
Abstract
Prevalence rates for the anxiety disorders have been somewhat variable across national epidemiological surveys, with 12-month prevalence rates ranging between 5.2% and 18.1% and lifetime rates between 19.3% and 28.8% [1–8]. In part, estimates vary across surveys due to a number of methodological differences, such as the inclusion of a different set of anxiety disorders and the use of different diagnostic tools and criteria (e.g. different versions of the
The World Health Organization's World Mental Health (WMH) Survey Consortium attempted to minimise these methodological differences by developing the World Mental Health – Composite International Diagnostic Interview (WMH-CIDI) [9], which has now been administered across some 28 countries. However, estimates of the prevalence of anxiety disorders reported by countries using the WMH-CIDI also vary substantially (2.4% to 18.2%) [10], suggesting that there may be real differences rather than only method variance in the prevalence estimates of mental disorders. Alternatively, the survey may be sensitive to cultural differences in the expression or reporting of mental disorders. Regardless of these potential differences one robust finding across surveys has been that anxiety disorders are more prevalent than affective disorders and substance use disorders (SUDs).
A number of sociodemographic correlates have been reliably associated with mental disorders in general, and anxiety disorders in particular. For instance, being female [2,4–8,11], being in the early to middle age ranges [2,4,7,8,11], never being married or being separated, divorced or widowed [5,6], obesity [12–14], and being of a lower socioeconomic status (education, income, occupational situation) [2,5,6,8] have all been associated with an increased odds of having an anxiety disorder. While the first Australian National Survey of Mental Health and Wellbeing (NSMHWB) in 1997 replicated many of these findings in relation to 12-month diagnoses, the second NSMHWB in 2007 enables, for the first time, the examination of correlates in relation to lifetime diagnoses. Demographic and clinical correlates that have not been previously investigated in Australia were also included in the 2007 survey, such as income, chronic medical conditions, social support, body mass index, and family history of mental disorders.
Comorbidity is also important to consider because it is often associated with increased service use, higher functional disability, and a more chronic illness course [15–17]. Anxiety disorders are particularly highly comorbid with affective disorders, but also increase the odds of meeting criteria for SUDs [16,18]. It has also been suggested that some disorders, particularly anxiety and affective disorders, may undergo a process of de-differentiation with age [19]. For instance, some authors have speculated that ‘generalized anxiety may represent a “core” anxiety syndrome, increasing with age as an apparent “de-differentiation” of the anxiety disorders takes place, and possibly interchanging over time with depression’(p. 95) [20]. Therefore, examining comorbidity in the emotional disorders across the lifespan may aid our understanding of the relationships between disorders.
The 2007 NSMHWB in Australia used the WMH-CIDI, which has a number of advantages over the 1997 survey. First, whereas the 1997 survey assessed 12-month diagnoses the 2007 survey assessed for lifetime diagnoses (from which 12-month diagnoses can be derived), and thus provides the first opportunity to estimate the lifetime prevalence of anxiety disorders in Australia. Second, while the use of the WMH-CIDI limits comparisons with the 1997 Australian survey, it facilitates more direct international comparisons. The first aim of this study was therefore to report 12-month and lifetime prevalence of DSM-IV anxiety disorders across the lifespan using the WMH-CIDI in Australia. Cohort effects have been observed in 12-month diagnoses in Australia [4] and New Zealand [8], and in lifetime diagnoses in New Zealand [11] and other international surveys [21], with prevalence rates typically being highest in the early and middle ages and declining after 55 years of age. Our study sought to determine whether these findings were replicated in the 2007 survey with both 12-month and lifetime diagnoses. The second aim of this study was to replicate and extend previous studies by examining additional demographic and clinical correlates of anxiety disorders, including income, comorbid physical conditions, smoking status, body mass index, and family history of mental disorders, in relation to 12-month and lifetime diagnoses. The third aim was to examine the rates of comorbidity among anxiety, affective, and SUDs across the lifespan.
Method
Sample
The data come from the Australian National Survey of Mental Health and Wellbeing (NSMHWB), a nationwide household survey of adults conducted in 2007. The purpose of the survey was to measure the current prevalence, severity, and impact of common mental disorders and health service utilization (see Slade
Measures
World Mental Health Survey Initiative version of the Composite International Diagnostic Interview
A modified version of the WMH-CIDI (3.0, Computer Assisted Personal Interview version 20 [9]) was used to collect diagnostic information on a broad range of mental disorders, along with information on risk factors, impacts, patterns and treatment of mental disorders. Modifications were undertaken for the purposes of brevity, making it more appropriate to the Australian context, and removing sequencing errors from earlier versions of the interview. These sequencing errors related to the diagnoses of alcohol/drug dependence [23] and obsessive–compulsive disorder [24]. The symptoms of PTSD were asked only in relation to the respondent's worst event. In addition, all respondents completed all diagnostic sections. The WMH-CIDI produces DSM-IV and ICD-10 diagnoses, but only DSM-IV diagnoses are reported here. The WMH-CIDI uses a lifetime time frame, with questions on experiences of symptoms in the previous 12 months in combination with lifetime diagnoses being used to establish 12-month diagnoses, respectively. Prevalence rates are reported using diagnosis variables with the hierarchy rules applied. In order to capture the true extent of co-occurring disorders the ‘without hierarchy’ diagnoses are used when exploring comorbidity. Diagnoses were categorised into three classes of mental disorder: (i) affective disorders (depression, dysthymia, bipolar affective disorder type I or II); (ii) anxiety disorders (agoraphobia, social phobia, panic disorder, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder), and (iii) substance use disorders (alcohol and drug abuse and dependence). Specific phobia was excluded from the survey.
Procedure
Interviews were conducted by Australian Bureau of Statistics (ABS) interviewers with extensive prior experience in conducting household surveys. Interviewers completed a 4 day training programme, with the programme trainers receiving official WMH-CIDI training from the US CIDI Training and Reference Centre based at the University of Michigan. Interviews were conducted in the respondent's households using a Computer-Assisted Personal Interview (CAPI) questionnaire and took an average of 90 min to complete. Survey participation was voluntary and not remunerated.
Analysis
Data were initially weighted according to the inverse of the probability of being selected in the survey. These initial weights were then calibrated against known population estimates derived from other data sources such as census data. In addition to the standard ABS procedures of calibration of initial weights to the benchmarks of state, part of state, age and sex, weights were further calibrated against benchmarks for household composition, educational attainment, and labour force status. Standard errors and 95% confidence intervals were calculated using jack-knife repeated replication to take into account the complex sampling design. Logistic regression analyses were carried out to examine the association between sociodemographic and clinical factors and the presence of both 12-month and lifetime any anxiety disorder. Estimates of projected lifetime risk and median age of onset were obtained using Kaplan-Meier survival estimates. Analyses were carried out using the SUDAAN [25] and Stata [26] software packages.
Results
Prevalence rates and age of onset
The 12-month prevalence rate of any anxiety disorder was estimated at 11.8% and lifetime prevalence at 20.0% (Table 1). Twelve month (lifetime) estimates for each anxiety disorder were 4.2% (8.4%) for social phobia, 4.4% (7.2%) for post-traumatic stress disorder (PTSD), 1.9% (6.1%) for generalised anxiety disorder (GAD), 2.7% (3.8%) for obsessive compulsive disorder (OCD), 1.8% (3.5%) for panic disorder, and 1.2% (2.3%) for agoraphobia. For comparison, the overall 12-month (lifetime) prevalence rates for affective disorders and SUDs were 5.8% (14.4%) and 5.1% (24.2%), respectively. Among those individuals with any 12-month anxiety disorder, 37.2% had PTSD, 35.7% had social phobia, 28.2% had GAD, 22.8% had OCD, 15.2% had panic disorder, and 9.8% had agoraphobia. The highest rates of anxiety disorders were generally evident in the 35–44 and the 45–54 year age groups. Prevalence steadily increased from the 16–24 year group, peaked in the 35–44 year group, and precipitously declined to the 75–85 year group. Specifically, between the 55–64 and 65–74 year groups the prevalence almost halved, and then almost halved again in the 75–85 year group. The one exception to this pattern was the 12-month prevalence for women, which remained steady from the 16–24 age group to the 45–54 age group, with a decline only evident from the 55–64 age group onwards. The prevalence of anxiety disorders was higher for women than men at all age groups, although the difference was largest in the youngest age group and smallest in the oldest age groups (Table 1).
Weighted prevalence (standard error) of lifetime and 12-month DSM-IV any anxiety disorder by age and sex in the NSMHWB, 2007
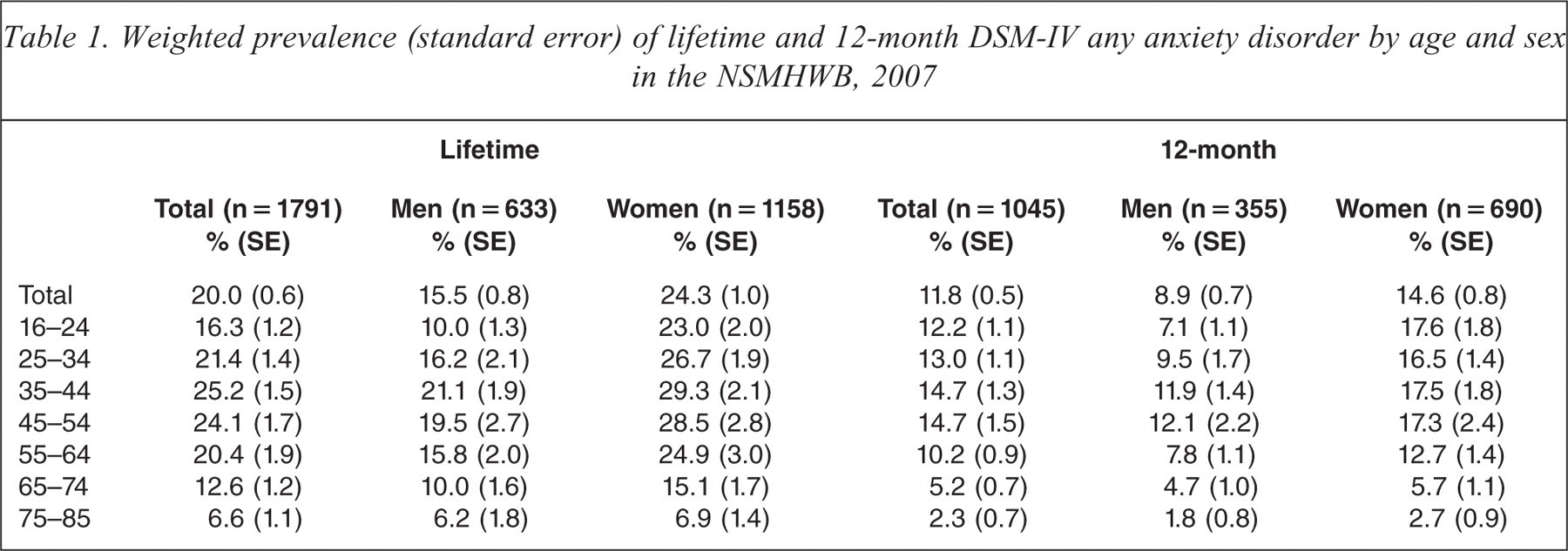
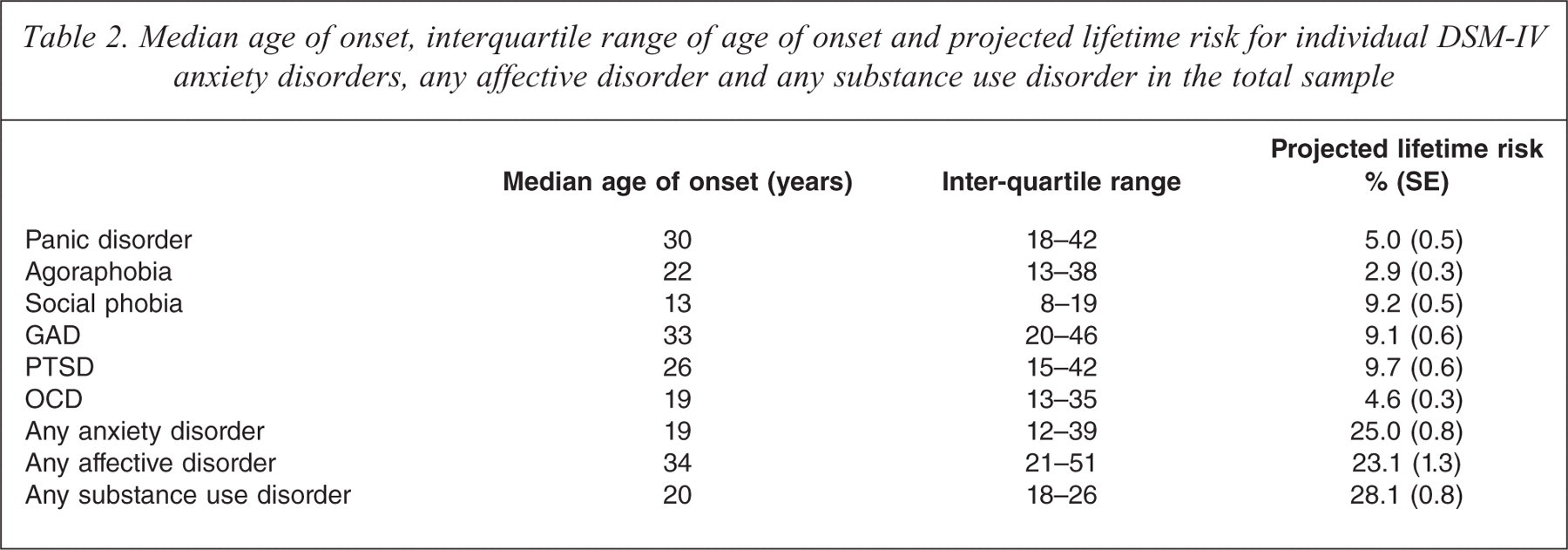
Table 2 shows that the median age of onset for any anxiety disorder was 19 years (interquartile range (IQR) = 12–39), which was earlier than for affective disorders (median = 34, IQR = 21–51) and around the same time as SUDs (median = 20, IQR = 18–26). There was considerable variability across the anxiety disorders, with social phobia having the earliest (13 years, IQR = 8–19) and GAD having the latest median age of onset (33 years, IQR = 20–46). Projected lifetime risk is an estimate of the lifetime prevalence of disorder had all respondents been aged 85 at the time of the interview. Results show that disorders with an early age of onset (e.g. social phobia) have a projected lifetime risk that is close to the estimated lifetime prevalence while disorders with a later age of onset (e.g. GAD) have a larger gap between projected lifetime risk and estimated lifetime prevalence.
Median age of onset, interquartile range of age of onset and projected lifetime risk for individual DSM-IV anxiety disorders, any affective disorder and any substance use disorder in the total sample
Demographic correlates of anxiety disorders
In the univariable analyses 12-month anxiety disorders were over-represented in women compared to men, and in those who were widowed/separated/divorced or never married compared to those who were married or in a de facto relationship. Those in the oldest age group (65–85) were less likely to attract a diagnosis than those in the youngest age group. Individuals with only a school qualification were more likely to have an anxiety disorder than those with post-school qualifications, and being in the fourth and fifth (top) quintiles for income was associated with lower odds of having an anxiety disorder compared to being in the first (bottom) quintile. Those from other non-English-speaking countries were less likely than those from other English-speaking countries or those from Australia to have an anxiety disorder. These findings were identical in the multivariable analyses, with two exceptions. First, the 25–44 and 45–64 age groups had higher odds of meeting criteria for an anxiety disorder than those in the 16–24 age group, and second, those not in the labour force had higher odds than those who were employed. Reasons for respondents not being in the labour force include, but are not limited to, ill health, physical disability, pregnancy, studying, retirement, childcare, lacking necessary school training, skills or experience, and difficulties with language (see Table 3). The pattern of findings for lifetime correlates was identical to that of the 12-month correlates, with two exceptions. First, having a post-school qualification was not associated with less odds of having a lifetime anxiety disorder compared to only having school qualifications with either the univariable or multivariable analyses. Second, the 25–44 and 45–64 age ranges had higher odds of having a lifetime anxiety disorder than the 16–24 age range for both univariable and multivariable analyses (see Supplementary Table 1).
Demographic correlates of 12-month diagnosis of a DSM-IV anxiety disorder
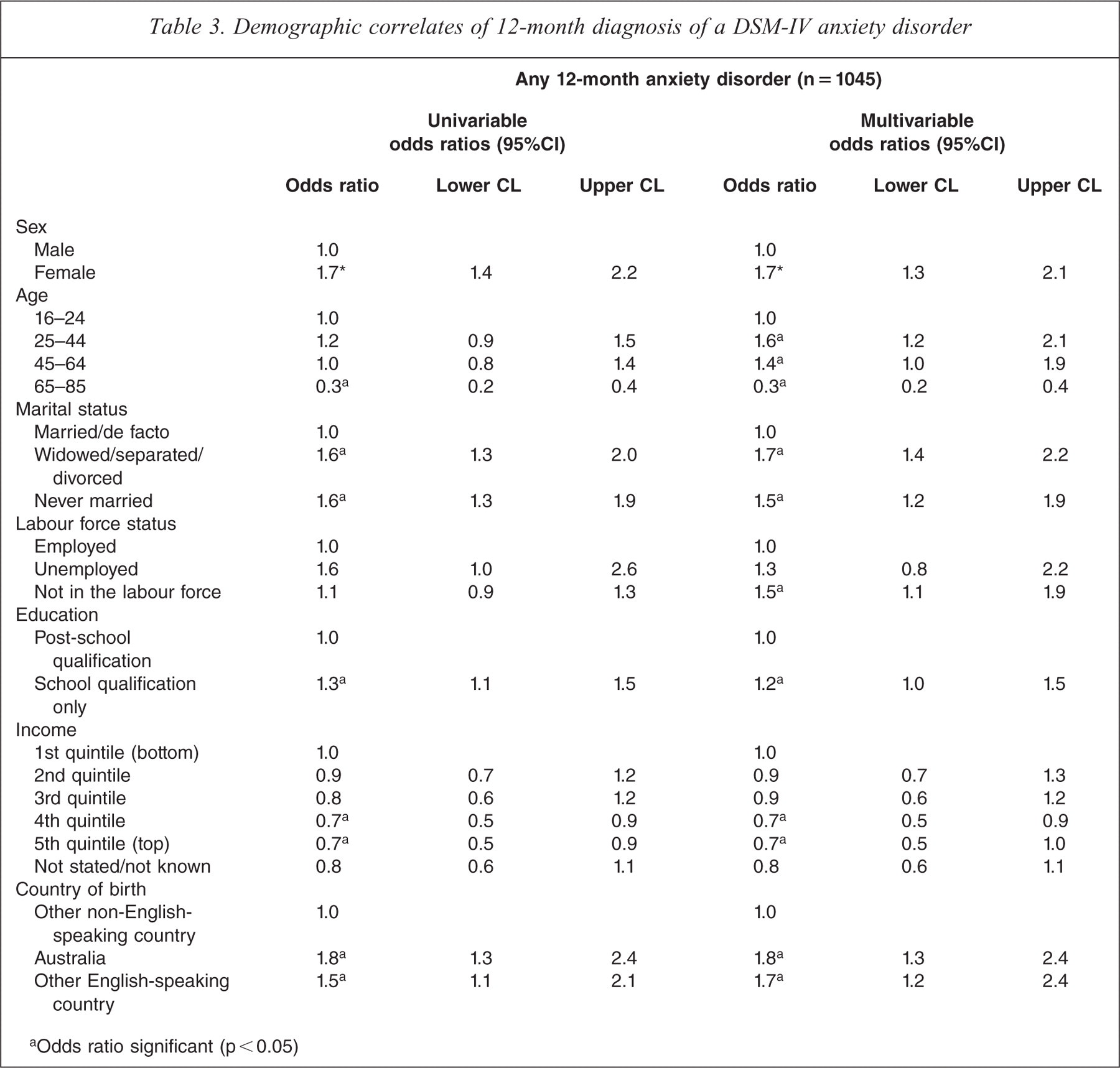
Odds ratio significant (p<0.05)
Clinical correlates of anxiety disorders
In addition to examining demographic correlates, odds ratios were calculated for a set of clinical correlates of anxiety disorders including comorbid physical conditions, smoking status, body mass index, and family history of anxiety, affective and SUDs. The presence of a physical condition (versus no physical condition), being a current or ex-smoker (versus never smoked), having a family history of anxiety disorders, affective disorders or SUDs (versus no family history) were all associated with increased odds of meeting criteria for an anxiety disorder in both univariable and multivariable analyses. Body mass index was not significantly associated with increased odds of an anxiety disorder (Table 4). The pattern of findings was identical with lifetime anxiety disorder diagnoses (see Supplementary Table 2).
Clinical correlates of 12-month diagnosis of a DSM-IV anxiety disorder
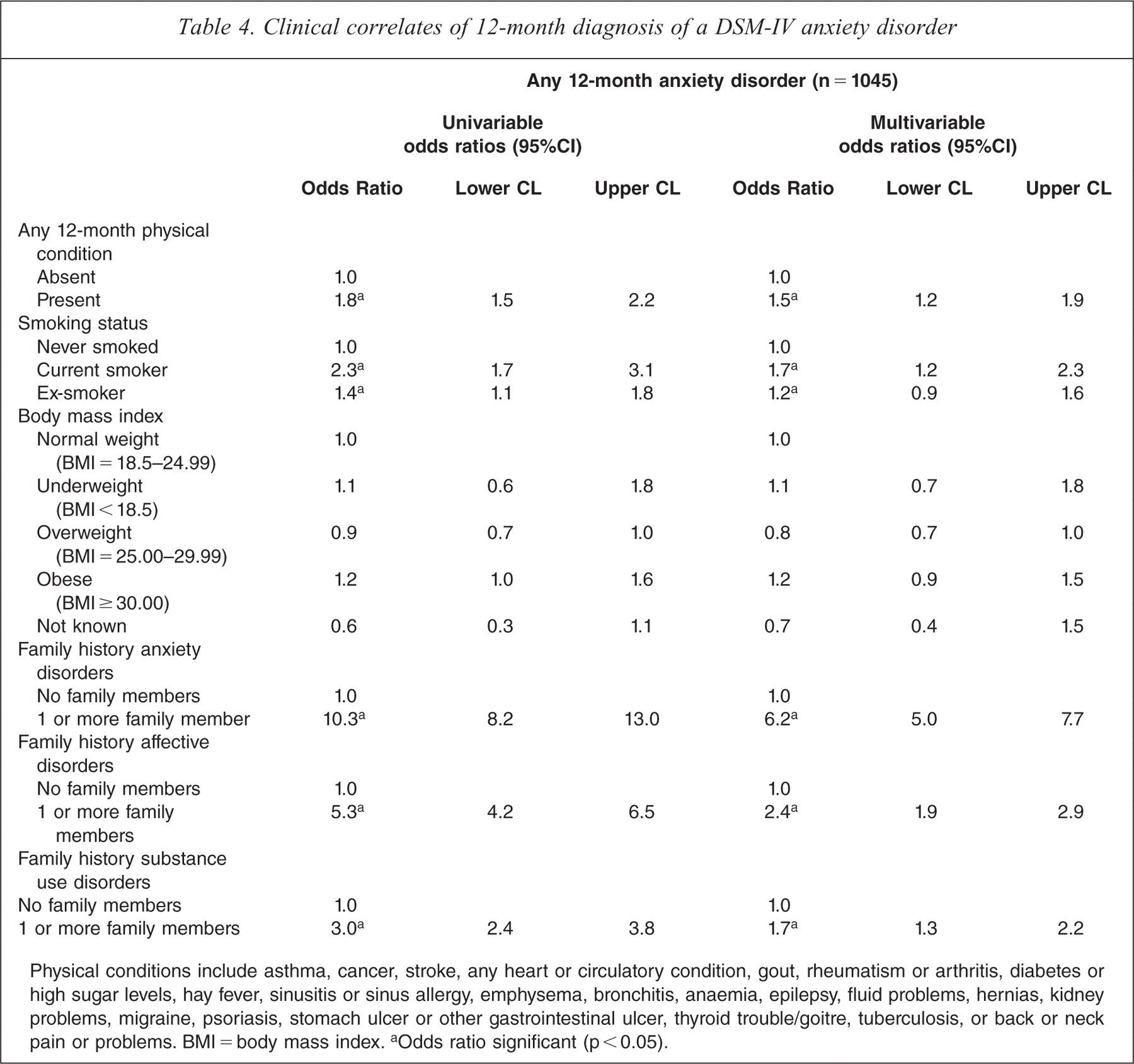
Physical conditions include asthma, cancer, stroke, any heart or circulatory condition, gout, rheumatism or arthritis, diabetes or high sugar levels, hay fever, sinusitis or sinus allergy, emphysema, bronchitis, anaemia, epilepsy, fluid problems, hernias, kidney problems, migraine, psoriasis, stomach ulcer or other gastrointestinal ulcer, thyroid trouble/goitre, tuberculosis, or back or neck pain or problems. BMI = body mass index.
Odds ratio significant (p<0.05).
Comorbidity
Among those individuals with any 12-month anxiety disorder, 67.8% met criteria for only one anxiety disorder, 21.5% had two anxiety disorders, 6.5% had three anxiety disorders, and 4.2% had four or more anxiety disorders. Individuals meeting criteria for an anxiety disorder were around 13 times more likely to meet criteria for an affective disorder than individuals not meeting criteria for an anxiety disorder. More specifically, individuals meeting criteria for an anxiety disorder were most likely to meet criteria for comorbid major depression, followed by dysthymia. Those meeting criteria for an anxiety disorder were not significantly more likely to meet criteria for bipolar affective disorder than those not meeting criteria for an anxiety disorder. Anxiety disorders were associated with a significant increase in the odds of meeting criteria for an alcohol use disorders, particularly alcohol dependence. However, they were not associated with a significant increase in drug use disorders or alcohol abuse (see Table 5).
Prevalence, odds ratios and 95% confidence interval for comorbid affective and substance use disorders among those with a 12-month anxiety disorder
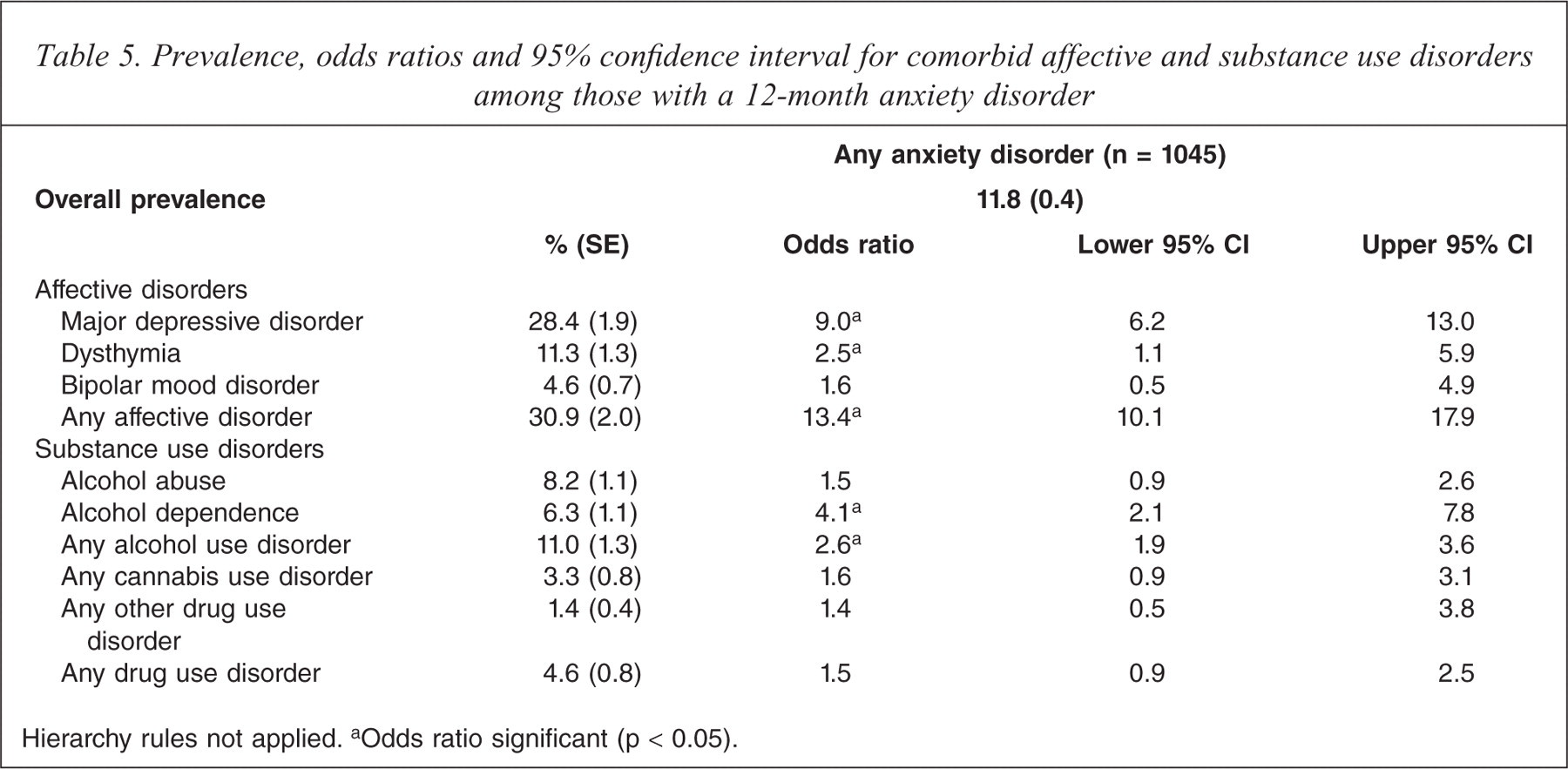
Hierarchy rules not applied.
Odds ratio significant (p < 0.05).
Comorbidity by age
Figure 1 shows rates of comorbidity between any anxiety disorder and other mood and substance use disorders across the lifespan. The rate of comorbidity with major depressive disorder is consistently high across the age categories. Interestingly, comorbidity with dysthymia increases slightly from the 16–24 to the 55–64 age ranges, before reducing in the 65–74 age range and then almost quadrupling in the 75–85 age category. In contrast, comorbidity with bipolar disorder and alcohol use and drug use disorders diminishes with age.
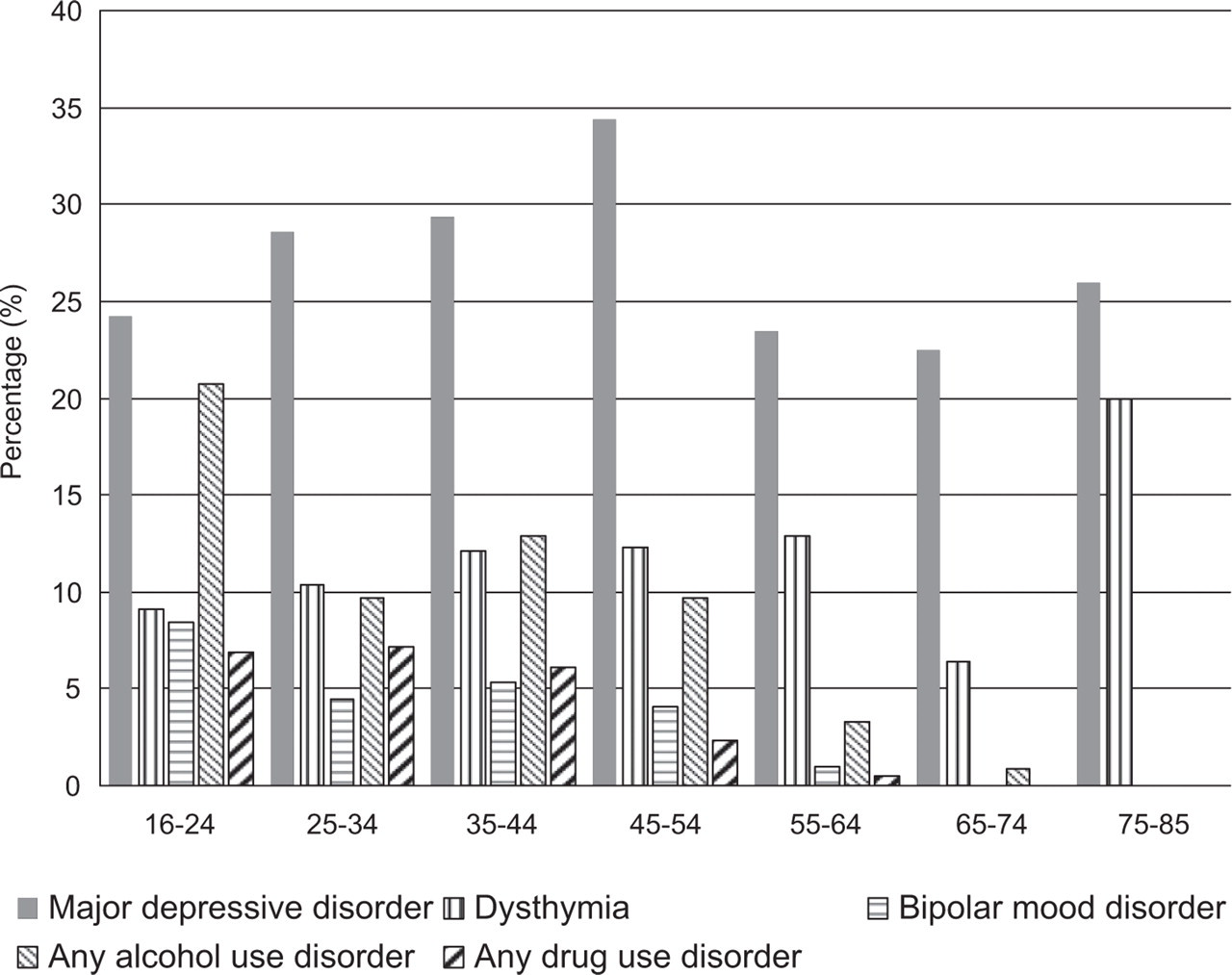
Prevalence of comorbid affective and substance use disorders among those with a 12-month anxiety disorder by age.
Discussion
The first aim of this study was to report 12-month and lifetime prevalence estimates of DSM-IV anxiety disorders from the Australian NSMHWB, 2007. The estimated lifetime prevalence was 20% and the 12-month prevalence was 11.8%, which is more than twice the rate reported in the 1997 Australian survey (5.2%) [1]. The higher prevalence rates found in the 2007 survey compared to the 1997 survey may be attributable to modifications made to the assessment of anxiety disorders. For instance, between 1997 and 2007 the potential list of specific traumas in the assessment of PTSD increased from 11 to 27, the list of specific social situations triggering social anxiety increased from 7 to 13, and the list of specific agoraphobic situations triggering agoraphobia increased from 4 to 11, all of which may have captured anxiety responses related to a broader array of situations [27].
Compared to other countries within the WHO World Mental Health Survey Consortium [10], the 12-month prevalence rate was within the range from the Americas (6.8–18.2%), at the upper end of the range for Europe (5.8–12%), similar to Lebanon (11.2%), and higher than in Nigeria (3.3%) and Asian countries (2.4%–5.3%). The Australian prevalence estimates are also similar to previous surveys in the Netherlands (12-month = 12.4%, lifetime = 19.3%, [2]), USA (12-month = 11.1%, [3]), and Germany (12-month = 14.5%, [5]), somewhat higher than in Europe (12-month 8.4%, lifetime = 14.5, [28]), but lower than the National Comorbidity Survey Replication (NCS-R) study in the USA (12-month = 18.1%, lifetime = 28.8%, [6,21]) and the New Zealand Mental Health Survey (NZMHS, 12-month = 14.8%, lifetime = 24.9% [7,11]). The NCS-R included specific phobias (12-month = 8.7%) and separation anxiety disorder (12-month = 0.9%), and the NZMHS included specific phobias (12-month = 7.3%, lifetime = 10.8%), which might explain these discrepancies.
Given the differences in the disorders included in each survey, clearer comparisons can be made for specific disorders [7]. Lifetime and 12-month prevalence rates from the Australian survey were higher for all disorders compared to the European survey, although the variability across the European countries makes comparisons difficult [28]. Comparisons with the NCS-R [6,21] and NZMHS (Wells 7,11] for social phobia showed that Australia had a similar lifetime prevalence rate (8.4%) to New Zealand (9.4%) but lower than the USA (12.1%), and a similar pattern was found for 12-month prevalence (4.2%, 5.1%, and 6.8%, respectively). For GAD, the lifetime prevalence was remarkably similar for Australia (6.1%), New Zealand (6.0%), and the USA (5.7%), although 12-month prevalence was higher for the USA (3.1%) compared to Australia (1.9%) and New Zealand (2.0%). For PTSD, Australia had a slightly higher lifetime (7.2%) and 12-month (4.4%) prevalence compared to New Zealand (6.0% and 3.0%, respectively) and the USA (6.8% and 3.5%, respectively). Australia also had higher lifetime (3.8%) and 12-month (2.7%) prevalence rates for OCD compared to New Zealand (1.2% and 0.6%, respectively) and the USA (1.6% and 1.0%, respectively), however this may have been a result of a skip error identified in earlier versions of the OCD section of the WMH-CIDI [24]. Similarly, Australia had higher lifetime (2.3%) and 12-month (1.2%) prevalence rates for agoraphobia compared to New Zealand (1.2% and 0.6%, respectively) and the USA (1.4% and 0.8%, respectively). For panic disorder, lifetime prevalence was highest in the US (4.7%), followed by Australia (3.5%) and New Zealand (2.7%), respectively. Twelve-month prevalence for panic disorder in Australia (1.8%) was similar to New Zealand (1.7%), but lower than in the USA (2.7%). In sum, prevalence rates in Australia were highest relative to New Zealand and the USA for PTSD, OCD and agoraphobia, were similar across countries for GAD (especially lifetime), and were in the lower range in Australia for social phobia and panic disorder.
Rates across countries could reflect true differences or method variance from variable response rates or survey questions. Method variance was minimized by using the WMH-CIDI and the same classification system, which resulted in more similar prevalence estimates to the NZMHS (particularly for PTSD and panic disorder) than when different classification systems have been used across the surveys in the past [see 29]. Despite potential differences, the rank order of disorders based on prevalence is remarkably similar across the Australian, European, New Zealand and USA studies. Social phobia was the most prevalent (lifetime and 12-month) anxiety disorder across all surveys, with the exception of 12-month prevalence in Australia where it was ranked behind PTSD. PTSD was the second most prevalent anxiety disorder (lifetime and 12-month) across most studies, with GAD generally being the third most prevalent disorder, although GAD ranked behind OCD in the Australian survey (12-month). The lower prevalence disorders (OCD, panic disorder, agoraphobia) were less consistent with their rankings across studies. Similar to previous findings, comparing across disorder groups anxiety disorders had higher 12-month prevalence than both SUDs and affective disorders [2, 6], although some studies have found similar lifetime prevalence estimates across the disorder groups [2].
On average, anxiety disorders and SUDs had similar median ages of onset (19 and 20 years respectively), followed by affective disorders (34 years). Previous studies have found the anxiety disorders tend to precede affective and SUDs [5,21]. However, temporal sequencing tends to vary depending upon the age of onset of the specific anxiety disorder [30] and there was considerable variability in our study, with social phobia having the earliest age of onset (13 years), followed by OCD, agoraphobia, PTSD, panic disorder, and generalized anxiety disorder (33 years). Phobic disorders (specific and social phobias) are consistently found to have the earliest age of onset, and GAD the latest age of onset, compared to other anxiety disorders [21,30,31]. The prevalence of anxiety disorders was significantly higher in the middle age categories and lower in the highest age categories, which is also consistent with previous research [2,4,29].
At first glance it may be surprising that lifetime prevalence reduces with age, given that older cohorts have by definition lived through a higher proportion of the risk period. It may be assumed that lifetime prevalence rates would be cumulative and thus be highest in older age groups. However, this pattern is consistent with previous literature and several explanations have been offered [20]. First, elderly people may be systematically absent from community samples due to non-response, emigration out of sampled areas, institutionalization or death. Second, older people may be less likely to disclose symptoms of emotional disorders or these symptoms may be attributed to physical illness, although recent evidence does not support the latter explanation [32]. Third, it may be that there has been a true historical increase in psychiatric disorders, so that lifetime prevalence will increase over the coming decades as younger cohorts age. A fourth possibility is that the diagnostic criteria are less valid for older individuals, such that the prominent symptoms of psychiatric disorders differ from those used in existing diagnostic nosologies. A fifth possibility is that older individuals fail to recall symptoms experienced early in their lifetimes, which would result in an underestimation of lifetime risk in older cohorts [33,34].
Significant demographic correlates of anxiety disorders in this study were consistent with numerous previous representative national surveys, including being female, not being in a committed relationship, being out of the labour force, being in the middle age ranges, and only having a high school qualification (12-month prevalence only). Interestingly, being born in Australia or another English-speaking country was associated with an increased risk, compared to those born in a non-English speaking country. This finding might reflect a healthy migrant effect, where immigrants are selected based on socioeconomic status and other factors associated with mental health, or alternatively the WMH-CIDI may not be sensitive to cultural differences in mental disorder phenotypes. A number of clinical correlates were also associated with meeting criteria for an anxiety disorder, including the presence of a physical condition and being a current or ex-smoker, although both had smaller odds in the multivariable model than the univariable models. It is plausible that smoking has both a direct effect and an indirect effect, via other physical conditions, on the prevalence of anxiety disorders. Having at least one family member with an anxiety disorder increased the odds of having an anxiety disorder 10-fold, whereas one or more family members with an affective disorder or SUD increased the odds of an anxiety disorder 5-fold and 3-fold, respectively. The pattern of findings was similar regardless of whether 12-month or lifetime diagnoses were examined.
Body mass index (BMI) has been found to be associated with mood disorders and the odds of having more than one disorder [12], as well as with anxiety disorders [13]. Being underweight, overweight or obese was not significantly related to the presence of an anxiety disorder in this study, although the odds ratio for obesity only just fell short of the conventional cut-off in the univariable model (OR = 1.2, 95%CI = 1.0–1.6). Scott et al. [13] collated data from 13 surveys with a total of 62 277 participants, so, although their odds ratio was similar (BMI 18.5–29.9 versus BMI ≥ 30, OR = 1.2, 95%CI = 1.1–1.3), our study had considerably less statistical power to detect an odds ratio of this magnitude.
As expected, anxiety disorders were highly comorbid with each other and with mood disorders and SUDs. Specifically, around one third of individuals with an anxiety disorder met criteria for at least one additional anxiety disorder. Compared to those without an anxiety disorder, respondents with an anxiety disorder were also much more likely to meet criteria for major depression, dysthymia and alcohol dependence, but not bipolar disorder, alcohol abuse or drug use disorders. While the rates of comorbidity between anxiety disorders and major depression were high and relatively consistent across the age cohorts, comorbidity with dysthymia substantially increased in the oldest age cohort. This finding suggests that internalizing disorders may undergo a process of de-differentiation over time and is consistent with previous studies demonstrating higher comorbidity [20] and higher correlations between anxiety and depression symptoms [35] in older compared to younger samples. These findings cannot be explained by poorer physical health leading to depression, given that the association between major depression and poor physical health weakens with age [36]. Future research investigating differential rates of comorbidity and sequencing of disorders across the lifespan for each anxiety disorder would be useful to better understand relationships between emotional disorders. Identification of biopsychosocial factors that could contribute to the coalescence of mood and anxiety disorders with age is also required. In contrast to affective disorders, the relationship between anxiety disorders and SUDs decreased with age, which suggests that these groups of disorders become more differentiated over time and thus are more separable from anxiety disorders than affective and anxiety disorder are from each other.
There are several limitations of this study that need to be considered. First, diagnostic criteria were assessed retrospectively and are therefore susceptible to multiple reporting and memory biases, particularly lifetime diagnoses. Second, diagnoses are limited to self-report and may therefore under or overestimate the true rates, although it has been suggested that self-reported psychiatric symptoms are more likely to be underestimated rather than overestimated [21]. Third, the response rate was only 60% so selection biases may limit the degree to which these findings generalise to the population as a whole or to specific subgroups. For instance, individuals who are non-English speaking, institutionalised, or homeless are likely to be underrepresented [21].
Anxiety disorders are common, have an earlier age of onset than affective and SUDs, and they are highly comorbid. Our findings suggest that almost 12% of Australian adults meet criteria for an anxiety disorder in any 12-month period, with one in five meeting criteria at some point in their lifetime. Similar to previous studies, we found evidence for a cohort effect, where both 12-month and lifetime prevalence estimates substantially reduced in the older age ranges. Together, these findings suggest that public health efforts should be focused on the prevention, early intervention, and treatment of anxiety disorders from early childhood through to the middle ages. Individuals who are single, not in the labour force, have a physical condition, have a history of smoking, or have a family history of mental disorders, particularly anxiety and affective disorders, may need to be targeted.