distributions of sole and partnered parents reduce the former's excess mental health risk by only approximately one-third (more for anxiety disorders and suicidal ideation, less for mood disorders and substance use disorders). In fact, we found that not having another adult living in the household is nearly as important a risk factor as low SEP (except for substance use disorder, which is positively associated with co-residence of another adult in the present study). Furthermore, most of the SEP effect is mediated by income; employment status seems to contribute little (independently of income). The combination of SEP and co-residence explained virtually all the excess risk of sole parents for suicidal ideation; two-thirds of the excess risk for anxiety disorders; just over half of the excess risk for mood disorders; but only one-quarter for substance use disorders.
Evidence from other studies
Only one previous New Zealand study has estimated the mental health risks experienced by sole compared with partnered parents, but that study did not use a diagnostic tool to examine specific mental illnesses, only overall self reported ‘mental health’ status [3]. That study also found significantly worse ‘mental health’ among sole parents, which persisted after sociodemographic adjustment.
A search of the international literature found relatively few studies that have recruited a nationally representative sample of sole and partnered parents, undertaken a comprehensive assessment of mental health status, and measured both SEP and social support (or adult co-residence) as covariates. Baker and North analysed cross-sectional data from the Avon Longitudinal Study of Pregnancy and Childhood (UK) with results similar to ours, at least for major depressive disorder (the only mental health outcome examined) [13]. Importantly, logistic regression showed no significant independent association between employment and depression among lone mothers, which was interpreted by the authors as evidence against ‘welfare to work’ policies. Similarly, Cairney et al. analysed cross-sectional data from the Canadian National Population Health Survey with similar findings, again restricted to major depressive disorder [14]. Those authors estimated that 40% of sole parents’ excess risk could be attributed to the joint effect of stress and perceived lack of social support. Finally, three Australian studies analysed cross-sectional data from the Australian National Survey of Mental Health, the Australian Longitudinal Study of Women's Health and the Household Income and Labour Dynamics in Australian Survey, respectively, once again with very similar findings to our own [15–17]. In particular, the Australian studies collectively support our conclusion that financial hardship and perceived lack of social support are the major measurable factors associated with sole parents’ excess risk of mental illness, while labour market attachment (independent of income) is at most a minor factor.
Strengths and limitations
The strengths of the present study are first, the large and nationally representative population-based sample of both sole and partnered parents, and second, the use of the CIDI survey instrument, which yields prevalence estimates for specific, diagnosable (and mostly treatable) mental illnesses.
At the same time the present study – like all studies – is not without limitations. First, its cross-sectional design prevents exploration of the temporal dynamics of relationships (e.g. spells of unpartnered parenting), social factors (e.g. spells of unemployment), and health states (e.g. spells of remission and relapse of chronic mental and physical illnesses and associated disability). Related to this, a cross-sectional study cannot prove causality, so the present conclusions are predicated on the assumption that the statistical associations we report are in fact causal, at least in part. Second, we focused on policy-sensitive variables and so paid little attention to non-modifiable demographic factors. Yet the sole parent population is very heterogenous, and differences between (for example) young never-partnered parents and older between-partner parents are worthy of further exploration. Third, some important explanatory variables have been omitted from our model (because the data were not collected in the New Zealand Mental Health Survey or elsewhere): including domestic violence and stigma/discrimination; number, age and health of children; availability of support from ex-partner and extended family; and access to local facilities and transport. And even those variables that have been included are (necessarily) imperfectly specified and measured. In particular, SEP is measured at only one point in time (rather than over the life course) and the combination of income and employment does not fully capture all dimensions of social status. Also, the co-resident adult variable is not an ideal proxy for social support in that it does not differentiate between kinds and qualities of support provided (e.g. financial or emotional support); it does not capture support sourced from outside the household; and for some sole parents co-residence may be a source of stress, conflict and negative interpersonal interactions rather than support. It could further be argued that co-residence in fact measures loneliness or social isolation rather than social support. Prevalence of loneliness has been found to be elevated among sole parents in Australia, and to be associated with sole parents’ poorer mental health [17]. It could also be argued that, to the extent that co-residence reflects financial support or household economies of scale, it is not independent of variables such as household income or SEP. No significant interactions, however, were found in the regression models. Finally, parenting status was self-reported so some misclassification may have occurred; but any such misclassification will have been non-differential with respect to mental health status and so will have biased the association between sole parenting and mental illness towards the null.
Finally, the present analysis could be criticized as being deficit rather than strengths based, thereby tending to pathologize sole parenthood and risk victim-blaming. While we recognize the limited view of this medical model, it is only through such an analysis that need can be quantitatively measured and appropriate social and health-care policies and services rationally designed and resourced.
What might explain the residual risk?
Before drawing conclusions for policy, explanations for the residual excess mental health risk borne by sole parents, after adjusting for SEP, presence/absence of a co-resident adult and physical health status, need to be considered (as shown earlier, this residual is estimated to be approximately half the total excess risk). First, imprecision in the measurement of the covariates included in the models may account for some of the unexplained variation. A second explanation is health selection: as well as sole parenthood leading to poorer mental health, mental illness may instead (or in turn) reduce the chances of finding a partner (or another partner). There is some evidence in support of health selection [18], and it could well account for part of the residual risk, although – given the large size of the residual – it is unlikely to explain all of it. A third explanation is stigma: the stigma and discrimination associated with sole parent status could be health damaging, although there is little evidence for this in the literature. Finally, a major Australian study has shown that sole parents are more likely than others to be victims of violence (including sexual abuse), even after adjusting for a wide range of socioeconomic and demographic variables [14] – which could again explain some of the residual risk (in particular, the excess risk of post-traumatic stress disorder and depression).
Implications for policy
The most obvious implication is the need to improve access to and quality of primary mental health care for sole parents. The higher rates of diagnosable (although not necessarily diagnosed) mental illness experienced by sole parents are definitively documented in this paper. In particular, sole parents are more at risk of serious mental illness, and of co-morbidity. Primary health-care providers need to be more aware of this heightened risk among their sole parent patients, screen such patients regularly for common mental disorders using appropriate brief instruments, and treat these disorders effectively or refer such patients to community mental health services for treatment. Alcohol and drug rehabilitation services are also clearly a priority for this vulnerable group, especially given the present finding that social policies would have only very limited effect on the risk of substance abuse and dependence. The small but significant impact of chronic physical conditions on sole parents’ excess risk of mental illness is also noteworthy – and this measures only the direct effect of physical health on mental health. Physical health status will also contribute indirectly via health selection, assuming that the latter does in fact account for at least some of the unexplained excess mental health risk of sole parents. Future research using this (and other) dataset(s) could examine health service use (and the appropriateness of such use), unmet need, and comorbidity in more detail.
The present results provide further evidence in support of policies mandating income or social transfers (e.g. increased domestic purposes benefits, and free or subsidized childcare) for sole parents: we estimate that up to one-quarter of the excess risk of mental illness experienced by sole parents could be eliminated through such policies. At the same time, the limited potential impact of such policies must also be recognized: clearly, income redistribution alone is not enough. Interestingly, the present results fail to support welfare-to-work policies: employment per se was only weakly associated with the mental health of sole parents (once any effect on income was adjusted for). One possible explanation for this may relate to conflict between the ‘parent’ and ‘provider’ roles. Active labour market policies are still important, but only in terms of sole parents gaining access to market income. For sole parents in paid work, the Working for Families package implemented between October 2004 and April 2007 (since the survey) will have had a substantial effect on household incomes [19].
The present results imply that policymakers and their advisors need to consider a wider array of policy responses, designed to enhance social support for sole parents as well as improving their incomes. A range of housing, transport, telecommunication and other policies could be implemented that would increase the opportunities for sole parents to enjoy emotional and instrumental support from other adults (whether co-resident or non-resident family, friends or neighbours) – with consequential improvement in their mental health status.
Reversing the gaze, the present study implies (assuming the associations reported here are causal) that sole parents who are well supported financially, emotionally and socially are more likely than unsupported sole parents to experience good mental health – with benefits not only for themselves and their dependent children but for wider New Zealand society as well. At the same time, efforts to reduce stereotyping and stigmatization of sole parents should be promoted, as should improvements in access for these parents to community mental health and primary health-care services.
Footnotes
Acknowledgements
We gratefully acknowledge the investigators and participants of Te Rau Hinengaro: the New Zealand Mental Health Survey, without whom this study would not have been possible. This study forms part of a cross-departmental research project led by the Ministry of Social Development, entitled ‘Resilience in vulnerable sole parent families’. We thank our project collaborators for thoughtful peer review of earlier drafts of this report. The report is published with the approval of the Deputy Director General of Health (Health and Disability Systems Strategy Directorate), but opinions are the authors’ own and do not necessarily reflect policy advice of the Ministry or the project partners.